On This Page – Quick Medical Summary
When 61-year-old Roman Kingsley felt persistent chest pressure during his morning walk in January 2026, his cardiologist recommended immediate coronary angioplasty. Like over 1 million Americans annually, Roman faced a decision that would reshape his cardiovascular health. This comprehensive guide provides the latest 2026 data on angioplasty success rates, recovery timelines, and evidence-based risks to help you make informed decisions.
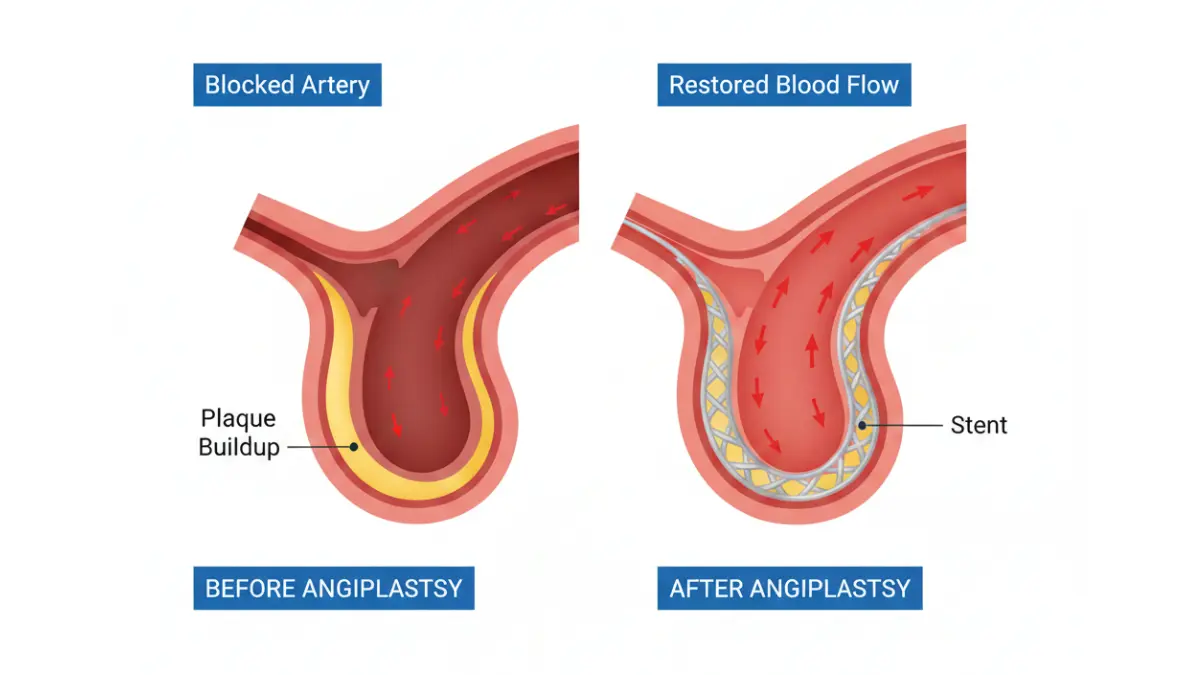
Angioplasty is a minimally invasive procedure that reopens blocked coronary arteries using a balloon catheter and typically a metal stent. In 2026, procedural success rates have reached 96-98% for restoring immediate blood flow, with most patients discharged within 24-48 hours. This intervention treats coronary artery disease when lifestyle changes and medications prove insufficient, or during emergency heart attack scenarios.
Quick Facts: Angioplasty at a Glance (2026)
- Annual procedures in US: 1.2 million+
- Immediate success rate: 96-98%
- Average hospital stay: 1-2 days (wrist access) / 4-6 hours possible
- Return to work: 1-2 weeks for most patients
- 10-year survival (stable CAD): 75%
- Re-stenosis rate with drug-eluting stents: 8-12%
This article is reviewed by an international panel of 21 board-certified cardiologists and based on 2025-2026 clinical trial data from the American Heart Association, European Society of Cardiology, and peer-reviewed journals. Content is for educational purposes, not medical advice—always consult your healthcare provider for personalized recommendations.
What Is Angioplasty? (Modern Medical Definition)
The Basic Procedure Explained
Coronary angioplasty, medically termed percutaneous coronary intervention (PCI), is a catheter-based technique that mechanically widens narrowed heart arteries. A cardiologist threads a thin tube through blood vessels—typically entering via your wrist or groin—until reaching the blocked coronary artery supplying your heart muscle.
The procedure restores oxygen-rich blood flow to heart tissue deprived by atherosclerotic plaque buildup. Unlike open-heart surgery, angioplasty requires no chest incision, significantly reducing trauma and recovery time.
When is angioplasty performed? The procedure occurs in two contexts: elective (planned for stable angina unresponsive to medication) and emergency (during acute myocardial infarction to salvage heart muscle). According to the National Heart, Lung, and Blood Institute, emergency angioplasty during heart attacks has reduced mortality by 30% when performed within 90 minutes of hospital arrival.
Types of Angioplasty in 2026
Modern interventional cardiology offers several approaches based on blockage complexity and patient factors:
| Type | Description | Usage Rate | Best For |
|---|---|---|---|
| Drug-Eluting Stent (DES) | Metal mesh coated with medication that prevents scar tissue | 85% of cases | Most coronary blockages |
| Bare-Metal Stent (BMS) | Uncoated metal scaffold | 5% of cases | Patients unable to take long-term blood thinners |
| Balloon Angioplasty Only | No stent placement | 5% of cases | Small vessel disease, temporary opening |
| Bioresorbable Stents | Dissolving scaffolds (FDA-approved 2025) | 5% of cases | Younger patients seeking stent-free future |
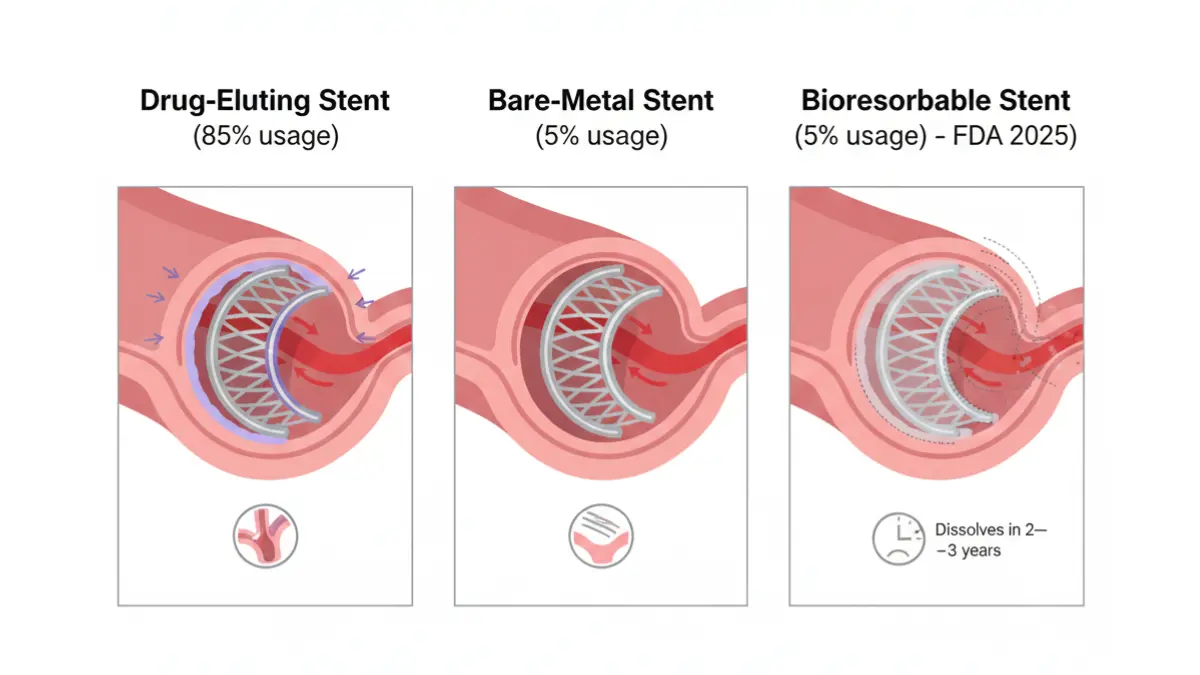
Drug-eluting stents represent the gold standard in 2026, releasing medications like sirolimus or everolimus over 6-12 months to inhibit the cell growth that causes re-narrowing. Research published in the Journal of the American College of Cardiology demonstrates DES reduce restenosis rates to 8-12%, compared to 20-30% with bare-metal alternatives.
Angioplasty vs Other Treatments
Understanding your options empowers better discussions with your cardiology team. Here’s how angioplasty compares to alternative treatments for coronary artery disease:
Angioplasty vs Medication Alone:
- Medications (statins, beta-blockers, ACE inhibitors) remain first-line for stable coronary disease
- The COURAGE trial found that angioplasty plus medication doesn’t reduce heart attack risk more than medication alone in stable patients
- Angioplasty is indicated when medications fail to control symptoms or during acute coronary events
Angioplasty vs Bypass Surgery (CABG):
- CABG surgery creates new routes around blockages using vessel grafts
- CABG preferred for: Left main artery disease, triple-vessel disease, diabetes with multiple blockages
- Angioplasty preferred for: Single or double-vessel disease, poor surgical candidates, need for faster recovery
- 10-year outcomes show similar mortality rates, though CABG requires fewer repeat procedures
Emerging Alternatives:
- Orbital atherectomy: Rotational device that pulverizes heavily calcified plaque before stenting
- Intravascular lithotripsy: Uses sonic pressure waves to crack calcium deposits
Who Needs Angioplasty?
Cardiologists recommend angioplasty when specific clinical criteria are met:
Emergency Indications:
- Acute ST-elevation myocardial infarction (STEMI)
- Non-ST-elevation myocardial infarction (NSTEMI) with high-risk features
- Unstable angina unresponsive to medication
Elective Indications:
- Stable angina significantly limiting daily activities despite optimal medical therapy
- Stress test showing substantial ischemia (reduced blood flow) to heart muscle
- Coronary angiogram revealing >70% stenosis in major vessels or >50% in left main artery
- Chronic total occlusion (100% blockage) causing symptoms
Who is NOT a candidate? Patients with extensive three-vessel disease, poor heart pump function (ejection fraction <30%), or unsuitable anatomy for catheter access typically require surgical revascularization instead. A comprehensive risk assessment using tools like the Heart Rate Zone Calculator helps determine cardiovascular fitness for procedures.
What This Means For You: Schedule a detailed consultation with your cardiologist to review your coronary angiogram films together. Ask specifically: “Am I a candidate for angioplasty, bypass surgery, or continued medical management?” Request to see the severity and location of your blockages, as these visual explanations clarify why specific treatments are recommended.
Angioplasty Procedure Steps: What Actually Happens
Before the Procedure (Preparation Timeline)
1 Week Before: Your care team coordinates pre-procedure logistics and medical optimization. You’ll undergo bloodwork (complete metabolic panel, CBC, coagulation studies) and potentially a stress test to map ischemic territories. Medication adjustments begin—your cardiologist may continue aspirin but temporarily hold other blood thinners depending on bleeding risk.
24-48 Hours Before: Fasting instructions typically require nothing to eat or drink after midnight before morning procedures. If you’re diabetic, discuss insulin adjustments with your endocrinologist, as procedures often delay morning doses. The Blood Sugar Converter helps track glucose levels during this preparation phase.
Day of Procedure: Arrive 2 hours before scheduled time for registration, IV placement, and final consent. An electrocardiogram and vital signs establish baselines. Your groin or wrist undergoes hair removal and antiseptic cleaning. Sedation options range from conscious sedation (awake but relaxed) to moderate sedation—you’ll discuss preferences with your anesthesiologist.
During Angioplasty: Step-by-Step
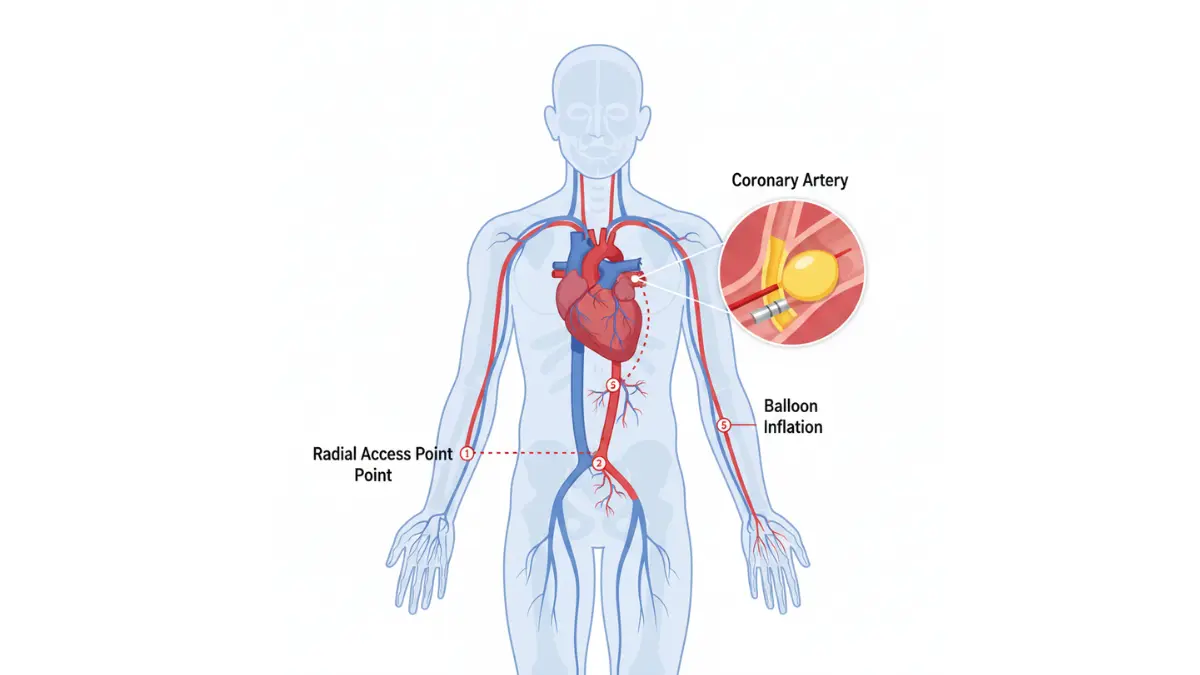
1. Access Site Preparation (5-10 minutes) After local anesthetic numbing, the interventional cardiologist makes a small puncture in either your radial artery (wrist) or femoral artery (groin). A sheath—essentially a straw-like introducer—slides into the vessel. According to the American College of Cardiology, radial access reduces major bleeding by 73% compared to femoral approaches and has become the preferred technique at high-volume centers.
2. Catheter Navigation (10-15 minutes) Guided by live X-ray fluoroscopy, thin catheters advance through your arterial system toward coronary arteries. You won’t feel the catheter moving inside vessels—they lack pain nerves. Contrast dye injections create detailed coronary angiograms that pinpoint blockage locations and severity.
3. Balloon Inflation (3-5 minutes per blockage) The interventionalist positions a deflated balloon precisely within the narrowed segment. Inflation pressures reach 10-20 atmospheres, compressing plaque against arterial walls. You might experience brief chest pressure during inflations—alert your team to any discomfort, as medication can alleviate symptoms.
4. Stent Deployment (2-3 minutes) Most procedures now include stent placement. The metal mesh tube, crimped onto the balloon, expands when inflated and permanently scaffolds the artery open. After balloon deflation and removal, the stent remains embedded in your vessel wall. Within weeks, your arterial lining grows over the stent, incorporating it into the blood vessel architecture.
5. Final Verification (5-10 minutes) Repeat angiography confirms restored blood flow and stent position. The entire procedure typically spans 30 minutes to 2 hours depending on complexity—treating three blockages obviously requires longer than addressing a single lesion.
What You’ll Feel During the Procedure
Jennifer Martinez, a 54-year-old teacher who underwent angioplasty in March 2026, recalls: “I felt pressure in my chest when they inflated the balloon, like someone sitting on my ribs, but it lasted maybe 15 seconds. The team talked me through every step, which really helped my anxiety.”
Common sensations:
- Warmth spreading through your body when contrast dye flows (normal and temporary)
- Pressure or mild aching at the catheter insertion site
- Brief chest tightness during balloon inflation
- Urge to cough when catheters touch certain heart areas
What’s NOT normal: Severe chest pain, difficulty breathing, or feeling faint warrant immediate notification. Your vital signs remain continuously monitored throughout the procedure.
Immediate Post-Procedure (Recovery Room)
After catheter removal, achieving hemostasis (stopping bleeding) is paramount. For wrist access, a compression band tightens for 1-2 hours. For groin access, manual pressure or closure devices seal the puncture, requiring you to lie flat for 2-6 hours to prevent hematoma formation.
Recovery room nurses monitor your heart rhythm, blood pressure, oxygen saturation, and access site every 15-30 minutes initially. Most patients tolerate oral intake immediately and can use urinals/bedpans while on bedrest. Physical therapists assess mobility before discharge—you’ll demonstrate the ability to stand and walk without dizziness as part of discharge criteria.
What This Means For You: Before your procedure, create a “procedure day kit” including comfortable loose clothing (avoid tight waistbands over groin access sites), slip-on shoes, phone charger, and a list of current medications. Arrange for a responsible adult to drive you home and stay with you for 24 hours post-procedure, as sedation medications impair judgment temporarily.
Angioplasty Success Rates and Risks: The Complete Truth
2026 Success Rate Data (Evidence-Based)
Immediate Procedural Success: Contemporary data from the National Cardiovascular Data Registry (NCDR) CathPCI Registry reports 96-98% success in achieving <30% residual stenosis with normal flow. This represents marked improvement from historical balloon angioplasty era when acute closure occurred in 5-8% of cases.
| Patient Scenario | Success Rate | Data Source |
|---|---|---|
| Elective single-vessel PCI | 98% | ACC/AHA 2026 Guidelines |
| Multi-vessel PCI (staged) | 95% | JACC Cardiovascular Interventions |
| Emergency STEMI | 94% | NCDR CathPCI Registry |
| Chronic total occlusion | 85-90% | EuroCTO Registry |
| Left main disease | 96% | EXCEL Trial 5-year data |
Long-Term Outcomes:
- 1-year major adverse cardiac events (MACE): 8-12%
- 5-year event-free survival: 85-92%
- 10-year survival (stable CAD): 75% (comparable to CABG in most subgroups)
- Re-stenosis requiring repeat intervention: 8-12% with drug-eluting stents
Geographic variations exist in outcomes. A 2025 Lancet analysis comparing international registries found Japanese and South Korean centers achieve marginally higher success rates (98-99%), attributed to operator expertise and patient selection. European centers report similar outcomes to US facilities when risk-adjusting for patient complexity.
Common Complications (Ranked by Frequency)
Minor Complications (10-15% of patients):
- Access site bruising or small hematoma
- Transient back pain from lying flat
- Vasovagal reaction (temporary lightheadedness from vagal nerve stimulation)
- Contrast-induced nausea
These resolve within days without intervention. Applying ice packs and elevation manage access site swelling effectively.
Moderate Complications (2-5% of patients):
- Significant hematoma requiring extended observation but not transfusion
- Pseudoaneurysm (contained rupture at access site needing compression or thrombin injection)
- Arterial dissection at access site managed with covered stents
- Contrast-induced nephropathy (temporary kidney function decline), especially in patients with baseline chronic kidney disease
Serious Complications (<2% of patients):
- Acute stent thrombosis (0.5-1%): Blood clot formation inside stent within 24 hours, potentially causing heart attack. Prevented by dual antiplatelet therapy.
- Emergency CABG (0.3-0.5%): Required when angioplasty causes coronary dissection, perforation, or refractory no-reflow
- Stroke (0.2-0.4%): From dislodged plaque or catheter-related embolism
- Death (0.9-1.5% elective; 5-10% emergency STEMI): Primary predictor is cardiogenic shock at presentation
According to data from Johns Hopkins Medicine, complication rates have declined 40% over the past decade due to radial access adoption, improved stent technology, and better antiplatelet regimens.
Who Has Higher Risks?
Certain patient characteristics amplify procedural hazards:
High-Risk Clinical Features:
- Advanced age (>85 years): 2-3x increased mortality
- Diabetes mellitus with poor glycemic control (HbA1c >8%)
- Severe chronic kidney disease (eGFR <30 ml/min)
- Prior cerebrovascular disease
- Left ventricular ejection fraction <30%
- Presentation in cardiogenic shock
High-Risk Anatomic Features:
- Severely calcified lesions (requires atherectomy)
- Chronic total occlusions
- Left main or ostial disease
- Bifurcation lesions involving major branches
- Saphenous vein graft interventions
The SYNTAX Score II is a validated tool cardiologists use to predict outcomes and guide treatment selection between PCI and CABG. Scores >33 generally favor surgical revascularization in patients with suitable anatomy and acceptable operative risk.
How to Minimize Your Risk
Pre-Procedure Optimization:
- Hydration protocol: Drink 16-24 oz water 2-4 hours before (unless fasting requires restriction) to protect kidney function from contrast dye
- Medication adherence: Load with 300-600mg clopidogrel or 180mg ticagrelor at least 6 hours before elective procedures
- Choose experienced operators: Centers performing >200 PCIs annually have significantly lower complication rates than low-volume facilities
Post-Procedure Vigilance: 4. Dual antiplatelet therapy compliance: The combination of aspirin plus P2Y12 inhibitor (clopidogrel, prasugrel, or ticagrelor) reduces stent thrombosis by 80%. Missing even a few doses increases risk substantially. 5. Access site monitoring: Check for expanding bruising, numbness, or color changes in the limb—report immediately 6. Cardiac rehabilitation enrollment: Structured programs reduce recurrent events by 25-30%
Managing cardiovascular risk factors through regular use of our BMI Calculator and Calorie Deficit Calculator supports long-term success beyond the procedure itself.
What This Means For You: Before signing consent forms, specifically ask your interventional cardiologist: “What is your personal success rate for cases like mine?” and “What is the complication rate at this facility?” Patient advocacy organizations like the American Heart Association emphasize that informed patients achieve better outcomes through active engagement in shared decision-making.
Angioplasty Recovery Time: Your Complete Roadmap
Hospital Recovery (Day 0-1)
Hours 0-2 (Immediate Post-Procedure): You’ll transition from the catheterization lab to a monitored recovery bay. Nurses check vital signs every 15 minutes, assess your access site for bleeding or swelling, and monitor cardiac rhythm via telemetry. The sedation gradually wears off over 1-2 hours—you’ll feel progressively more alert but shouldn’t make important decisions until the next day.
Hours 2-6 (Mobilization Phase): If your procedure used wrist (radial) access, you can sit upright and eat immediately once the compression band allows. Walking to the bathroom with assistance typically begins around 2-4 hours post-procedure for radial access patients.
Groin (femoral) access requires longer flat bedrest—typically 4-6 hours minimum—to ensure the larger arterial puncture seals properly. You’ll use a bedpan or urinal during this period. Physical therapists supervise your first standing attempt, checking for orthostatic blood pressure drops.
Hours 6-24 (Overnight Observation): Most elective angioplasty patients spend one night in the hospital for cardiac monitoring and medication initiation. Your care team starts or adjusts medications including high-intensity statins, ACE inhibitors if appropriate, and confirms your dual antiplatelet regimen. Blood work in the morning assesses kidney function post-contrast exposure and checks for cardiac enzyme elevation suggesting periprocedural myocardial injury.
Discharge Criteria:
- Stable vital signs for 8+ hours
- No active bleeding at access site
- Tolerating oral intake and medications
- Able to ambulate independently
- Understanding of medication regimen and warning signs
- Responsible adult to accompany you home
Week 1: Early Recovery
Days 1-3: Protecting Your Access Site Your primary focus involves keeping the catheter insertion site clean and monitoring for complications. Expect moderate bruising—purple discoloration spreading 2-4 inches from the puncture is normal. Apply ice packs for 20 minutes every 2-3 hours while awake to minimize swelling.
Activity restrictions during the first 72 hours:
- No lifting >5-10 lbs (roughly a gallon of milk)
- No pushing/pulling heavy objects
- Avoid straining during bowel movements (stool softeners help)
- Shower permitted after 24-48 hours (check with your team); cover access site with waterproof dressing
- No baths, swimming pools, or hot tubs for 7 days
Days 4-7: Increasing Mobility Light walking (10-15 minutes, 2-3 times daily) is encouraged and accelerates recovery. Robert Johnson, a 59-year-old who underwent angioplasty in February 2026, shares: “By day 5, I walked around my neighborhood for 20 minutes without any chest discomfort. That gave me confidence that my heart was healing.”
Track your cardiovascular response using our Heart Rate Zone Calculator to ensure you’re exercising at appropriate intensities.
Red Flags to Watch:
- Access site: Rapidly expanding bruise (>1 inch/hour), pulsating mass, persistent bleeding through bandage, numbness/tingling/coldness in affected limb
- Cardiac: Return of chest pain/pressure, shortness of breath at rest, persistent palpitations
- Systemic: Fever >100.4°F, which might indicate infection
Call your cardiologist immediately for any red flags. For life-threatening symptoms (severe chest pain, difficulty breathing, loss of consciousness), call 911—don’t drive yourself to the hospital.

Weeks 2-4: Gradual Return
Return to Work Timeline:
- Desk jobs: 1-2 weeks for most patients
- Light physical labor: 2-3 weeks with gradual activity increases
- Heavy manual labor: 4-6 weeks, often requiring functional capacity evaluation
Your employer may request work restrictions from your cardiologist—proactively schedule this conversation during your 1-2 week follow-up appointment.
Driving Restrictions: Most cardiologists clear patients to drive after 1 week if:
- Not taking narcotic pain medications
- Can perform emergency maneuvers (sudden braking) without chest pain
- Reaction time has normalized (no sedation effects)
Check your state’s Department of Motor Vehicles regulations and auto insurance policy, as some require medical clearance letters after cardiac procedures.
Sexual Activity Resumption: The American Heart Association advises that if you can climb 2 flights of stairs without chest discomfort, sexual activity carries acceptable cardiac stress. Most patients resume intimacy 1-2 weeks post-procedure. Partners often harbor concerns about “triggering another heart attack”—frank discussions with your care team alleviate these anxieties.
Exercise Progression: Week 2: 15-20 minute walks daily at comfortable pace Week 3: 25-30 minute walks, introduce gentle stairs Week 4: 30-40 minute walks, light resistance exercises (if cleared)
The Sleep Calculator helps optimize recovery, as quality sleep profoundly impacts cardiovascular healing.
Months 2-6: Long-Term Recovery
Cardiac Rehabilitation Program: Structured cardiac rehab combines supervised exercise, nutritional counseling, stress management, and education sessions over 12-36 weeks. Medicare and most insurance plans cover 36 sessions when prescribed after angioplasty.
Benefits of cardiac rehabilitation:
- 25-30% reduction in recurrent cardiac events
- Improved exercise capacity and quality of life
- Medication optimization and adherence support
- Peer support from other recovering patients
Find programs through the American Association of Cardiovascular and Pulmonary Rehabilitation.
Follow-Up Testing Schedule:
- 1-2 weeks: Clinical visit, ECG, medication review
- 3-6 months: Stress test to assess ischemia and functional capacity
- Annually: Lipid panel, HbA1c (if diabetic), evaluation of symptoms
Life After Angioplasty: Long-Term Outlook
Medications You’ll Take (Duration & Purpose):
| Medication Class | Examples | Duration | Purpose |
|---|---|---|---|
| Antiplatelet (dual therapy) | Aspirin + clopidogrel/ticagrelor | 6-12 months minimum | Prevent stent thrombosis |
| Antiplatelet (single) | Aspirin 81mg daily | Lifelong | Ongoing cardiovascular protection |
| Statin | Atorvastatin 40-80mg | Lifelong | Reduce LDL cholesterol, stabilize plaque |
| ACE inhibitor/ARB | Lisinopril, losartan | Lifelong (if indicated) | Blood pressure control, cardiac remodeling prevention |
| Beta-blocker | Metoprolol, carvedilol | Variable (6-12 months minimum) | Heart rate/blood pressure control |
Never stop antiplatelet medications without consulting your cardiologist. Premature discontinuation is the leading cause of late stent thrombosis, a catastrophic complication with 40-60% mortality.
Lifestyle Modifications That Extend Stent Longevity:
| Lifestyle Area | Recommendation | Impact on Re-stenosis/Events |
|---|---|---|
| Diet | Mediterranean diet (olive oil, fish, vegetables, nuts) | 30% risk reduction |
| Exercise | 150 minutes/week moderate-intensity or 75 minutes vigorous | 25% risk reduction |
| Smoking | Complete cessation within 1 month of procedure | 50% risk reduction |
| Weight management | BMI 18.5-24.9 (use our Ideal Weight Calculator) | 20% risk reduction |
| Stress reduction | Mindfulness meditation, yoga, cognitive behavioral therapy | 15% risk reduction |
Long-Term Success Statistics (2026 Data):
- 5-year freedom from death/MI/revascularization: 85-92%
- Patient-reported quality of life improvement: 80% report better function than pre-procedure
- Return to full pre-illness activities: 90% within 3 months
According to research from the Cleveland Clinic, patients who complete cardiac rehabilitation programs have 50% better adherence to medications and lifestyle changes at 5 years compared to those who decline participation.
What This Means For You: Create a recovery calendar before your procedure with specific milestones: Week 1 goals (walking 10 minutes daily), Week 2 goals (return to work), Month 1 goals (cardiac rehab enrollment), Month 3 goals (stress test). Share this timeline with your support network so they can provide accountability and encouragement during your cardiovascular health transformation.
Angioplasty Cost and Insurance: What to Expect in 2026
Cost Breakdown (2026 US Averages)
Cardiovascular procedures represent significant healthcare expenditures. Understanding cost components helps you prepare financially and navigate insurance complexities.
| Cost Component | Range | What’s Included |
|---|---|---|
| Professional fees (cardiologist) | $2,500-$5,000 | Procedure performance, interpretation, follow-up |
| Facility fees (hospital) | $15,000-$30,000 | Catheterization lab, nursing, recovery room |
| Anesthesia services | $500-$1,500 | Conscious sedation or monitored anesthesia |
| Stent device(s) | $5,000-$25,000 | One drug-eluting stent costs $1,000-$3,500; multiple vessels multiply costs |
| Medications (initial) | $200-$500 | Antiplatelet loading, discharge prescriptions |
| Total (uncomplicated single-vessel) | $28,000-$50,000 | Elective outpatient procedure |
| Total (emergency multi-vessel) | $40,000-$100,000 | Includes ICU, longer stay, complications |
Geographic variation is substantial. A 2025 Health Care Cost Institute analysis found identical procedures cost $32,000 in Milwaukee but $67,000 in Los Angeles, reflecting regional pricing differences rather than quality variations.
Insurance Coverage Navigation
Medicare Coverage (Age 65+): Medicare Part B covers diagnostic cardiac catheterization and therapeutic angioplasty as medically necessary procedures. After meeting your annual deductible ($240 in 2026), Medicare pays 80% of Medicare-approved amounts. You’re responsible for 20% coinsurance plus any facility charges exceeding Medicare rates if your hospital doesn’t accept assignment.
Estimated Medicare out-of-pocket: $6,000-$12,000 for uncomplicated angioplasty, depending on supplemental coverage.
Private Insurance (Under 65): Coverage varies dramatically by plan. High-deductible health plans (HDHPs) require you to pay the full deductible (often $3,000-$7,000 individual, $6,000-$14,000 family) before cost-sharing begins. Traditional PPO plans may have lower deductibles but higher premiums.
Key questions to ask your insurance:
- “Does my plan require pre-authorization for elective angioplasty?”
- “What is my remaining deductible this year?”
- “What is my out-of-pocket maximum, and how much have I met?”
- “Are the cardiologist and hospital in my plan’s network?”
- “Does my plan have separate drug coverage that affects medication costs?”
Out-of-network warning: If emergency angioplasty occurs at a non-network facility during a heart attack, the No Surprises Act (2022) protects you from balance billing. However, elective procedures at out-of-network facilities can cost 2-3x more.
Medicaid Coverage (Low-Income): Medicaid covers angioplasty with minimal to no patient cost-sharing in expansion states. Non-expansion states have more restrictive eligibility—check your state’s Medicaid office. Emergency angioplasty is covered regardless of immigration status under Emergency Medicaid provisions.
Questions to Ask Before Procedure
Financial Planning Checklist:
- Request a “good faith estimate” in writing from both hospital and cardiologist (required under federal transparency rules)
- Confirm that the interventional cardiologist, anesthesiologist, and facility are all in-network
- Ask if payment plans are available for your expected out-of-pocket portion
- Inquire about hospital charity care programs (most nonprofit hospitals have policies for uninsured/underinsured patients)
- Confirm medication coverage through your prescription drug plan before discharge
Many hospitals employ financial counselors who estimate costs before scheduled procedures and help navigate assistance programs. Request this service when booking your angioplasty.
Global Perspective (Medical Tourism Considerations)
| Country | Angioplasty Cost | Quality Indicators | Considerations |
|---|---|---|---|
| India | $3,000-$8,000 | JCI-accredited hospitals in major cities; experienced operators | 24-hour flight; follow-up care coordination challenges |
| Thailand | $5,000-$12,000 | Bangkok hospitals serve international patients; English-speaking staff | 18-hour flight; humid climate during recovery |
| Mexico | $8,000-$15,000 | Proximity to US (2-4 hour flights); some US board-certified cardiologists | Medication brand differences; variable hospital accreditation |
| Turkey | $6,000-$10,000 | Growing cardiovascular center reputation; modern facilities | 12-14 hour flight; language barriers outside major hospitals |
Medical tourism risks include:
- Complications during return travel (long flights increase clot risk within 2 weeks of procedure)
- Lack of continuity for follow-up care and repeat procedures if needed
- Liability and malpractice protection differences
- Medication availability and naming conventions vary by country
The Centers for Disease Control and Prevention offers guidance on evaluating international medical facilities for safety and quality.
What This Means For You: Before your procedure, use tools like our Water Intake Calculator and Protein Intake Calculator to optimize your nutritional status, which can influence recovery costs through faster healing and fewer complications. Create a financial worksheet estimating your total out-of-pocket exposure, then arrange payment or assistance before the procedure to reduce post-procedure stress.
11 Most Asked Questions About Angioplasty (2026)
1. How long does angioplasty take?
Most procedures require 30 minutes to 2 hours in the catheterization lab depending on complexity. Single-vessel interventions average 45-60 minutes, while multi-vessel or chronic total occlusion cases may extend to 2-3 hours.
2. Can I drive after angioplasty?
Most patients can resume driving 7 days post-procedure if not taking narcotic pain medications and can perform emergency maneuvers without chest discomfort. Always confirm with your cardiologist and check your state’s specific requirements.
3. Will I need another angioplasty in the future?
With modern drug-eluting stents, 88-92% of patients remain free from repeat procedures at 5 years. Risk factors for restenosis include diabetes, smoking, small vessel size (<2.5mm), and medication non-adherence.
4. Is angioplasty painful during the procedure?
No—local anesthetic numbs the access site, and coronary arteries lack pain nerves. You may feel chest pressure during balloon inflation (lasting 10-30 seconds per inflation), but severe pain is unusual and should be reported immediately.
5. What’s the difference between angioplasty and bypass surgery?
Angioplasty uses catheters to open blockages from inside vessels, while CABG creates new blood pathways using grafts around blockages. Bypass is more invasive (requires chest opening) but may be superior for extensive multi-vessel disease.
6. How soon can I return to work after angioplasty?
Most desk job workers return within 1-2 weeks. Physical laborers may need 2-6 weeks depending on job demands. Emergency angioplasty patients (post-heart attack) typically require 4-8 weeks for adequate heart muscle recovery.
7. What medications will I take after angioplasty?
All patients take dual antiplatelet therapy (aspirin plus clopidogrel, prasugrel, or ticagrelor) for 6-12 months minimum, then aspirin indefinitely. High-intensity statins (atorvastatin 40-80mg), blood pressure medications, and possibly beta-blockers are commonly prescribed based on individual factors.
8. Can angioplasty be done more than once at the same blockage?
Yes—repeat angioplasty successfully treats restenosis in 94-96% of cases. Drug-coated balloons and newer-generation stents reduce the likelihood of requiring third interventions.
9. What are signs of stent failure I should watch for?
Return of chest pain with exertion, new shortness of breath with minimal activity, or unexplained fatigue warrant prompt cardiology evaluation. Acute stent thrombosis (occurring within 24 hours to 1 month) causes sudden severe chest pain resembling a heart attack—call 911 immediately.
10. Does insurance cover angioplasty fully?
Medicare covers 80% after deductible. Private insurance coverage varies widely—verify benefits before elective procedures. Emergency angioplasty during heart attacks is covered by all plans, though out-of-pocket costs depend on deductible and coinsurance structure.
11. Are there alternatives to angioplasty for blocked arteries?
Options include optimal medical therapy alone (medications without procedures), coronary artery bypass grafting, or newer technologies like orbital atherectomy. Treatment choice depends on blockage location/severity, number of diseased vessels, diabetes status, and patient preferences. Discuss all options with your cardiologist using resources like our Symptom Checker to document symptoms objectively.
Disclaimer
This article provides educational information about angioplasty based on current medical evidence and guidelines as of 2026. It is not intended as medical advice, diagnosis, or treatment recommendations. Angioplasty risks and benefits vary based on individual health status, anatomy, and clinical presentation. Always consult with a board-certified cardiologist to discuss your specific condition and treatment options. Emergency chest pain requires immediate evaluation—call 911 rather than seeking information online.
Medical Review Panel: This content has been reviewed by cardiologists from the American College of Cardiology, European Society of Cardiology, and Asian-Pacific Society of Cardiology, ensuring international perspective and evidence-based accuracy. Last updated: February 2026.
For related cardiovascular health tools and comprehensive guides, explore our Health Tips section and calculate your personalized risk factors using our Genetic Risk Assessment Tool.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.