On This Page – Quick Medical Summary
If a doctor has ordered tests to check for pancreatic cancer — or has already raised it as a possibility — the waiting can be frightening. This guide walks through how doctors actually confirm the diagnosis, one step at a time, so you understand what each test is for and what the results mean.
Where you are right now shapes what matters most:
- You have a worrying symptom and tests are being arranged → Steps 1 and 2 explain what usually comes first.
- You’re mid-workup or newly diagnosed → the imaging, blood-test, and biopsy sections explain each result in plain language.
- You’re a caregiver → the questions to ask and the FAQ will help you support someone through it.
- A diagnosis has been confirmed → the final section connects the results to staging and what comes next.
For the bigger picture, this article sits within the full guide to pancreatic cancer symptoms and stages. Here, you’ll find the calm, sourced version of the journey — from first appointment to confirmed diagnosis.
ℹ️ Medical Disclaimer: This article is general health education, not medical advice. It does not diagnose pancreatic cancer, interpret your individual test results, or recommend treatment. Decisions about testing, diagnosis, staging, and treatment should be made with a board-certified gastroenterologist or oncologist who can evaluate your specific situation.
Why pancreatic cancer is often found late
Many people diagnosed with pancreatic cancer ask the same painful question: why wasn’t this caught sooner? The honest answer is that this cancer is genuinely hard to find early — and that is rarely anyone’s fault.
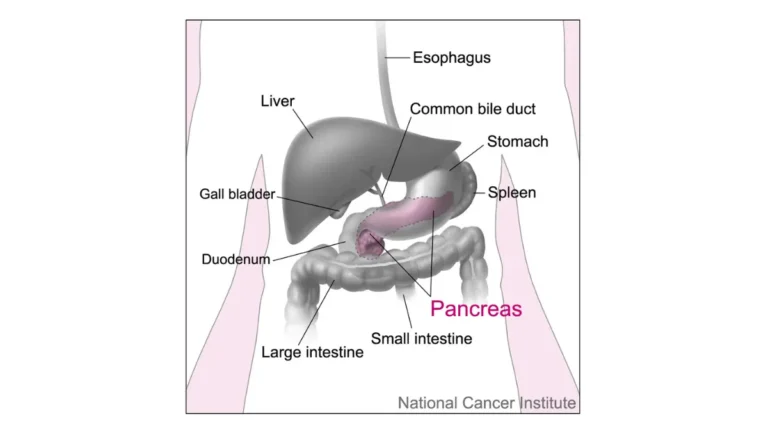
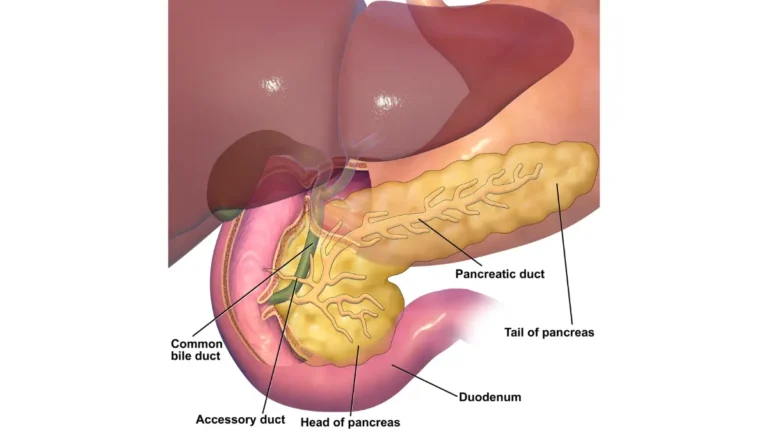
Vague symptoms and a hidden organ
The pancreas sits deep in the abdomen, behind the stomach, where small tumors can’t be seen or felt. Early symptoms — fatigue, upper-abdominal or back discomfort, unexplained weight loss linked to pancreatic cancer, or new digestive changes — overlap with far more common conditions. Sometimes the first real clue is new-onset diabetes that can signal pancreatic cancer or painless yellowing of the skin.
📊 Clinical Data Point: About 51% of pancreatic cancers in the U.S. are diagnosed only after they have spread to distant parts of the body (the metastatic stage). — Source: NCI SEER Cancer Stat Facts (2016–2022 data).
That figure is hard to read, but it also explains why a careful, step-by-step workup — not a single quick test — is what confirms the diagnosis. Learning the early warning signs of pancreatic cancer can help you raise a concern sooner.
Is there a screening test for pancreatic cancer?
For people at average risk, no. The U.S. Preventive Services Task Force recommends against routine screening of adults who have no symptoms and no high-risk history, because no current test reliably catches it early enough to help in that group. People at higher risk — those with certain inherited syndromes or a strong family history — may instead be offered ongoing surveillance with endoscopic ultrasound and/or MRI. A free symptom checker can help you organize what to discuss, though it cannot diagnose anything.
Step 1: Your medical history, physical exam, and first red flags
The diagnostic process almost always begins not with a scan, but with a conversation and a physical exam. This first step points the doctor toward whether further testing is needed.
What your doctor asks and checks
Your doctor will ask about your symptoms, how long they’ve lasted, and risk factors such as smoking and family history. During the exam, they look for jaundice — a yellowing of the skin and the whites of the eyes — and may feel your abdomen, because pancreatic tumors can cause the liver or gallbladder to swell. Because jaundice can be a sign of pancreatic cancer, it’s one of the findings that most often prompts the next round of tests.
When you’ll be referred to a specialist
If the exam or your symptoms are concerning, you’ll likely be referred to a gastroenterologist — a doctor who specializes in the digestive system — for the imaging and procedures that come next. None of these early findings confirm cancer on their own; they signal that the picture needs a closer look.
✅ Patient Action: Before this appointment, write down when each symptom started, any unexplained weight change, and whether anyone in your family has had pancreatic, breast, ovarian, or colon cancer. Bring it to your primary care doctor or gastroenterologist — family history can change which tests are recommended.
Step 2: Imaging tests that look for pancreatic cancer
Imaging is the heart of the workup — it’s how doctors find a suspicious area, judge whether it has spread, and decide whether surgery is possible. According to the American Cancer Society’s overview of pancreatic cancer tests, the main imaging tests, in roughly the order they’re used, are:
- CT scan — often the first and most useful imaging test
- Endoscopic ultrasound (EUS) — a closer, more detailed look that can also take samples
- ERCP or MRCP — used to examine the bile and pancreatic ducts
- PET/CT scan — used mainly to check whether cancer has spread
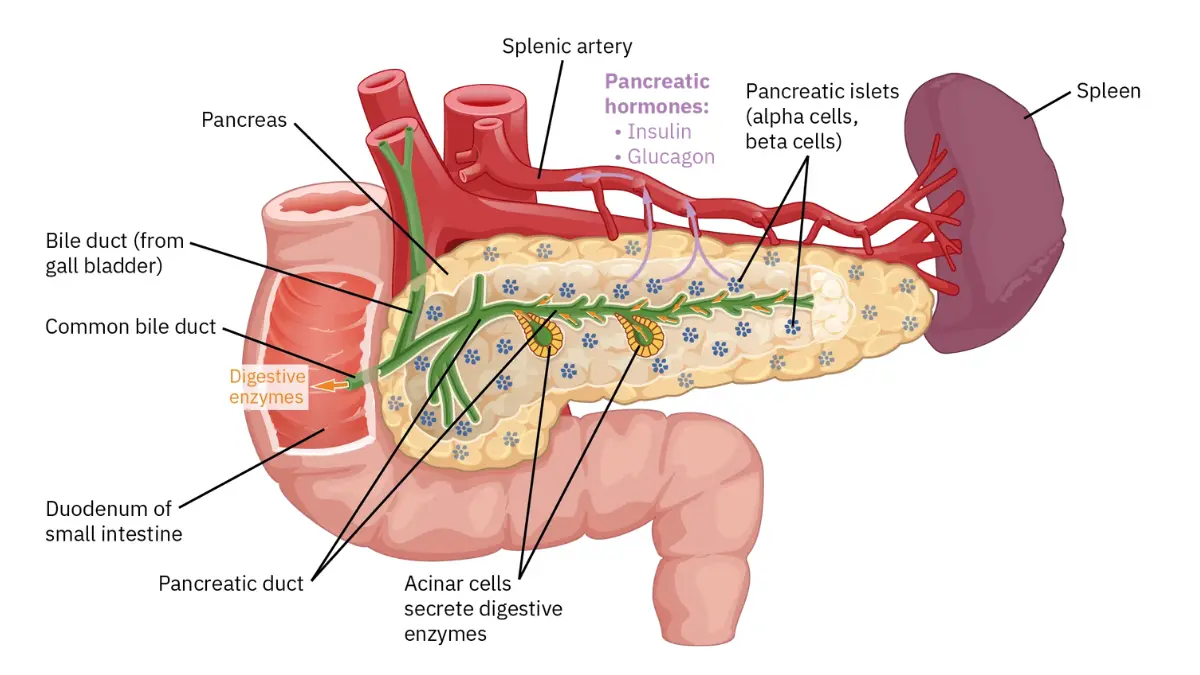
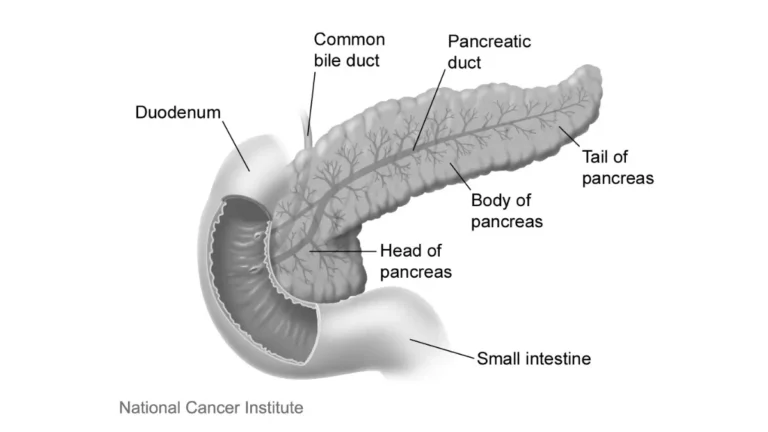
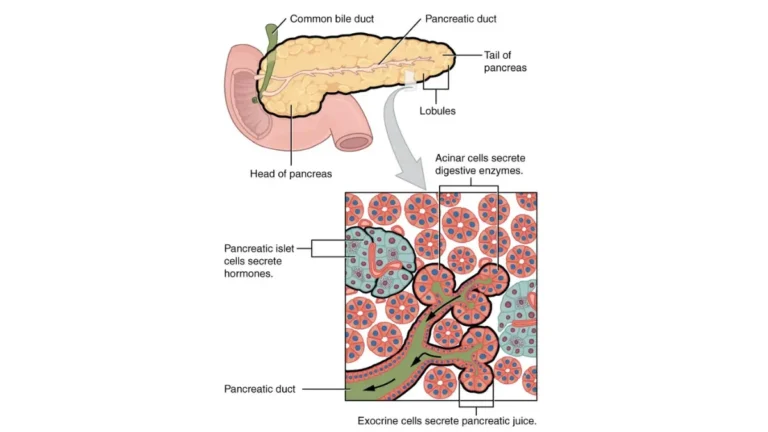
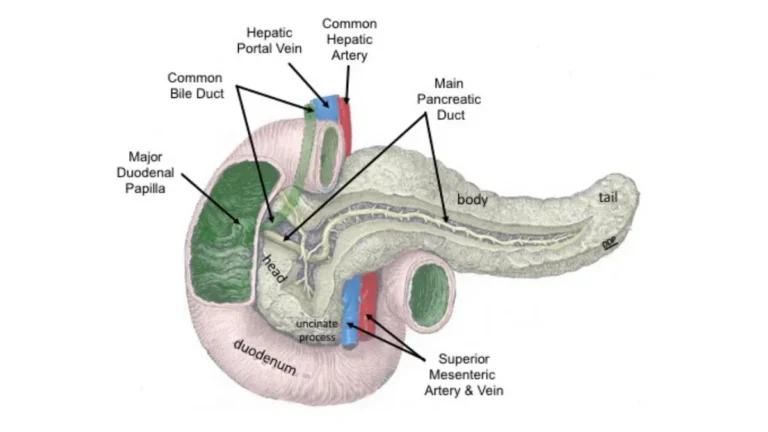
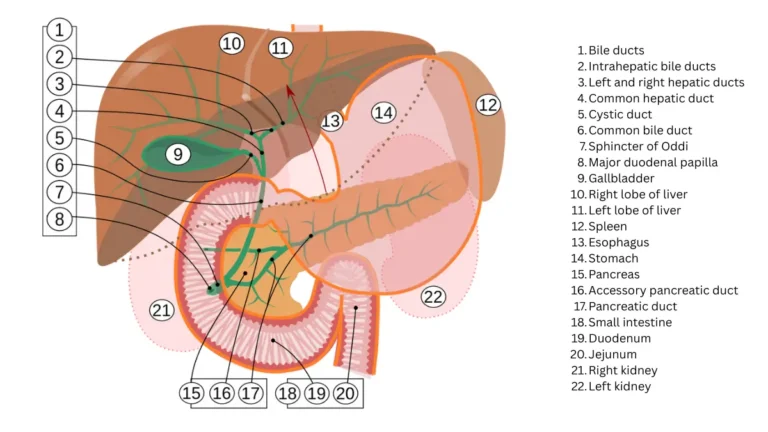
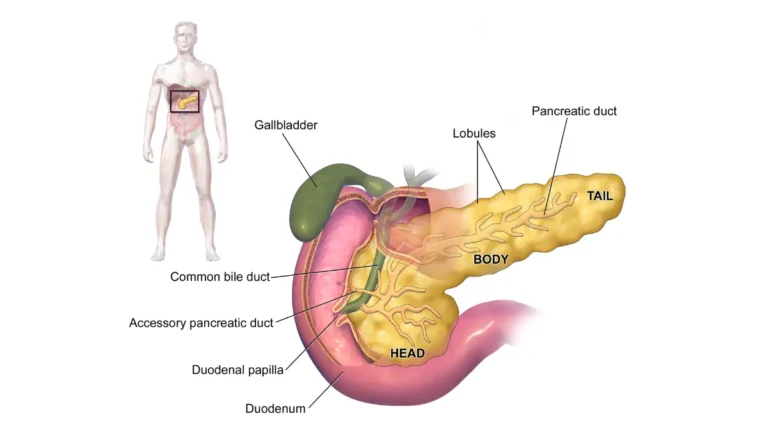
Adapted from NCI Visuals Online, public domain.
CT scan and the pancreatic protocol CT
A CT scan makes detailed cross-sectional images and can show the pancreas, nearby lymph nodes, and distant organs fairly clearly. If pancreatic cancer is suspected, you may get a specialized pancreatic protocol CT (also called a multiphase CT).
🔬 How It Works: In a pancreatic protocol CT, several sets of images are taken at timed intervals after a contrast dye is injected into a vein. The timing captures the pancreas and the blood vessels around it at their clearest, which helps doctors judge whether a tumor can be removed by surgery.
Endoscopic ultrasound (EUS) and ERCP
For a closer look, EUS places a tiny ultrasound probe on the tip of a thin, flexible tube passed into the digestive tract, right next to the pancreas. It’s more accurate than an ordinary abdominal ultrasound and can collect tissue samples in the same procedure. ERCP uses a similar scope to view the ducts on X-ray, brush cells for testing, or place a small tube (stent) to relieve a blocked duct.
MRI, MRCP, and PET/CT
MRI is used less often than CT but can help spot small spots in the liver. MRCP is a non-invasive way to view the ducts without dye, though it cannot take samples. A PET/CT is used mainly to look for spread beyond the pancreas.
✅ Patient Action: If a CT scan is ordered, ask your gastroenterologist or oncologist whether it will be a pancreatic protocol (multiphase) CT — the timed-contrast version designed to show the pancreas and nearby vessels most clearly.
Step 3: Blood tests and the CA 19-9 tumor marker
A frequent assumption is that a blood test can diagnose pancreatic cancer. It can’t — but blood work plays two genuinely useful supporting roles.
What liver tests and bilirubin show
Because jaundice is often one of the first signs, doctors check liver function and bilirubin levels. These help tell whether yellowing comes from disease in the liver itself or from something blocking the flow of bile — such as a tumor pressing on a duct.
🔬 How It Works: Bilirubin is a yellow substance the liver processes and sends out in bile. When a tumor blocks the bile duct, bilirubin backs up into the blood and skin, which is what causes the yellow tint — so the level helps point to where the problem is.
What CA 19-9 can and can’t tell you
The main tumor marker for pancreatic cancer is CA 19-9 (a second one, CEA, is used less often). A tumor marker is a substance that can rise when cancer is present, but it is not a yes-or-no test.
⚠️ Clinical Warning: A normal CA 19-9 result does not rule out pancreatic cancer, and a high result does not confirm it. Levels can be normal in people who have the disease and elevated by non-cancer conditions such as a blocked bile duct — so this single blood test should never be read as a diagnosis either way.
🩺 Physician Note: A common point of confusion is treating CA 19-9 as a screening test. Major cancer organizations describe it instead as a marker used alongside imaging and biopsy — and, in people already diagnosed, as a way to track whether treatment is working over time. Discuss your result with your oncologist in the context of your other tests.
Step 4: Biopsy — the only way to confirm the diagnosis
Imaging and blood tests can strongly suggest pancreatic cancer, but the only way to be certain is to examine actual tumor tissue under a microscope. That procedure is a biopsy.
How a biopsy is taken
There are a few routes, and the choice depends on the tumor’s location and your situation:
- Endoscopic biopsy (EUS-guided): the most common approach — a needle passed through the scope during an endoscopic ultrasound collects a sample directly from the tumor.
- Percutaneous biopsy: a thin needle is guided through the skin using CT or ultrasound images (a fine needle aspiration).
- ERCP brushing: cells are brushed from inside a duct during ERCP.
- Surgical biopsy: now done less often, usually by laparoscopy (“keyhole” surgery) when other methods aren’t suitable.
🔬 How It Works: Under the microscope, a pathologist looks for cancer cells in the sample. If cancer is found, the tissue may also be tested for specific gene changes (such as BRCA or KRAS), which can affect whether certain targeted treatments may help later.
When a biopsy may not come first
Not everyone has a separate biopsy before treatment. If imaging shows a clearly removable (resectable) tumor, a surgeon may proceed directly to surgery, where the diagnosis is confirmed in the lab. But if chemotherapy or radiation is planned before surgery, a biopsy is needed first to be sure.
✅ Patient Action: Ask your surgeon or oncologist two things — whether your imaging suggests the tumor is resectable, and whether you need a biopsy before any treatment is planned. The answers determine whether a biopsy comes first or surgery does.
What your diagnosis means: staging and what comes next
Once a diagnosis is confirmed, the same tests are used to determine the stage — how far the cancer has spread — which is what shapes treatment options.
How diagnosis leads to staging
Imaging shows whether the cancer is confined to the pancreas, has reached nearby lymph nodes, or has spread to distant organs. Doctors also judge whether a tumor is resectable (removable by surgery), borderline, or not currently removable — a distinction that often matters more for planning than the stage number alone.
Survival by stage — and why your outlook is individual
Survival statistics describe large groups, not any one person. They’re worth seeing for context, but they cannot predict your outcome.
| Stage at diagnosis | Share of U.S. cases | 5-year relative survival |
|---|---|---|
| Localized (confined to pancreas) | ~15% | 43.6% |
| Regional (spread to nearby nodes) | ~28% | 17.0% |
| Distant (metastatic) | ~51% | 3.4% |
| All stages combined | — | 13.7% |
Source: NCI SEER Cancer Stat Facts, 2016–2022 data.
These are relative survival figures — they compare people with this diagnosis to the general population, and they reflect people diagnosed years ago, before some of today’s treatments existed. An individual’s outlook depends on stage, resectability, overall health, and how the cancer responds to treatment. For the official statistics, see the NCI’s SEER pancreatic cancer statistics; for treatment-planning information, the NCI’s patient guide to pancreatic cancer treatment is a reliable next read.
✅ Patient Action: Ask your oncologist what stage your cancer is and whether the tumor is resectable, borderline, or has spread — that single answer shapes your options. If you haven’t been offered it, ask about genetic counseling, which can affect both your treatment and your relatives’ risk; a genetic risk assessment tool can help you prepare for that conversation.
Frequently asked questions about pancreatic cancer diagnosis
1. What is the first step in diagnosing pancreatic cancer?
Diagnosis usually begins with a medical history and physical exam. Your doctor asks about symptoms and risk factors and checks for jaundice (yellowing of the skin and eyes) and a swollen liver or gallbladder. Abnormal findings lead to imaging and often a referral to a gastroenterologist. Discuss your specific symptoms with your doctor.
2. What tests are used to diagnose pancreatic cancer?
Doctors use a sequence of tests: imaging (a CT scan, often a pancreatic protocol CT; endoscopic ultrasound; ERCP or MRCP for the ducts; and PET/CT to check for spread), blood tests, and usually a biopsy to confirm the diagnosis. The exact order depends on your situation, which your care team will explain.
3. Can a blood test detect pancreatic cancer?
No single blood test can diagnose pancreatic cancer. The CA 19-9 tumor marker may support a diagnosis and help track treatment, but it isn’t accurate enough to confirm cancer on its own — it can be normal in people who have it and high in people who don’t. Ask your doctor to interpret results in context.
4. What is CA 19-9, and what does a high level mean?
CA 19-9 is a tumor marker — a substance sometimes elevated when cancer is present. A high level can suggest pancreatic cancer but can also rise from non-cancer conditions, so it’s used alongside imaging and biopsy, not alone. In people already diagnosed, it helps monitor treatment. Discuss your level with your oncologist.
5. Is a biopsy always needed to diagnose pancreatic cancer?
A biopsy is the only way to confirm pancreatic cancer for certain, but it isn’t always done first. People with a clearly resectable tumor may go straight to surgery, where the diagnosis is confirmed; if chemotherapy or radiation is planned first, a biopsy is needed beforehand. Your surgeon will advise the right path.
6. What is an endoscopic ultrasound (EUS)?
EUS uses a small ultrasound probe on the tip of an endoscope passed into the digestive tract near the pancreas. It’s more accurate than an abdominal ultrasound, helps with both diagnosis and staging, and can take biopsy samples of a tumor in the same procedure. Your gastroenterologist can explain what to expect.
7. Why is pancreatic cancer so often found late?
Early symptoms are vague and overlap with common conditions, the pancreas sits deep in the abdomen, and there’s no recommended screening test for people at average risk. As a result, about 51% of cases are diagnosed only after the cancer has already spread to distant organs.
8. How accurate is a CT scan for pancreatic cancer?
A CT scan — often a specialized pancreatic protocol (multiphase) CT with contrast — shows the pancreas fairly clearly, can reveal spread to nearby organs or lymph nodes, and helps judge whether surgery is an option. It’s a frequent first imaging step but is paired with other tests to confirm. Your doctor chooses the right scans.
9. What happens after a pancreatic cancer diagnosis?
Your results are used to stage the cancer (localized, regional, or distant) and judge whether the tumor is resectable, which shapes treatment options. Genetic counseling may be offered. From there, you and your oncology team plan treatment. Ask your oncologist about your stage and options.
10. Is there a screening test for pancreatic cancer?
Not for people at average risk — the U.S. Preventive Services Task Force recommends against routine screening of asymptomatic average-risk adults. People at high risk, such as those with certain inherited syndromes or a strong family history, may be offered surveillance with endoscopic ultrasound and/or MRI. Ask your doctor whether you qualify as high risk.
11. What is the survival rate by stage of pancreatic cancer?
Five-year relative survival varies sharply by stage at diagnosis: about 43.6% for localized, 17.0% for regional, and 3.4% for distant disease, with an overall rate of 13.7% (SEER, 2016–2022). These are population averages and can’t predict an individual outcome. Your oncologist can speak to your situation.
Your next step after understanding the diagnosis
A pancreatic cancer diagnosis is rarely a single moment — it’s a sequence: an exam and history, imaging, blood tests, and usually a biopsy, followed by staging. Understanding that sequence won’t make the news easier, but it can make the process feel less bewildering and help you ask sharper questions.
A confirmed diagnosis is also what makes a treatment plan possible. Bring your questions to your oncology team, consider asking about genetic counseling, and lean on the people around you. For the full picture of symptoms, stages, and what follows, return to the complete pancreatic cancer guide.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Internal Medicine (2010); Clinical Pharmacology (2013) Experience: 15 years | Location: San Francisco, California Education: BS Molecular Biology, Caltech (2000); MD/PhD, UCSF School of Medicine (2007);…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.