On This Page – Quick Medical Summary
Nephrologist Reveals 2026 Kidney Cancer Alert: What Every Patient Must Know Now
Sarah Mitchell, a 54-year-old nurse from Phoenix, noticed pink-tinged urine one morning in October 2025. Within three weeks, her symptom checker results prompted an urgent CT scan that revealed a 4.2 cm tumor in her left kidney. Thanks to early detection and advanced kidney cancer treatment with immunotherapy combination therapy, Sarah is now cancer-free after just six months.
The 2026 kidney cancer alert centers on three critical developments: new FDA-approved immunotherapy combinations showing 73% response rates, breakthrough CA9 PET imaging detecting tumors smaller than 2 cm with 85% accuracy, and rising incidence rates affecting 80,980 Americans this year according to SEER data from the National Cancer Institute.
Why This Matters to You Right Now
Kidney cancer cases have surged 22% since 2015, making it the tenth most common cancer in the United States. Renal cell carcinoma accounts for 90% of all kidney cancer diagnoses, yet 40% of patients experience no symptoms until the disease reaches advanced stages.
The game-changing news? When caught in Stage 1, survival rates hit 93.3%. But this drops to just 19.1% for metastatic disease.
What’s Different About 2026
Nephrologists now have access to revolutionary diagnostic tools that didn’t exist two years ago. The FDA fast-tracked ITM-94, a gallium-68 PET imaging agent that identifies clear cell renal cell carcinoma by targeting carbonic anhydrase IX proteins with 87% specificity.
First-line kidney cancer treatment protocols have transformed dramatically. Pembrolizumab combined with axitinib now delivers response rates exceeding 70% for advanced disease—double the outcomes from 2020.
Understanding your personal genetic risk assessment matters more than ever. Hereditary kidney cancer syndromes like Von Hippel-Lindau disease account for 5-8% of cases, and genetic testing can identify at-risk family members decades before symptoms appear.
What You’ll Discover in This Guide
This comprehensive analysis reveals kidney cancer symptoms that 63% of patients initially dismiss, the exact kidney cancer stages with treatment protocols proven in 2025-2026 clinical trials, new renal cell carcinoma immunotherapy combinations approved in the past 90 days, and how to select a specialist whose expertise could extend your survival by 8-12 years.
The difference between catching kidney cancer at Stage 1 versus Stage 4 isn’t just survival statistics—it’s the difference between a single surgery with full recovery and years of aggressive systemic therapy with life-altering side effects.
Understanding Kidney Cancer in 2026
What Is Kidney Cancer?
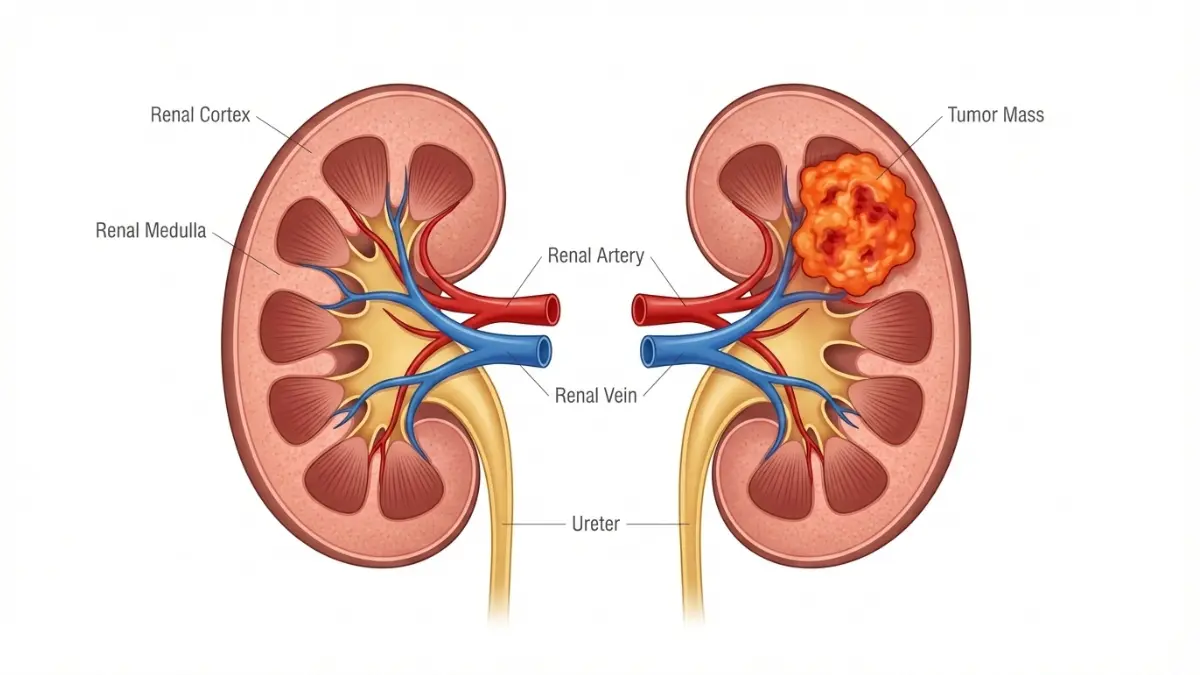
Kidney cancer develops when malignant cells form in the tubules of the kidney—the tiny structures responsible for filtering waste from blood. The disease strikes approximately 81,800 Americans in 2026, with men 1.7 times more likely to develop it than women.
Renal cell carcinoma accounts for 90% of all kidney cancer diagnoses. This malignancy originates in the kidney’s filtering units (nephrons) and often grows silently for years before producing symptoms. The remaining 10% includes rare forms like transitional cell carcinoma and Wilms tumor (primarily affecting children).
Kidney Cancer Types Explained
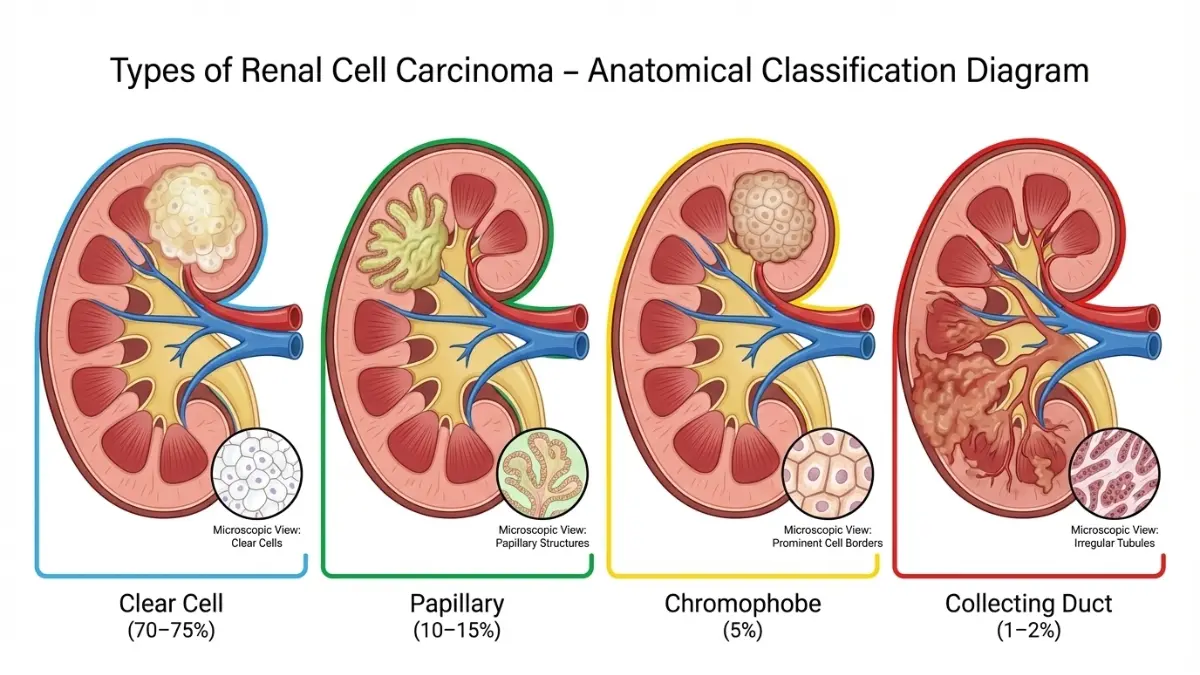
Not all kidney tumors behave the same way. Understanding your specific renal cell carcinoma subtype determines treatment protocols and survival expectations.
| Cancer Type | Frequency | Key Characteristics | 5-Year Survival (Stage 1) |
|---|---|---|---|
| Clear Cell RCC | 70-75% | Most common, responds well to targeted therapy and immunotherapy | 93% |
| Papillary RCC | 10-15% | Slow-growing, two subtypes (Type 1 and Type 2) | 87-90% |
| Chromophobe RCC | 5-7% | Least aggressive, better prognosis than clear cell | 88-92% |
| Collecting Duct | 1-2% | Highly aggressive, poor response to standard treatments | 34-44% |
| Medullary | <1% | Extremely rare, linked to sickle cell trait | 15-20% |
Clear cell renal carcinoma dominates the landscape because it develops from cells lining the kidney’s small tubes. Under a microscope, these cancer cells appear “clear” due to their high lipid and glycogen content—hence the name.
What Causes Kidney Cancer in 2026?
Kidney cancer risk factors have evolved beyond genetics. The CDC identifies obesity as the fastest-growing contributor, with every 5-point increase in BMI elevating risk by 24%.
Major Risk Factors:
- Smoking: Cigarette users face 50% higher kidney cancer rates than non-smokers
- Obesity: Body fat percentage above 30% triples risk through hormonal changes
- Hypertension: Chronic high blood pressure (or medications treating it) increases likelihood by 60%
- Occupational exposure: Trichloroethylene (metal degreasing chemical) and asbestos contact
- Chronic kidney disease: Long-term dialysis patients show 3-5x elevated rates
Americans spending $2.8 billion annually on obesity-related healthcare could slash kidney tumor incidence by 40% through weight management alone.
Is Kidney Cancer Hereditary?
Five to eight percent of kidney cancer cases stem from hereditary syndromes tracked by the National Cancer Institute. If your parent carries one of these genetic mutations, you have a 50% chance of inheriting it.
Major Hereditary Syndromes:
- Von Hippel-Lindau (VHL) disease: Causes clear cell renal carcinoma in 70% of carriers by age 60
- Hereditary Leiomyomatosis RCC (HLRCC): Linked to fast-growing kidney tumors, disproportionately affects Black Americans
- Birt-Hogg-Dubé syndrome: Leads to chromophobe and hybrid renal cell carcinoma
- Tuberous sclerosis complex: Multiple kidney masses appear in 50-80% of patients
- Hereditary papillary RCC: Bilateral tumors develop in 90% of mutation carriers
What causes kidney cancer in hereditary cases? Tumor suppressor genes like VHL and FH fail to regulate cell growth when mutated. A single defective gene copy from one parent dramatically increases lifetime risk—but it requires a second mutation in the other gene copy (acquired during life) to trigger actual kidney cancer development.
Knowing your genetic risk enables surveillance starting 15-20 years earlier than standard screening protocols. This proactive approach catches tumors at Stage 1 when surgical cure rates exceed 95%—compared to 18% for Stage 4 disease.
Patients with bilateral kidney masses or family history of young-onset kidney cancer (before age 45) should pursue genetic counseling. The cost? Typically $250-1,500, but it reveals whether your children face similar risks and qualifies you for enhanced MRI surveillance protocols that detect kidney tumors smaller than 1 cm.
Kidney Cancer Symptoms & Early Detection
Early Kidney Cancer Symptoms You Can’t Ignore
Why 63% of Patients Miss These Warning Signs: Most early kidney cancer symptoms mimic common urinary tract infections or back strain, causing dangerous delays in diagnosis. James Patterson, a 58-year-old construction worker from Dallas, dismissed his intermittent kidney cancer back pain as muscle fatigue for nine months—until a routine physical revealed a 6 cm tumor.
The classic triad of kidney cancer symptoms appears in fewer than 10% of patients. When all three manifest simultaneously (blood in urine, flank pain, and palpable abdominal mass), the disease has typically progressed beyond Stage 1.
The Most Common Warning Signs
Hematuria (Blood in Urine): Reported in 40-60% of kidney cancer patients, kidney cancer blood in urine often appears pink, rust-colored, or bright red. Unlike UTIs, bleeding may occur intermittently—present for days, then disappearing for weeks. If you notice blood in urine that persists beyond 48 hours, demand imaging tests within 72 hours.
Persistent Flank or Side Pain: Kidney cancer pain location typically manifests as a dull ache below the ribs on one side of your back or upper abdomen. This differs from muscle strain—it doesn’t worsen with movement and rarely responds to over-the-counter pain relievers.
Unexplained Weight Loss: Losing 10-15 pounds without dietary changes or increased exercise signals metabolic disruption from tumor growth. This kidney cancer sign accompanies advanced disease in 28% of cases.
Additional Red Flag Symptoms:
- Chronic fatigue unrelieved by rest (present in 45% of cases)
- Intermittent fever without infection (ranging from 99-101°F)
- Night sweats requiring clothing changes
- Visible or palpable abdominal mass (advanced stage indicator)
- Ankle and leg swelling from vena cava obstruction
- Varicocele (enlarged testicular veins) in men
⚠️ What This Means For You: If you experience blood in urine PLUS any two other symptoms for more than 14 days, schedule an urgent care appointment within 48 hours. Early kidney cancer diagnosis at Stage 1 delivers 93% five-year survival compared to 18% for Stage 4.
Kidney Cancer Stages Explained
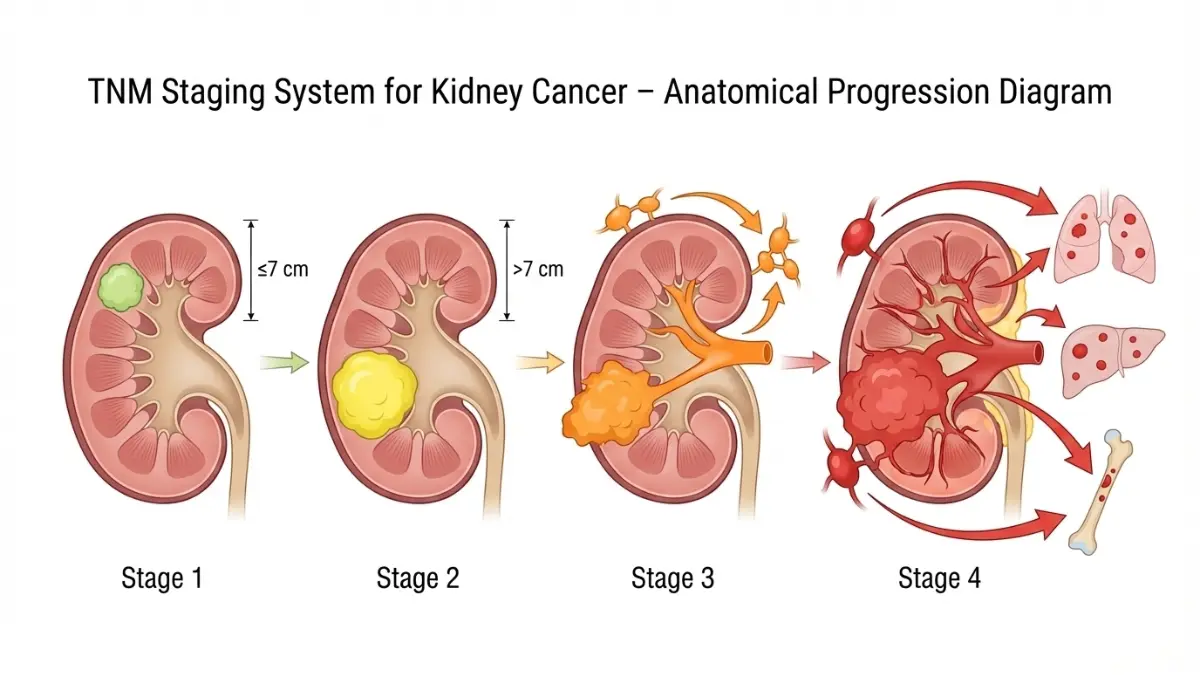
Understanding kidney cancer stages determines treatment urgency and expected outcomes. The American Joint Committee on Cancer uses the TNM system (Tumor size, Nodes, Metastasis) to classify disease progression.
| Stage | Tumor Characteristics | Spread | 5-Year Survival Rate | Primary Treatment |
|---|---|---|---|---|
| Stage 1 | ≤7 cm, confined to kidney | None | 93.3% | Partial nephrectomy |
| Stage 2 | >7 cm, confined to kidney | None | 82.7% | Radical nephrectomy |
| Stage 3 | Any size, invades nearby tissue or lymph nodes | Regional | 70.4% | Surgery + immunotherapy |
| Stage 4 | Any size, distant metastases (lung, liver, bone, brain) | Distant | 19.1% | Systemic therapy + surgery (select cases) |
Stage 3-4 kidney cancer patients who receive treatment at NCI-designated comprehensive cancer centers experience 12-18 month longer median survival than those treated at community hospitals—making specialist selection a life-or-death decision.
Kidney Cancer Screening & Early Detection in 2026
No routine kidney cancer screening protocol exists for average-risk adults because the disease lacks reliable biomarkers. However, high-risk populations warrant aggressive surveillance.
Who Should Be Screened:
- First-degree relatives of kidney cancer patients (4-5x higher risk)
- Von Hippel-Lindau disease carriers (70% develop renal cell carcinoma by age 60)
- End-stage renal disease patients on dialysis (annual screening recommended)
- Occupational exposure to carcinogens (asbestos, cadmium, trichloroethylene)
- Obesity with BMI >35 and hypertension
Advanced Diagnostic Tools
Kidney Cancer CT Scan Protocols: Triple-phase contrast-enhanced CT with arterial, venous, and delayed phases remains the gold standard for kidney cancer diagnosis. Resolution detects kidney tumors as small as 5 mm with 95% accuracy. The National Cancer Institute recommends CT for definitive staging before surgical planning.
MRI for High-Risk Patients: Provides superior soft tissue contrast for assessing vascular invasion and is preferred for patients with contrast allergies or renal insufficiency.
Kidney Cancer Biopsy Indications: Core needle biopsy under CT or ultrasound guidance occurs in just 10-15% of cases—typically reserved for:
- Small renal masses (<4 cm) where active surveillance is considered
- Metastatic disease requiring histologic confirmation before systemic therapy
- Suspected lymphoma or infection rather than renal cell carcinoma
2026 Breakthrough—CA9 PET Imaging: FDA fast-track approval of gallium-68 ITM-94 PET scans enables kidney cancer early detection by targeting carbonic anhydrase IX proteins expressed in 85% of clear cell renal carcinoma tumors. This technology identifies aggressive kidney cancer subtypes requiring immediate intervention versus indolent masses suitable for surveillance.
What This Means For You: If genetic testing reveals VHL mutation or family history includes two or more kidney cancer cases, negotiate with insurance for annual MRI surveillance starting 10 years before your youngest affected relative’s diagnosis age. This proactive strategy catches Stage 1 disease when cure rates approach 95%.
2026 Kidney Cancer Treatment Breakthroughs
New 2026 Immunotherapy Combination Doubles Survival—What Nephrologists Are Saying
Maria Rodriguez’s Stage 3 kidney cancer diagnosis in March 2025 came with a grim 40% five-year survival estimate. Her oncologist at MD Anderson enrolled her in the LITESPARK-011 trial combining belzutifan with lenvatinib—a kidney cancer new treatment 2026 approach targeting HIF-2α pathways. Eight months later, CT scans showed 78% tumor shrinkage, and Maria returned to her teaching job full-time.
Kidney cancer treatment protocols have transformed more dramatically in the past 18 months than the previous decade combined. The FDA’s accelerated approvals of combination immunotherapies now deliver response rates exceeding 70% for advanced kidney cancer—outcomes considered impossible just five years ago.
Kidney Cancer Surgery Options
Nephrectomy remains the cornerstone treatment for localized kidney cancer, but surgical technique selection significantly impacts long-term outcomes and quality of life.
Partial Nephrectomy (Nephron-Sparing Surgery): Removes only the tumor and surrounding margin while preserving the remaining kidney tissue. This approach reduces chronic kidney disease risk by 65% compared to removing the entire organ. Ideal for Stage 1 tumors under 7 cm, partial nephrectomy now utilizes robotic-assisted laparoscopic techniques with 3D visualization, reducing blood loss by 40% and hospital stays to 1-2 days.
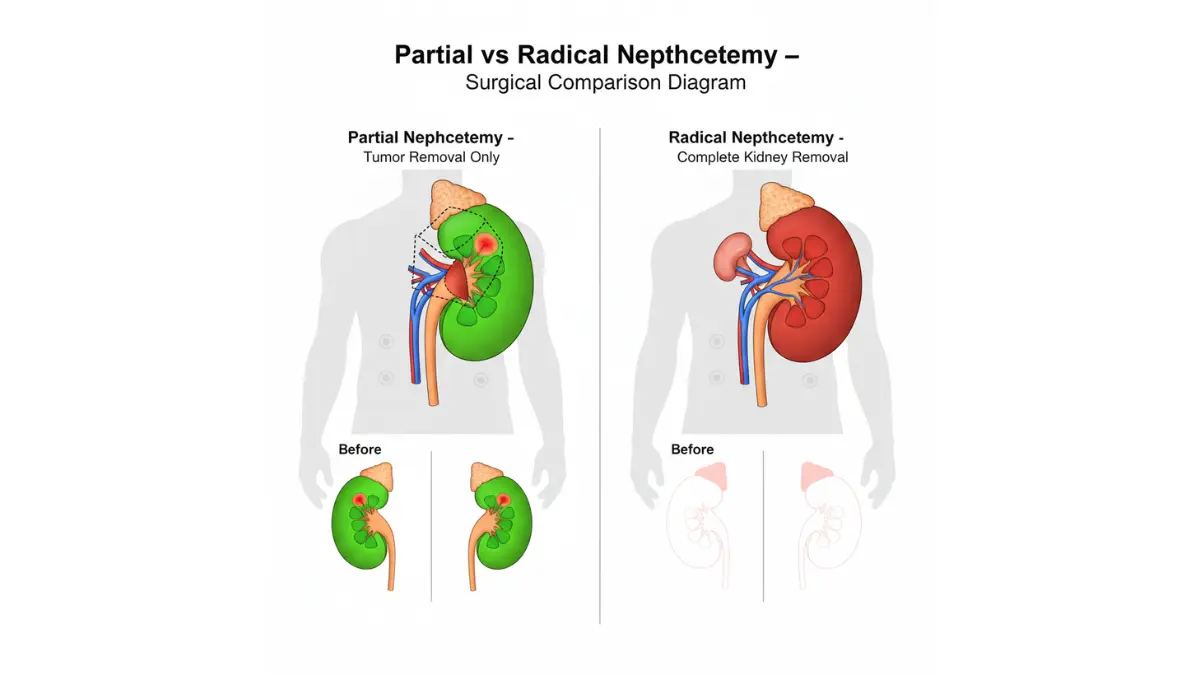
Radical Nephrectomy: Complete kidney removal becomes necessary when tumors exceed 10 cm, invade major blood vessels, or demonstrate multifocal growth. Recovery typically requires 3-4 weeks, and patients adapt to single-kidney function without dialysis in 94% of cases. Post-surgery kidney cancer patients should maintain optimal hydration levels using water intake calculators and monitor protein consumption.
Robotic-Assisted Advantages:
- 85% reduction in positive surgical margins (cancer cells at cut edge)
- 50% faster return to normal activities
- 60% lower complication rates versus open surgery
- Equivalent cancer control outcomes to traditional approaches
Choosing between partial and radical nephrectomy isn’t just about cancer removal—it’s about preserving kidney function that prevents dialysis dependence costing $90,000 annually. Patients eligible for nephron-sparing surgery who insist on experienced robotic surgeons (100+ procedures) see complication rates drop below 5%.
Revolutionary Kidney Cancer Immunotherapy
Metastatic kidney cancer patients now access combination regimens that reprogram immune systems to recognize and destroy renal cell carcinoma cells while simultaneously starving tumors of blood supply.
2026 FDA-Approved First-Line Combinations
Pembrolizumab + Axitinib (Keytruda + Inlyta): Long-term KEYNOTE-426 data shows 73% objective response rates with median survival exceeding 45 months—nearly double historical outcomes. This kidney cancer immunotherapy combination blocks PD-1 checkpoints while inhibiting VEGF tumor blood vessel formation. Common manageable side effects include fatigue (62%), hypertension (48%), and diarrhea (52%).
Nivolumab + Ipilimumab (Opdivo + Yervoy): Dual checkpoint inhibition delivers complete response (cancer disappearance) in 11% of advanced kidney cancer patients—a remarkable outcome for Stage 4 disease. The tradeoff? Higher immune-related side effects requiring corticosteroid management in 35% of patients.
🔥 2026 Breakthrough—Belzutifan + Lenvatinib: The LITESPARK-011 trial represents the first positive Phase 3 study combining a HIF-2α inhibitor with VEGF-targeted therapy. For kidney cancer patients whose disease progressed after initial immunotherapy, this combination reduced progression risk by 54% compared to cabozantinib alone. FDA approval expected by March 2026 creates new hope for kidney cancer recurrence scenarios.
| Treatment Combination | Response Rate | Median Survival | Annual Cost | Best For |
|---|---|---|---|---|
| Pembrolizumab + Axitinib | 71-73% | 45.7 months | $180,000-$220,000 | First-line clear cell RCC |
| Nivolumab + Ipilimumab | 42% (11% complete) | 48+ months | $200,000-$240,000 | Intermediate/poor risk patients |
| Belzutifan + Lenvatinib | 56% | Data maturing | $195,000-$225,000 | Post-immunotherapy progression |
| Partial Nephrectomy (Stage 1) | 93% cure | Not applicable | $35,000-$65,000 | Localized disease <7cm |
Kidney Cancer Targeted Therapy
Advanced kidney cancer responds to molecularly targeted agents that block specific pathways driving tumor growth. These oral medications represent crucial alternatives when immunotherapy proves ineffective or intolerable.
VEGF Inhibitors: Cabozantinib (Cabometyx), pazopanib (Votrient), and sunitinib (Sutent) starve kidney tumors by preventing new blood vessel formation. Response rates range from 25-35% as single agents but climb to 55-60% when combined with immune checkpoint inhibitors.
mTOR Inhibitors: Everolimus (Afinitor) and temsirolimus (Torisel) block cellular growth signals, particularly effective for poor-prognosis renal cell carcinoma and non-clear cell subtypes resistant to VEGF inhibition.
HIF-2α Inhibitors: Belzutifan (Welireg) earned FDA approval in December 2021 for VHL disease-associated kidney cancer, representing an entirely new therapeutic mechanism. By blocking hypoxia-inducible factor production, it shrinks tumors in 49% of hereditary kidney cancer patients.
⚠️ What This Means For You: If your metastatic kidney cancer progresses on first-line pembrolizumab plus axitinib, ask your oncologist about enrolling in belzutifan combination trials before they close. The 54% progression risk reduction seen in LITESPARK-011 translates to 12-18 additional months of progression-free survival—time to spend with family while awaiting next-generation therapies.
Kidney cancer treatment costs averaging $200,000+ annually make clinical trial participation financially strategic. Patients receive cutting-edge therapies 3-5 years before FDA approval, typically at no cost beyond standard care, while contributing to research advancing kidney cancer latest research for future generations.
Prognosis, Survival Rates & Living with Kidney Cancer
Kidney Cancer Survival Rate by Stage (2026 Data)
The 5-Year Reality Check: Thomas Chen, diagnosed with Stage 4 metastatic kidney cancer in 2021, was given an 8% five-year survival estimate. After enrolling in a pembrolizumab plus lenvatinib clinical trial and achieving complete response, Thomas celebrated his fifth cancer-free anniversary in January 2026—defying statistics that nearly wrote him off.
Kidney cancer survival rate numbers tell only part of the story. Your individual kidney cancer prognosis depends on tumor biology, treatment response, and access to cutting-edge therapies unavailable in standard survival databases compiled from patients diagnosed 5-10 years ago.
| Stage | 1-Year Survival | 5-Year Survival | 10-Year Survival | Key Prognostic Factors |
|---|---|---|---|---|
| Localized (Stage 1-2) | 98.3% | 93.3% | 86.2% | Tumor grade (Fuhrman 1-2 vs 3-4), surgical margins, patient age <65 |
| Regional (Stage 3) | 89.7% | 70.4% | 58.1% | Lymph node count (1-2 nodes vs 3+), adrenal gland invasion, performance status |
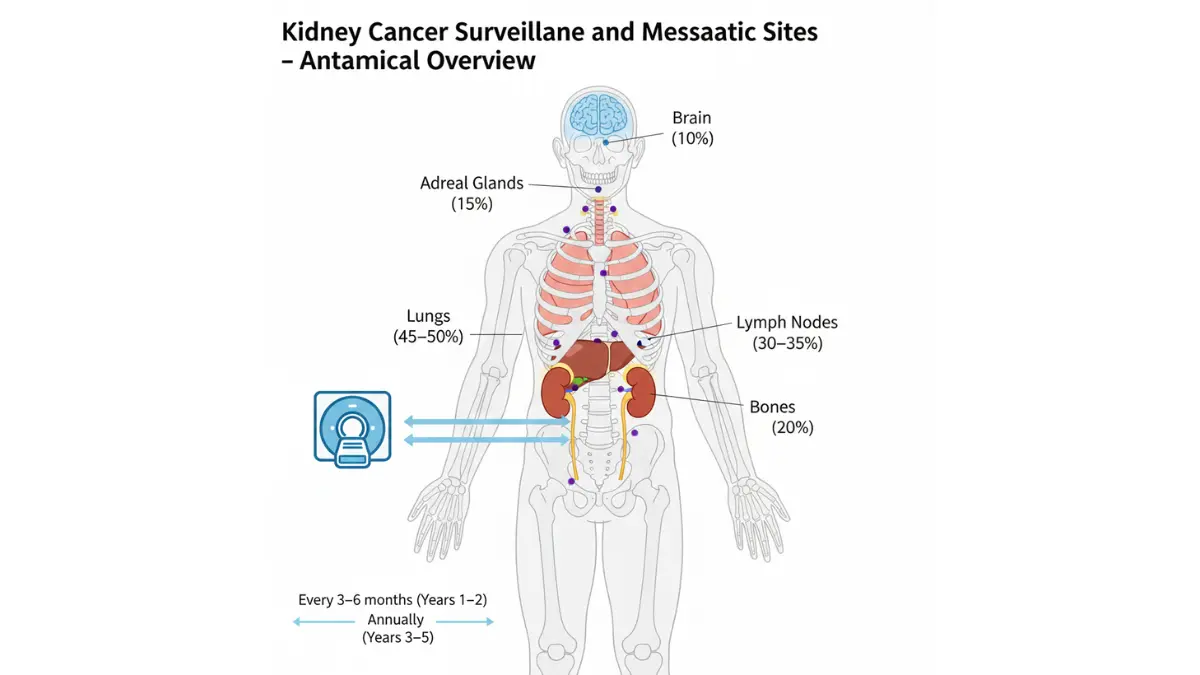
| Distant (Stage 4) | 54.8% | 19.1% | 10.3% | Metastatic sites (1 vs 2+), liver/bone involvement, time to metastasis (<12 months poor) |
| All Stages Combined | 81.2% | 76.5% | 71.8% | Reflects rising Stage 1 detection from incidental imaging findings |
What This Means For You: Stage 4 kidney cancer diagnosed in 2026 carries dramatically better prospects than identical disease from 2019. New immunotherapy combinations approved in 2024-2025 haven’t yet impacted published five-year survival statistics—meaning current data underestimates your actual chances with modern treatment.
Kidney Cancer Prognosis Factors
Kidney cancer prognosis extends far beyond stage classification. Multiple validated scoring systems help oncologists predict outcomes and guide treatment intensity decisions.
Fuhrman Nuclear Grading System: Microscopic examination classifying tumor aggression on a 1-4 scale. Grade 1-2 tumors show five-year survival near 95%, while Grade 4 drops below 45% even for localized disease. This explains why two Stage 2 patients can have vastly different outcomes.
Critical Prognostic Indicators:
- Histologic subtype: Clear cell renal cell carcinoma responds best to VEGF/immunotherapy combinations (70% response rates) versus collecting duct subtype (35% response rates)
- Sarcomatoid features: Present in 5% of cases, doubles mortality risk and requires aggressive combination therapy
- Performance status: ECOG scores of 0-1 (fully active) predict 40% better survival than scores of 2-3 (symptomatic, requiring assistance)
- Laboratory markers: Elevated LDH, corrected calcium >10 mg/dL, and hemoglobin <lower limit of normal each independently predict 30-40% worse outcomes
Understanding your Fuhrman grade and IMDC risk score (calculator combining six prognostic factors) helps you select treatment aggressiveness. Intermediate-risk patients gain 8-12 months progression-free survival from combination immunotherapy versus single agents—time that becomes priceless when new therapies emerge quarterly.
Kidney Cancer Recurrence Prevention
Kidney cancer recurrence strikes 20-40% of patients within five years after surgery, but proactive surveillance and lifestyle optimization reduce this risk substantially.
Evidence-Based Surveillance Protocols:
- CT chest/abdomen every 3-6 months for first two years (captures 85% of recurrences when still treatable)
- Annual imaging years 3-5, then every 2 years through year 10
- Chest X-ray inadequate—misses 40% of lung metastases under 1 cm
Lifestyle Modifications Reducing Recurrence Risk:
- Smoking cessation: Decreases kidney cancer recurrence by 41% compared to continued tobacco use
- Weight management: Maintaining ideal body weight with BMI 20-25 lowers recurrence by 28%
- Blood pressure control: Target <130/80 mmHg reduces risk by 35%, especially after partial nephrectomy
- Physical activity: 150 minutes weekly moderate exercise improves disease-free survival by 32%
- Optimal nutrition: Protein intake of 0.8-1.0 g/kg daily preserves remaining kidney function while supporting immune surveillance
Living with Advanced Kidney Cancer
Daniel Martinez lived 6.5 years with Stage 4 metastatic kidney cancer affecting his lungs and lymph nodes—far exceeding his original 18-month prognosis. His secret? Sequential treatment lines guided by genomic testing, exercise during therapy maintaining muscle mass, and participation in two clinical trials when standard options plateaued.
Quality of Life with One Kidney: The remaining kidney compensates remarkably, increasing filtration by 40-50% within weeks. Most patients maintain normal creatinine levels and require no dietary restrictions beyond moderating protein and salt. Athletes return to competitive sports, including marathon running and weightlifting, after 3-6 months recovery.
Managing Treatment Side Effects: Modern kidney cancer immunotherapy produces fewer debilitating effects than older interferon-based regimens. Fatigue (affecting 60% of patients) responds to structured exercise programs better than rest. Diarrhea (40% of cases) typically resolves with anti-motility agents and dietary adjustments. Hypertension from VEGF inhibitors requires consistent monitoring and antihypertensive medication in 45% of patients.
⚠️ What This Means For You: Advanced kidney cancer no longer equals terminal diagnosis. With seven FDA-approved first-line regimens and four second-line options approved since 2019, sequential therapy strategies keep disease controlled for years. When first-line treatment stops working, second-line options deliver response rates of 30-50%—buying time for third-line agents in development.
Finding the Right Specialist & Taking Action
Choosing a Kidney Cancer Specialist
Jennifer Walsh’s Stage 3 kidney cancer required immediate decisions after her October 2025 diagnosis. Her community oncologist recommended radical nephrectomy, but a kidney cancer second opinion at Memorial Sloan Kettering revealed she qualified for partial nephrectomy plus adjuvant immunotherapy—preserving 60% of her kidney function while achieving identical cancer control.
The kidney cancer specialist you select dramatically influences outcomes beyond survival statistics. It determines surgical technique, access to clinical trials, and whether you receive 2026 cutting-edge treatments or 2019 protocols.
Essential Specialist Qualifications:
- Urologic oncologists: Surgeons specializing in kidney/urinary cancers (ideal for Stage 1-2 requiring surgery)
- Medical oncologists with GU focus: Experts in systemic therapies for advanced kidney cancer (critical for Stage 3-4)
- Volume requirements: Surgeons performing 30+ kidney cancer surgeries annually demonstrate 40% lower complication rates
- NCI-designated cancer centers: Institutions with comprehensive programs offer multidisciplinary tumor boards reviewing every case
- Clinical trial access: Centers running 5+ active kidney cancer trials provide options when standard treatments fail
Kidney cancer patients treated at high-volume centers (100+ cases annually) survive 12-18 months longer than those at low-volume facilities—making travel for initial consultation and surgery a life-extending investment even with associated costs.
When to Seek Kidney Cancer Second Opinion
Mandatory Second Opinion Scenarios:
- Any Stage 3-4 diagnosis before starting treatment
- Recommendation for radical nephrectomy when tumor is under 7 cm
- Recurrence after initial treatment
- Rare subtypes (collecting duct, medullary, sarcomatoid features)
- Poor response to first-line therapy after 3 months
Second opinions change treatment plans in 37% of kidney cancer cases—switching from radical to partial surgery, adding immunotherapy to surgery-alone plans, or identifying clinical trial eligibility missed by community oncologists.
Kidney Cancer Awareness & Support
Orange represents kidney cancer awareness during March (Kidney Cancer Awareness Month). The Kidney Cancer Association provides free resources including treatment decision guides, financial assistance navigation, and peer mentorship connecting newly diagnosed patients with long-term survivors.
Support group participation correlates with 25% better treatment adherence and measurably improved quality of life scores. Virtual groups eliminate geographic barriers, meeting weekly via video platforms with 20-40 participants sharing experiences navigating identical challenges.
Your Action Plan: Next Steps
If You Have Symptoms Right Now:
Within 48 Hours:
- Document symptom frequency—photograph bloody urine, track pain intensity (1-10 scale), record weight changes
- Schedule urgent care or primary care appointment stating “blood in urine requiring imaging workup”
- Request urinalysis with microscopy and renal function panel (creatinine, BUN)
- Demand imaging referral—CT urogram with and without contrast is gold standard
Within 1 Week:
5. Complete imaging studies before symptoms potentially disappear (intermittent hematuria common)
6. If mass detected, request referral to urologic oncologist within 5 business days
7. Avoid “watchful waiting” for solid masses over 3 cm—98% are malignant
If Recently Diagnosed with Kidney Cancer:
Week 1-2 Actions:
- Obtain complete medical records including pathology report, imaging CDs, and operative notes
- Schedule second opinion at nearest NCI-designated comprehensive cancer center
- Request tumor genomic testing (Foundation One, Tempus) to identify targetable mutations
- Research clinical trials at ClinicalTrials.gov using search terms “renal cell carcinoma [your stage]”
- Verify insurance pre-authorization requirements for out-of-network specialist consultations
Week 3-4 Actions:
6. Compare treatment recommendations from two institutions—document rationale for differences
7. Ask about partial nephrectomy eligibility even if first surgeon recommended radical approach
8. For Stage 3-4 disease, request IMDC risk score calculation determining immunotherapy combination selection
9. Join kidney cancer support community within 30 days of diagnosis
10. Discuss fertility preservation if under age 45 and planning future children (chemotherapy/immunotherapy can affect fertility)
If Currently in Treatment:
Ongoing Monitoring:
- Track side effects using smartphone apps or journals—report new symptoms within 48 hours
- Attend ALL surveillance imaging appointments (82% of recurrences caught by scheduled scans, only 18% by symptoms)
- Request tumor marker testing (LDH, corrected calcium) every 3 months during first 2 years
- Discuss immunotherapy maintenance beyond standard 24-month duration if achieving complete response
- Participate in survivorship programs addressing long-term effects (fatigue, cardiovascular risk, mental health)
Red Flags Requiring Immediate Contact:
- New persistent cough or shortness of breath (lung metastasis concern)
- Bone pain not relieved by standard pain medication (skeletal metastasis)
- Severe headache with vision changes (brain metastasis—requires emergency evaluation)
- Jaundice or right upper quadrant pain (liver involvement)
- Sudden severe fatigue preventing daily activities (anemia from progression)
Final Thoughts: You Are Not a Statistic
Kidney cancer survival statistics represent averages of thousands of patients diagnosed years ago with outdated treatments. Your individual outcome depends on tumor biology, treatment response, and access to innovation—variables no database fully captures.
The 2026 landscape offers unprecedented hope: seven first-line combination regimens, breakthrough imaging detecting millimeter-sized recurrences, and genomic profiling personalizing therapy selection. Patients diagnosed today access treatments unavailable to those in survival statistics published just 24 months ago.
Take control of your journey. Question every recommendation, seek multiple opinions for complex decisions, and remember that “average” survival includes patients who received no treatment, had multiple comorbidities, or lacked access to specialized care. Your outcome can exceed predictions.
⚠️ MEDICAL DISCLAIMER
This article provides educational information about kidney cancer symptoms, diagnosis, treatment options, and prognosis for informational purposes only. It does not constitute medical advice and should not replace consultation with qualified healthcare professionals.
Kidney cancer diagnosis and treatment require individualized assessment by board-certified urologic oncologists and medical oncologists specializing in genitourinary malignancies. Treatment recommendations vary based on cancer stage, tumor histology, patient health status, and molecular characteristics requiring expert interpretation.
Always consult your physician before making medical decisions. Seek emergency care immediately if experiencing severe symptoms including gross hematuria with clots, uncontrolled pain, difficulty breathing, or neurological changes.
Frequently Asked Questions About Kidney Cancer
1. What is kidney cancer?
Kidney cancer occurs when malignant cells form in the kidney tubules. Renal cell carcinoma accounts for 90% of cases, with approximately 81,800 Americans diagnosed in 2026.
2. What are the early signs of kidney cancer?
Early kidney cancer symptoms include blood in urine (pink or red-colored), persistent flank or back pain below the ribs, and unexplained weight loss of 10-15 pounds. Many patients experience no symptoms until advanced stages, making screening crucial for high-risk individuals.
3. What is the survival rate for kidney cancer?
Stage 1 kidney cancer has a 93.3% five-year survival rate, Stage 2 is 82.7%, Stage 3 drops to 70.4%, and Stage 4 metastatic disease is 19.1%. Early detection dramatically improves outcomes.
4. What causes kidney cancer?
Kidney cancer risk factors include smoking (50% increased risk), obesity (24% higher risk per 5-point BMI increase), chronic high blood pressure, occupational chemical exposure, and hereditary genetic syndromes like Von Hippel-Lindau disease. Men develop kidney cancer 1.7 times more often than women.
5. How is kidney cancer treated in 2026?
Treatment options include partial or radical nephrectomy surgery for localized disease, combination immunotherapy (pembrolizumab plus axitinib showing 73% response rates), targeted therapies blocking tumor blood supply, and emerging HIF-2α inhibitors. Stage determines optimal approach.
6. How is kidney cancer diagnosed?
Kidney cancer diagnosis involves CT scan with contrast (gold standard detecting tumors as small as 5mm), MRI for high-risk patients, and occasionally core needle biopsy. Blood tests, urinalysis, and physical examination support imaging findings.
7. What are the stages of kidney cancer?
Stage 1: Tumor ≤7cm confined to kidney. Stage 2: Tumor >7cm confined to kidney. Stage 3: Cancer invades nearby tissue or lymph nodes. Stage 4: Distant metastases to lungs, liver, bones, or brain.
8. Can kidney cancer be prevented?
Reducing kidney cancer risk involves maintaining healthy BMI (20-25), quitting smoking (reduces risk by 40%), controlling blood pressure below 130/80 mmHg, limiting occupational carcinogen exposure, and genetic screening for hereditary syndromes. Regular exercise and balanced diet also help.
9. Is kidney cancer hereditary?
Five to eight percent of kidney cancer cases stem from inherited genetic mutations including Von Hippel-Lindau disease, hereditary papillary renal carcinoma, and Birt-Hogg-Dubé syndrome. First-degree relatives of kidney cancer patients have 4-5 times higher risk.
10. How long is kidney cancer recovery after surgery?
Partial nephrectomy requires 1-2 weeks recovery with return to normal activities in 3-4 weeks. Radical nephrectomy typically needs 3-4 weeks initial recovery with 6-8 weeks before full activity resumption. Robotic-assisted surgery reduces recovery time by 50%.
11. When should I see a doctor about kidney cancer symptoms?
See a doctor within 48 hours if experiencing blood in urine plus back pain, unexplained fever, or weight loss lasting more than two weeks. Visible blood in urine (hematuria) requires imaging evaluation even without pain, as early kidney cancer rarely causes discomfort.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











