On This Page – Quick Medical Summary
The best sunscreen for melanoma prevention is a broad-spectrum, water-resistant formula with SPF 30 minimum — ideally SPF 50+ for high-risk individuals. Used correctly and consistently, daily sunscreen reduces your melanoma risk by up to 50%, according to a landmark 10-year Australian randomised controlled trial.
Marcus, a 48-year-old roofing contractor from Houston, spent two decades working under direct Texas sun without daily sunscreen. By 2023, he was sitting in a dermatologist’s office hearing the words “Stage II melanoma” — a tumour on his left forearm, directly tied to cumulative UV exposure. His dermatologist’s first words after surgery: “This was largely preventable.”
His story is not rare. According to our detailed analysis of melanoma statistics in 2026, an estimated 9,500 Americans are diagnosed with skin cancer every single day. Melanoma specifically accounts for the majority of skin cancer deaths. The critical fact: approximately 90% of melanomas are directly caused by UV radiation — making them largely preventable with the right protective strategy.
Evidence published in the Journal of Clinical Oncology (ASCO) confirms that using SPF ≥ 15 reduced melanoma risk by 30% compared to lower SPF use in a Norwegian cohort of over 140,000 women — and correct application of higher SPF formulas pushes that protection further.
Before grabbing any bottle from a shelf, your best sunscreen for melanoma prevention must meet three non-negotiable clinical criteria:
- ✅ “Broad Spectrum” on the label — protects against both UVA and UVB rays
- ✅ SPF 30 or higher — minimum threshold for meaningful melanoma risk reduction
- ✅ Water-resistant — maintains SPF protection during sweat and swimming
If you carry a family history of skin cancer or know you have fair skin with a history of sunburns, use our Genetic Risk Assessment Tool to understand your personalised melanoma risk level before selecting your SPF protocol.
SPF 15, 30, 50, or 100 — Which Number Actually Prevents Melanoma?
Most people choose their SPF based on marketing. Here is what the numbers actually mean in clinical context.
SPF Protection Levels: A Clinical Comparison
| SPF Level | UVB Blocked | Best Suited For | Melanoma Risk Context |
|---|---|---|---|
| SPF 15 | ~93% | Indoor-dominant days | Reduces SCC risk ~40%; insufficient for outdoor melanoma prevention |
| SPF 30 | ~97% | Daily use, commuting, errands | AAD/WHO minimum standard for melanoma prevention |
| SPF 50 | ~98% | Outdoor activities, fair or high-risk skin | Recommended for athletes, high-risk patients, beach days |
| SPF 100 | ~99% | Post-treatment, melanoma survivors | Only 1% extra coverage; FDA proposing “SPF 50+” cap to prevent consumer deception |
The American Academy of Dermatology officially recommends SPF 30 as the minimum daily standard and SPF 50+ for extended outdoor exposure or high-risk individuals.
The SPF Time-Protection Myth
Many people believe SPF 50 means they can stay outdoors 50 times longer without burning. This is clinically incorrect — and acts as a false security that increases melanoma risk.
UV radiation dose is not equal to time spent in the sun. UV intensity peaks between 10 AM and 4 PM, increases with altitude, and intensifies in summer months. Your sunscreen’s protective window is a maximum of 2 hours regardless of SPF number. This fact alone changes how you should use every bottle.
The Under-Application Crisis
Studies consistently show most people apply only 20–50% of the required sunscreen amount. An SPF 50 product applied at 25% of the recommended dose performs like SPF 12–15 in real-world conditions. This single mistake undermines the entire label claim you’re relying on.
UVA vs. UVB: Why Broad Spectrum Is Non-Negotiable for Melanoma
Two types of UV radiation drive melanoma risk:
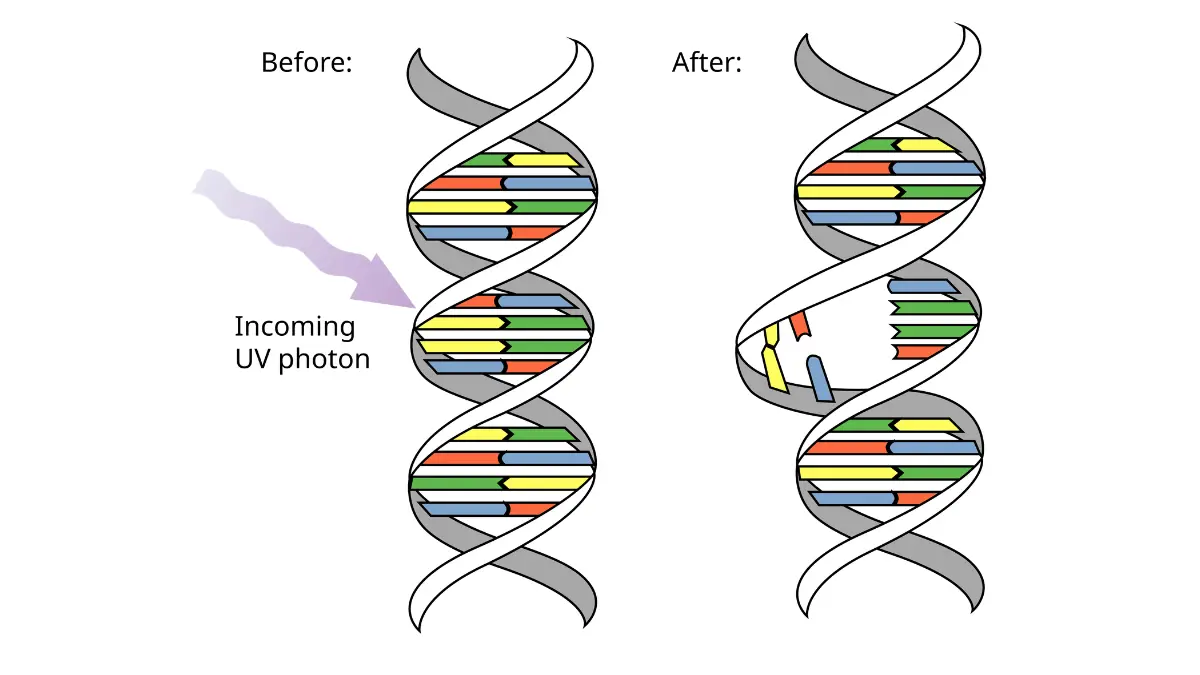
- UVB rays — the “burning rays,” primary drivers of direct DNA mutation and acute melanoma risk
- UVA rays — penetrate the deep dermis, present year-round, pass through glass and clouds, and drive cumulative cellular mutations over decades
A sunscreen labelled only with SPF addresses UVB protection alone. Per FDA sunscreen regulations, a product can only carry the “broad spectrum” designation if it protects against both UVA and UVB. For melanoma prevention, broad-spectrum coverage is clinically mandatory — not a preference.
Mineral vs. Chemical Sunscreen — The Definitive Melanoma Prevention Breakdown (2026)
Every top-ranking article gives a generic answer here. This is the clinically precise breakdown that melanoma prevention actually requires.
Mineral vs. Chemical Sunscreen: Full Comparison
| Feature | Mineral (Zinc Oxide / Titanium Dioxide) | Chemical (Avobenzone, Oxybenzone, Homosalate) |
|---|---|---|
| Mechanism | Reflects and scatters UV rays physically | Absorbs UV radiation, converts to heat |
| Time to effectiveness | Immediate upon application | 15–20 minutes absorption required |
| UVA coverage | Excellent — zinc oxide covers the full UVA spectrum | Variable — only avobenzone covers UVA broadly |
| Sensitive skin suitability | Preferred; less irritating | Risk of contact dermatitis in some patients |
| Melanoma survivor use | Clinically preferred | Not recommended for immunocompromised skin |
| Hormone concern | None | Oxybenzone detected in 70%+ of Americans; estrogenic activity documented |
| White cast | Common, improving with nano-zinc formulas | Minimal to none |
Which Ingredients Actually Cover UVA for Melanoma Prevention?
Of all FDA-approved sunscreen ingredients, only three protect meaningfully against UVA radiation — the rays that drive deep dermal melanoma mutations: zinc oxide, avobenzone, and oxybenzone. The Skin Cancer Foundation recommends verifying at least one of these is present on the active ingredients label of your chosen sunscreen.
Expert insight: Dr. Aditi Menon MD (Dermatology) advises: “For high-risk patients and melanoma survivors, I consistently recommend zinc oxide-based broad-spectrum formulas. They provide immediate, reliable UVA and UVB coverage with no systemic absorption concerns — and they perform better on reactive or post-treatment skin.”
The 2026 “Sunscreen Doping” Warning — What Competitors Haven’t Told You
A significant 2026 consumer safety issue: products marketed as “100% mineral” are increasingly found to contain unregulated chemical UV-boosting ingredients added to improve texture and raise SPF readings — without disclosure on front labels.
How to protect yourself:
- Read the Active Ingredients section specifically — not front marketing claims
- A genuinely mineral sunscreen lists only zinc oxide and/or titanium dioxide under Active Ingredients
- If you see homosalate, octinoxate, or oxybenzone in any ingredient list on a “mineral” product, it has been adulterated
- This matters critically for patients avoiding chemical filters due to skin sensitivity, hormone concerns, or post-melanoma treatment protocols
Research context from PMC/NCBI underscores why filter transparency directly affects melanoma risk reduction outcomes — what’s on the label must match what’s in the formula.
Best Sunscreen by Skin Type and Melanoma Risk — The 2026 Clinical Matrix
No top competitor personalises this. Here is the clinical matrix that makes this guide uniquely actionable for your specific situation.

Fair Skin, Light Eyes, or Family History of Melanoma
Fair-skinned individuals with a personal or family history of melanoma carry the highest cumulative UV damage risk. Critically, Harvard T.H. Chan School of Public Health research confirms that 60% of all US melanoma deaths occur in white men aged 50 and above — the demographic least likely to use daily sunscreen.
Clinical protocol:
- SPF 50+, broad-spectrum, water-resistant mineral sunscreen
- Apply 15–30 minutes before outdoor exposure
- Reapply every 80 minutes during activity; every 2 hours at rest
- Evaluate your inherited risk: Is Melanoma Hereditary?
- Use our Genetic Risk Assessment Tool to model your personal risk profile
Darker Skin Tones — The Critical Warning
A dangerous and persistent myth: that melanin provides full sun protection. It does not.
UVA rays penetrate all skin tones, driving deep dermal DNA damage regardless of pigmentation. In people with darker skin, melanoma frequently appears on palms, soles, under nails (subungual melanoma), and mucous membranes — and is consistently diagnosed at later, more aggressive stages due to delayed detection and the misconception of immunity.
Clinical protocol:
- SPF 30+ broad-spectrum daily
- Tinted mineral formulas significantly reduce the white cast barrier to daily use
- Prioritise zinc oxide or avobenzone for full UVA coverage
- If you notice an unusual skin change, use our Symptom Checker as a first step before your dermatology appointment
Melanoma Survivors and Immunosuppressed Patients
For post-treatment patients, broad-spectrum sunscreen is a medical protocol, not a lifestyle preference.
Clinical protocol:
- SPF 50+ zinc oxide-based, full-body coverage including scalp, ears, lips, and backs of hands
- Reapply every 40–80 minutes; always after towel drying
- Coordinate sun protection strategy with your oncologist
- Full clinical overview: Melanoma Symptoms, Stages & Treatment
Children (6 Months and Older)
- Under 6 months: No sunscreen. Use shade, UPF clothing, and wide-brim hats exclusively
- 6 months+: Mineral SPF 30+, zinc oxide-based, oxybenzone-free
- Reapply every 2 hours; immediately after swimming or sweating
Active Lifestyles and Outdoor Workers
“Water-resistant” is an FDA-defined claim — it means SPF is maintained for 40 or 80 minutes of water exposure, not indefinitely.
Clinical protocol:
- SPF 50+ water-resistant (80-minute rated) for outdoor workers and athletes
- Reapply every 40 minutes during sustained high-sweat activity
- Layer with UPF 50+ clothing and wide-brim hat for all-day outdoor exposure
Applying Sunscreen Correctly — The Mistakes That Completely Destroy Your SPF Protection
The best sunscreen for melanoma prevention fails entirely if applied incorrectly. These are the clinical errors costing patients their protection.
The Shot Glass Rule
- Full body coverage: 1 ounce (30 ml) — approximately one full shot glass
- Face only: Two full finger-lengths of product across index and middle fingers
- Most people apply 25% of this amount — which degrades SPF 50 to SPF 12 performance in practice

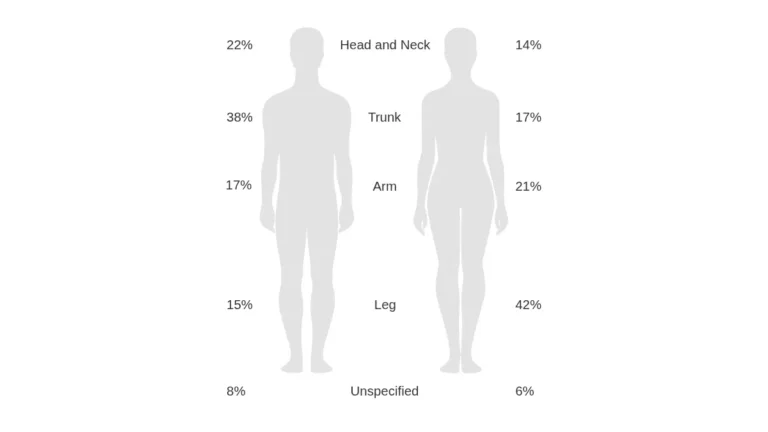
The Body Map — Missed Zones Where Melanomas Form
| Body Zone | Application Miss Rate | Clinical Importance |
|---|---|---|
| Ears | ~78% | Frequent melanoma site; cartilage is rarely protected |
| Scalp part line | ~90% | High-risk zone; particularly dangerous in balding men |
| Lips | ~85% | Lip melanoma has poor prognosis due to late-stage detection |
| Back of legs | ~68% | Site of 20% of melanomas in women |
| Tops of feet | ~72% | Constant exposure in sandals; UV accumulation over years |
| Back of hands | ~55% | One of the highest daily UV exposure sites on the body |
| Neck and nape | ~65% | High cumulative UV zone; frequently forgotten entirely |
Timing by Sunscreen Type
- Mineral (zinc oxide/titanium dioxide): Works immediately — apply right before going outdoors
- Chemical filters (avobenzone, etc.): Require 15–20 minutes of skin absorption to activate — apply before dressing
Reapplication: The Most Ignored Rule in Sun Protection
- Every 2 hours when outdoors — regardless of SPF number on the label
- Every 40–80 minutes when swimming or sweating
- Immediately after towel drying — mechanical friction strips sunscreen from skin
- Sunscreen applied at 8 AM provides zero meaningful protection by mid-afternoon
Our guide on sunburn and melanoma risk explains exactly how each unprotected UV exposure episode accumulates toward long-term melanoma development.
The 2026 DNA-Repair Ingredient Upgrade
Emerging clinical evidence supports a new generation of sunscreens incorporating photolyase enzymes and niacinamide — active ingredients that initiate repair of UV-induced DNA strand breaks post-exposure. These are supplementary to SPF, not replacements.
Per UCSF Health skin cancer prevention protocols, the foundational standard remains broad-spectrum SPF 30+ applied correctly and reapplied consistently — advanced ingredients add a second layer of cellular protection for high-risk individuals.
What This Means For You: One morning application without reapplication leaves you functionally unprotected from midday onward — regardless of whether your bottle says SPF 30 or SPF 100. Reapplication is not optional. It is the entire protocol.
Beyond the Bottle — Your Complete 2026 Melanoma Prevention Protocol
The best sunscreen for melanoma prevention is one critical pillar of a layered clinical strategy. Sunscreen use alone is not sufficient.
UV Index: Your Daily Decision Framework
| UV Index | Risk Level | Minimum Action Required |
|---|---|---|
| 1–2 | Low | SPF 15–30; limited outdoor duration fine |
| 3–5 | Moderate | SPF 30+; seek shade between 10 AM–2 PM |
| 6–7 | High | SPF 30–50+; protective clothing recommended |
| 8–10 | Very High | SPF 50+; minimise 10 AM–4 PM exposure significantly |
| 11+ | Extreme | SPF 50+; full UPF clothing mandatory |
In parts of the US Sun Belt, Arizona, and Florida, UV index exceeds 10 regularly — making SPF 50+ the non-negotiable daily standard, not just a high-exposure option.
Tanning Beds: A Direct Melanoma Cause
Tanning beds emit the same UV radiation categories as the sun. The World Health Organization classifies indoor tanning as a Group 1 carcinogen — confirmed causal agent of cancer. Any tanning bed use before age 35 increases lifetime melanoma risk by 59%. Our full breakdown of tanning beds and melanoma risk details the clinical evidence and why no SPF compensates for active UV-seeking behaviour.
Sun-Protective Clothing
- UPF 50+ rated fabrics block 98% of UV radiation — often outperforming sunscreen under real conditions
- A wide-brim hat with a 3-inch+ brim reduces facial and neck UV exposure by up to 95%
- UV-rated wraparound sunglasses protect periorbital skin — a melanoma site frequently overlooked
The Vitamin D Question — Answered
Concern: “Will daily sunscreen block my Vitamin D production?”
Clinical answer: No — not meaningfully. Real-world sunscreen use does not cause clinically significant Vitamin D deficiency. If your blood panel shows deficiency, oral Vitamin D3 supplementation is the safe evidence-based solution — not intentional unprotected UV exposure.
Genetic Risk and Family History
CDKN2A and MC1R gene mutations significantly elevate lifetime melanoma susceptibility. Two or more first-degree relatives diagnosed with melanoma places you in a high-risk category requiring SPF 50+ year-round and annual full-body dermatological skin checks. Review our complete clinical analysis of melanoma causes and risk factors to understand where you sit on the risk spectrum.
Annual Full-Body Skin Examinations
No sunscreen routine replaces professional surveillance. Melanoma detected at Stage I carries a 5-year survival rate exceeding 98%. Stage IV survival drops dramatically and treatment becomes far more complex. Annual examination is your most powerful single tool after daily sun protection.
Know the ABCDE warning signs of melanoma with our guide on melanoma warning signs and symptoms. And if you notice an unusual mole, dark streak, or skin change today, use our Symptom Checker as your first step before booking your dermatology appointment.
For additional clinical resources, the AIM at Melanoma Foundation sunscreen guide, the Melanoma Research Alliance prevention resource, and the World Health Organization’s UV radiation health effects overview offer peer-reviewed global context that extends well beyond any individual product choice.
FAQs: Best Sunscreen for Melanoma Prevention (2026)
1. What is the best sunscreen for melanoma prevention?
A broad-spectrum, water-resistant, SPF 50+ formula — zinc oxide-based mineral for high-risk or sensitive skin; well-formulated chemical for daily lightweight use. The best sunscreen is ultimately the one you apply correctly and reapply every 2 hours.
2. Does SPF 50 protect against melanoma better than SPF 30?
Marginally in theory — SPF 50 blocks 98% vs SPF 30’s 97% of UVB rays. The real advantage: higher SPF compensates for under-application, which is nearly universal. Most people apply far too little, making SPF 50 a practical buffer that brings real-world protection significantly closer to what the label claims.
3. Is mineral sunscreen better than chemical for skin cancer prevention?
For melanoma specifically, mineral (zinc oxide) is clinically preferred for high-risk patients and survivors. It provides immediate, reliable full-spectrum UVA/UVB coverage with no systemic absorption concerns. Chemical formulas are effective for daily moderate-risk use and often more cosmetically acceptable under makeup.
4. How much sunscreen do I need to prevent melanoma?
One full ounce (30 ml) for the whole body — approximately one shot glass. For the face alone, squeeze sunscreen along your index and middle fingers. Most people apply only 25% of this — dramatically reducing actual SPF performance.
5. Does sunscreen actually reduce melanoma risk?
Yes — confirmed by multiple clinical trials. A 10-year Australian RCT showed 50% reduction in new melanomas in daily sunscreen users. The ASCO-published Norwegian Women and Cancer cohort study confirmed SPF ≥ 15 reduced melanoma risk by 30% compared to lower-SPF use.
6. What SPF should melanoma survivors use?
SPF 50+ broad-spectrum mineral sunscreen, applied daily to all exposed skin including scalp, ears, lips, and hands. Coordinate with your dermatologist or oncologist for a post-treatment sun protection protocol — some patients require additional precautions based on immunosuppression status.
7. Can people with dark skin get melanoma?
Yes. Melanoma affects all skin tones. In people with darker skin, it frequently presents on palms, soles, nail beds, and mucous membranes — sites where it is routinely diagnosed late. UVA rays penetrate all skin tones and drive cumulative DNA damage regardless of melanin levels. Daily SPF is recommended universally.
8. Is SPF in moisturiser enough to prevent melanoma?
No. Studies consistently show moisturisers with SPF are applied too thinly and unevenly to achieve label-level protection outdoors. Use a dedicated broad-spectrum sunscreen as a separate product for any meaningful exposure — SPF moisturisers serve as minimal daily baseline protection indoors only.
9. Should I use sunscreen indoors to prevent melanoma?
Yes, if you spend significant time near windows. UVA rays penetrate standard glass and continue to cause skin damage during indoor exposure — particularly during long car journeys or extended window-side desk work. SPF 30+ daily is clinically advisable in these scenarios.
10. What sunscreen ingredients should I look for to prevent melanoma?
Look for zinc oxide (immediate, full UVA/UVB protection) or avobenzone paired with a UVB filter. Verify “broad spectrum” on the label. Avoid products claiming to be mineral that list homosalate, octinoxate, or oxybenzone in their ingredient list — this is the sunscreen doping pattern that compromises your intended protection.
11. Does sunscreen expire and lose protection against melanoma?
Yes. FDA regulations require sunscreens to maintain full effectiveness for 3 years. After the expiry date, UV filters degrade and actual SPF drops significantly. Discard any expired sunscreen — an expired SPF 50 bottle may deliver as little as SPF 10 in real use. Check expiry dates on every bottle at the start of each summer season.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.