On This Page – Quick Medical Summary
A blood test showing low sodium can be unsettling, especially when the number arrives with no explanation. The medical term is hyponatremia, and it means your blood sodium has fallen below the normal range. How much it matters comes down to two things: how low the level is, and how fast it dropped.
Where you are right now shapes what to read first. If you or someone with you has a seizure, has fainted, or is severely confused, treat it as an emergency and get medical help immediately — then return to this. If you just received a result and feel well, the sections on causes and severity will help most. If you’re a caregiver noticing new confusion or unsteadiness in an older adult, the symptoms section is written with you in mind.
One reframe makes the rest of this easier to follow: low sodium is usually a problem of too much water relative to sodium, not of eating too little salt. Understanding your comprehensive metabolic panel (CMP) results as a whole helps put this single number in context.
ℹ️ Medical Disclaimer: This article is general health education — not a diagnosis, treatment plan, or medication guidance. Low sodium has many possible causes, and the right response depends on the underlying reason and your overall health, so decisions about testing, medications, fluids, and follow-up should be made with a licensed clinician who knows your history. If you have severe symptoms such as a seizure, fainting, or marked confusion, seek emergency care. For diagnosis and treatment, consult your physician or a board-certified nephrologist.
What sodium does and why low sodium is a problem
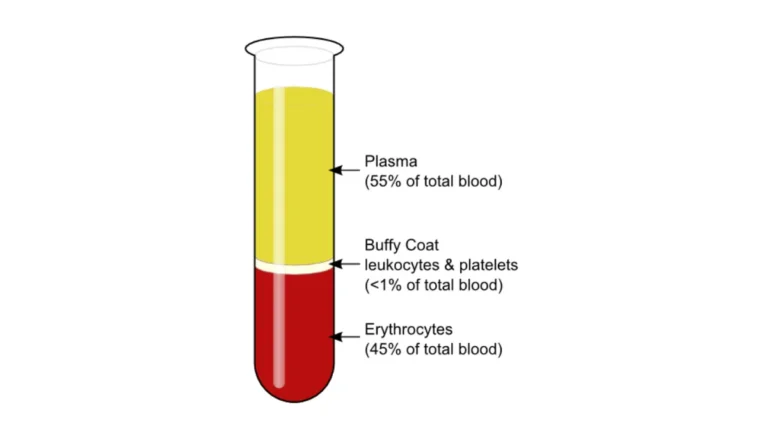
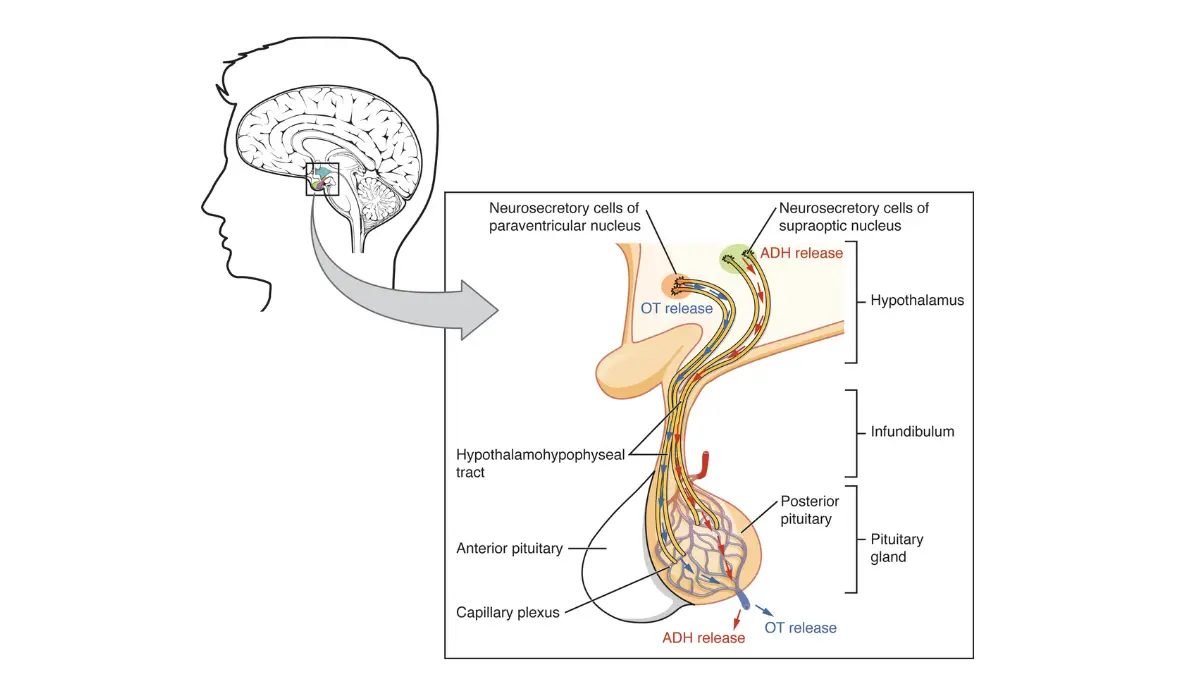
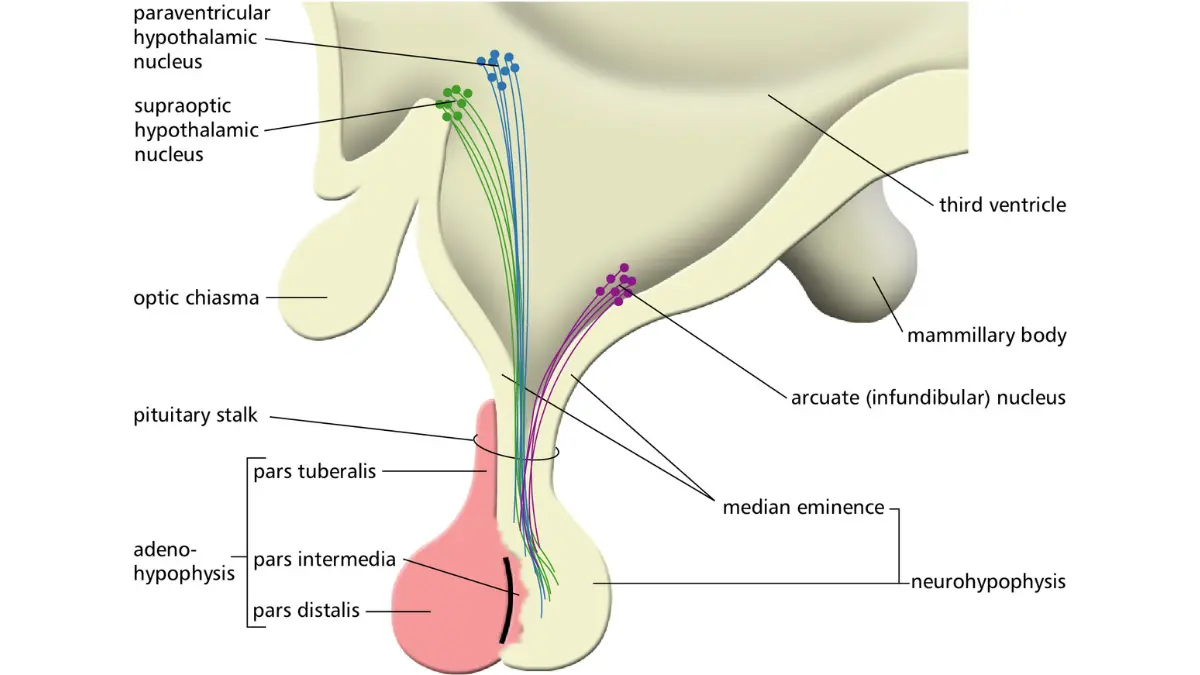
Sodium is an electrolyte — a mineral that carries an electrical charge and runs some of the body’s most basic functions. It regulates the balance of fluid inside and outside your cells, and it helps nerves fire and muscles contract. Your kidneys, together with a hormone called antidiuretic hormone (ADH, or vasopressin), keep that balance within a narrow range.
How your body keeps sodium balanced
Sodium and water move together. When you take in more water than you need, healthy kidneys simply excrete the surplus. When something disrupts that system — a hormone signal, a medication, or an organ that isn’t clearing fluid well — water builds up and dilutes the sodium already in your blood. Because sodium travels with the other electrolytes, it’s often read alongside potassium and chloride; here’s how the electrolytes work together on your panel.
Why brain cells are most affected
🔬 How It Works: When blood sodium falls, water shifts out of the bloodstream into your cells and makes them swell. Most tissues tolerate some swelling, but the brain sits inside a rigid skull with almost no room to expand. That pressure is what drives the headache, confusion, and — in severe cases — the dangerous symptoms of low sodium.
What causes low sodium?
Low sodium causes fall into a few recognizable patterns, and nearly all of them come down to the balance between water and sodium. Clinicians usually sort them by how much fluid is in the body: too much water diluting normal sodium, the body holding onto water it should release, or sodium being lost along with fluid.
The most common contributors include:
- Too much fluid. Drinking very large volumes of water quickly — sometimes during endurance events — can outpace the kidneys and dilute blood sodium.
- Medications. Thiazide diuretics such as hydrochlorothiazide are a frequent cause, and some antidepressants (SSRIs) and other drugs can lower sodium as well.
- Heart, liver, and kidney disease. These conditions cause the body to retain fluid, which dilutes sodium; problems clearing fluid often show up alongside abnormal kidney function markers.
- Vomiting or diarrhea. Heavy fluid loss carries sodium out with it.
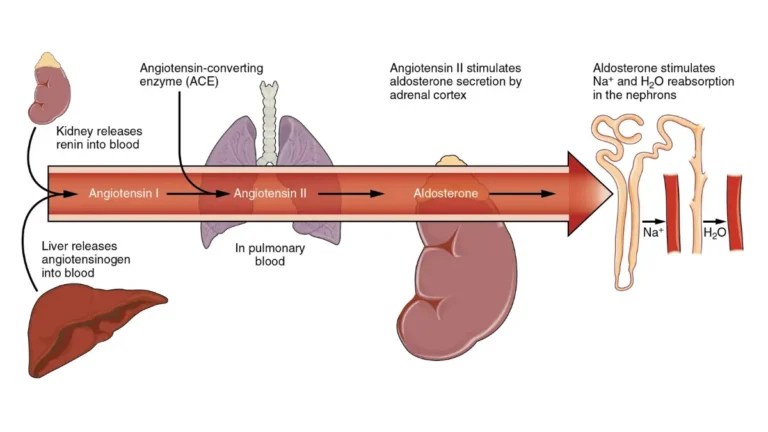
- SIADH. In the syndrome of inappropriate antidiuretic hormone, the body releases too much ADH and holds onto water; it can be triggered by some cancers, lung and brain conditions, and certain medications.
- Very high blood sugar. Markedly elevated glucose can pull water into the blood and lower the measured sodium, so clinicians use a corrected value — one reason a very high blood sugar result is read alongside sodium.
🩺 Physician Note: A frequent point of confusion is assuming low sodium means you need more salt. In most cases it reflects a water imbalance, and adding salt on your own can be ineffective or unsafe. Pinning down the real cause usually takes a physical exam plus blood and urine tests.
If over-hydration is a concern for you, it can help to estimate your daily water needs rather than guess. For a plain-language patient reference, the low blood sodium overview from MedlinePlus is a reliable starting point.
How low is dangerous? Mild, moderate, and severe
A normal blood sodium level runs about 135 to 145 mEq/L. Anything below 135 is hyponatremia, and risk generally rises as the number falls — but the speed of the drop matters as much as the number itself.
One classification used in clinical practice sorts hyponatremia by severity:
| Category | Sodium level (mEq/L) | What it generally means |
|---|---|---|
| Normal | 135–145 | Reference range |
| Mild | 130–134 | Often no symptoms |
| Moderate | 125–129 | Symptoms may appear |
| Severe | Below 125 | Higher risk; can be an emergency when symptoms are present |
Source note: severity bands based on a clinical review in American Family Physician (2023). Some clinicians define “severe” as below 120 mEq/L, and laboratories vary slightly — for example, MedlinePlus lists 136–144 as normal. Compare against your lab’s own CMP reference ranges, since your result is interpreted in context.
Why speed matters: acute vs chronic
📊 Clinical Data Point: Hyponatremia that develops in under 48 hours (acute) is considered more dangerous than a slow decline over days or weeks (chronic) — Source: American Family Physician, 2023. In chronic cases, brain cells adapt over time and swell less, which is why two people with the same number can face very different risk.
Symptoms of low sodium and when to get help
Many people with mild or slowly developing low sodium have no symptoms at all. When symptoms do appear, they tend to track with how low the level is and how quickly it fell.
Mild to moderate symptoms
Early symptoms of low sodium are easy to mistake for something else:
- Nausea or vomiting
- Headache
- Fatigue, weakness, or low energy
- Trouble concentrating or mild confusion
- Muscle cramps or unsteadiness
Emergency warning signs (seek care now)
⚠️ Clinical Warning: Some symptoms signal that the brain is under dangerous pressure and need emergency care without delay. Call 911 or go to the nearest emergency room for a seizure, fainting or loss of consciousness, severe or worsening confusion or agitation, or an inability to stay awake. These are not symptoms to wait out or manage at home.
For milder symptoms after a low result, the safer path is prompt evaluation rather than self-treatment. A general symptom checker can help you organize what you’re noticing, but it is not a substitute for emergency care when red-flag signs are present.
✅ Patient Action: If you have new or worsening symptoms, contact your primary care clinician or a nephrologist and tell them your sodium level, when the symptoms started, and every medication you take — especially any water pill (diuretic) or antidepressant.
How doctors diagnose and treat low sodium
Low sodium is usually first spotted on a routine blood panel, then investigated to find the cause before it’s treated.
Finding the cause
Sodium is measured as part of a basic or comprehensive metabolic panel. To work out why it’s low, a clinician may add blood and urine osmolality plus a urine sodium test, which help separate a dilution problem from a sodium-loss problem. A physical exam and your medication list matter as much as the numbers themselves. You can read more about what a sodium blood test measures and where it fits in a panel.
How it’s treated (and why correction is slow)
Treatment depends entirely on the cause and on how much fluid your body is holding. Approaches range from treating an underlying condition and adjusting a medication, to fluid restriction (often used for SIADH), to intravenous fluids given in a hospital for severe or symptomatic cases.
⚠️ Clinical Warning: Raising sodium too quickly can cause a rare but serious brain injury called osmotic demyelination syndrome. That is why low sodium — particularly when it has been low for a while — is corrected slowly and monitored by clinicians, and why you should never try to raise it yourself with salt tablets or by changing how much you drink.
Who’s most at risk, and one important warning
Certain groups are more prone to low sodium, and knowing whether you’re one of them helps you and your clinician stay ahead of it.
Who is most at risk
Higher-risk groups include:
- Older adults, who are more sensitive to fluid shifts and to medications
- People taking thiazide diuretics or SSRIs
- Endurance athletes who drink large volumes of water during long events
- People living with heart failure, liver disease, or kidney disease
The overcorrection warning
🩺 Physician Note: Low sodium is corrected carefully in a medical setting because the risk of osmotic demyelination syndrome is higher in people with long-standing low sodium, heavy alcohol use, malnutrition, or liver disease. This is precisely why self-treating low sodium is unsafe — the correction itself has to be paced and monitored.
✅ Patient Action: If you’re in a higher-risk group, ask your clinician whether your medications or fluid habits should be monitored, and how often your sodium level should be rechecked.
Low sodium: frequently asked questions
1. What causes low sodium levels?
Low sodium, or hyponatremia, usually stems from an imbalance between water and sodium rather than from low salt intake. Common causes include drinking too much fluid, diuretics and some antidepressants, heart, liver, or kidney disease, vomiting or diarrhea, SIADH, and very high blood sugar. A clinician pinpoints the specific cause with a physical exam and blood and urine tests.
2. What is a dangerously low sodium level?
A normal blood sodium level is about 135 to 145 mEq/L, and hyponatremia is anything below 135. Levels below 125 mEq/L are generally considered severe, and that combined with symptoms can be a medical emergency. How dangerous a number is also depends on how quickly it fell. Ask your clinician what your specific result means for you.
3. What are the symptoms of low sodium?
Many people with mild low sodium have no symptoms. When present, symptoms of low sodium include nausea, headache, fatigue, muscle cramps, unsteadiness, and trouble concentrating; worsening cases bring confusion, drowsiness, seizures, or loss of consciousness. Because these overlap with many conditions, a blood test confirms the cause — check with your clinician if symptoms appear.
4. When is low sodium an emergency?
Low sodium becomes an emergency when it causes a seizure, fainting, severe or worsening confusion, or an inability to stay awake — signs the brain is under dangerous pressure. If any of these appear, call 911 or go to the emergency room rather than waiting. Milder symptoms still warrant prompt evaluation by your clinician.
5. Can drinking too much water cause low sodium?
Yes. Drinking very large amounts of water in a short time can overwhelm the kidneys’ ability to excrete it and dilute blood sodium, which is one reason endurance athletes are cautioned against over-hydrating during long events. In most cases of low sodium, the problem is this water balance rather than how much salt is in your diet.
6. Does low sodium mean I should eat more salt?
Usually not. Because low sodium most often reflects too much water rather than too little salt, adding salt on your own generally doesn’t fix the problem and can be unsafe. Treatment targets the underlying cause — sometimes fluid restriction, a medication change, or hospital care. Don’t change your salt or fluid intake for low sodium without guidance from your clinician.
7. What medications cause low sodium?
Several medications can lower sodium. Thiazide diuretics such as hydrochlorothiazide are among the most common, and some antidepressants (SSRIs) and other drugs can contribute, often by triggering SIADH. If you take one of these and your sodium is low, don’t stop the medication on your own — ask your prescriber whether it should be adjusted.
8. Is low sodium the same as SIADH?
No. SIADH — the syndrome of inappropriate antidiuretic hormone — is one cause of low sodium, not a synonym for it. In SIADH, the body releases too much antidiuretic hormone and holds onto water, diluting sodium. Low sodium has many other causes too, including diuretics, heart, liver, and kidney disease, and fluid loss from vomiting or diarrhea.
9. How is low sodium treated?
Treatment for low sodium depends on the cause and on how much fluid the body is holding. It may involve treating an underlying condition, adjusting a medication, restricting fluids, or intravenous fluids in a hospital for severe cases. Sodium is raised slowly to avoid a rare brain complication. Your clinician will choose the approach based on your specific situation.
10. Can very high blood sugar cause a false low sodium reading?
Yes. Very high blood sugar can pull water into the bloodstream and lower the measured sodium, a dilutional effect. Clinicians account for it by calculating a corrected sodium value from your glucose level. This is one reason a low sodium result is read alongside the rest of your metabolic panel rather than on its own.
11. Who is most at risk for low sodium?
Higher-risk groups include older adults, people taking thiazide diuretics or SSRIs, endurance athletes who over-hydrate, and people with heart failure, liver disease, or kidney disease. Long-standing low sodium, heavy alcohol use, and malnutrition also raise the risk of complications from treatment. If you’re in one of these groups, ask your clinician about monitoring.
The bottom line on a low sodium result
A low sodium result is common, and for many people — especially when it’s mild or developed slowly — it’s manageable once the cause is found. The two things that determine how serious it is are how low the number is and how fast it fell, which is why the same value can mean different things for different people. Severe symptoms like a seizure, fainting, or marked confusion are always an emergency. For anything milder, the safest next step is to bring your result to your clinician to confirm the cause and plan follow-up — and it helps to make sense of your full panel before that visit.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.