
On This Page – Quick Medical Summary
David, a 34-year-old teacher from Chicago, first noticed clumps of hair on his pillow in November. His scalp was covered in thick, silvery plaques — itchy, sore, and spreading toward his forehead. After two months of wrong diagnoses, a dermatologist confirmed what he feared: scalp psoriasis.
Scalp psoriasis can cause hair loss in up to 50% of patients — but in the vast majority of cases, hair grows back fully once inflammation is controlled. The key is understanding exactly why hair falls out, and acting fast with the right treatment.
What Is Scalp Psoriasis? (And Why It’s Not Just Dandruff)
Scalp psoriasis is a chronic autoimmune skin condition where the immune system misfires, driving skin cells to reproduce every 3–4 days instead of the normal 28–30 days. Those excess cells pile up on the scalp surface, forming the thick, scaly plaques this condition is known for.
It is not contagious. It is not caused by poor hygiene. And critically — it is not dandruff.
According to the National Psoriasis Foundation, 45–56% of all people living with psoriasis have scalp involvement, making it one of the most common — and most mismanaged — forms of the disease in the United States.
Who Gets Scalp Psoriasis?
- Adults between 15–35 and 50–60 (two peak onset windows)
- People with a family history of psoriasis
- Individuals under chronic stress, or who smoke or drink alcohol
- Those with other autoimmune conditions
Scalp psoriasis doesn’t stay contained to the top of the head. It frequently spreads to the hairline, forehead, back of the neck, and behind or inside the ears. If you’re unsure whether your symptoms match, use our free Symptom Checker to help map your presentation before your appointment.
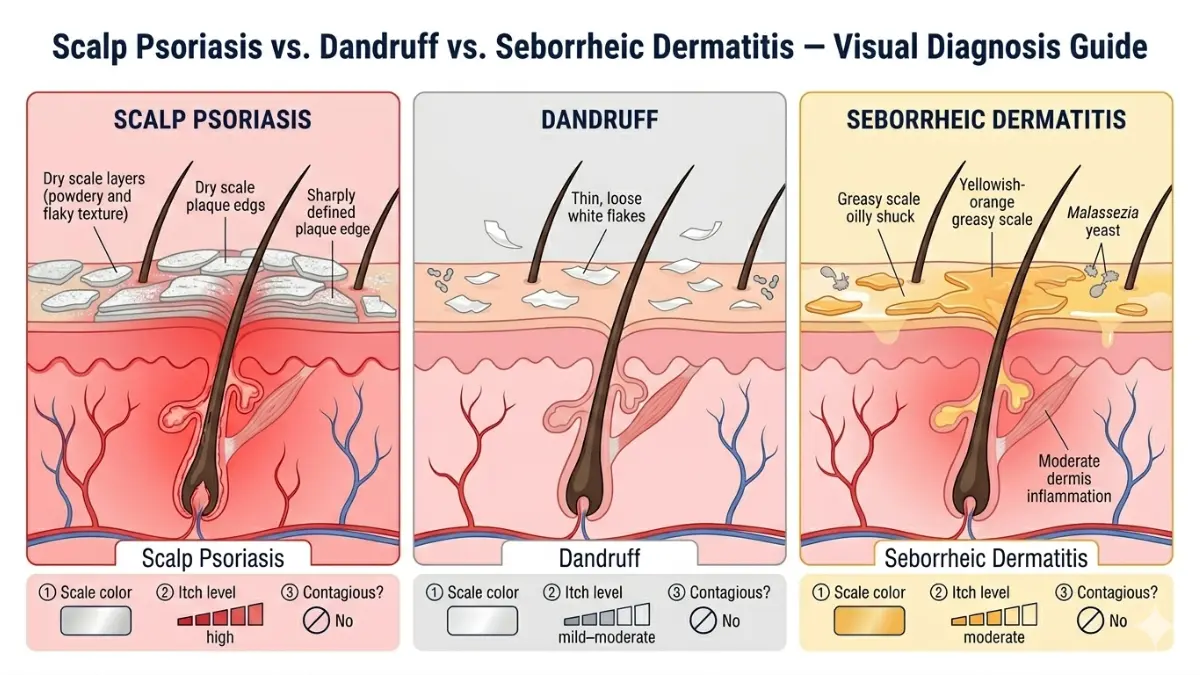
Scalp Psoriasis vs. Dandruff vs. Seborrheic Dermatitis
Misdiagnosis is extremely common. Here’s how to tell the difference:
| Feature | Scalp Psoriasis | Dandruff | Seborrheic Dermatitis |
|---|---|---|---|
| Scale appearance | Silvery-white, powdery | Small white flakes | Yellowish, greasy |
| Texture | Thick, dry plaques | Fine, loose | Oily, crusty |
| Itch level | Moderate to severe | Mild | Moderate |
| Skin involvement beyond scalp | Yes (ears, neck, forehead) | No | Sometimes (eyebrows, chest) |
| Cause | Autoimmune | Yeast/fungal | Yeast + oily skin |
On darker skin tones, scalp psoriasis plaques often appear purple or dark brown with gray scales — not the classic red-and-silver many online photos show. This distinction matters because misidentification leads to delayed treatment.
For a deeper look at how psoriasis affects the rest of the body, read our comprehensive guide on psoriasis treatment and plaque psoriasis.
Why Scalp Psoriasis Causes Hair Loss — The 3 Mechanisms Nobody Explains
This is where every competitor article fails you. Healthline, WebMD, and Cleveland Clinic all say “scratching can cause temporary hair loss” and move on. The biology is far more complex — and understanding it is what prevents permanent damage.
A 2025 review published in PMC (NIH) identified three distinct mechanisms of hair loss in scalp psoriasis patients. Here’s what’s actually happening:
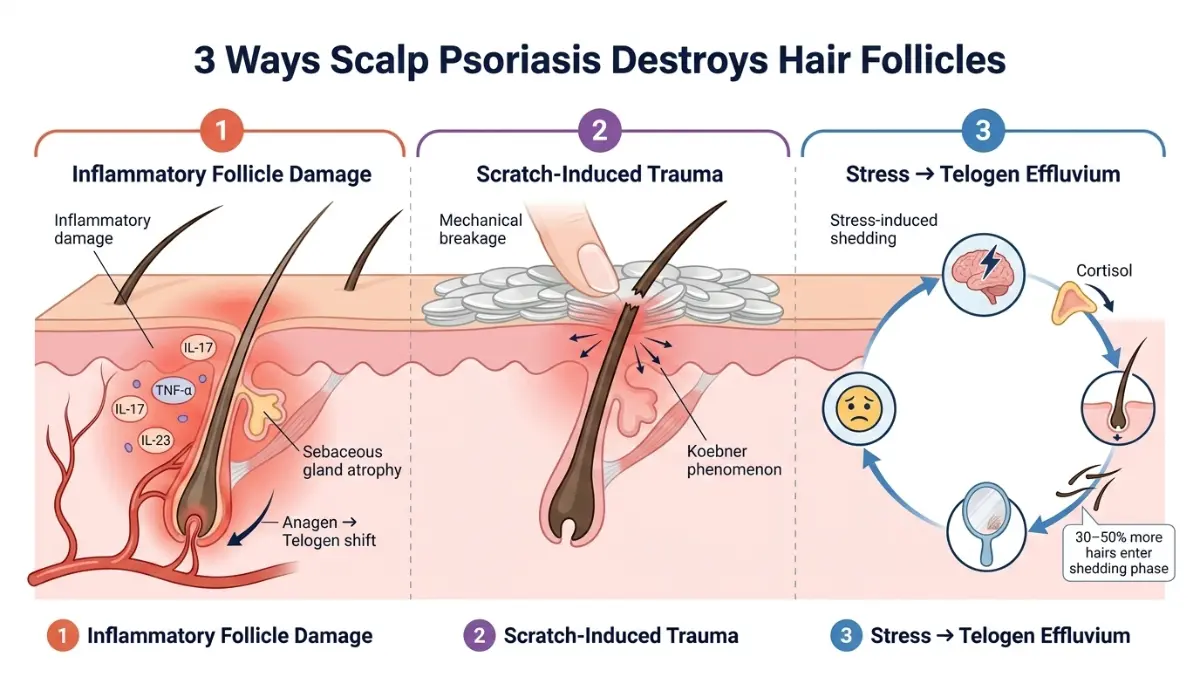
Mechanism 1 — Inflammatory Follicle Damage (The Hidden Driver)
The immune response in scalp psoriasis is driven by the Th17/IL-23 axis — a cascade of inflammatory signals including IL-17, IL-22, TNF-α, and IL-1β. These cytokines don’t just attack the skin surface. They directly disrupt the anagen (growth) phase of the hair cycle, pushing follicles prematurely into resting and shedding phases.
Additionally, psoriatic lesions cause sebaceous gland atrophy — the oil glands around hair follicles shrink and stop functioning properly. This weakens the structural environment around each hair shaft, making follicles fragile and prone to fallout even without physical trauma.
What this means for you: Even if you never scratch, active scalp psoriasis inflammation can silently damage follicles. Early treatment is not optional — it’s protective.
Mechanism 2 — Scratch-Induced Trauma & the Koebner Effect
Scalp psoriasis is intensely itchy. Scratching delivers short-term relief but causes two forms of damage:
- Mechanical breakage — hair shafts snap at the plaque surface
- Koebner phenomenon — trauma to previously unaffected skin triggers new psoriatic lesions in those areas, spreading the disease while worsening hair loss
Picking at thick scale — which many patients do to remove plaques — is particularly destructive. It removes hair in tufts and can create micro-wounds that become entry points for infection.
Mechanism 3 — The Stress–Telogen Effluvium Loop
This is the cycle that traps most scalp psoriasis patients for years, yet almost no mainstream health website explains it:
- Chronic psoriasis pain, itch, and embarrassment elevate cortisol levels
- Elevated cortisol triggers telogen effluvium — a form of diffuse hair shedding where 30–50% more hairs enter the resting/shedding phase simultaneously
- Visible hair loss increases psychological stress
- Increased stress worsens psoriasis flares
- Worse flares cause more hair loss — and the cycle repeats
Research from the National Psoriasis Foundation confirms that psoriasis patients have significantly higher rates of depression and reduced quality of life scores, both of which directly feed this cortisol-telogen loop.
Rare but important: In a small percentage of patients with severe, long-untreated scalp psoriasis, follicle destruction leads to psoriatic scarring alopecia — a permanent form of hair loss. This affects fewer than 5% of cases, and is almost entirely preventable with timely treatment.
Will Your Hair Grow Back? What the Evidence Says in 2026
The direct answer: Yes — in over 95% of cases, hair regrows fully after scalp psoriasis is treated and inflammation clears.
The type of hair loss determines the timeline and outcome:
| Hair Loss Type | Cause | Regrowth Prognosis |
|---|---|---|
| Non-scarring alopecia | Follicle inflammation (reversible) | Full regrowth — most common outcome |
| Telogen effluvium | Stress-cortisol shedding | Full regrowth within 3–6 months of flare control |
| Psoriatic scarring alopecia | Severe long-term inflammation | Partial or no regrowth — rare, preventable |

What to Expect on the Recovery Timeline
- Week 4: Itching and scaling begin reducing with consistent treatment
- Week 8: Plaque thickness decreases; most dermatologists see meaningful clearing
- Month 3: New hair growth visibly emerging in previously thinned areas
- Month 6: Most patients report near-complete or complete hair regrowth
The single biggest risk factor for extended hair loss is delayed treatment. Every month of uncontrolled scalp psoriasis inflammation is a month of ongoing follicle stress.
Because psoriasis has a significant genetic component, understanding your family risk profile can help you act earlier. Explore your hereditary risk factors using our free Genetic Risk Assessment Tool. You can also explore how related hair loss conditions respond to treatment in our guides on hair loss therapy and hair loss reversible treatment guide.
Scalp Psoriasis Treatments — From $8 Shampoos to 2026 Biologics
No competitor article gives you a complete, tiered treatment comparison with real efficacy data. Here’s the full picture — from what you can buy tonight to what your dermatologist can prescribe next week.
Step 1 — OTC Treatments (Mild Cases)
These are your first line of defense for mild scalp psoriasis. Look for these active ingredients:
- Coal tar (1%–2.5%): Slows skin cell overproduction, reduces inflammation and scaling. Effective for thin plaques
- Salicylic acid (2%–6%): Softens and loosens thick scale, improving penetration of other treatments
- Zinc pyrithione / selenium sulfide: Reduce scaling and itching
- Ketoconazole: Antifungal that also helps if seborrheic dermatitis is co-present
Application tip: Leave medicated shampoo on your scalp for 5 full minutes before rinsing. Apply to dry scalp before showering for maximum absorption through thick plaques.
The American Academy of Dermatology recommends coal tar as a core first-line OTC option for scalp psoriasis and provides a detailed application guide for each formulation type.
Step 2 — Prescription Topical Treatments (Mild to Moderate Cases)
When OTC products don’t deliver adequate control within 4 weeks, dermatologists prescribe:
- Topical corticosteroids — #1 prescribed treatment for scalp psoriasis in the US. Potent formula applied once daily for up to 4 weeks per NICE guidelines
- Calcipotriene (vitamin D analog) — Applied before bed; cover with shower cap to improve penetration through thick plaques. Most effective when combined with a steroid
- Calcipotriene + betamethasone combination — Studies show this combo outperforms either ingredient alone while reducing irritation side effects
- Tazarotene — Applied at night, rinsed in the morning. Often paired with a corticosteroid for enhanced clearance
Important: Using salicylic acid products before applying topical corticosteroids significantly improves their absorption through the scale barrier — a step many patients skip.
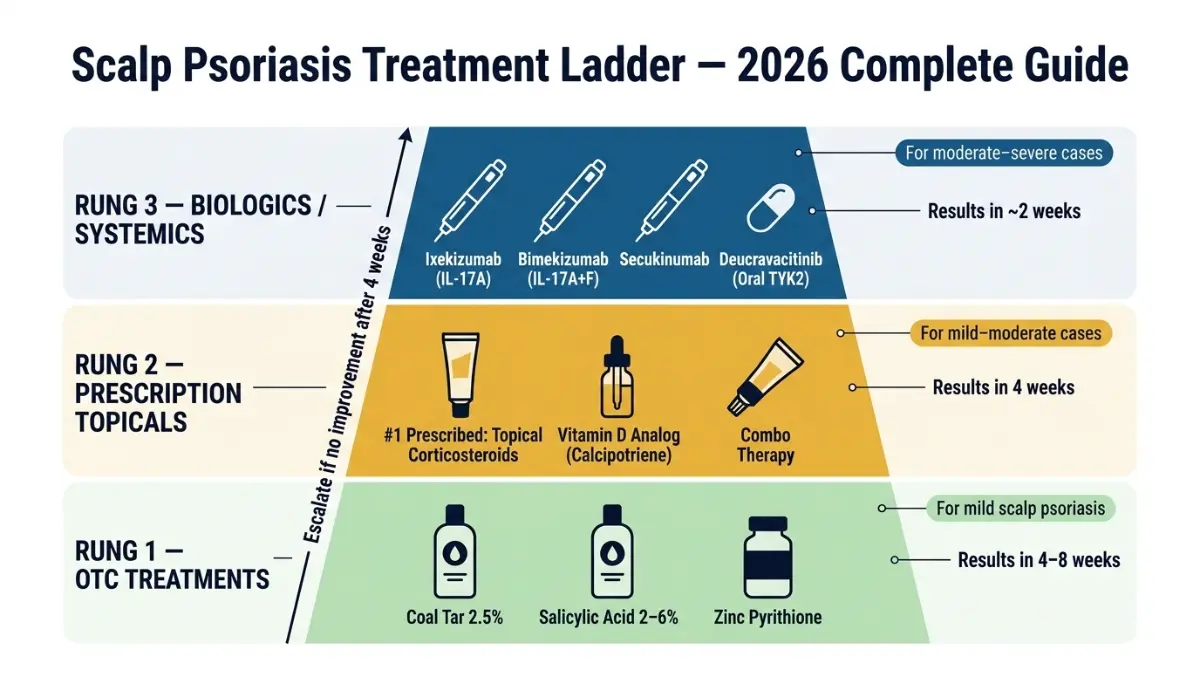
Step 3 — Systemic & Biologic Treatments (Moderate to Severe Cases, 2026 Data)
For patients with moderate-to-severe scalp psoriasis — or those who’ve failed topical treatments — biologics have transformed outcomes. A January 2026 network meta-analysis (Gupta et al., Journal of Cosmetic Dermatology) ranked biologics by scalp-specific efficacy:
| Biologic | Mechanism | Scalp Response | Speed of Response |
|---|---|---|---|
| Ixekizumab (Taltz) | IL-17A inhibitor | Highest PSSI-100 at 8 wks | Fastest — 2 weeks |
| Bimekizumab (Bimzelx) | IL-17A+F inhibitor | Highest ScPGA 0/1 at 16 wks | 2–4 weeks |
| Secukinumab (Cosentyx) | IL-17A inhibitor | High ScPGA 0/1 | 4 weeks |
| Guselkumab (Tremfya) | IL-23 p19 inhibitor | Superior to adalimumab | 8–16 weeks |
| Deucravacitinib (Sotyktu) | Oral TYK2 inhibitor | Good for scalp/difficult sites | 12–16 weeks |
2026 Update: Dermatology Times reported in February 2026 that TYK2 inhibitors like deucravacitinib are showing “meaningful response rates in difficult-to-treat regions such as the scalp” — and as an oral daily pill, they’re a game-changer for patients who can’t or won’t self-inject.
On methotrexate: This older systemic is effective for scalp psoriasis but carries a known risk of hair loss as a side effect. Dermatologists often avoid it in patients already experiencing psoriatic alopecia.
If you’ve just been prescribed a new psoriasis medication, our free Pill Identifier can help you verify your prescription details before your first dose.
How to Stop Hair Loss From Scalp Psoriasis — 8-Step Action Plan
Most health websites give you a treatment list. This is an action plan — what to do, in order, starting today.
Step 1: Start treatment immediately — don’t wait for a “bad flare” Even mild scalp psoriasis causes ongoing follicle stress. Every week of untreated inflammation is a week of potential hair follicle damage. Begin with a coal tar or salicylic acid shampoo tonight.
Step 2: Stop scratching — use targeted itch relief instead Cold compresses applied to the scalp for 10 minutes provide significant itch relief without trauma. Menthol-based sprays are also effective and can be applied between wash days.
Step 3: Choose the right shampoo and use it correctly Apply to a dry scalp. Part your hair in sections and work the medicated shampoo directly onto the skin — not just through the hair. Leave on for a full 5 minutes. Rinse. Follow with your regular conditioner.
Step 4: Apply topical treatments properly Part your hair in 1-inch sections. Use a dropper or nozzle applicator to apply medication directly to the scalp skin. Cover with a shower cap for 1–2 hours (or overnight) to improve penetration through thick plaques.
Step 5: Break the stress–hair loss loop Since cortisol directly worsens both psoriasis flares and telogen effluvium, stress management is a legitimate medical intervention — not just lifestyle advice. Consistent sleep is one of the most powerful cortisol regulators available. Use our free Sleep Calculator to identify and optimize your ideal sleep schedule to help reduce flare frequency.
Step 6: Protect your scalp during flares
- Avoid hair dye, bleach, and chemical relaxers during active flares
- Use fragrance-free, sulfate-free shampoo as your base cleanser
- Avoid tight hairstyles (ponytails, braids) that pull on the scalp
- Use a wide-tooth comb — never brush aggressively over plaques
Step 7: Identify and eliminate your personal triggers Common scalp psoriasis triggers include: stress, cold/dry weather, scalp injury, certain medications (lithium, beta-blockers, antimalarials), and alcohol. Track your flares in a journal for 4–6 weeks to identify patterns specific to you.
Step 8: See a dermatologist if there’s no improvement within 4 weeks This is not optional. The AAD scalp psoriasis symptom guidelines confirm that persistent or severe scalp psoriasis rarely resolves adequately with OTC management alone. Biologics can begin working in as little as 2 weeks for appropriate patients.
For patients also experiencing non-psoriatic hair loss, our guides on minoxidil for hair loss and hair loss treatments 2026 provide complementary information your dermatologist may find useful for dual-condition management.
Living With Scalp Psoriasis — Emotional Impact, Hair Care & When to See a Doctor Urgently
Scalp psoriasis carries a psychological burden that the clinical literature consistently underestimates. Dermatology Life Quality Index (DLQI) scores in scalp psoriasis patients frequently exceed 10 — indicating moderate-to-severe impairment of daily life quality, regardless of how much of the body is affected.
Patients report:
- Avoiding social events because of visible flaking on clothing
- Anxiety about people noticing their scalp or hair loss
- Reluctance to wear dark clothing or remove hats
- Depression linked to chronic itch, pain, and unpredictable flares
This is not vanity. It is a recognized, measurable component of disease burden — and it’s something your dermatologist should be actively addressing alongside your skin symptoms.
Hair Care Tips During Active Flares
- Brush gently — use a soft bristle brush or wide-tooth comb; never force through plaques
- Wash every 2–3 days with your medicated shampoo; daily washing can irritate already-inflamed skin
- Avoid heat styling — blow-dryers, flat irons, and curling tools can dry and crack plaques, increasing bleeding risk
- Use fragrance-free, alcohol-free products — fragrance is a common irritant that worsens scalp inflammation
- Pat dry after washing — never rub the scalp with a towel
When to Seek Urgent Medical Attention
See a dermatologist promptly if:
- OTC treatments have shown no improvement after 4 weeks of consistent use
- Hair loss is becoming visibly significant or occurring in defined patches
- Psoriasis is spreading beyond the scalp to face, neck, or ears
- Scalp plaques are cracking, bleeding, or showing signs of infection (warmth, pus, fever)
- Your current prescription treatment has stopped working
The National Psoriasis Foundation scalp resource provides a clinical-level overview of escalation criteria and a free patient helpline (1-800-723-9166) for guidance on finding a specialist.
A Note on Immunotherapy and Systemic Autoimmune Conditions
Scalp psoriasis is increasingly understood as a systemic inflammatory disease, not just a skin condition. One in three psoriasis patients will develop psoriatic arthritis. If you’re experiencing joint pain alongside your scalp symptoms, it’s critical to be screened by a rheumatologist — not just a dermatologist.
For a broader understanding of how immune-modulating therapies work across conditions, our guide on immunotherapy provides useful context on how biologic treatments function systemically.
The most important message: With today’s treatment options — including next-generation IL-17 and IL-23 biologics that show scalp clearance rates above 80% — nearly every person with scalp psoriasis can achieve significant or complete remission. The window for preventing permanent hair loss is open. The only variable is when you act.
Frequently Asked Questions — Scalp Psoriasis
Q1: Is scalp psoriasis contagious?
No. Scalp psoriasis is an autoimmune condition driven by your own immune system. It cannot be passed from person to person through any form of contact.
Q2: Does scalp psoriasis cause permanent hair loss?
Rarely. Over 95% of patients experience full hair regrowth once scalp psoriasis inflammation is properly controlled. Permanent scarring alopecia occurs only in untreated, severe long-term cases — and is considered largely preventable.
Q3: What does scalp psoriasis look like?
Raised, well-defined plaques covered in silvery-white or gray scale. On lighter skin, the base is often pink-red. On darker skin, plaques tend to appear purple or dark brown with gray scale. Plaques can appear in isolated patches or cover the entire scalp.
Q4: What triggers scalp psoriasis flares?
The most common triggers are stress, cold and dry weather, scalp injury or sunburn, certain medications (lithium, beta-blockers, antimalarials), alcohol consumption, and infections — particularly strep throat.
Q5: Can I color my hair if I have scalp psoriasis?
Avoid all chemical hair treatments — dye, bleach, relaxers — during active flares. During remission, choose ammonia-free dyes, always patch-test 48 hours before full application, and inform your stylist of your condition.
Q6: What is the best shampoo for scalp psoriasis?
Coal tar shampoos (2.5%) and salicylic acid shampoos (2%–6%) are the most evidence-backed OTC options. Apply directly to dry scalp, leave on for 5 minutes, then rinse. Rotate between different active ingredients if one stops working effectively.
Q7: Is scalp psoriasis the same as seborrheic dermatitis?
No — these are distinct conditions. Scalp psoriasis features silvery, dry, powdery scales on thick plaques. Seborrheic dermatitis produces yellowish, greasy flakes on oily skin. A dermatologist can confirm the diagnosis on examination, sometimes with a skin biopsy.
Q8: Can children get scalp psoriasis?
Yes. Children can develop scalp psoriasis at any age. Treatment principles are similar to adults but must be age-appropriate — topical steroid strength and duration are adjusted for pediatric use. Always consult a pediatric dermatologist.
Q9: How long before scalp psoriasis treatment works?
OTC shampoos typically show results within 4–8 weeks of consistent use. Prescription topicals often deliver meaningful clearing within 4 weeks. Biologics can begin producing visible scalp improvement within 2 weeks for appropriate candidates.
Q10: Does diet affect scalp psoriasis?
Emerging evidence supports anti-inflammatory dietary patterns (Mediterranean diet) in reducing flare frequency and severity. Alcohol and highly processed foods are consistently linked to worsening symptoms. Obesity is an independent risk factor for more severe psoriasis.
Q11: When should I urgently see a doctor for scalp psoriasis?
See a dermatologist promptly if: OTC treatments fail after 4 weeks, hair loss is significant or accelerating, plaques spread beyond the scalp, skin shows signs of infection, or your current prescription has stopped working. Do not wait for a “severe enough” flare — earlier intervention means better hair outcomes.
⚕️ Disclaimer: This article is for educational purposes only and does not constitute medical advice. The information provided is not a substitute for professional medical consultation, diagnosis, or treatment. Always seek the advice of a qualified dermatologist or healthcare provider with any questions you may have regarding scalp psoriasis or any other medical condition.
For more expert-reviewed health guides on skin, autoimmune conditions, and treatment options, visit our Health Tips hub.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.





