On This Page – Quick Medical Summary
If you are reading this because the pain is getting harder to manage, you are not alone, and there is real reason for hope. Around three in four people with pancreatic cancer have pain when they are diagnosed, and more than nine in ten in advanced disease — yet for most people that pain can be brought under meaningful control. Effective pancreatic cancer pain management is not a single pill; it is a structured, step-by-step set of options that your care team can escalate as needed.
This guide is written for several people at once. If you are newly diagnosed and bracing for what is ahead, start with why the pain happens. If you are in treatment and your pain is rising, the sections on medication and procedures are for you. If you are a caregiver advocating for someone you love, the palliative-care and warning-sign sections will help you act. Here is the path: why pancreatic cancer hurts, how the team measures it, medications, procedures, palliative care, and the warning signs that mean call now.
ℹ️ Medical Disclaimer: This article is general education, not medical advice, and does not replace care from your own qualified clinicians. Do not start, stop, or change any medication, dose, nerve block, pump, or radiation plan based on this page — pain medicines (including opioids) and procedures carry real risks and must be chosen and managed by your care team. If your pain is severe, uncontrolled, or rapidly worsening, or you notice the warning signs described below, contact your care team or emergency services immediately. Talk with a board-certified oncologist, palliative-care physician, or pain-management specialist before acting. Any product links are clearly labeled and are not clinical recommendations.
Why pancreatic cancer causes such severe pain
The pain of pancreatic cancer is physical, specific, and treatable — not vague or imagined — and understanding its source helps explain why each treatment works.
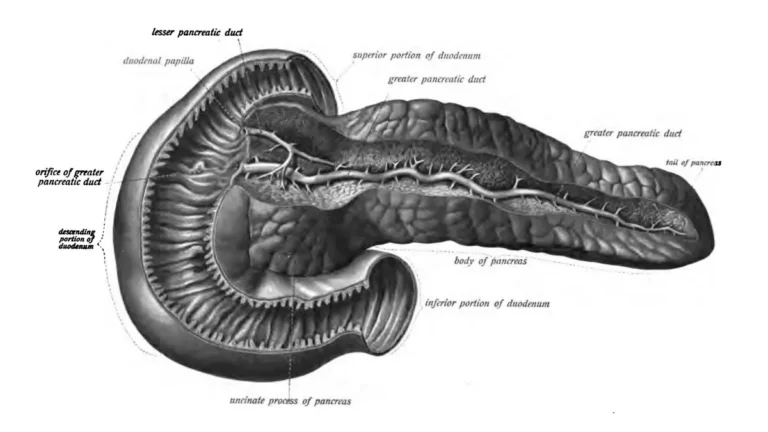
Tumor pressing on nerves: perineural invasion
Pancreatic tumors tend to grow into the nerves around the pancreas, a process called perineural invasion. This neurotropism is a defining feature of the disease and a major reason the pain can be so intense.
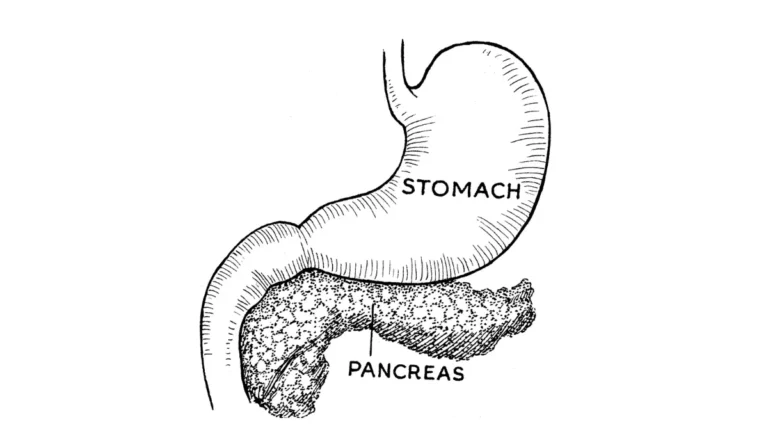
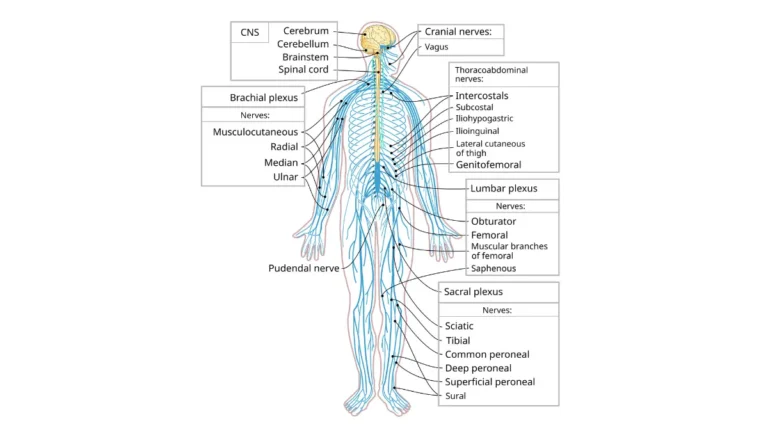
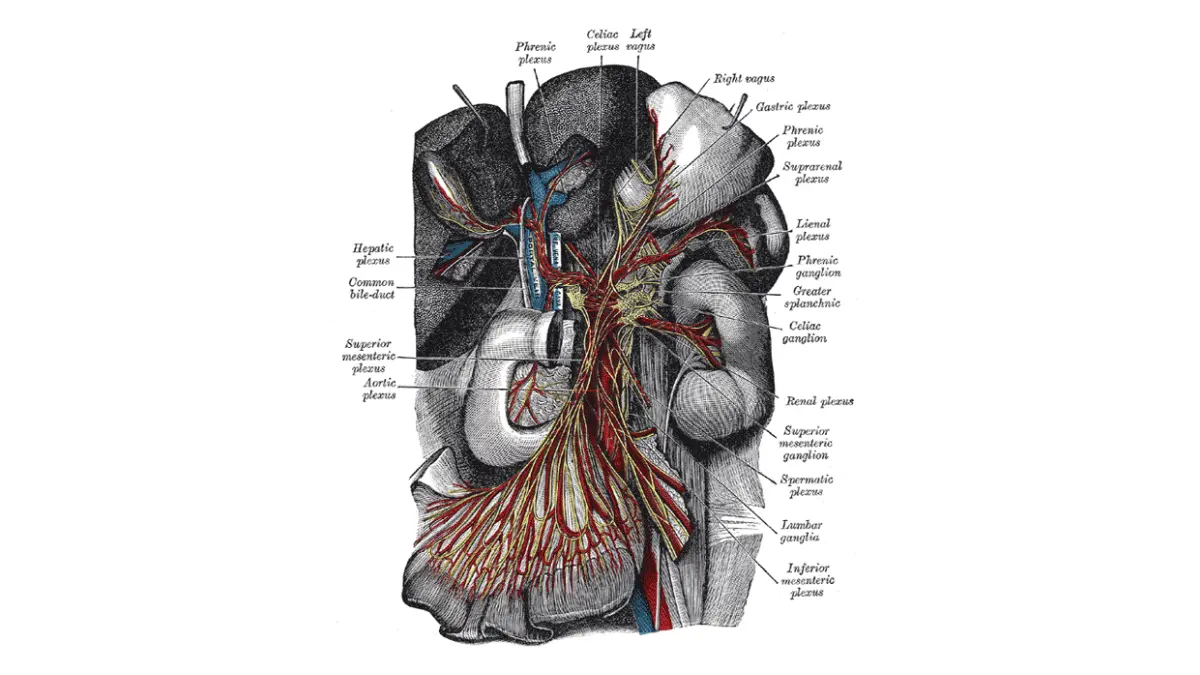
🔬 How It Works: The pancreas sits in a dense web of nerves, including a bundle called the celiac plexus deep in the upper abdomen. When the tumor invades or presses on these nerves, it sends continuous pain signals toward the spinal cord and brain — which is why the pain can be felt deep in the belly and through to the back.
📊 Clinical Data Point: Perineural invasion is found in roughly 70% of pancreatic adenocarcinomas — Source: National Library of Medicine (NIH), peer-reviewed review on pancreas cancer–associated pain management.
Visceral, somatic, and neuropathic pain
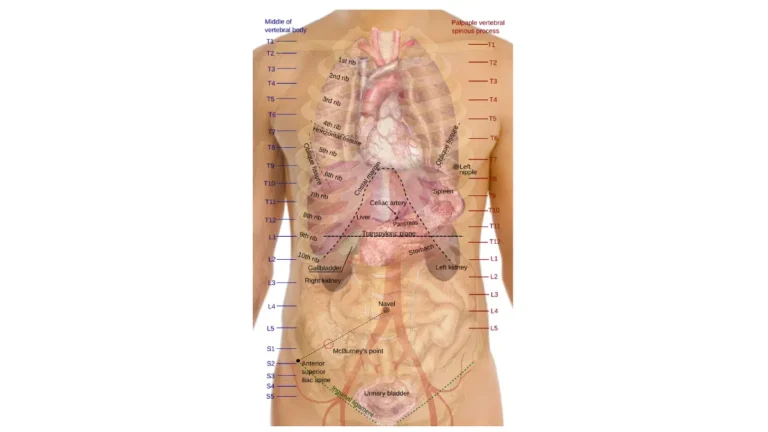
People often feel more than one kind of pain at once. Visceral pain is a deep, dull, hard-to-pinpoint ache from the organ itself; somatic pain is sharper and more localized; and neuropathic pain is a burning or shooting sensation from nerve damage. Because the celiac plexus carries signals from the upper abdomen, this pain frequently radiates to the mid-back, which is why some people first notice it as back pain rather than stomach pain. (More on this in our guide to where pancreatic cancer pain is felt.)
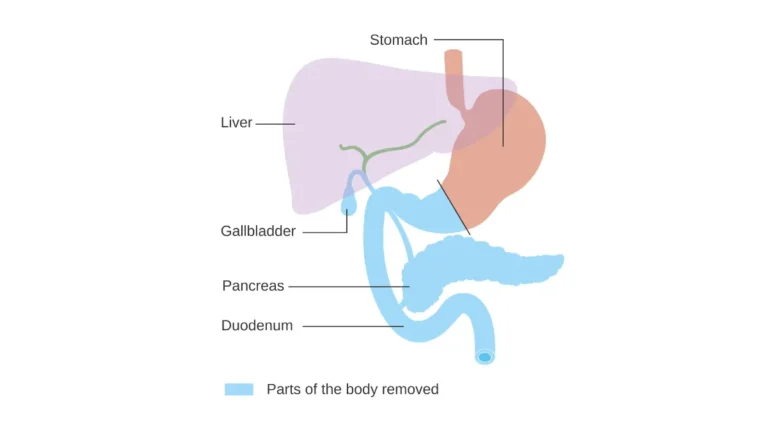
When the tumor blocks the pancreatic duct
A tumor can also obstruct the pancreatic duct or push on nearby organs, adding a cramping, pressure-like pain and sometimes contributing to digestive symptoms. Each of these mechanisms responds to different parts of the treatment plan that follows.
How your care team measures and tracks your pain
Better pain assessment leads directly to better pain relief, and you are the most important source of that information.
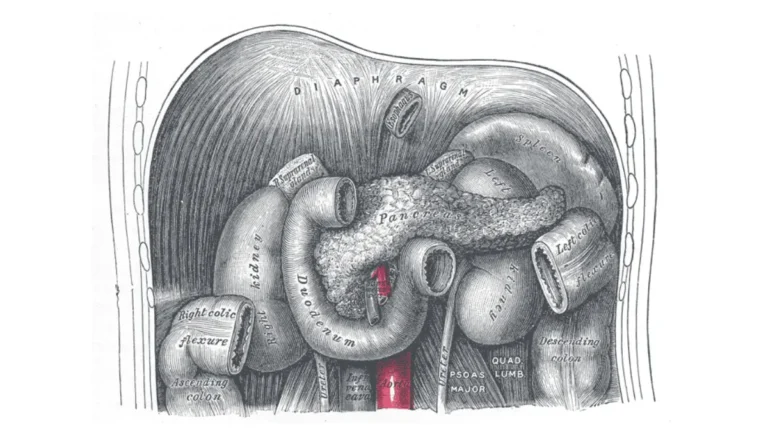
Describing your pain: the 0-to-10 scale and what to note
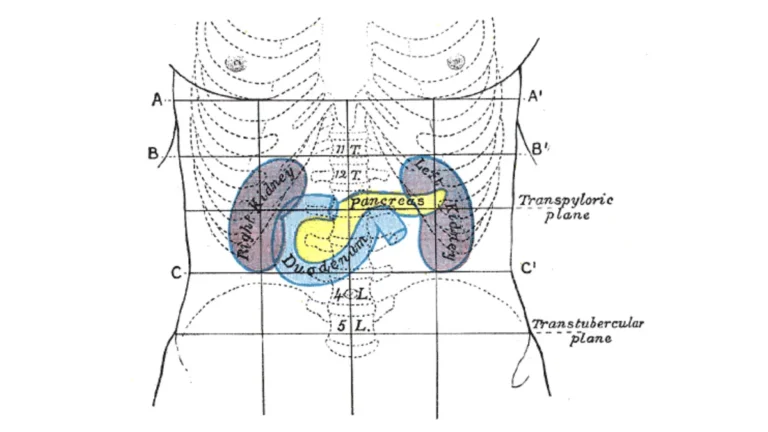
Care teams usually ask you to rate pain on a 0-to-10 scale, where 0 is none and 10 is the worst imaginable. Numbers alone are not enough, so it helps to also describe the location, the quality (dull, sharp, burning), what makes it better or worse, and whether it spreads to your back.
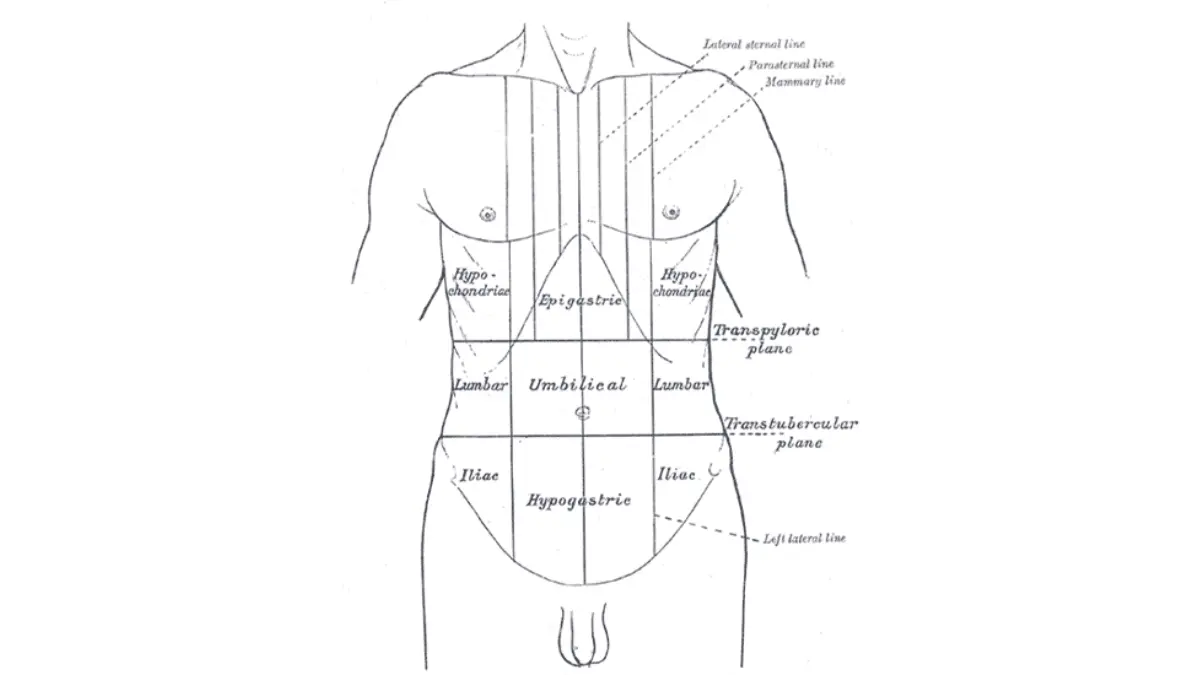
Adapted from Wikimedia Commons Gray1220, licensed under public domain.
🩺 Physician Note: Research on cancer pain shows that using structured, validated pain-assessment tools is associated with higher odds of achieving complete pain relief. In plain terms: the more precisely your team can characterize the pain, the better they can target it.
Why round-the-clock beats waiting for pain to return
For ongoing cancer pain, medicines taken on a regular schedule tend to work better than waiting until pain returns, and can lower the total daily amount needed. Treating pain early, before it escalates, makes it easier to control.
✅ Patient Action: Keep a simple pain journal — time, score, location, and what you took — and bring it to every appointment. Ask directly: “Should a palliative-care or pain-management specialist join my team?”
Medications for pancreatic cancer pain: the WHO ladder
⚠️ High-stakes section — general education only. The specific drugs and doses in your plan are decisions for your care team; nothing here is a dosing instruction.
Medication is the foundation of pancreatic cancer pain control, and most plans follow a framework from the World Health Organization.
The three-step approach: non-opioids, then opioids
The WHO analgesic ladder, introduced in 1986 and updated in the WHO’s 2018 cancer-pain guidelines, organizes pain medication into escalating steps:
- Step 1 — non-opioid analgesics such as acetaminophen and NSAIDs for milder pain.
- Step 2 — weak opioids added for moderate pain.
- Step 3 — strong opioids (for example, morphine) for moderate-to-severe pain.
🔬 How It Works: Each step adds stronger pain control while the team monitors relief and side effects. Modern practice individualizes this rather than rigidly climbing each rung — many people with severe cancer pain move to strong opioids directly, guided by their clinician.
📊 Clinical Data Point: In validation studies, the WHO approach controls cancer pain in roughly 70–80% of patients — Source: World Health Organization cancer-pain guidance and validation literature.
Adjuvant medicines for nerve pain
Because much pancreatic pain is neuropathic, teams often add adjuvant medicines — certain antidepressants, anticonvulsants, or steroids — that target nerve pain through different pathways. Some pain is also a side effect of treatment itself, such as chemotherapy-related nerve pain.
Will I get addicted? What the evidence says
This fear is common and causes real harm when it leads to under-treatment. When opioids are taken as prescribed for cancer pain and monitored by your team, the risk of addiction is low; some people feel foggy or tired for a few days, and that usually eases.
⚠️ Clinical Warning: Never adjust opioid doses on your own. Too little leaves pain uncontrolled; too much can cause dangerous sedation or slowed breathing. Any change goes through your care team.
Managing side effects like constipation
Constipation is nearly universal with opioids and is managed proactively, not after the fact, alongside nausea and drowsiness. Staying hydrated is one practical support — tracking your daily fluids can help — but ask your team about a bowel regimen from day one. For a deeper authoritative overview, see the National Cancer Institute’s guide to cancer pain.
Procedures and radiation that target the pain directly
When medication alone is not enough, procedures can interrupt the pain signal at its source.
Celiac plexus block and neurolysis: what a trial actually found
A celiac plexus block (or neurolysis) places a numbing or nerve-destroying agent near the celiac plexus to interrupt pain signals from the pancreas. It can reduce pain and lower how much opioid medication a person needs — but it is important to know exactly what it does and does not do.
📊 Clinical Data Point: In a double-blind randomized trial of 100 patients with unresectable pancreatic cancer (Mayo Clinic), over the first 6 weeks fewer patients who received a neurolytic celiac plexus block reported moderate-to-severe pain than those on opioids alone — 14% versus 40%. The block improved pain relief but did not significantly improve overall quality of life or survival — Source: Wong et al., JAMA, 2004.
Intrathecal pain pumps and splanchnicectomy
An intrathecal pump delivers pain medicine directly to the fluid around the spinal cord, allowing much lower doses and fewer body-wide side effects. Thoracoscopic splanchnicectomy is a minimally invasive surgery that cuts specific pain-carrying nerves. Both are options when pain is hard to control.
Radiation therapy for pain relief
Targeted radiation therapy can shrink a tumor enough to ease pain even when cure is not the goal, and is a recognized part of pancreatic treatment options.
| Pain option | What it can do | Effect on quality of life / survival | Best for / ask your team |
|---|---|---|---|
| Opioids + adjuvants (WHO ladder) | Controls pain in ~70–80% of patients | Relieves pain; managed for side effects | First-line; “Should we escalate or add an adjuvant?” |
| Celiac plexus block/neurolysis | Cuts moderate-to-severe pain (14% vs 40% in trial), lowers opioid need | Pain relief only — no proven QOL/survival gain | Pain not controlled on medication; “Am I a candidate?” |
| Intrathecal pump | Lower doses, fewer body-wide side effects | Pain/side-effect relief | Refractory pain or intolerable side effects |
| Palliative radiation | Eases tumor-related pain | Symptom relief | Localized pain; “Could radiation help my pain?” |
Verified from Wong et al., JAMA 2004, and WHO cancer-pain guidance.
✅ Patient Action: Ask an interventional pain specialist or radiation oncologist: “Am I a candidate for a celiac plexus block, a pump, or palliative radiation — and what should I realistically expect each to achieve?”
When to start palliative care (earlier than most people think)
One of the most damaging misconceptions in cancer care is that palliative care means giving up — and correcting it can change how you feel for months.
Palliative care is not the same as hospice
Palliative, or supportive, care focuses on relieving symptoms and protecting quality of life, and it runs alongside your cancer treatment at any stage. It is not hospice, which is specific end-of-life care; you can receive palliative care from the day of diagnosis.
What the evidence says about starting early
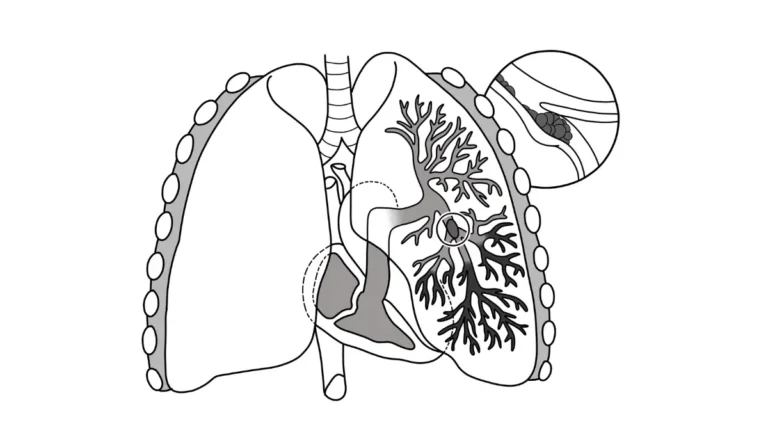
The case for starting early is strong. In a landmark randomized trial, patients with metastatic lung cancer who received early palliative care reported better quality of life and mood — and, notably, lived longer (median 11.6 versus 8.9 months).
📊 Clinical Data Point: Early palliative care improved quality of life, mood, and median survival (11.6 vs 8.9 months) in metastatic non-small-cell lung cancer — Source: Temel et al., NEJM, 2010. This is lung-cancer evidence supporting the principle of starting supportive care early; it is not a pancreatic-cancer survival figure. Pancreatic cancer organizations likewise urge supportive care from diagnosis onward.
Building your pain and supportive-care team
Your team may include palliative-care physicians, pain specialists, nurses, dietitians, and social workers working alongside your oncologist.
✅ Patient Action: Ask your oncologist for a palliative-care referral now, not later. Learn more about supportive (palliative) care from the American Cancer Society.
Warning signs: when pancreatic cancer pain is an emergency
Most pain is managed in the routine course of care, but some changes mean you should reach out right away.
Pain symptoms that mean call your care team now
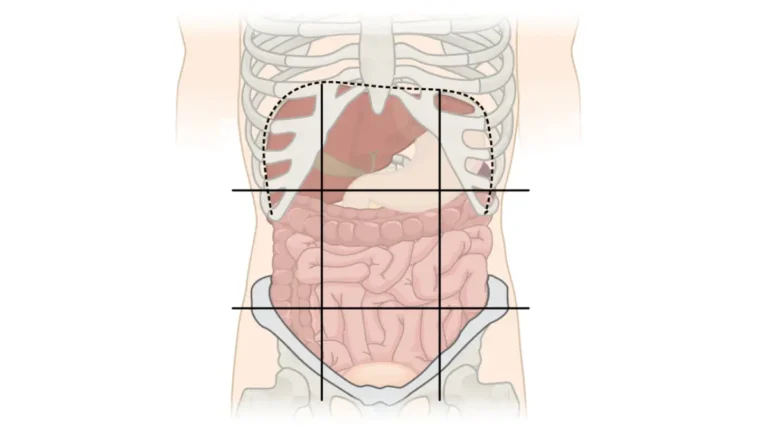
Contact your care team urgently if pain suddenly worsens or stops responding to medicines that were working, if you develop new or severe back pain, or if you notice signs of a bowel blockage such as persistent vomiting, a swollen belly, and no bowel movements or gas (see our guide to pancreatic cancer and bowel obstruction).
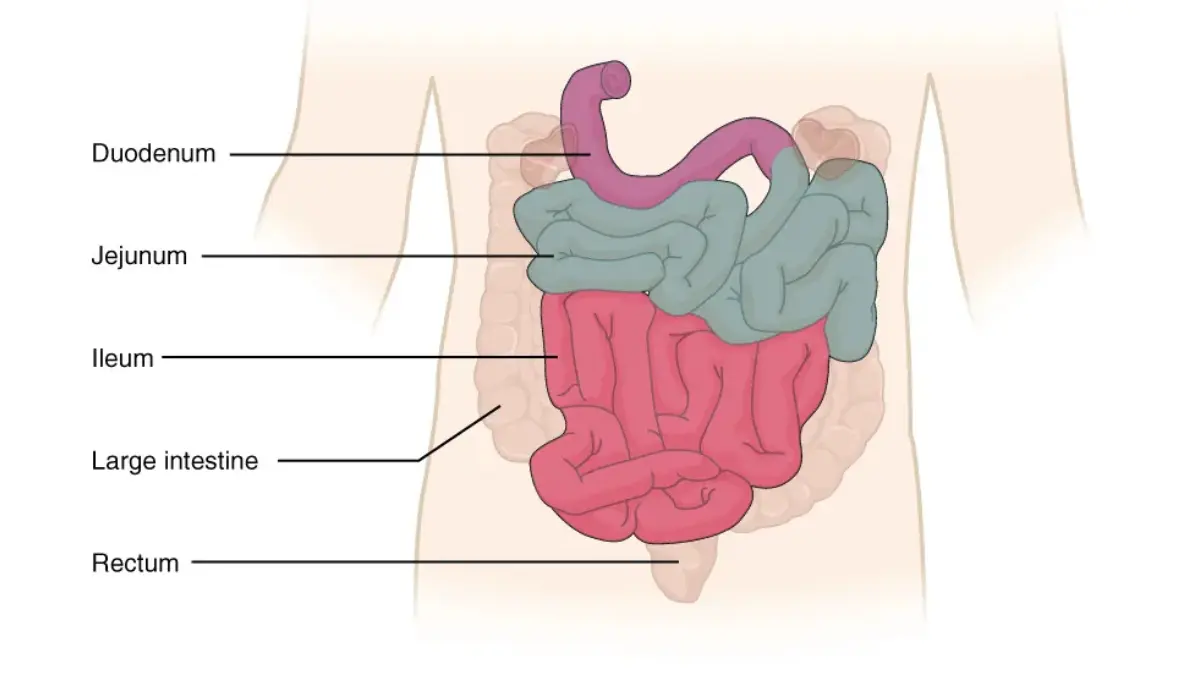
Adapted from OpenStax Anatomy and Physiology 2e Figure 23.18, licensed under CC BY 4.0.
Medication side effects to report urgently
⚠️ Clinical Warning: Seek urgent help for severe drowsiness or confusion, very slow or shallow breathing, or constipation that will not resolve. These can signal an opioid problem that needs prompt adjustment.
Caring for the emotional weight, too
Severe illness carries a heavy emotional load, and distress is a normal response — not a weakness. If you or your caregiver are struggling, tell your care team; counseling and palliative psychosocial support are part of cancer care. In the US, the 988 Suicide & Crisis Lifeline offers free, confidential support any time. For a trusted overview and more resources, see MedlinePlus pancreatic cancer information.
Frequently asked questions about pancreatic cancer pain
1. What is the main cause of pancreatic cancer pain?
Pancreatic cancer pain is driven mainly by the tumor invading or pressing on nearby nerves — perineural invasion, found in about 70% of cases — plus duct obstruction. It can be visceral, somatic, or neuropathic and often radiates to the mid-back. Understanding the cause helps your team target relief.
2. What medications treat pancreatic cancer pain?
Treatment usually follows the WHO analgesic ladder: non-opioids like acetaminophen and NSAIDs, then weak and strong opioids such as morphine for severe pain, plus adjuvants like certain antidepressants or anticonvulsants for nerve pain. Your care team chooses and adjusts the specifics.
3. Will I get addicted to opioids for cancer pain?
When opioids are taken as prescribed for cancer pain and monitored by your team, the risk of addiction is low. Some people feel foggy or tired for a few days, which usually eases. Never adjust doses yourself; discuss any concerns with your care team.
4. What is a celiac plexus block and does it help?
A celiac plexus block places a numbing or nerve-destroying agent near the nerves behind the pancreas to interrupt pain signals. In a randomized trial it reduced moderate-to-severe pancreatic cancer pain (14% versus 40% on medication alone) and lowered opioid needs. Ask a pain specialist whether you are a candidate.
5. Does a celiac plexus block help you live longer?
No. The randomized trial that showed better pain control with a celiac plexus block found it did not significantly improve overall quality of life or survival. It is a tool for reducing pain and opioid side effects, not for extending life. Your care team can explain its role for you.
6. Can radiation therapy reduce pancreatic cancer pain?
Yes. Targeted radiation can shrink a tumor enough to ease pain even when the goal is not to cure the cancer. It is a recognized part of palliative pancreatic cancer pain management for localized pain. Ask your radiation oncologist whether radiation could help your specific pain.
7. What is an intrathecal pain pump?
An intrathecal pump delivers pain medicine directly into the fluid around the spinal cord, allowing much lower doses and fewer body-wide side effects. It is typically considered when pain is hard to control or medication side effects are intolerable. Your pain-management specialist can assess whether it fits your situation.
8. When should palliative care start?
Early — ideally from diagnosis. Palliative care relieves symptoms and protects quality of life alongside cancer treatment, and it is not the same as hospice. Evidence in other cancers links early palliative care to better quality of life. Ask your oncologist for a referral now.
9. How do I describe my pain to my care team?
Use the 0-to-10 scale, and add the location, quality (dull, sharp, burning), what makes it better or worse, and whether it spreads to your back. Keeping a pain journal and bringing it to appointments helps your team target relief more precisely.
10. What pancreatic cancer pain symptoms are an emergency?
Call your care team urgently if pain suddenly worsens or stops responding to medication, if you have severe new back pain, or signs of bowel obstruction (persistent vomiting, swollen belly, no bowel movements). Also report severe drowsiness, confusion, or very slow breathing right away.
11. Can pancreatic cancer pain be completely relieved?
For most people, pain can be brought under meaningful control — the WHO approach helps roughly 70–80% of patients, and procedures, radiation, and palliative care add further options. Complete relief is not guaranteed for everyone, but most people achieve real improvement. Your care team can build a plan for you.
Taking the next step on pain control
Severe pancreatic cancer pain is one of the hardest parts of this disease, but it is also one of the most treatable — through a structured, escalating set of options from medication to nerve blocks to early palliative care. The single most useful step you can take is to ask your care team, today, for a palliative-care or pain-management referral, and to bring a pain journal so your team can see the full picture. For the broader context of diagnosis and treatment, return to our pillar guide on understanding pancreatic cancer from first signs to treatment. You do not have to manage this pain alone, and you do not have to accept it as inevitable.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.