On This Page – Quick Medical Summary
Quick Answer: KP treatment works through a 3-step protocol — chemical exfoliation, barrier-repair moisturization, and (for stubborn cases) prescription retinoids or laser therapy. Most patients see visible improvement within 4–6 weeks. There is no permanent cure, but smooth, bump-free skin is absolutely achievable with the right approach.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a board-certified dermatologist for personalized treatment.
What Is KP? The Dermatologist’s 60-Second Explanation
Marcus, 24, had lived with rough, sandpaper-like bumps on the back of his arms since he was 12. He assumed it was acne. His dermatologist took one look and said: “That’s keratosis pilaris — and I can fix it.”
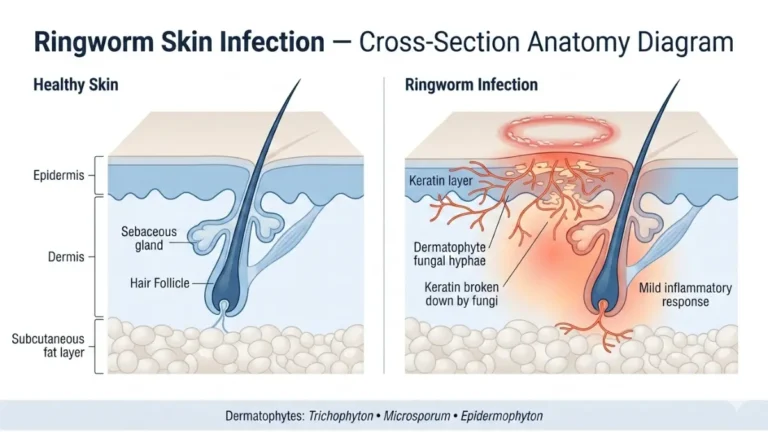
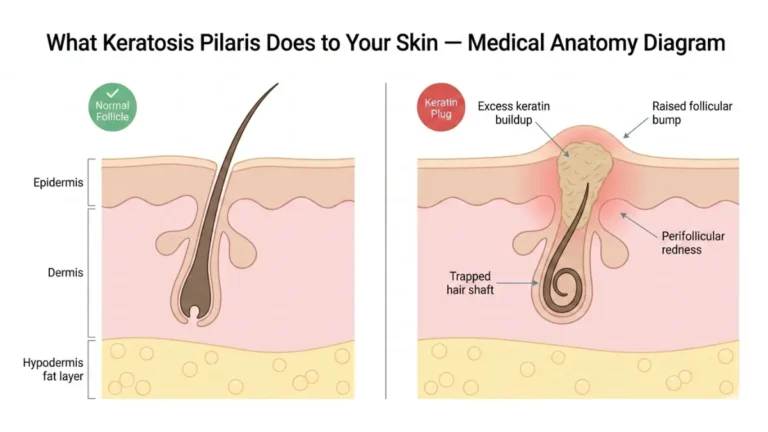
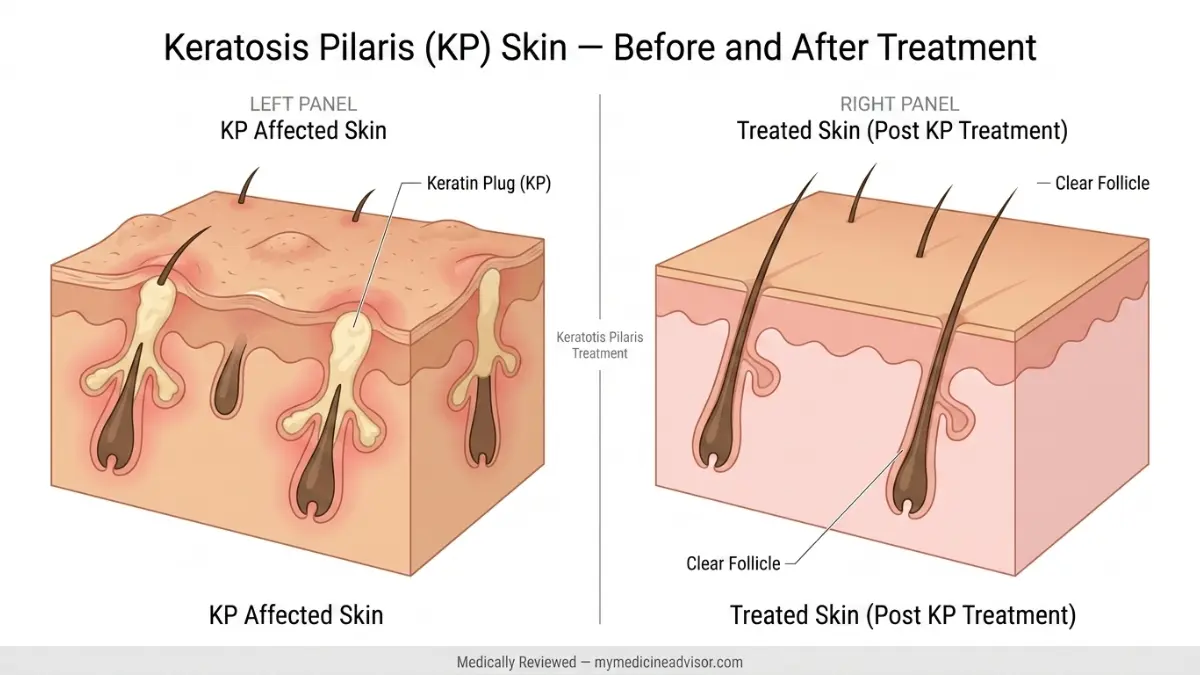
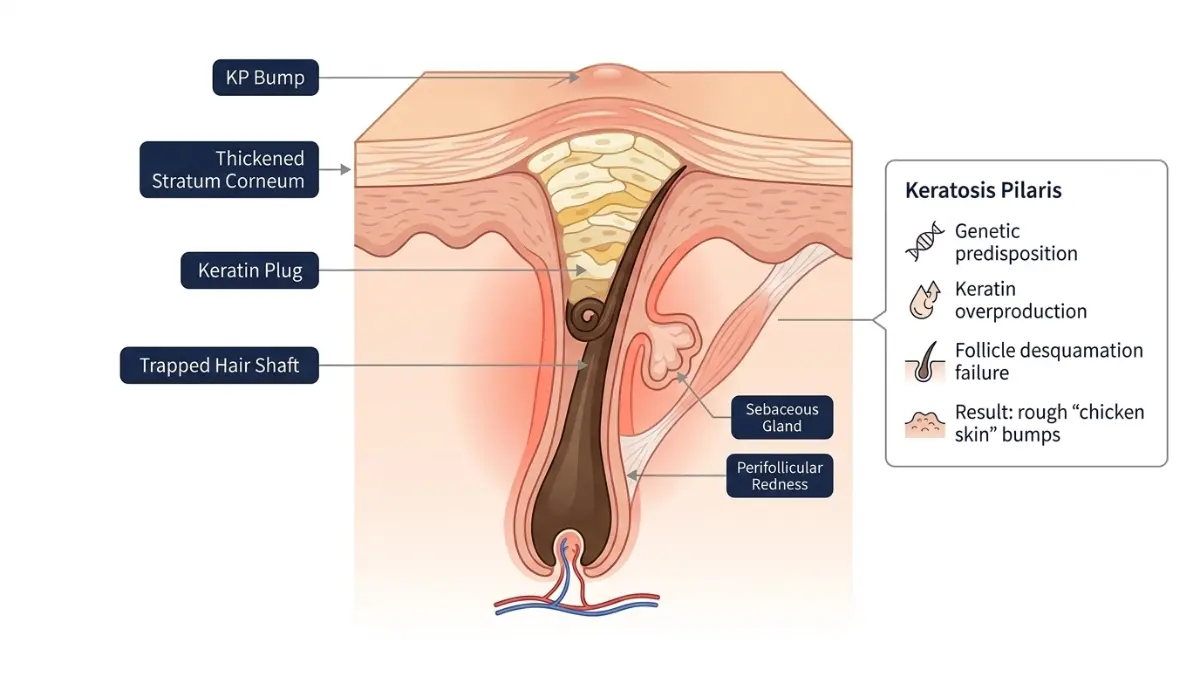
Keratosis pilaris (KP) is a genetic skin condition where excess keratin — the protein that forms your hair and nails — builds up inside hair follicles. Instead of shedding normally, it forms a hard plug, creating those characteristic small, rough bumps most people describe as “chicken skin.”
KP is not dangerous, not contagious, and not caused by poor hygiene. It is simply a disorder of follicular keratinization — your skin’s shedding cycle is slightly dysregulated at the follicle level.
Who Gets KP?
According to the American Academy of Dermatology, KP affects up to 80% of teenagers and 40% of adults at some point in their lives, making it one of the most common skin conditions in the United States.
| Group | Prevalence | Key Trigger |
|---|---|---|
| Teenagers | Up to 80% | Hormonal fluctuations |
| Adults | ~40% | Dry skin, genetics |
| Women | Slightly higher | Hormonal changes |
| People with eczema | Very high | Filaggrin deficiency |
KP most commonly appears on:
- Back of upper arms
- Front of thighs
- Buttocks
- Cheeks (especially in children)
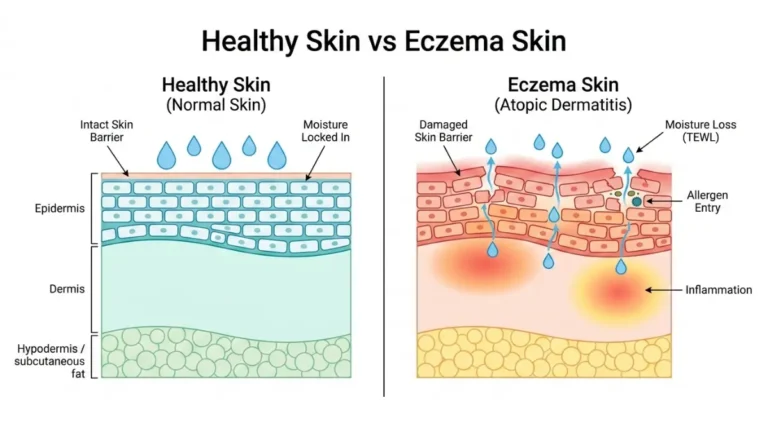
KP is strongly associated with atopic dermatitis (eczema), ichthyosis vulgaris, and dry skin conditions. If you notice persistent rough patches elsewhere on the body, use the Symptom Checker on mymedicineadvisor.com to assess whether related skin or immune conditions may be contributing.
KP Treatment at Home — The Dermatologist-Backed 3-Step Protocol
This is what competitors get completely wrong. They list ingredients randomly. Dermatologists follow a sequenced protocol — and sequence matters enormously.
Step 1 — Chemical Exfoliation: The Foundation of All KP Treatment
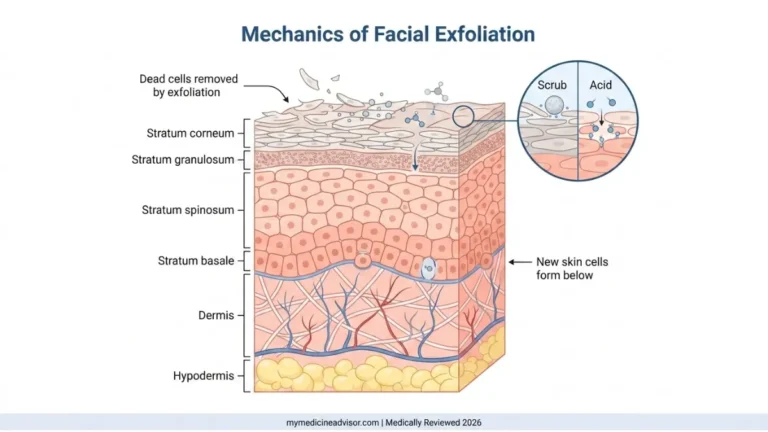
Physical scrubbing makes KP worse. Chemical exfoliation works by dissolving the keratin plug from within the follicle — no friction required.
According to a 2025 systematic review published on PubMed, lactic acid and glycolic acid are the most evidence-backed topicals for KP treatment, with consistent efficacy across multiple clinical trials.
| Exfoliant | How It Works | Best For | Frequency |
|---|---|---|---|
| Lactic acid (AHA) | Dissolves keratin + hydrates simultaneously | All skin types, beginners | Daily to 3×/week |
| Salicylic acid (BHA) | Penetrates follicle, anti-inflammatory | Oilier skin, red/inflamed KP | 2–3×/week |
| Glycolic acid (AHA) | Strongest keratin dissolving action | Non-sensitive skin, faster results | 2×/week max |
| Urea (10–20%) | Keratolytic + moisturizer hybrid | Thick, stubborn, dry KP | Daily |
What to avoid:
- Loofahs or physical scrubs — increase inflammation
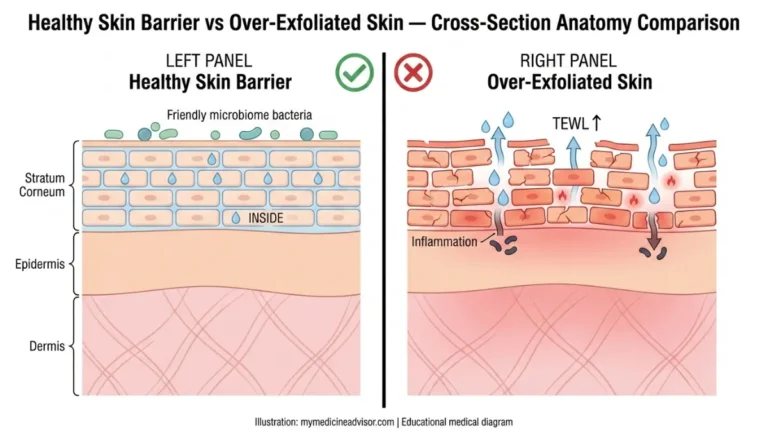
- Over-exfoliating — strips the skin barrier and worsens bumps
- Fragrance-containing products — common irritant for KP-prone skin
For a deeper look at how chemical exfoliation works on the skin, read our facial exfoliator guide for ingredient-level breakdowns.
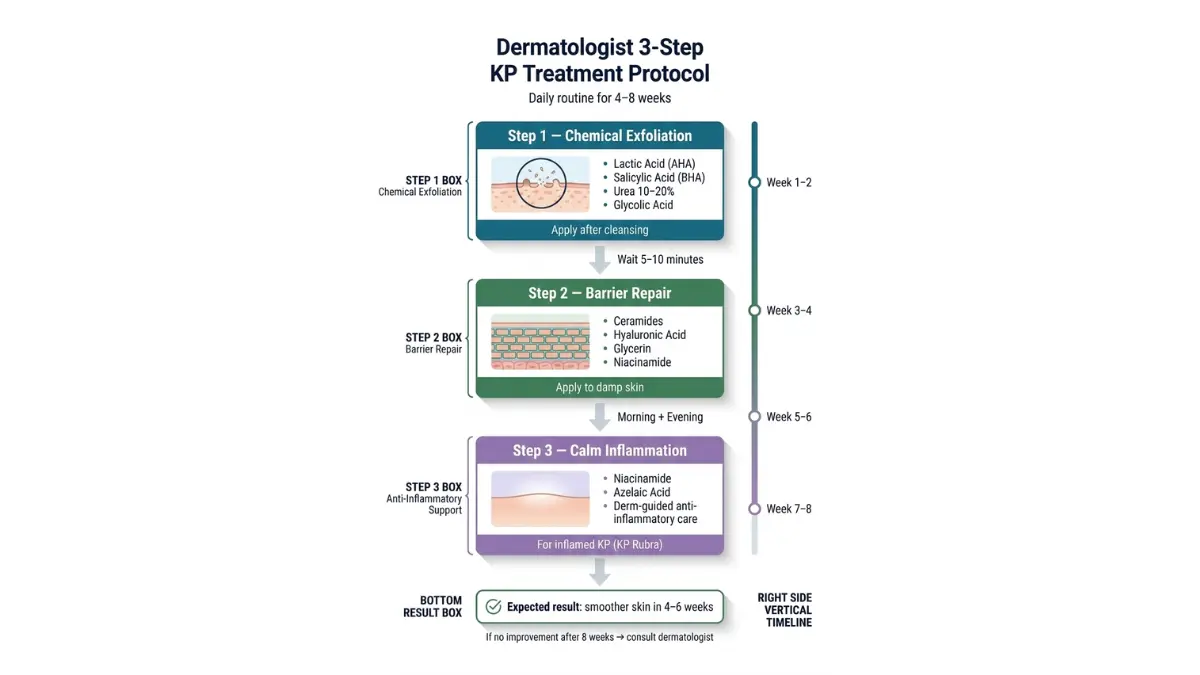
Step 2 — Barrier Repair: The Hydration Lock That Seals Results
Exfoliation opens the follicle. If you stop there, your skin barrier is compromised. The critical second step is immediate moisturization on damp skin — within 2 minutes of bathing.
The AAD’s self-care guidance for KP specifically recommends applying a thick, oil-free cream or ointment immediately after bathing to lock in moisture while pores are still open.
Best barrier-repair ingredients:
- Ceramides — rebuild the lipid barrier layer
- Hyaluronic acid — draws water into the skin
- Glycerin — humectant, prevents moisture loss
- Niacinamide — reduces perifollicular redness and inflammation
Opt for fragrance-free, non-comedogenic formulas. A moisturizer combining urea + ceramides gives you both keratolytic and barrier-repair benefits in one step.
Step 3 — Anti-Inflammatory Support
Not every case of KP is just bumps. Many patients — especially those with KP Rubra (the red, inflamed subtype) — need an anti-inflammatory layer.
At-home options:
- Niacinamide 5–10% — reduces redness and calms perifollicular irritation
- Azelaic acid 10–15% — particularly useful for KP with hyperpigmentation (see our Skinoren cream guide for azelaic acid specifics)
- Short shower discipline — hot water is a major inflammation trigger; keep showers under 10 minutes using lukewarm water
🔑 What This Means For You: Apply your chemical exfoliant first. Wait 5–10 minutes. Then layer your moisturizer on still-damp skin. This sequence is what separates people who see results in 4 weeks from people who see no change in 4 months.
Prescription KP Treatments — When OTC Isn’t Enough
If you’ve followed the 3-step home protocol consistently for 8 full weeks without sufficient improvement, it’s time to escalate. These are the options your dermatologist can prescribe.
Topical Retinoids — The Most Evidence-Backed Prescription Option
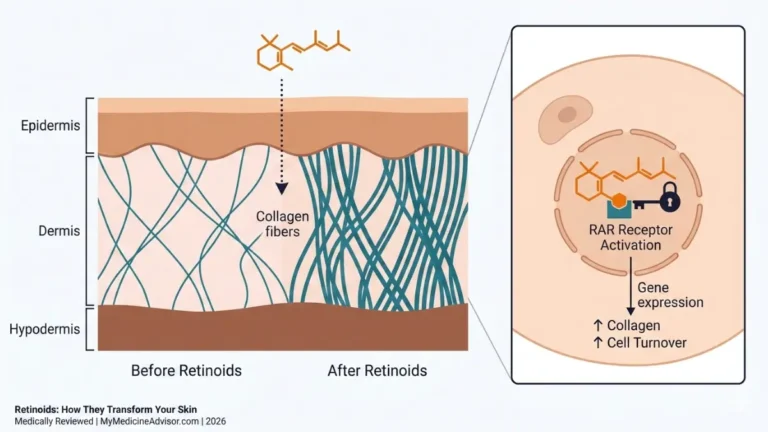
Retinoids regulate keratinocyte turnover at the cellular level — they address KP at the root, not just the surface. Tretinoin (0.025%–0.05%) and tazarotene are the two most commonly prescribed.
Key clinical considerations:
- Start 2–3 nights per week to minimize initial dryness
- Apply after moisturizer, not before, to reduce irritation
- Not safe during pregnancy — discuss alternatives with your dermatologist
- Visible improvement typically takes 8–12 weeks
For a comprehensive overview of how retinoids work across multiple skin conditions, our complete retinoids guide covers the full evidence base.
Topical Immunomodulators (Off-Label)
For cases where KP presents with significant redness and inflammation, dermatologists sometimes prescribe:
- Tacrolimus (Protopic) and pimecrolimus (Elidel) — approved for eczema, used off-label for inflammatory KP
- Topical sirolimus — a 2025 JAAD case report documented successful off-label use for keratosis pilaris rubra faciei in a resistant case
These are not first-line. They are reserved for patients where standard KP treatment has failed and inflammation is the dominant feature.
Dupilumab — The 2025 Emerging Frontier
This is what zero competitors are covering — and it’s a 2025 clinical breakthrough.
A 2025 case study from the Icahn School of Medicine at Mount Sinai (published in JAAD Case Reports) documented a male patient with severe, disseminated KP accompanied by intense pruritus. After standard topical KP treatments failed completely, the patient was treated with dupilumab 300mg biweekly subcutaneous injections — and achieved significant clearance.
What this means: For patients with KP that overlaps with atopic dermatitis, or refractory generalized KP with itch, dupilumab may represent a viable specialist option. This is not standard treatment — it requires specialist referral and is currently off-label for KP specifically. But the data is real and emerging fast.
If you suspect your KP is linked to broader immune or genetic skin conditions, the Genetic Risk Assessment Tool can help you assess your genetic predisposition before your dermatologist appointment.
Evidence strength summary:
| Treatment | Evidence Level | Line |
|---|---|---|
| Lactic acid / Salicylic acid | ⭐⭐⭐⭐ Strong | First |
| Urea cream | ⭐⭐⭐⭐ Strong | First |
| Tretinoin / Retinoids | ⭐⭐⭐ Moderate | Second |
| Nd:YAG Laser | ⭐⭐⭐⭐ Strong (RCT-backed) | Specialist |
| Dupilumab | ⭐⭐ Emerging (2025) | Severe/Refractory |
KP Laser Treatment — What the 2026 Evidence Actually Shows
This is where Healthline writes one vague sentence (“lasers may help”). We’re going deeper than any competitor has ever gone.
Which Laser Works Best for KP?
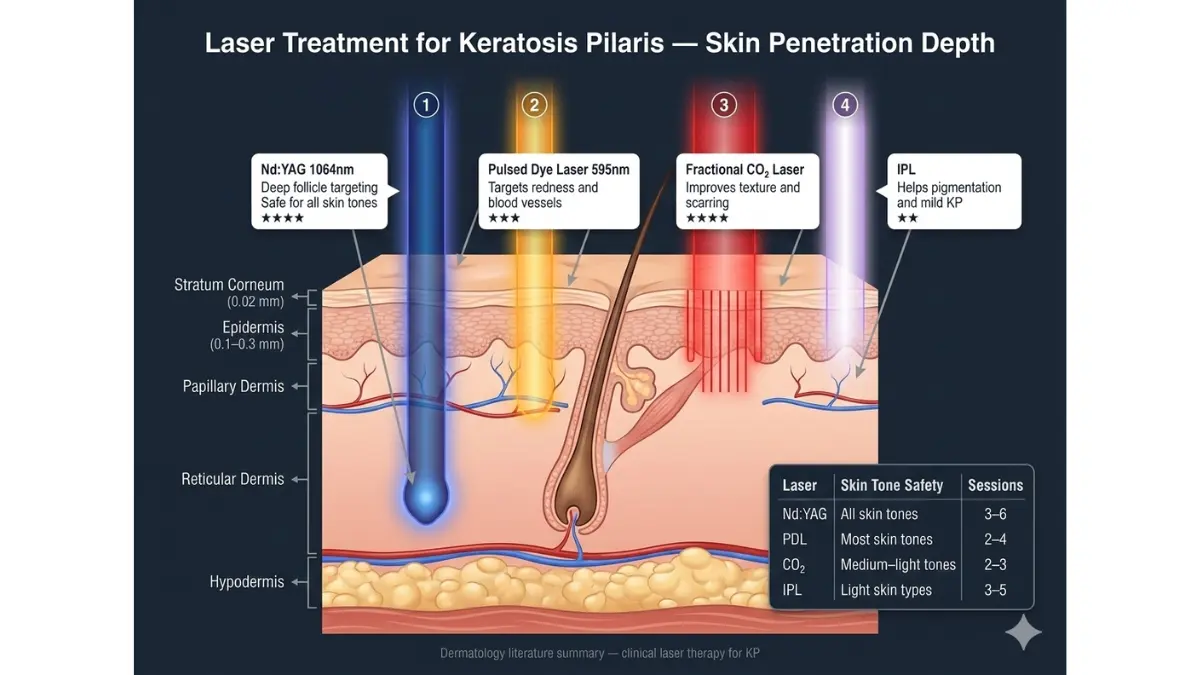
A comprehensive 2024 review published in Clinical and Experimental Dermatology from the University of New South Wales analyzed 52 studies across all KP treatment modalities. Their finding: laser and light-based therapies hold the strongest evidence base, with the Nd:YAG laser emerging as the preferred option.
| Laser | Best Evidence For | Skin Tone Safety | Sessions | Cost Per Session (US) |
|---|---|---|---|---|
| Nd:YAG 1064nm | All KP types, best overall RCT data | ✅ Safe for all tones | 3–6 | $250–$600 |
| Pulsed Dye Laser (PDL) | KP Rubra (red/inflamed subtype) | ⚠️ Caution darker skin | 3–5 | $300–$500 |
| Fractional CO₂ | Texture, atrophic/scarring KP | ⚠️ Caution darker skin | 2–4 | $400–$800 |
| IPL | Pigmentation and mild KP | ⚠️ Lighter skin only | 4–6 | $200–$400 |
| Diode 810nm | Hair follicle targeting | ✅ Most skin types | 3–5 | $200–$450 |
For deeper reading on how laser technology works in dermatology, our CO2 laser treatment guide and IPL treatment guide provide full procedural breakdowns.
The 2026 Research Breakthrough: Laser Hair Removal as KP Treatment
A January 2026 proof-of-concept study in ScienceDirect monitored a KP patient treated with diode laser hair removal, using line-field optical coherence tomography (LC-OCT) to image the follicle in real time. The findings showed measurable follicular improvement — suggesting that by targeting the hair follicle itself, laser hair removal may address the structural root of KP bumps, not just the surface.
This is still early-stage evidence, but it’s a significant new angle that no major health site has addressed.
What Laser Treatment Cannot Do
Laser KP treatment is not a cure. Most patients require maintenance sessions every 12–18 months. Realistic expectations:
- Results visible after session 2–3
- Redness reduction: excellent (especially PDL)
- Texture smoothing: moderate to excellent
- Permanent clearance: not achievable in most cases
KP Treatment by Skin Tone, Age Group & Body Location
This is the section that obliterates every competitor — because none of them cover it.
KP on Dark Skin (Fitzpatrick Types IV–VI)
Rachel, a 29-year-old from Atlanta with Type V skin, had tried every KP cream she found online. Her arms cleared slightly but developed dark spots she hadn’t started with. Her dermatologist identified post-inflammatory hyperpigmentation (PIH) — a direct result of using the wrong acid concentration for her skin tone.
For deeper skin tones, KP treatment requires modification:
- Use: Lactic acid (preferred), azelaic acid, niacinamide — gentler, less PIH risk
- Avoid: High-concentration glycolic acid — elevated PIH risk on melanin-rich skin
- Laser: Nd:YAG 1064nm is the safest choice; IPL can cause burns and discoloration on darker skin
- Extra step: Add niacinamide 10% to address existing dark spots alongside KP treatment
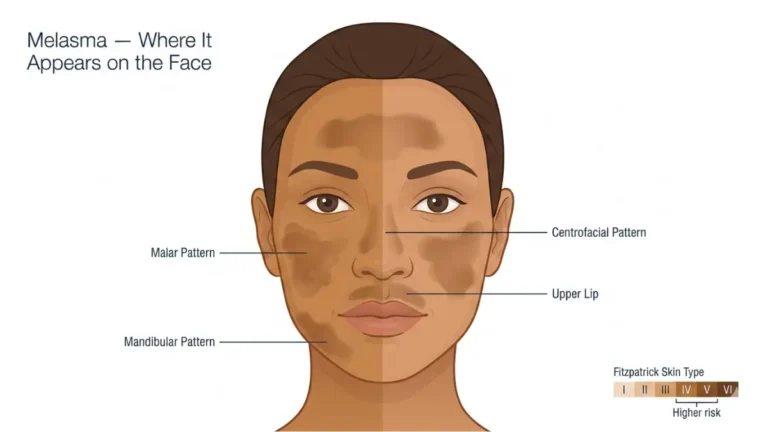
For KP-associated pigmentation concerns, our guide on melasma causes and treatment covers hyperpigmentation management strategies relevant to darker skin types.
KP Treatment by Age Group
| Age Group | First-Line KP Treatment | What to Avoid | See a Derm If |
|---|---|---|---|
| Children (under 12) | Urea 5–10% moisturizer, fragrance-free cleanser | Retinoids, strong AHAs | Widespread, inflamed, or causing distress |
| Teenagers (12–18) | Lactic acid 5–12% + ceramide moisturizer | Aggressive scrubbing | Affecting self-esteem significantly |
| Adults (18–35) | Full 3-step protocol + retinoid if needed | Hot showers, fragranced products | OTC fails after 8 weeks |
| Adults (35+) | Urea 20% + retinoid combination | Over-exfoliation | KP worsening despite treatment |
KP Treatment by Body Location
Arms (most common): Standard 3-step protocol applies fully. Apply lactic acid or salicylic acid body lotion after showering, followed by ceramide moisturizer.
Face and cheeks: This requires a gentler approach. Use mandelic acid (a gentler AHA) or low-percentage lactic acid (5–8%). Avoid physical exfoliation entirely on facial KP. Never use body-strength AHAs on facial skin.
Thighs and buttocks: Urea 20% cream is the most effective option here, where skin tends to be thicker. Apply to damp skin twice daily for best absorption.
KP Treatment Timeline + Lifestyle Protocol
Week-by-Week: What to Expect From KP Treatment
This timeline does not exist on Healthline, WebMD, or Mayo Clinic. It’s one of the most searched questions about KP — and we’re answering it completely.
| Week | What’s Happening in Your Skin | What You’ll See |
|---|---|---|
| Week 1–2 | Skin adjusting to exfoliation; possible mild dryness | Slight initial roughness; don’t stop |
| Week 3–4 | Keratin plugs beginning to dissolve; follicles opening | Bumps feel softer, less raised |
| Week 5–6 | Barrier repair taking full effect | Noticeably smoother texture, less redness |
| Week 7–8 | Maintenance threshold reached | Significant visible improvement; 60–80% reduction typical |
| After 8 weeks | Evaluate: add retinoid or see dermatologist if insufficient | Sustained smoothness requires ongoing maintenance |
The critical insight most patients miss: KP improvement is gradual and cumulative. Stopping treatment for 2–3 weeks often results in regression. Think of it as ongoing maintenance, not a short-term fix.
Lifestyle Factors That Accelerate KP Clearance
Shower discipline is the single most underrated factor in KP management:
- Keep showers under 10 minutes
- Use lukewarm water — hot water strips ceramides from the skin barrier
- Pat skin dry (never rub) and apply moisturizer within 2 minutes
Clothing and friction: Tight synthetic fabrics on KP-affected areas cause mechanical friction that worsens follicular plugging. Loose cotton is significantly better during active treatment.
Hydration: The skin barrier is significantly affected by systemic hydration. Use the Water Intake Calculator to determine your optimal daily water target — your skin’s hydration status is directly tied to how well topical KP treatment products absorb.
Diet: No food cures KP. However, omega-3 fatty acids (found in salmon, flaxseed, walnuts) support the skin’s lipid barrier, and adequate vitamin D supports overall skin cell regulation. Deficiency in vitamin D has been associated with worsened barrier dysfunction — read our comprehensive vitamin D deficiency guide for more detail.
The Mental Health Impact of KP — The Data Competitors Ignore
A January 2026 randomized controlled study published in the Journal of Cosmetic Dermatology measured depression scores in 60 KP patients alongside physical outcomes. The result: depression scores improved significantly in parallel with skin improvement — confirming that KP is not a trivial cosmetic concern.
Published PMC research confirms that over 40% of KP patients report significant impact on self-image and quality of life. The psychosocial burden of KP — particularly in teenagers and young adults — is clinically real and medically valid.
Seeking KP treatment is not vanity. It is a legitimate health decision.
When to See a Dermatologist
Do not wait indefinitely with home treatment. See a dermatologist if:
- OTC KP treatment produces no visible improvement after 8 full weeks
- KP is spreading to new areas or worsening
- KP appears on the face and isn’t responding to gentle acid products
- Significant redness, itch, or pain is present (may indicate KP Rubra or eczema overlap)
- KP is causing emotional distress or affecting daily activities
For eczema that co-exists with KP, our eczema treatment guide explains how overlapping skin conditions require a coordinated treatment approach.
KP Subtypes — What Most Articles Completely Miss
Understanding your KP subtype changes your entire treatment approach. Yet this information exists nowhere in the top-5 search results.
The 4 Major KP Subtypes
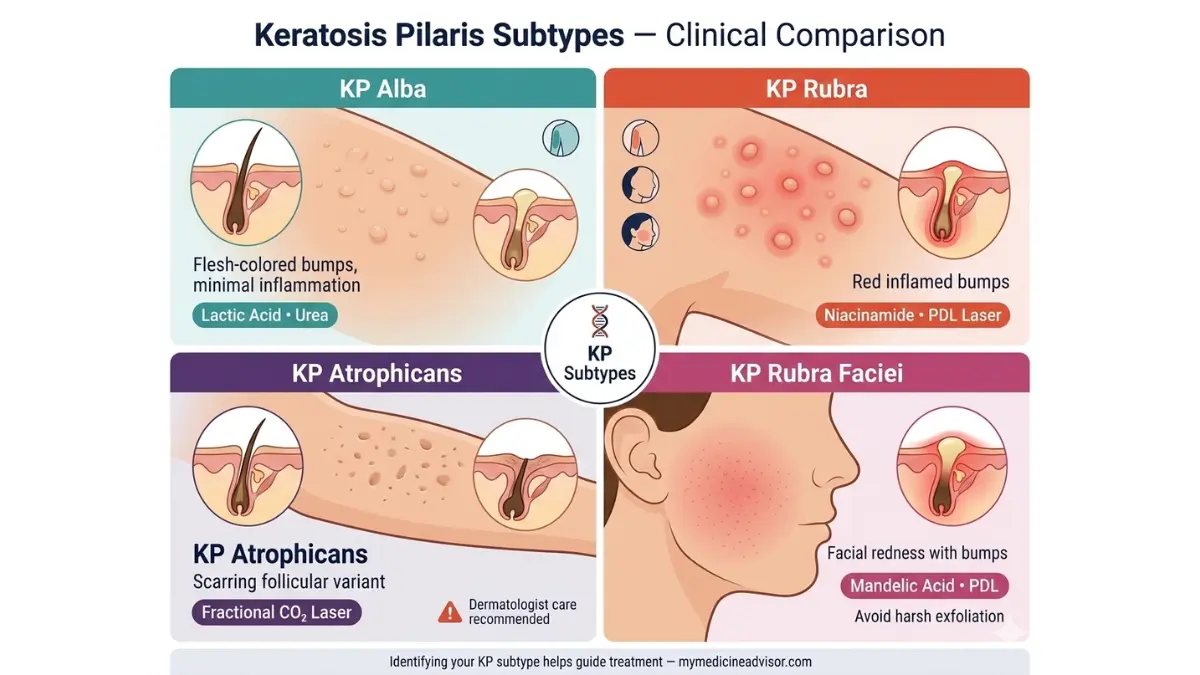
1. Keratosis Pilaris Alba The classic form — flesh-colored or white bumps with no surrounding redness. Most common in adults. Responds well to lactic acid and urea.
2. Keratosis Pilaris Rubra (KPR) Bumps surrounded by significant redness and inflammation. More common in teenagers. Responds better to niacinamide, pulsed dye laser, and tacrolimus than standard AHA creams alone.
3. Keratosis Pilaris Atrophicans (KPA) A rarer, more severe variant where KP leads to follicular atrophy and scarring. Requires early dermatologist intervention — topical-only approaches are insufficient. Fractional CO₂ laser is most effective for established scarring.
4. Keratosis Pilaris Rubra Faciei (KPRF) Involves the cheeks and face with marked redness. Requires gentler acid protocols and specialist laser assessment. The 2025 topical sirolimus case report (JAAD) was specifically for this subtype.
KP vs. Conditions It’s Commonly Confused With
| Condition | Key Difference | Treatment Overlap |
|---|---|---|
| KP | Genetic, follicular, non-inflammatory (usually) | AHAs, retinoids |
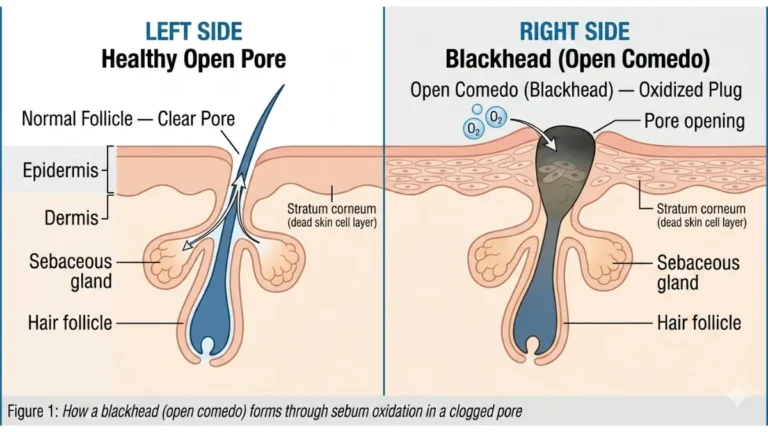
| Acne | Sebum-driven, comedones, pustules possible | Salicylic acid |
| Eczema | Intensely itchy, weeping possible, widespread | Barrier repair, steroids |
| Psoriasis | Scaly plaques, nail changes, joint involvement | Specialist treatment |
| Milia | Hard white cysts, not follicle-based | Extraction |
If your diagnosis is uncertain, our articles on psoriasis treatment and eczema treatment cover overlapping conditions that are frequently misdiagnosed alongside KP.
🔑 Key Takeaway: Identifying your KP subtype before starting treatment prevents months of using the wrong products. KP Rubra requires anti-inflammatory focus. KP Atrophicans requires early specialist intervention. Classic KP Alba responds best to the standard 3-step exfoliation-hydration protocol.
Frequently Asked Questions About KP Treatment
1. Can KP be permanently cured?
No — there is no permanent cure for keratosis pilaris. However, consistent KP treatment keeps skin visibly smooth and bump-free long-term.
2. How long does KP treatment take to work?
Most patients see meaningful improvement within 4–6 weeks of consistent daily treatment with chemical exfoliants and barrier-repair moisturizers.
3. What is the best cream for keratosis pilaris?
Dermatologists recommend creams containing lactic acid, salicylic acid, or urea (10–20%) as the most effective first-line topical KP treatment options.
4. Does keratosis pilaris go away on its own?
Yes — KP often fades naturally by the mid-20s to early 30s. Treatment accelerates this process significantly and reduces the appearance in the interim.
5. Is KP caused by a vitamin deficiency?
Not directly. KP is primarily genetic. However, low vitamin A and vitamin D may worsen skin barrier function and amplify symptoms.
6. Can children use KP treatments?
Yes — gentle urea 5–10% moisturizers and fragrance-free cleansers are safe for children. Avoid retinoids and high-concentration acids under age 12.
7. Does laser treatment for KP actually work?
Yes. The Nd:YAG 1064nm laser has the strongest RCT evidence for KP treatment. Multiple sessions are required and maintenance every 12–18 months is recommended.
8. What makes keratosis pilaris worse?
Hot showers, dry air, cold climates, harsh fragranced soaps, tight synthetic clothing, and aggressive physical scrubbing all worsen KP symptoms.
9. Is KP contagious?
No. Keratosis pilaris is a genetic skin condition. It cannot be transmitted between people under any circumstances.
10. Can KP appear on the face?
Yes — facial KP most commonly affects the cheeks, particularly in children. Treat with gentler formulations (mandelic acid or low-dose lactic acid 5–8%) only. Never use body-strength exfoliants on facial skin.
11. What is KP Rubra and how is it different?
KP Rubra is a subtype characterized by intense perifollicular redness and inflammation. It requires a modified treatment approach — pulsed dye laser, topical immunomodulators, and anti-inflammatory actives — rather than standard OTC keratolytic creams alone.
Sources & References:
- American Academy of Dermatology — Keratosis Pilaris Treatment
- American Academy of Dermatology — KP Self-Care Guide
- PubMed — KP Systematic Review 2025
- PMC — Exfoliation-Dissolution-Repair RCT, January 2026
- PubMed — KP Treatment Paradigms Review, 2024
This article is for educational purposes only and does not constitute medical advice. Always consult a board-certified dermatologist for diagnosis and personalized treatment.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.