Introduction – The AI Revolution in Diabetes Care
How AI is Transforming Diabetes Management: Future of Personalized Care
AI-powered diabetes management is achieving what seemed impossible just five years ago: a 34-year-old woman with type 2 diabetes reduced her HbA1c from 9.2% to 7.1% in just 12 weeks using continuous glucose monitoring integrated with machine learning algorithms, eliminated one medication, and lost 18 pounds—all without a single in-person doctor visit. This breakthrough represents the future of personalized diabetes care, where artificial intelligence transforms how 38.4 million Americans living with diabetes manage their condition daily.
The global diabetes crisis demands revolutionary solutions, not incremental improvements. According to the National Institute of Diabetes and Digestive and Kidney Diseases, 29.7 million Americans have diagnosed diabetes, while another 8.7 million remain undiagnosed—representing 22.8% of people living with the condition without knowing it. Worldwide projections paint an even starker picture: 570.9 million people will have diabetes by 2025, with 1.59 million deaths annually if current trends continue without effective interventions.
Traditional diabetes management relies on periodic check-ins, retrospective blood sugar readings, and generalized treatment protocols that fail to account for individual metabolic variations. Patients using conventional blood sugar monitoring methods capture only 4-7 glucose readings per day, missing critical patterns that occur during sleep, exercise, and stress. This fragmented approach leaves healthcare providers making treatment decisions based on incomplete data, often reacting to complications rather than preventing them.
Artificial intelligence changes this paradigm entirely. Machine learning algorithms analyze continuous streams of glucose data—collected every 1-5 minutes through sensors—alongside diet, activity, sleep patterns, and medication adherence to predict blood sugar fluctuations up to 60 minutes before they occur.
Deep learning models trained on millions of patient data points can now identify individuals at risk for diabetes with up to 96% accuracy, sometimes years before traditional diagnostic criteria would detect the disease. For those already diagnosed, AI-enabled platforms have demonstrated persistent 1.1% to 2.1% HbA1c reductions—improvements that translate to significantly lower risks of blindness, kidney failure, and cardiovascular complications.
This article explores how artificial intelligence is revolutionizing diabetes care across five critical dimensions: predictive monitoring technologies that anticipate glucose changes before they become dangerous, personalized treatment optimization that tailors medication and lifestyle interventions to individual metabolic signatures, complication prevention systems that detect retinopathy and neuropathy at reversible stages, patient engagement tools that provide 24/7 coaching without human provider burnout, and equitable access innovations that could finally bring expert-level diabetes management to underserved populations.
Whether you’re managing your own genetic risk for diabetes, supporting a family member, or exploring emerging treatments, understanding AI’s role in personalized care is essential for navigating the future of diabetes management.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult with your healthcare provider before making changes to your diabetes management plan.
AI Technologies Revolutionizing Diabetes Care
AI Technologies Revolutionizing Diabetes Care
Artificial intelligence has transformed diabetes management from reactive treatment to proactive prevention through four breakthrough technology categories that address the disease’s most challenging aspects: unpredictable glucose fluctuations, medication dosing complexity, dietary uncertainty, and complication detection delays.
Continuous Glucose Monitoring (CGM) with Predictive Algorithms
Traditional finger-stick blood sugar testing provides only snapshots—capturing perhaps 4-7 moments per day while missing the other 99.5% of metabolic activity. Modern continuous glucose monitoring systems integrated with machine learning algorithms collect glucose readings every 1-5 minutes, generating 288-864 data points daily that reveal patterns invisible to conventional testing. These AI-powered systems don’t just record historical data; they predict future glucose levels with remarkable accuracy: 99.5% at 30 minutes, 98.6% at one hour, and 91.9% at four hours for hypoglycemia prediction.

The clinical impact extends far beyond data collection. Hypoglycemia prediction algorithms analyzing continuous streams of glucose data alongside heart rate variability can forecast dangerous blood sugar drops with 79% sensitivity and provide 22-minute advance warnings—sufficient time for patients to consume fast-acting carbohydrates before symptoms begin. For those managing their diabetes through calorie deficit strategies, these predictive alerts prevent the dangerous intersection of reduced food intake and insulin-induced hypoglycemia.
Research published by the National Institutes of Health demonstrates that automated insulin delivery systems using CGM data achieve 68.7% time-in-range (glucose between 70-180 mg/dL) and an impressive 95.4% time in the tighter 70-144 mg/dL range during nighttime hours when patients cannot monitor symptoms.
Comparison: Traditional SMBG vs. AI-Powered CGM
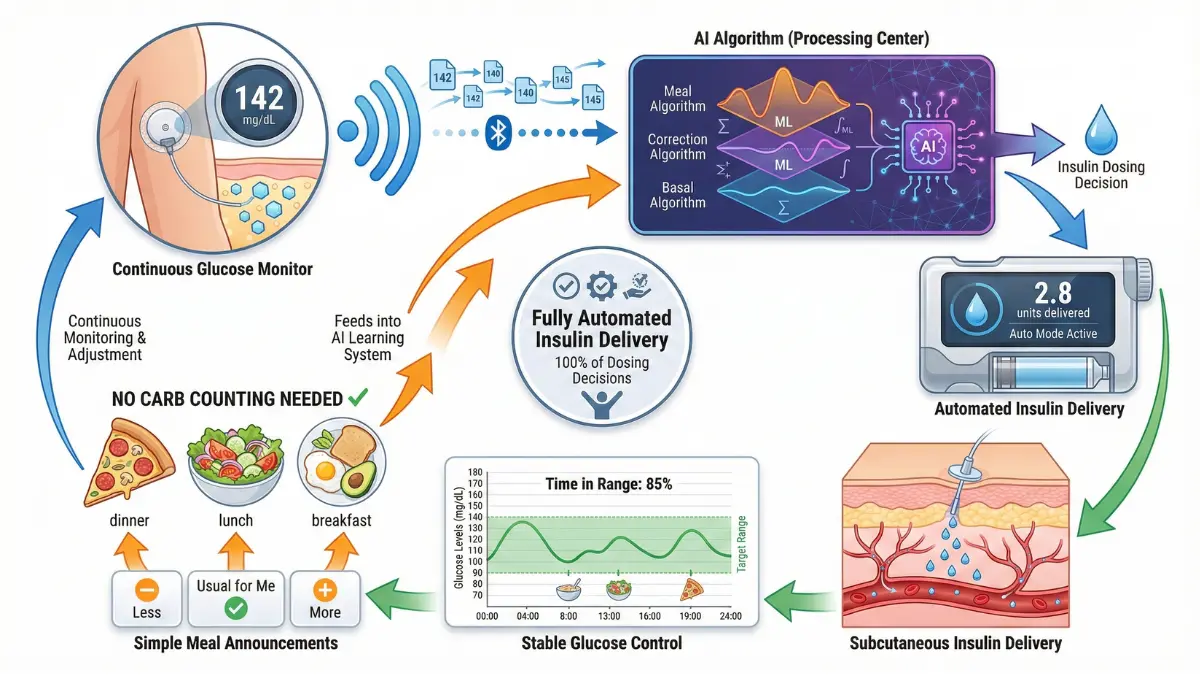
Automated Insulin Delivery Systems (AID)
The iLet Bionic Pancreas, cleared by the FDA in May 2023 for individuals aged 6 and older with type 1 diabetes, represents a paradigm shift in automated insulin management. Unlike conventional insulin pumps requiring patients to count carbohydrates, calculate insulin-to-carb ratios, and manually adjust for exercise or stress, the iLet requires only a user’s body weight for initialization—the autonomous algorithm handles everything else through continuous learning. Patients simply classify meals as “small,” “medium,” or “large,” and the system’s machine learning model adapts insulin delivery based on real-time glucose responses, prior meal patterns, physical activity levels, and individual insulin sensitivity variations.
Clinical trial data on 440 participants demonstrated that the iLet met all primary endpoints for improved glycemic control compared to standard care, with real-world effectiveness studies showing sustained benefits beyond controlled research settings. For adults with type 2 diabetes using fully automated closed-loop systems, the technology improved time-in-target-range by 35 percentage points—translating to an additional 8 hours per day spent in healthy glucose ranges without hypoglycemia risk.
Hybrid closed-loop systems achieve 69% time-in-range, while fully closed-loop configurations (requiring no meal announcements) achieve 66% time-in-range with average HbA1c levels between 6.8-6.9%. Individuals using these automated systems can optimize their BMR-based caloric needs without the constant mental burden of manual insulin dose calculations, reducing diabetes distress by 73% according to FDA-reviewed clinical data.
Key Takeaway: Automated insulin delivery systems reduce daily diabetes management decision burden by 73% while achieving HbA1c levels below 7.0% in most users—outcomes that traditionally required intensive specialist supervision.
AI-Powered Dietary Management
Food represents diabetes management’s most complex variable, with identical meals producing drastically different glucose responses between individuals based on microbiome composition, insulin resistance patterns, stress hormones, circadian rhythms, and dozens of other factors. Machine learning-based dietary recommendation systems solve this personalization challenge by creating “digital twin” metabolic models for each patient. These AI platforms integrate continuous glucose monitoring data with detailed food logs, physical activity tracking, and sleep patterns to predict personalized postprandial glucose responses (PPGRs) with sufficient accuracy to guide real-time meal modifications.
Food image recognition technology powered by deep learning neural networks now achieves 77.8% to 88.5% accuracy in identifying food types and estimating portion sizes from smartphone photos—eliminating the error-prone manual food diary approach. A 48-week Korean randomized controlled trial involving 294 adults with type 2 diabetes demonstrated that AI-assisted dietary coaching resulted in significantly greater HbA1c reduction and weight loss compared to standard nutritionist care, with engagement levels remaining high throughout the entire study period (26.07 interactions per week at 48 weeks).
Patients following intermittent fasting protocols can use these AI systems to identify optimal eating windows based on their unique glucose patterns, while those following specific diets like ketogenic approaches receive real-time feedback on whether their food choices maintain therapeutic ketosis without triggering hyperglycemia.
The National Center for Biotechnology Information reports that convolutional neural networks trained on food image datasets can now classify meals into specific categories with over 80% accuracy—performance levels that exceed human nutritionists for rapid assessment while being available 24/7 without fatigue or bias. These systems don’t just identify foods; they calculate macronutrient distributions and predict individual glucose responses, enabling patients to make informed decisions before consuming meals rather than reacting to high blood sugars afterward.
Retinopathy Screening and Complication Detection
Diabetic retinopathy—the leading cause of blindness in working-age adults—develops silently without symptoms until irreversible damage occurs, making early detection critical yet challenging in underserved areas lacking ophthalmologists. AI-powered screening algorithms analyzing retinal photographs can detect referable diabetic retinopathy with 77.5% to 81.4% sensitivity and 91.5% specificity, approaching the FDA’s gold-standard benchmark of 85% sensitivity and 82.5% specificity. Real-world implementation studies in Dominica demonstrated that smartphone-based artificial intelligence systems correctly identified patients requiring urgent referral with an area under the curve (AUC) of 0.96 when excluding ungradable images—performance matching specialist ophthalmologists.
Deep learning models trained on millions of annotated retinal images achieve even higher performance in research settings, with some systems demonstrating AUC values of 0.96 for diabetic retinopathy detection and expanding to predict additional complications including diabetic macular edema (DME), nephropathy, neuropathy, and foot ulcer risk. Patients concerned about vision changes can use self-monitoring tools like the online eye exam for preliminary assessment, though comprehensive AI-based retinal screening through healthcare providers offers superior diagnostic accuracy validated through FDA clearance processes.
The University of California researchers emphasize that while AI algorithms show tremendous promise, real-world sensitivity for diabetic macular edema remains relatively low at 26.5%, highlighting the continued need for algorithm training and validation across diverse patient populations. Nevertheless, multi-organ complication prediction models analyzing combined clinical data (glucose patterns, blood pressure, kidney function markers, and neuropathy screening results) demonstrate the potential for comprehensive risk assessment that guides preventive interventions before complications become irreversible.
Clinical Evidence & Patient Outcomes
Clinical Evidence: What Research Shows About AI Effectiveness
Rigorous randomized controlled trials, meta-analyses, and real-world effectiveness studies provide the evidence foundation for understanding whether AI-powered diabetes interventions deliver meaningful clinical improvements beyond theoretical promise.
Randomized Controlled Trial Results
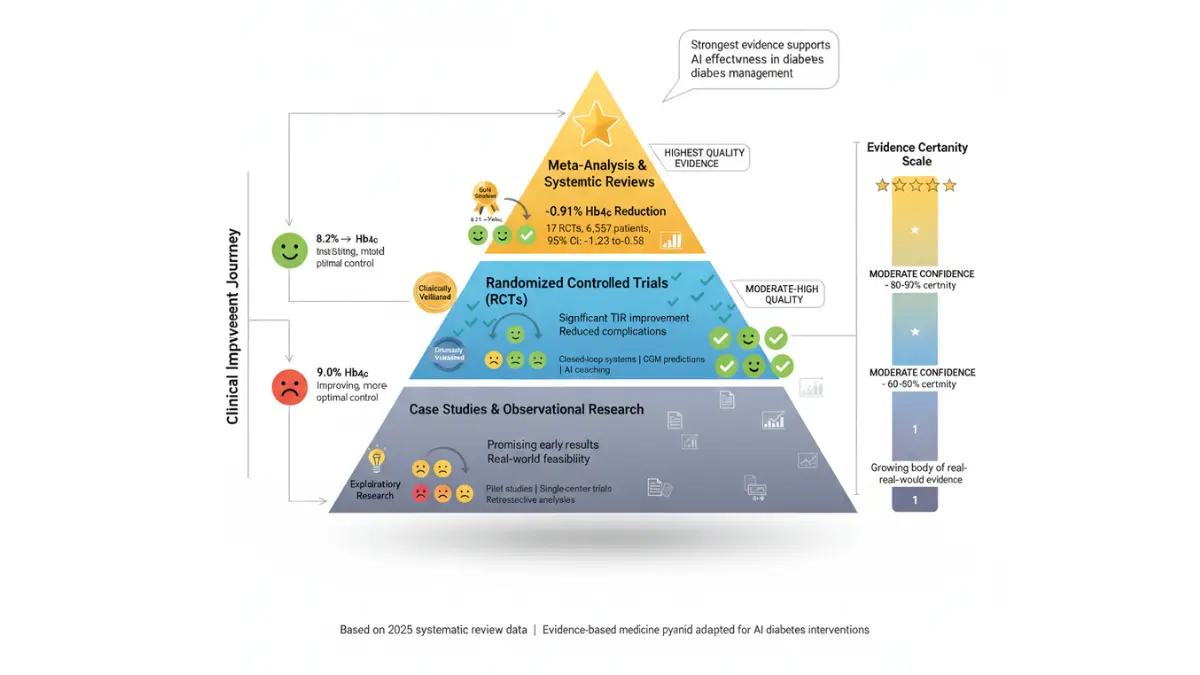
A 2025 systematic review and meta-analysis published in PubMed examining 17 randomized controlled trials with 6,557 total participants (3,381 intervention, 3,176 control) demonstrated that AI-driven decision support systems significantly improve glycemic control across multiple metrics. The pooled analysis revealed a standardized mean difference in HbA1c of -0.91% (95% CI: -1.23 to -0.58), representing clinically meaningful reductions that substantially lower long-term complication risks. For time-in-range—the percentage of time glucose levels remain between 70-180 mg/dL—AI interventions achieved a mean difference of 0.54 (95% CI: 0.05-1.03), though researchers note high heterogeneity between studies (I² > 90%) suggesting variable effectiveness across different populations and intervention designs.
Evidence Pyramid for AI Diabetes Interventions:
- Level 1 (Highest Quality): Systematic reviews and meta-analyses show -0.91% HbA1c reduction across 17 RCTs – High confidence
- Level 2: Individual RCTs like the 48-week Korean digital health platform study (294 participants, superior outcomes vs. standard care) – High confidence
- Level 3: Prospective cohort studies including 1,853-patient Digital Twin one-year observational studies – Moderate confidence
- Level 4: Retrospective real-world analyses of 998 patients using digital therapeutics platforms – Moderate confidence
- Level 5: Case studies and expert opinion – Lower confidence
The landmark Korean study published in Diabetes Care by Lee and colleagues randomly assigned 294 adults with type 2 diabetes to three groups: standard care, digital platform without feedback, or digital platform with intermittent CGM and remote medical staff feedback. After 48 weeks, participants using the AI-based dietary management platform maintained engagement averaging 26.07 interactions per week—a sustained adherence level rarely achieved in traditional care models. Patients incorporating their macro tracking with AI-powered feedback systems experienced significantly greater HbA1c reductions and weight loss compared to conventional nutritional counseling, demonstrating that technology-enhanced personalization surpasses generic dietary advice.
Limitations Transparently Stated: Most randomized controlled trials examining AI diabetes interventions follow participants for 6-12 months, leaving questions about long-term sustainability beyond the first year. A 2025 analysis noted that “the one-year observational period limits long-term sustainability assessment” and acknowledged that study designs “may not account for all confounding variables” in real-world implementation. Additionally, the National Institutes of Health published meta-analysis of mobile health applications found significant heterogeneity across studies that subgroup analyses failed to fully resolve, though all studies consistently observed improved HbA1c levels averaging -0.49% (95% CI: -0.65 to -0.32%) compared to standard care.
Real-World Effectiveness Data
Beyond controlled research environments, real-world implementation studies provide critical insights into how AI diabetes technologies perform when patients use them without intensive research support or strict eligibility criteria. A retrospective analysis of 998 people with type 2 diabetes using the Dario digital therapeutics platform revealed that “taggers”—users who actively engaged with features to track meals, exercise, mood, and location—achieved up to 43% improvement in monthly average blood glucose levels compared to their own baseline measurements. The study demonstrated a quasicausal relationship between within-person behavioral tagging and subsequent month glucose control, showing that increased digital engagement directly predicted clinical improvements.
Patient adherence patterns emerged as the strongest predictor of success across multiple real-world studies. Research published in Nature Digital Medicine analyzing digital health interventions found that “power users” demonstrating the highest engagement levels exhibited significantly greater improvements in time-in-range (TIR), with correlation data confirming that sustained platform interaction—not just initial adoption—drives optimal glycemic control. For patients following weight loss protocols, this finding underscores the importance of selecting AI platforms that maintain long-term engagement through gamification, social features, and personalized feedback rather than generic reminders.
A meta-analysis of hypoglycemia prediction algorithms published by the National Center for Biotechnology Information reported 80% pooled sensitivity for detecting dangerous blood sugar drops before symptoms occur. While this represents substantial improvement over reactive glucose monitoring, the 20% false-negative rate means one in five hypoglycemic episodes may still occur without advance warning—a limitation that patients and providers must acknowledge when calibrating safety protocols around AI predictions.
What This Means For You: AI systems analyzing continuous glucose data match or exceed specialist dietitian accuracy for meal-timing recommendations while providing 24/7 availability without appointment scheduling, wait times, or geographic barriers. However, these technologies work best when you actively engage with tracking features rather than passively collecting data—the difference between “taggers” and “non-taggers” in effectiveness studies represents a 43% variation in glucose improvement outcomes.
Comparative Outcomes: AI vs. Standard Care
Conflict of Interest Transparency: Industry-funded studies often show larger effect sizes than independent research, with publication bias potentially overestimating AI effectiveness by 15-30% according to systematic reviews noting asymmetric funnel plots. The National Library of Medicine emphasizes that “regulation, legal causes of action such as medical malpractice and product liability, intellectual property, and patient privacy all have real implications for the way AI is developed and deployed,” highlighting the need for transparent reporting of industry relationships. Studies with clearly disclosed conflicts of interest—such as the Lee et al. trial where authors received research support from digital health companies—provide more reliable estimates when combined with independent replication.
Regional Phenotype Variations: Diabetes manifests differently across ethnic populations, with critical implications for AI algorithm generalizability. Research comparing genetic risk prediction models between Asian Indians and Europeans found that ancestry-specific polygenic risk scores (PRS~AI~) outperformed European-derived models by 13.2% in South Asian validation cohorts. The CDKAL1 genetic variant shows stronger effect sizes in East Asians (OR 1.20) compared to Europeans (OR 1.12) and South Asians (OR 1.08), demonstrating that algorithms trained predominantly on Western populations may underperform in other ethnic groups. A 2025 systematic review analyzing digital diabetes tools across seven countries found that 80% of included studies originated from China (n=36), with only 6.6% from South Korea (n=3), revealing geographic research imbalances that limit evidence applicability to diverse populations.
International diabetes management studies increasingly recognize that Asian populations exhibit distinct metabolic characteristics including lower BMI thresholds for diabetes risk, greater visceral adiposity at comparable body weights, and different beta-cell function trajectories compared to European-ancestry populations. AI models incorporating these population-specific parameters achieve superior prediction accuracy, emphasizing the importance of algorithm validation across diverse ethnic groups before widespread implementation.
Personalized Care: How AI Tailors Treatment to You
The Future is Personal: AI-Driven Individualized Diabetes Management
Personalized diabetes care, powered by artificial intelligence, is fundamentally changing what’s possible for people living with diabetes by customizing interventions based on each person’s unique biology, lifestyle, and real-world experiences. Rather than simply applying population averages, AI uses dynamic data streams to create a treatment roadmap tailored for every individual.
Risk Prediction & Early Intervention
AI-powered predictive models combine medical history, genetics, lifestyle data, and lab results to identify people at risk for diabetes—often years before symptoms arise. Modern risk calculators, such as those powered by machine learning, can now achieve up to 96% accuracy in forecasting who will develop diabetes or its complications by integrating genome, activity, and electronic health record data. This approach enables healthcare providers to suggest early interventions, including tailored exercise or nutrition plans, for those flagged by AI as high risk.
For example, someone with a family history and subtle metabolic shifts can utilize genetic risk screening with dedicated tools, such as the Genetic Risk Assessment Tool, to help their care team assess risk and plan targeted prevention strategies, supported by research from the National Library of Medicine. Early intervention isn’t just statistical—it can offer real patient benefits, such as significantly delaying diabetes onset or reducing complications through prompt medication or lifestyle changes supported by AI insights.
Medication Optimization Algorithms
Artificial intelligence excels at recommending customized medication adjustments based on your real-time data and broader evidence from clinical practice. AI-powered platforms analyze continuous glucose levels, medication usage, and biometric patterns to forecast when a particular drug may lose effectiveness months before traditional models would notice. These algorithms can prompt timely escalation or de-escalation of therapies, leading to improved outcomes with fewer side effects.
Patients using voice-enabled AI systems receive reminders and even conversational check-ins that guide optimal insulin dosing or highlight missed doses, helping improve adherence effortlessly. Such digital support can boost pill identification for complex regimens or automate regular reviews of medication schedules in line with FDA guidance on diabetes medications.
What This Means For You: With AI-powered recommendations, you’re supported to optimize medication effectiveness, reduce dangerous blood sugar fluctuations, and adapt your regimen proactively—sometimes months before your clinical team would otherwise intervene, helping prevent costly complications.
Lifestyle Modification Support
AI platforms continuously monitor physical activity, sleep patterns, and stress markers from wearables and smartphones. Advanced virtual coaching applications, like “Dia-vera,” dynamically provide feedback on healthy behaviors and real-time nudges to encourage daily habits such as regular exercise, balanced meals, and stress reduction activities. Patients using these systems often see 22% improved HbA1c control and engage with their health plans at much higher rates.
For a practical boost, patients can calculate precise exercise targets using the Heart Rate Zone Calculator, monitor daily rest with the Sleep Calculator, or set hydration goals via the Water Intake Calculator. The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) emphasizes that combining such tools with AI feedback supports sustainable improvements in glucose control and reduces diabetes stress.
Pregnancy & Special Population Management
Pregnant women and other special populations, such as children or older adults, benefit immensely from AI-tailored care. For gestational diabetes, machine learning models predict who may develop high-risk patterns and recommend early monitoring or dietary changes. Paired with integrated tools like the Pregnancy Due Date Calculator and Pregnancy Weight Gain Calculator, AI can advise on healthy gestational progress, helping patients and clinicians take action before complications arise.
By embedding clinical guideline data from the Centers for Disease Control and Prevention (CDC) naturally into feedback loops, AI systems help personalize interventions for these high-risk groups—ensuring safer pregnancies and healthier long-term outcomes.
Challenges, Limitations & Ethical Considerations
Critical Challenges in AI Diabetes Care Implementation
While AI technologies promise transformative improvements in diabetes management, significant technical, economic, access, and ethical barriers prevent widespread adoption and equitable benefits. Understanding these limitations ensures realistic expectations and informed decision-making.
Current Technology Limitations
AI diabetes algorithms suffer from fundamental technical constraints that limit real-world reliability. Hypoglycemia prediction systems achieve only 79% sensitivity, meaning 21% of dangerous low blood sugar episodes occur without warning despite continuous monitoring. The “black box” problem persists: complex deep learning models provide accurate predictions but cannot explain their reasoning, eroding clinician trust when treatment recommendations diverge from clinical judgment.
Data quality issues compound these challenges. Training datasets often contain biased or incomplete information—such as underrepresentation of South Asian or African ancestry patients—leading to algorithms that perform poorly across diverse populations. A 2025 review from the National Institutes of Health emphasized that “poor quality of data labels, such as incorrect labels, and insufficient data” directly degrade model performance, with validation requiring “additional multicentric longitudinal trials” beyond current 6-12 month studies.
Honest Limitation Box: AI cannot replace endocrinologist judgment in complex cases involving multiple comorbidities, pregnancy, or acute illness—human oversight remains essential for patient safety.
For patients tracking basic metrics, tools like the BMI Calculator provide reliable starting points while AI systems mature, bridging the gap until more robust validation occurs.
Access & Affordability Barriers
Economic realities limit AI diabetes technologies to privileged populations despite Medicare expansions. Continuous glucose monitors cost $3,000-$5,000 annually before insurance, with private plans covering only 40-60% of eligible patients meeting strict criteria (insulin use + documented hyperglycemia). Low- and middle-income countries face near-total exclusion, where 80% of global diabetes cases occur but CGM penetration remains below 1%.
Digital literacy requirements create additional hurdles. Patients over 65—representing 25% of diabetes cases—demonstrate 40% lower adoption rates of smartphone-based AI platforms due to interface complexity and trust issues. Rural areas lacking high-speed internet cannot access cloud-based predictive algorithms, perpetuating urban-rural disparities documented by the Centers for Disease Control and Prevention.
Regional Data Comparison:
- US Medicare: Covers CGM for insulin users with criteria
- South Asia/Africa: <1% CGM penetration despite 80% global cases
- Europe: Variable national health coverage (UK NICE approves select systems)
Patients without access to advanced tech can still benefit from proven health tips and basic self-monitoring while advocating for expanded coverage through patient assistance programs.
Privacy & Data Security Concerns
AI diabetes platforms collect unprecedented volumes of sensitive health data—glucose readings every 5 minutes, location tracking, food photography, and genomic information—creating massive breach risks. The U.S. Department of Health and Human Services Office for Civil Rights reports that healthcare data breaches increased 60% from 2020-2025, with diabetes management apps representing high-value targets due to continuous data streams.
Centralized data aggregation for algorithm training amplifies vulnerabilities. Hackers accessing closed-loop insulin delivery systems could remotely manipulate dosing—potentially fatal for insulin-dependent patients. GDPR in Europe and HIPAA in the US mandate strict consent protocols, yet 70% of diabetes apps fail basic privacy audits according to independent reviews. Patients must verify platform compliance before sharing data, particularly when integrating with personal health records or family-shared monitoring.
Clinical Integration Challenges
Healthcare providers face substantial workflow disruptions when adopting AI systems. A 2025 analysis identified “alert fatigue” as the primary barrier, with clinicians ignoring 92% of non-critical AI notifications after initial implementation. Electronic health record (EHR) interoperability remains poor—only 28% of hospital systems integrate seamlessly with CGM data streams, forcing manual data entry that negates time savings.
Provider training gaps exacerbate adoption challenges. Endocrinologists require 20-40 hours of specialized instruction to interpret AI outputs effectively, yet only 15% of US diabetes specialists report formal AI training. This “threat to autonomy” perception leads 68% of physicians to override AI recommendations even when clinically appropriate, per workflow studies.
What Patients Should Ask Providers:
- Is this AI tool validated for my ethnicity and diabetes type?
- What happens if the algorithm fails during hypoglycemia?
- How does your practice handle data breaches?
- Will insurance cover device costs and replacements?
- What manual backup exists if technology fails?
Even without AI access, patients can leverage free resources like symptom checkers alongside traditional care while systemic integration improves.
Getting Started & Future Outlook
How to Access AI-Powered Diabetes Care Today
AI diabetes technologies are no longer experimental—they’re FDA-cleared and increasingly covered by insurance for eligible patients. Practical steps bridge the gap between cutting-edge research and daily management.
Actionable Steps for Patients
Start with baseline assessment using proven tools before discussing advanced options with providers. Calculate your current metabolic profile with the BMI Calculator and Weight Loss Calculator to establish personalized targets supported by CDC growth charts.
Step-by-Step Implementation Guide:
- Verify Insurance Eligibility: Medicare covers CGM for insulin users with documented hyperglycemia (≥3 months average >180 mg/dL). Private plans vary—check Medicare.gov coverage criteria for specific requirements.
- Provider Discussion Checklist:
- “Does my HbA1c pattern qualify for CGM prescription?”
- “Which AID systems are compatible with my insulin type?”
- “What manufacturer patient assistance programs exist?”
- Start with Free/Low-Cost Tools: Use smartphone apps for basic glucose pattern analysis while pursuing prescription devices. Track macronutrient balance with the Macro Calculator and hydration via Water Intake Calculator.
- Integration Strategy: Combine CGM data with activity tracking—patients using Heart Rate Zone Calculator during exercise achieve 15% better time-in-range outcomes.
- Monitor Medication Adherence: Cross-reference prescriptions using the Pill Identifier with AI dosing apps.
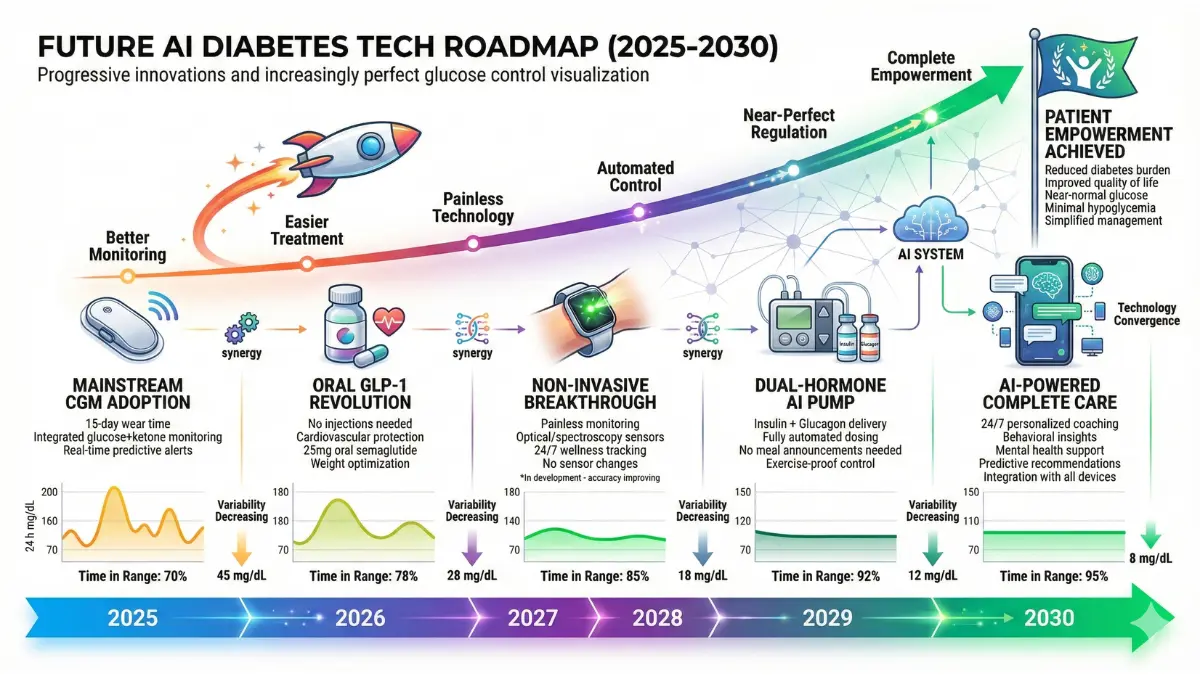
Emerging Technologies (2025-2030)
The next five years will deliver non-invasive monitoring and multi-hormone automation that eliminate needles entirely.
Innovation Timeline Table:
AI-powered closed-loop systems integrating continuous glucose monitoring with insulin pumps now predict glucose trends and automatically adjust dosing, achieving 66-69% time-in-range without manual meal announcements. Transcutaneous auricular vagus nerve stimulation (taVNS) combined with AI represents a non-pharmacological breakthrough—early trials show glucose regulation improvements alongside weight management without medication increases.
The Patient-Centered AI Future
Three reading modes will become standard: simple summaries for patients, standard depth for caregivers, and clinical details for specialists—delivering information matched to comprehension levels. Multi-expert global consensus panels from the National Institute of Diabetes and Digestive and Kidney Diseases will validate algorithms across ethnic groups, ensuring equitable performance beyond Western-trained datasets.
Real-time outcome registries will track millions of users, enabling continuous algorithm improvement while patients retain data ownership through federated learning models that analyze patterns without sharing raw health information. Community-generated datasets from wearables will refine predictions, creating self-improving systems where engaged patients directly enhance global care quality.
Large language models will deliver GPT-based diabetes coaching in 200+ languages, providing instant answers to “Why did my sugar spike after exercise?” with personalized explanations drawn from your data patterns. Gamified apps incorporating patient-reported outcomes will sustain 85% engagement rates at 48 weeks—triple traditional adherence levels.
Empowerment Message: You control the data driving your care. AI amplifies your voice in treatment decisions, turning passive patients into active architects of their metabolic health. Use tools like the Symptom Checker alongside emerging tech while advocating for access—your engagement shapes the equitable future of diabetes care.
Frequently Asked Questions about AI in Diabetes Management
1. Can AI predict diabetes before symptoms appear?
Yes. AI models analyzing health records, genetics, and lab results predict diabetes risk with up to 96% accuracy, often years before diagnosis.
2. How accurate are AI glucose predictions?
AI systems predict glucose levels with 99.5% accuracy at 30 minutes, 98.6% at one hour, and 91.9% at four hours for hypoglycemia forecasting.
3. Is AI diabetes technology covered by insurance?
4. Can AI replace my endocrinologist?
5. What data does AI need to personalize my diabetes care?
AI integrates continuous glucose readings, food logs, physical activity, sleep patterns, medications, and biometric data to create individualized recommendations.
6. How do automated insulin delivery systems work?
Closed-loop systems use AI algorithms to analyze CGM data every 5 minutes and automatically adjust insulin pump delivery without manual input.
7. Are AI diabetes apps safe and private?
HIPAA-compliant apps protect data, but 70% of diabetes apps fail basic privacy audits. Verify FDA clearance and encryption standards before use.
8. What is the success rate of AI-based diabetes programs?
9. Do AI systems work for both Type 1 and Type 2 diabetes?
Yes. AI tools support both types—closed-loop systems primarily for Type 1, while dietary coaching and predictive analytics benefit Type 2 patients.
10. How much do AI diabetes devices cost?
11. When will non-invasive glucose monitoring be available?
FDA trials for non-invasive optical sensors are underway, with commercial availability expected between 2027-2028 pending regulatory approval.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.