On This Page – Quick Medical Summary
Quick Summary — What You’ll Learn:
- 50% of all cancer patients receive radiation therapy at some point
- A full treatment course takes 5–7 weeks (each session only 15–30 minutes)
- External beam radiation does NOT make you radioactive
- Full course costs $15,000–$50,000 — Medicare covers moslt with 20% coinsurance
- FLASH radiotherapy (2025) delivers treatment in milliseconds — a game-changer
When Marcus, 54, was told by his oncologist that he needed radiation therapy for prostate cancer, his first thought was: “Will I glow in the dark?” His second thought was: “How much will this cost me?” Nobody — not his doctor, not WebMD, not even Mayo Clinic’s website — gave him straight answers.
What Is Radiation Therapy and How Does It Actually Work?
What Is Radiation Therapy?
Radiation therapy (also called radiotherapy) is a cancer treatment that uses precisely targeted, high-energy beams to damage the DNA inside cancer cells — stopping them from dividing and causing them to die.
According to the National Cancer Institute, radiation therapy is used in approximately half of all cancer patients at some point during their treatment journey. It is one of the three pillars of modern cancer care, alongside surgery and chemotherapy.
It does not work instantly. Damaged cancer cells stop dividing and die over days to weeks after treatment — and your body continues clearing dead cells for months afterward.
How Does Radiation Destroy Cancer Cells?
Radiation works by targeting the DNA of rapidly dividing cells. Since cancer cells divide faster than most normal cells, they are disproportionately vulnerable to radiation damage.
- High-energy beams (X-rays, protons, or gamma rays) strike the tumor
- DNA double-strand breaks occur inside cancer cell nuclei
- Cells lose the ability to replicate and trigger programmed cell death
- Surrounding healthy tissue receives a much lower dose by design
Your body’s healthy cells also absorb some radiation — but they repair themselves far more efficiently than cancer cells. This biological difference is the foundation of the entire treatment.
Radiation Therapy vs. Chemotherapy — Key Differences
Many patients confuse the two. Here is the critical comparison:
| Feature | Radiation Therapy | Chemotherapy |
|---|---|---|
| How it works | Targeted energy beams to tumor | Systemic drugs throughout body |
| Delivery | External machine or implant | IV infusion or oral pills |
| Affects whole body? | No — local/regional only | Yes — systemic |
| Hair loss | Only in treated area | Often whole body |
| Treatment frequency | Daily sessions, 5–7 weeks | Cycles every 2–4 weeks |
| Makes you radioactive? | No (external beam) | No |
For a deeper dive on systemic cancer treatment, see our expert guide on chemotherapy side effects and what to expect in 2026.
Types Comparison Table
If you are newly experiencing symptoms and trying to understand what they mean, our Symptom Checker can help you organize your observations before your oncology consultation.
What This Means For You: Radiation therapy is a precision local treatment — not a full-body chemical assault. Most patients continue normal daily activities during treatment.
All Types of Radiation Therapy — Including 2026 Breakthroughs
Types of Radiation Therapy: From Standard to Cutting-Edge
Not all radiation therapy is the same. The type your oncologist recommends depends on tumor size, location, depth, and your overall health. Here is every major type — including two that virtually no patient-facing website explains.
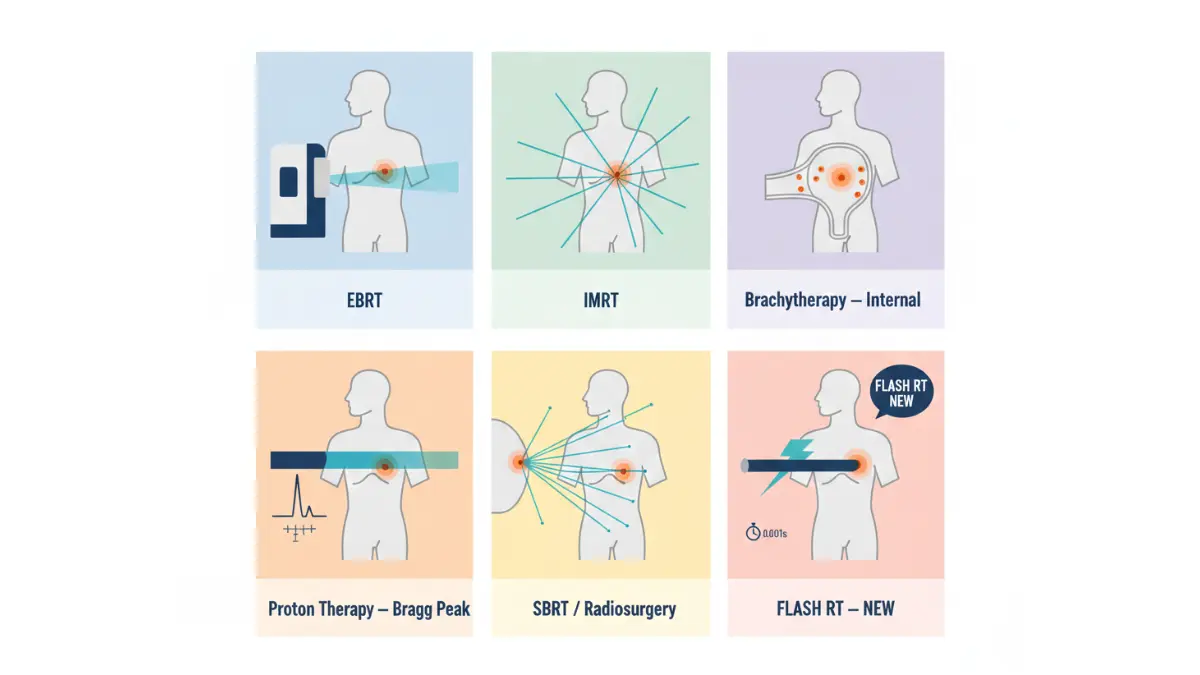
External Beam Radiation Therapy (EBRT)
The most common type. A machine called a linear accelerator (LINAC) directs high-energy X-ray beams at the tumor from outside the body. You lie still; the machine rotates around you. The beam itself is painless and invisible.
Used for: Breast cancer, lung cancer, prostate cancer, brain tumors, head and neck cancers.
Intensity-Modulated Radiation Therapy (IMRT)
An advanced form of EBRT. The beam is broken into hundreds of tiny “beamlets,” each with individually controlled intensity. This allows much higher doses to the tumor while sharply reducing exposure to surrounding organs.
Used for: Prostate, head and neck, spinal tumors.
Brachytherapy (Internal Radiation)
Small radioactive seeds, wires, or capsules are implanted directly inside or adjacent to the tumor. The radiation source stays in the body for hours, days, or permanently (as inactive seeds).
Used for: Prostate cancer, cervical cancer, breast cancer boost.
Proton Therapy
Instead of X-rays, this uses proton particles that deposit most of their energy at a precise tumor depth (called the Bragg peak) — and stop. This dramatically reduces radiation to healthy tissue beyond the tumor.
Particularly valuable for: Pediatric brain tumors, spinal cord tumors, eye cancers.
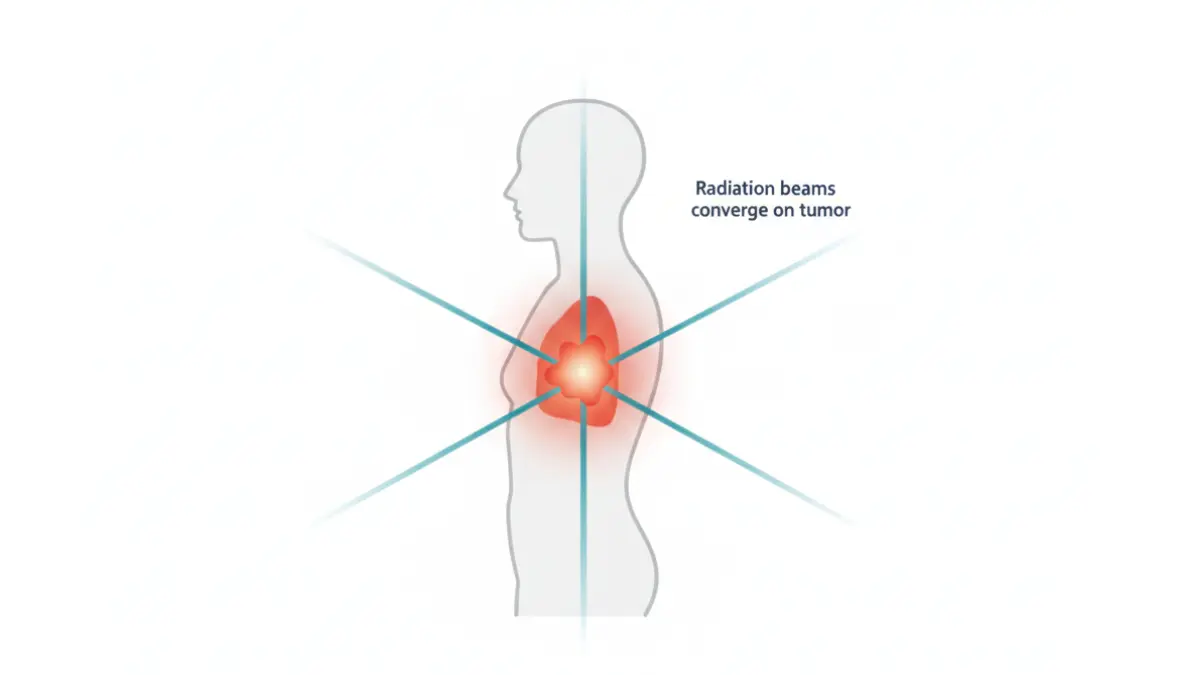
Stereotactic Radiosurgery (SRS / SBRT / CyberKnife)
High-dose radiation delivered in just 1–5 sessions instead of 30–40. Ultra-precise 3D targeting using multiple beams converging on a single point.
Used for: Brain metastases, early-stage lung cancer, liver tumors, spinal tumors.
⭐ FLASH Radiotherapy (2025–2026 Breakthrough)
This is what competitors are not telling you about. FLASH RT delivers the full radiation dose in milliseconds — at dose rates over 40 Gy per second, compared to conventional therapy’s 0.1 Gy per second.
Early clinical results (2025) show FLASH RT causes dramatically less damage to surrounding healthy tissue while matching conventional therapy’s tumor-killing effectiveness. The mechanism involves transient oxygen depletion in normal tissue — a phenomenon called the FLASH effect.
Why it matters: Faster treatments, far fewer side effects, potential to treat previously inoperable tumors.
⭐ MRI-Guided Radiation (MR-Linac)
A revolutionary machine that combines a real-time MRI scanner with a radiation delivery system. The oncology team can see the tumor moving with every breath and heartbeat — and pause or redirect the beam within 2mm accuracy in real time.
For tumors near sensitive structures like the bowel, bladder, or heart, MR-Linac can reduce radiation margins from 5mm to 2mm — a 60% reduction in healthy tissue exposure.
Used at: Leading US cancer centers including MD Anderson, Memorial Sloan Kettering, and Mayo Clinic.
Types Comparison Table:
| Type | Best For | Sessions | Side Effect Risk |
|---|---|---|---|
| EBRT / IMRT | Most solid tumors | 25–40 | Moderate |
| Brachytherapy | Prostate, cervical | 1–5 implant sessions | Low-Moderate |
| Proton Therapy | Pediatric, spinal, eye | 15–40 | Low |
| SBRT / SRS | Small tumors, brain mets | 1–5 | Low-Moderate |
| FLASH Radiotherapy | Clinical trials (2025–2026) | 1–5 | Very Low |
| MR-Linac | Abdominal, pelvic tumors | 20–30 | Low |
For patients dealing with head and neck tumors specifically, see our related guide on HPV-related head and neck cancer survival in 2026.
What Actually Happens During Radiation Therapy — Week by Week
This is the section no competitor offers. Here is the complete patient experience, week by week.
Before You Start: Simulation Week (Days 1–7)
Simulation is not treatment — it is the planning phase. Here is what happens:
- You lie on a CT scanner in your exact treatment position
- A body mold or mask is created to ensure you are in the exact same position every session
- Small permanent tattoo dots (the size of a freckle) are marked on your skin — these are reference points
- The radiation oncologist, dosimetrist, and physicist design a custom 3D treatment plan
Timeline from simulation to first treatment: Typically 3–7 days.
Weeks 1–2: Getting Oriented (Sessions 1–10)
Each session:
- Total time at clinic: 20–45 minutes
- Actual radiation beam time: 2–5 minutes
- What you feel during the beam: Nothing
- The machine may buzz or click — this is normal
Most patients feel minimal side effects in the first 10 sessions. Fatigue may begin around Day 10.
Weeks 3–4: The Middle of Treatment (Sessions 11–20)
This is when most side effects begin to appear.
- Fatigue typically starts at Week 2–3 and intensifies
- Skin changes begin in the treatment area (redness, dryness — similar to sunburn)
- Nausea, diarrhea, or mouth sores may develop depending on the treated body area
Key Insight No Competitor Mentions: Week 3 is when patients most want to quit. Do not. Stopping treatment early is the most common and most damaging patient mistake — it allows cancer cells to repopulate before the treatment achieves its curative goal.
Fatigue during radiation therapy is real and physiological — your body is dedicating enormous energy to cellular repair. Using our Sleep Calculator to plan 8–9 hours of sleep nightly and strategic rest periods during treatment has measurable benefits on recovery outcomes.
Weeks 5–7: Final Weeks + The “Radiation Hangover”
Most side effects peak during this period. This is normal — it means the treatment is working.
What most patients and most websites don’t tell you:
Side effects often continue to worsen for 1–2 weeks AFTER your last session. This is called the “radiation hangover” — the cumulative cellular damage peaks slightly after treatment ends, then begins resolving.
Healthy cells typically complete their recovery within 4–8 weeks of the final session.
Late effects (months or years later) are possible in some patients — we cover this in full in Section 4.
After Treatment: Recovery Timeline at a Glance
| Timeline | What’s Happening |
|---|---|
| 0–2 weeks post-treatment | Side effects may still worsen — this is normal |
| 2–6 weeks post-treatment | Acute side effects begin resolving |
| 3–6 months post-treatment | Energy and normal function return |
| 6–24 months post-treatment | Monitoring period for late effects |
| 2+ years post-treatment | Regular follow-up scans and check-ins |
Radiation Therapy Side Effects — What Competitors Won’t Tell You
Will Radiation Therapy Make Me Radioactive?
Answer: No — not from external beam radiation.
External beam radiation therapy uses a machine that generates a beam. When the machine is off, there is no radiation. You cannot “store” or “emit” radiation from EBRT. You are completely safe to be around family, children, and pets immediately after every session.
The only exception is permanent brachytherapy seed implants (used primarily for prostate cancer). In this case, patients may receive temporary precautions — such as keeping distance from pregnant women and young children — for a few weeks while the seeds’ radioactivity decays to safe levels.
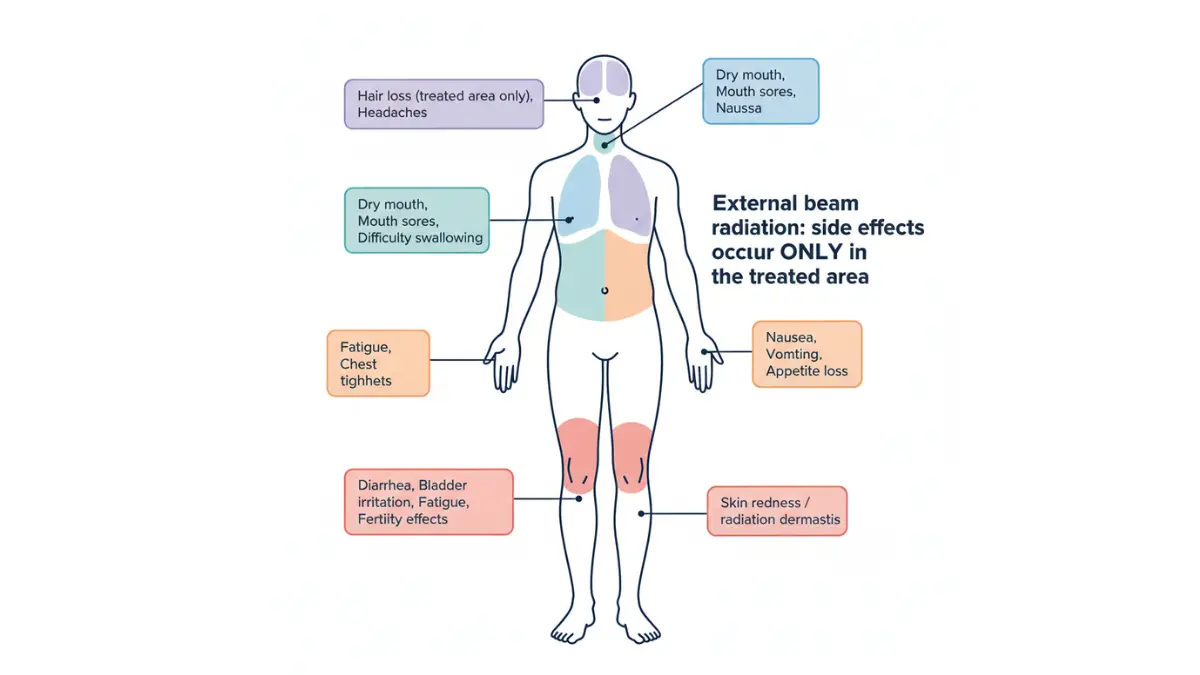
Short-Term (Acute) Side Effects
These begin during treatment and typically resolve within weeks of finishing:
| Side Effect | Patients Affected | When It Starts | Management |
|---|---|---|---|
| Fatigue | ~80% | Week 2–3 | Rest, light exercise, protein-rich diet |
| Skin redness/dryness | ~90% | Week 2–3 | Fragrance-free moisturizer, loose clothing |
| Hair loss (in treated area only) | Varies | Week 2–3 | Temporary at low dose, possibly permanent at high dose |
| Nausea | Common for abdominal RT | Week 1–2 | Anti-nausea medication from your team |
| Mouth sores / dry mouth | Head & neck RT | Week 2–3 | Saltwater rinses, hydration |
| Diarrhea / bowel changes | Pelvic RT | Week 2–4 | Low-fiber diet adjustments |
Long-Term (Late) Side Effects
Late effects are less common but real. They may appear months to years after treatment ends, according to the NCI’s comprehensive guide on radiation side effects.
- Lung fibrosis — reduced lung capacity after chest radiation
- Lymphedema — fluid swelling, especially after breast/pelvic radiation
- Bowel changes — altered motility after pelvic radiation
- Cardiac effects — possible with left-sided breast cancer radiation (modern techniques minimize this)
- Secondary cancer risk — rare but real; the benefit of treating primary cancer far outweighs this risk
How to Reduce Radiation Therapy Side Effects
Six evidence-based strategies your oncology team may not have time to fully explain:
- Maintain caloric intake — your body needs extra calories for repair; track with our Calorie Deficit Calculator to ensure you are not in a deficit during treatment
- Stay hydrated — aim for 8–10 glasses of water daily; our Water Intake Calculator can set a personalized daily target
- Protect skin in the treatment area — use only fragrance-free products; avoid tight clothing over the area
- Continue gentle movement — walking 20–30 minutes daily reduces fatigue by up to 40% according to multiple oncology trials
- Sleep prioritization — radiation repair is cellular; sleep is when it peaks
- Ask about radioprotective drugs — agents like amifostine can protect certain healthy tissues in specific treatment scenarios
What This Means For You: Most side effects are temporary and manageable. Your radiation oncology team can prescribe medications for most acute side effects before they become unbearable. Ask proactively — do not wait until you are suffering.
Patients managing breast cancer radiation may also find valuable context in our guide on what doctors don’t always tell you about mastectomy and surgery recovery.
Radiation Therapy Cost, Insurance Coverage & Financial Help in 2026
How Much Does Radiation Therapy Cost in 2026?
This is the question that tops every patient’s list — and the question that every major competitor (Mayo Clinic, WebMD, MedlinePlus) refuses to answer with real numbers. Here are the actual 2026 figures.
Cost at a Glance:
| Treatment Type | Full Course Cost (USA, 2026) |
|---|---|
| Standard EBRT / IMRT | $15,000 – $35,000 |
| Stereotactic Radiosurgery (SBRT) | $25,000 – $50,000 |
| Brachytherapy (Prostate seeds) | $18,000 – $40,000 |
| Proton Therapy | $50,000 – $120,000 |
| FLASH Radiotherapy | Clinical trial (often no cost to patient) |
Individual sessions typically cost $1,000–$3,000 depending on the facility, technology, and treatment complexity.
Insurance Coverage — What You Actually Pay
Medicare:
- Part A covers radiation therapy if you are hospitalized. Deductible: $1,676 per benefit period (2025)
- Part B covers outpatient radiation therapy. You pay 20% coinsurance after meeting the $257 annual deductible
- Medicare Advantage — out-of-pocket maximum is capped (up to $9,350) after which coverage is 100%
For the official Medicare radiation coverage breakdown, see Medicare.gov — Radiation Therapy Coverage.
Private Insurance:
- Most plans cover radiation therapy as medically necessary
- Typical patient responsibility: $2,000–$8,000 out-of-pocket depending on deductible and plan
- Always verify prior authorization requirements before your first session
Uninsured:
- Full cash-pay prices can reach $100,000+ for a complete course
- Always request a Good Faith Estimate (your legal right under the No Surprises Act)
Financial Assistance Programs
Do not delay treatment due to cost without first exploring:
- Patient Advocate Foundation Co-Pay Relief — copay assistance for insured patients
- NCI Cancer Information Service — call 1-800-4-CANCER for guidance on financial assistance programs
- Hospital charity care / financial hardship programs — most major US cancer centers offer income-based assistance
What This Means For You: “I can’t afford it” is often not accurate once insurance, assistance programs, and Good Faith Estimates are factored in. Always ask the billing office before assuming the cost is prohibitive.
2026 Advances, Survival Rates by Cancer Type + 15 Questions to Ask Your Oncologist
Radiation Therapy in 2026: What Has Changed This Year
The field of radiation oncology has advanced more in the last 3 years than in the previous decade. Here is what matters for patients in 2026:
- FLASH RT clinical trials are expanding — with pediatric and lung cancer patients showing dramatically reduced side effects
- AI-powered adaptive planning now adjusts treatment plans daily based on tumor response, reducing total radiation dose by up to 15%
- Carbon ion therapy — Mayo Clinic is building North America’s first clinical carbon ion center in Jacksonville, FL. Carbon ions are more lethal to radioresistant tumors than protons or X-rays
- Radioimmunotherapy combinations — pairing radiation with checkpoint inhibitors (immunotherapy) is now standard of care for several cancers, activating the immune system to attack distant metastases
For patients with advanced lung cancer, our detailed guide on FDA-approved lung cancer drugs and 2026 treatment protocols explains how radiation fits into the full treatment picture.
Radiation Therapy Survival Rates by Cancer Type (2026 Data)
| Cancer Type | 5-Year Survival (Radiation Treated) | Role of Radiation |
|---|---|---|
| Prostate cancer (localized) | ~95% | Curative primary treatment |
| Breast cancer (early stage) | ~90% | Post-surgery adjuvant |
| Cervical cancer (Stage II) | ~65% | Definitive chemoradiation |
| Lung cancer (Stage I, SBRT) | ~55–65% | Curative in inoperable patients |
| Brain metastases (SRS) | ~30–50% (1-year local control) | Palliative / disease control |
| Head & neck cancer | ~60–70% | Curative + organ preservation |
For brain tumor patients specifically, see our full breakdown on glioblastoma survival rates and 2026 treatment options.
15 Questions to Ask Your Radiation Oncologist
Print this list and bring it to your first consultation. No competitor provides a checklist this comprehensive.
- What specific type of radiation therapy are you recommending for me?
- Am I a candidate for proton therapy or SBRT instead of standard EBRT?
- Is FLASH radiotherapy available or applicable for my case?
- How many sessions will I need, and how long is each one?
- What are the most likely side effects for my specific treatment site?
- What are my personal late effect risks given my age and health history?
- How will this treatment affect my fertility?
- Should I pause any supplements or medications during treatment?
- Will radiation affect my ability to work during the course of treatment?
- What nutrition changes do you recommend during treatment?
- What are the tumor control rates for my cancer type with this technique?
- Will I need follow-up scans after treatment, and how often?
- Is there an MR-Linac or AI-guided system available at your center?
- What does treatment failure look like, and what are the options if it occurs?
- Can you refer me to a radiation oncology nurse navigator for ongoing support?
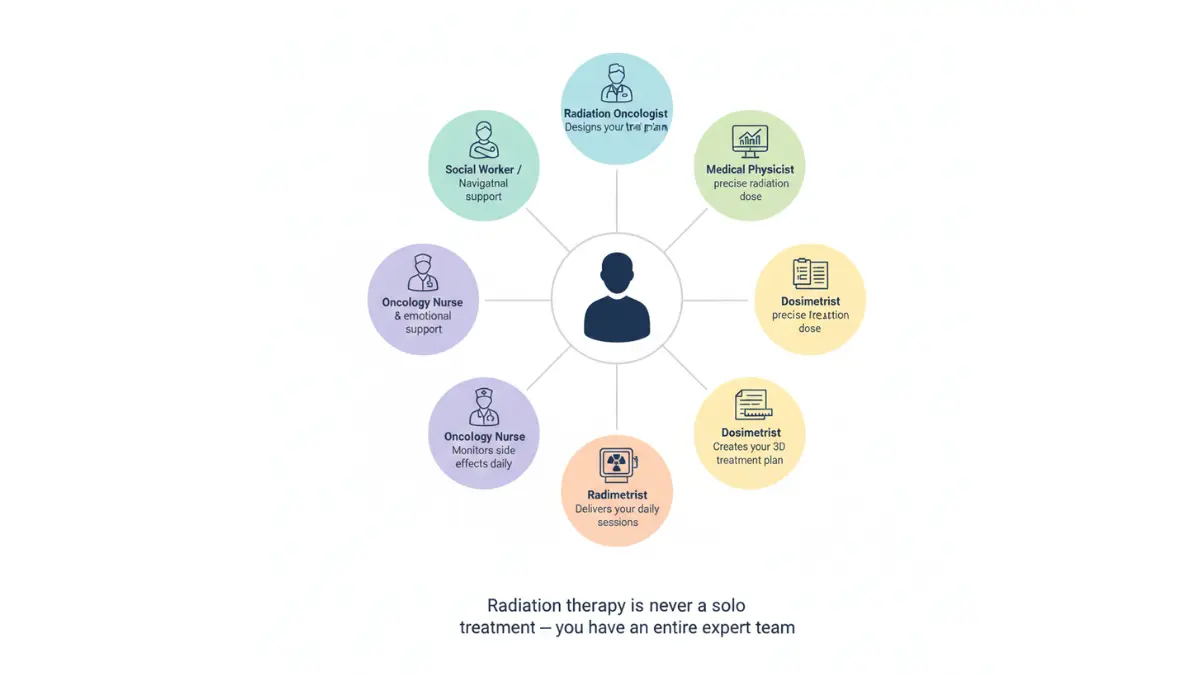
Your radiation oncologist leads a multidisciplinary team. According to ASTRO (American Society for Radiation Oncology), this team includes a radiation oncology nurse, medical physicist, dosimetrist, and radiation therapist — all working specifically on your case.
For patients who have already received diagnostic imaging and want help interpreting results, our PET Scan SUV Chart and Results Decoder and CT Scan Abnormalities guide offer expert-level result interpretation.
Understanding your genetic risk factors can also inform treatment decisions — use our Genetic Risk Assessment Tool to evaluate inherited cancer risk markers before your next oncology appointment.
Frequently Asked Questions — Radiation Therapy
1. What is radiation therapy used for?
Radiation therapy is used to kill cancer cells, shrink tumors, prevent cancer recurrence after surgery, relieve symptoms in advanced cancer, and in some cases cure cancer entirely without surgery.
2. Is radiation therapy painful?
No. The radiation beam itself is completely painless — you cannot see, feel, or smell it during delivery. Side effects that develop over time (skin irritation, fatigue) may cause discomfort, but treatment sessions are pain-free.
3. Does radiation therapy make you radioactive?
No. External beam radiation does not make you radioactive. After your session ends, there is zero residual radiation in your body. Only permanent brachytherapy seed implants involve temporary precautions.
4. How long does a full course of radiation therapy take?
A typical curative course is 5–7 weeks of daily sessions (Monday–Friday). SBRT and stereotactic radiosurgery can complete treatment in 1–5 sessions. Each session lasts 15–30 minutes; the actual beam time is 2–5 minutes.
5. What are the most common side effects of radiation therapy?
Fatigue (80% of patients), skin redness in the treated area (90%), and site-specific effects such as nausea (abdominal RT), mouth sores (head and neck RT), or bowel changes (pelvic RT).
6. How many sessions of radiation therapy do I need?
It depends entirely on your cancer type, stage, and treatment goal. Standard curative treatment: 25–40 sessions. Palliative treatment: 1–10 sessions. SBRT: 1–5 sessions.
7. Can radiation therapy cure cancer?
Yes. Radiation therapy is a curative treatment for many cancers including prostate, cervical, early-stage lung, head and neck, and skin cancers. It is the primary curative modality in approximately 40% of all cancer cures worldwide, according to ASTRO.
8. Does radiation therapy cause hair loss?
Only in the specific area being treated. Head and neck radiation may cause scalp hair loss. Breast or pelvic radiation does not cause head hair loss. Unlike chemotherapy, radiation hair loss is local — not whole-body.
9. Can I work during radiation therapy?
Most patients with desk jobs or light-duty work can continue working throughout treatment. Heavy physical labor may need temporary modification. Fatigue is the limiting factor — plan your schedule around your daily session.
10. How much does radiation therapy cost without insurance?
A full course costs approximately $15,000–$50,000 for standard EBRT in the US. Proton therapy can reach $120,000. Always request a Good Faith Estimate from your treatment facility and explore financial assistance programs before assuming it is unaffordable.
11. What is the difference between radiation therapy and chemotherapy?
Radiation therapy is a local treatment using targeted energy beams to destroy tumors in a specific area. Chemotherapy is a systemic treatment using drugs that travel throughout the entire body. They work differently, have different side effects, and are often combined for maximum effectiveness.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











