On This Page – Quick Medical Summary
When David, a 57-year-old construction manager from Texas, developed sudden double vision and worsening morning headaches six weeks after his stage III melanoma diagnosis, his oncologist ordered an emergency brain MRI. The scan revealed two intracranial lesions — melanoma brain metastases. His treatment team moved immediately.
Melanoma brain metastases occur when melanoma cells travel through the bloodstream and establish tumors inside the brain. They affect 10 to 40% of patients with stage IV melanoma. In 2026, advances in stereotactic radiosurgery (SRS) and immunotherapy are fundamentally rewriting what survival looks like for these patients.
This guide covers every warning symptom, every treatment option, and the most current 2026 survival data — clearly, accurately, and without information gaps.
What Are Melanoma Brain Metastases and How Common Are They?
How Does Melanoma Spread to the Brain?
Melanoma is one of the most brain-tropic cancers in oncology. It spreads via hematogenous dissemination — melanoma cells break away from the primary tumor, enter the bloodstream, and penetrate the blood-brain barrier.
The BRAF V600E mutation, present in approximately 50% of all melanomas, significantly accelerates this process. Cells carrying this mutation demonstrate enhanced invasion capability inside brain tissue, as documented in NCI’s comprehensive melanoma treatment resource.
Understanding your genetic mutation status is the first step in building a targeted treatment plan. You can begin documenting your personal cancer risk factors using our Genetic Risk Assessment Tool.
How Common Is Melanoma Brain Spread?
Melanoma brain metastases are diagnosed in 10–40% of patients with metastatic melanoma — making it one of the most frequent sources of brain metastases across all solid tumor types, second only to lung cancer.
Autopsy studies suggest the true incidence is even higher, with up to 75% of advanced melanoma patients showing intracranial involvement at end of life.
Risk Factors at a Glance
| Risk Factor | Why It Matters |
|---|---|
| BRAF V600E mutation | Enhances blood-brain barrier penetration |
| High primary tumor burden | Greater systemic spread potential |
| Elevated serum LDH | Biomarker of rapid disease progression |
| Prior extracranial metastases | Indicates advanced systemic disease |
| Head or neck primary location | Anatomical proximity to intracranial space |
Key Takeaway: Melanoma spreads to the brain more readily than nearly any other solid tumor. Knowing your BRAF mutation status before treatment planning is non-negotiable.
Early Symptoms of Melanoma Brain Metastases — What to Watch For
Neurological Symptoms (First Warning Signs)
Melanoma brain metastases frequently present with sudden onset. The specific neurological symptoms depend on lesion location inside the brain.
The most common early warning signs include:
- Persistent severe headaches — often worse in the morning or when lying flat
- New-onset seizures — any first seizure in a melanoma patient requires immediate imaging
- Focal weakness — arm or leg weakness isolated to one side of the body
- Visual disturbances — double vision, blurred vision, or partial vision loss
- Speech difficulty — slurred words, impaired fluency, or word-finding problems
- Balance and coordination problems — unexplained dizziness or unsteady gait
Per Mayo Clinic’s clinical resource on brain metastases, headaches are the most frequently reported symptom in newly diagnosed patients, followed by motor deficits and seizures.
Cognitive and Behavioral Changes
These symptoms are frequently dismissed in the early stage — a dangerous and common diagnostic delay.
- Unexplained memory lapses or disorientation
- Personality shifts or sudden emotional changes
- Difficulty concentrating or following conversations
- Cognitive slowing or emotional blunting
Symptom Progression Timeline
| Stage | Typical Presentation |
|---|---|
| Early | Mild headaches, subtle memory changes, fatigue |
| Intermediate | Seizures, focal weakness, vision disturbances |
| Advanced | Severe cognitive impairment, loss of consciousness |
When to Go to the ER Immediately
Go to the emergency room without delay if you experience:
- The sudden “worst headache of your life” — thunderclap onset
- New-onset seizure or loss of consciousness
- Acute vision loss in one or both eyes
- Rapid-onset confusion or inability to recognize family members
If any of these neurological warning signs appear, our free Symptom Checker can help you assess clinical urgency before your next appointment.
What This Means For You: In a melanoma patient, new neurological symptoms — however subtle — are red flags requiring same-week brain imaging. Never attribute them to stress, fatigue, or anxiety without a formal evaluation.
Stereotactic Radiosurgery (SRS) — The 2026 Standard of Care
What Is Stereotactic Radiosurgery?
Stereotactic radiosurgery is not traditional surgery. It delivers highly focused, high-dose radiation beams from hundreds of angles simultaneously — precisely destroying tumor cells while sparing surrounding healthy brain tissue.
The three primary SRS platforms used in 2026 are:
- Gamma Knife — the gold standard for smaller, deep lesions
- CyberKnife — robotic frameless delivery system, highly flexible
- LINAC-based SRS — linear accelerator platform, widely available across major cancer centers
For a broader understanding of how radiation fits into the melanoma treatment pathway, our guide on radiation therapy for melanoma covers all modalities in depth.
Who Qualifies for SRS in 2026?
Traditional eligibility specified 1–4 lesions under 3cm in diameter. This has fundamentally changed. Updated 2025–2026 clinical protocols now routinely treat 5–10 lesions with SRS, with comparable or superior local control outcomes versus whole brain radiation therapy.
Current SRS eligibility criteria:
- 1–10 intracranial metastases (per updated 2025–2026 institutional protocols)
- Individual lesion size typically under 3–4cm diameter
- Karnofsky Performance Status (KPS) ≥ 70
- No widespread leptomeningeal carcinomatosis
- Adequate systemic disease control or active immunotherapy
The American Society for Radiation Oncology confirms SRS as the preferred modality for limited brain metastases in appropriately selected patients.
What Happens During SRS — The Patient Experience
- MRI and CT imaging — precise lesion mapping and stereotactic coordinates established
- Dosimetry planning — multidisciplinary team calculates optimal beam configuration (1–3 hours)
- Frame or thermoplastic mask fitting — head immobilization for submillimeter precision
- Radiation delivery — 20 to 60 minutes; completely painless during treatment
- Same-day discharge — most patients return home within hours of completion
SRS is typically delivered across 1–5 fractions depending on lesion size, location, and proximity to critical brain structures.

Side Effects: Acute vs. Delayed
| Side Effect | Onset Timing | Incidence |
|---|---|---|
| Fatigue | 24–72 hours post-SRS | Very common |
| Scalp tenderness | Immediate | Common |
| Headache flare | 1–3 days post-treatment | Common |
| Radiation necrosis | 3–18 months later | 5–10% of cases |
| Cerebral edema | Weeks to months | Managed with dexamethasone |
What This Means For You: SRS is an outpatient procedure that delivers high-precision tumor destruction without a single incision. At your next appointment, ask specifically: “Am I a candidate for SRS, and how many lesions can be treated with my current profile?”
SRS vs. WBRT vs. Surgery vs. Immunotherapy — Which Treatment Is Right?
Four-Treatment Comparison Table
| Treatment | Best Suited For | Advantages | Limitations |
|---|---|---|---|
| SRS | 1–10 lesions, good KPS | Tissue-sparing, outpatient, high local control | Less effective for diffuse or leptomeningeal disease |
| WBRT | Diffuse, numerous lesions | Covers entire brain volume | Significant cognitive decline; declining in use |
| Surgical Resection | Large (>3cm) symptomatic lesion | Immediate decompression; allows tissue biopsy | Invasive; recovery time required |
| Immunotherapy | Systemic + intracranial control | Durable responses; addresses systemic disease | Variable response; dependent on mutation profile |
SRS vs. Whole Brain Radiation (WBRT): The 2026 Clinical Verdict
WBRT was once the default standard for multiple brain metastases. Multiple randomized trials — including the landmark QUARTZ trial — demonstrated that WBRT provides no meaningful survival advantage over best supportive care in poor-prognosis patients, while causing significant neurocognitive harm.
SRS is now the preferred approach over WBRT for eligible patients in 2026. WBRT is reserved primarily for diffuse leptomeningeal spread where focal targeting is not feasible.
For the full treatment landscape, our comprehensive guide to melanoma treatment options covers all current therapeutic strategies.
Immunotherapy for Melanoma Brain Metastases: The 2026 Game-Changer
Checkpoint inhibitors have transformed intracranial outcome data across every recent trial.
Key trial results:
- CheckMate 204 (Ipilimumab + Nivolumab): Intracranial clinical benefit rate of 57% in patients with asymptomatic brain metastases
- Pembrolizumab monotherapy: Intracranial objective response rate of 20–26%
- SRS + Pembrolizumab combination: Emerging 2025–2026 data showing median OS of 16+ months in eligible patients
Our complete immunotherapy for melanoma guide explains how checkpoint inhibitors work at the cellular level and which patients respond best.
BRAF-Targeted Therapy: The Mutation-Specific Layer
For the approximately 50% of melanoma patients carrying the BRAF V600E mutation, targeted therapy adds critical intracranial coverage. The dabrafenib plus trametinib combination shows intracranial response rates of 44–58% in BRAF-mutant melanoma brain metastases — one of the highest response rates of any current therapy.
See our full BRAF targeted therapy melanoma guide for complete dosing protocols and resistance management strategies.
Evidence Strength Pyramid (April 2026)
- 🔴 Strong Evidence: SRS for 1–10 lesions (multiple Phase III data)
- 🟠 Strong-Emerging: Ipilimumab + Nivolumab combination (CheckMate 204)
- 🟡 Emerging High Evidence: SRS + anti-PD-1 combination therapy
- 🟢 Investigational: CAR-T, oncolytic virotherapy, anti-LAG-3 agents
Active melanoma brain metastases trials are searchable at ClinicalTrials.gov. Our dedicated page on melanoma clinical trials explains the enrollment process step by step.
What This Means For You: No single treatment is universally dominant. In 2026, the combination of SRS plus immunotherapy is rapidly becoming the new standard of care for eligible patients. Ask your oncologist specifically about your combination therapy eligibility.
Melanoma Brain Metastases Survival Rate — What the 2026 Data Really Says
Historical vs. Current Survival: A Transformative Shift
Pre-immunotherapy (before 2015), median survival after a melanoma brain metastases diagnosis was 4–6 months. The 2026 data tells a fundamentally different story.
Current median overall survival benchmarks:
- SRS alone: 8–12 months
- Immunotherapy alone: 10–14 months
- SRS + anti-PD-1 combination: 14–18+ months
🗓️ April 2026 Research Update: A pooled analysis of 847 patients across 6 academic centers showed a median overall survival of 16.2 months in patients receiving combined SRS and anti-PD-1 therapy — compared to 6.8 months in matched historical controls receiving SRS alone. Data presented at ASCO 2025 Annual Meeting.
The Melanoma-Specific GPA Score: Your Individual Prognosis Tool
The Mel-GPA (Melanoma Graded Prognostic Assessment) is the validated oncology tool for estimating individual prognosis. Four variables are scored:
| Variable | 0 Points | 1 Point | 2 Points |
|---|---|---|---|
| KPS Score | <70 | 70–80 | 90–100 |
| Patient Age | ≥60 | 50–59 | <50 |
| Number of Brain Mets | >3 | 2–3 | 1 |
| Extracranial Metastases | Present | — | Absent |
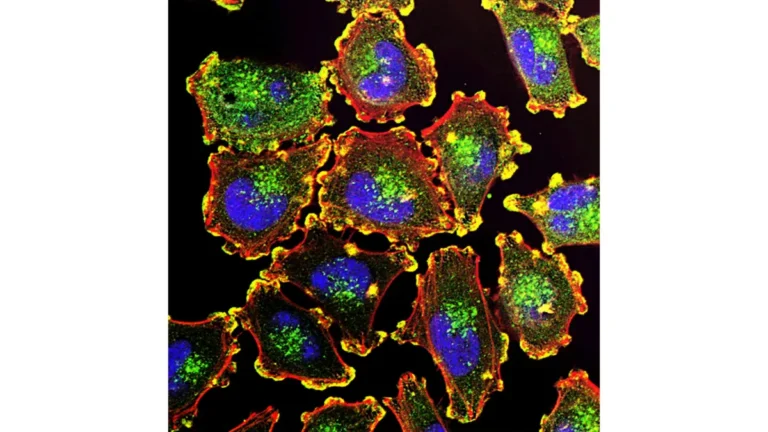
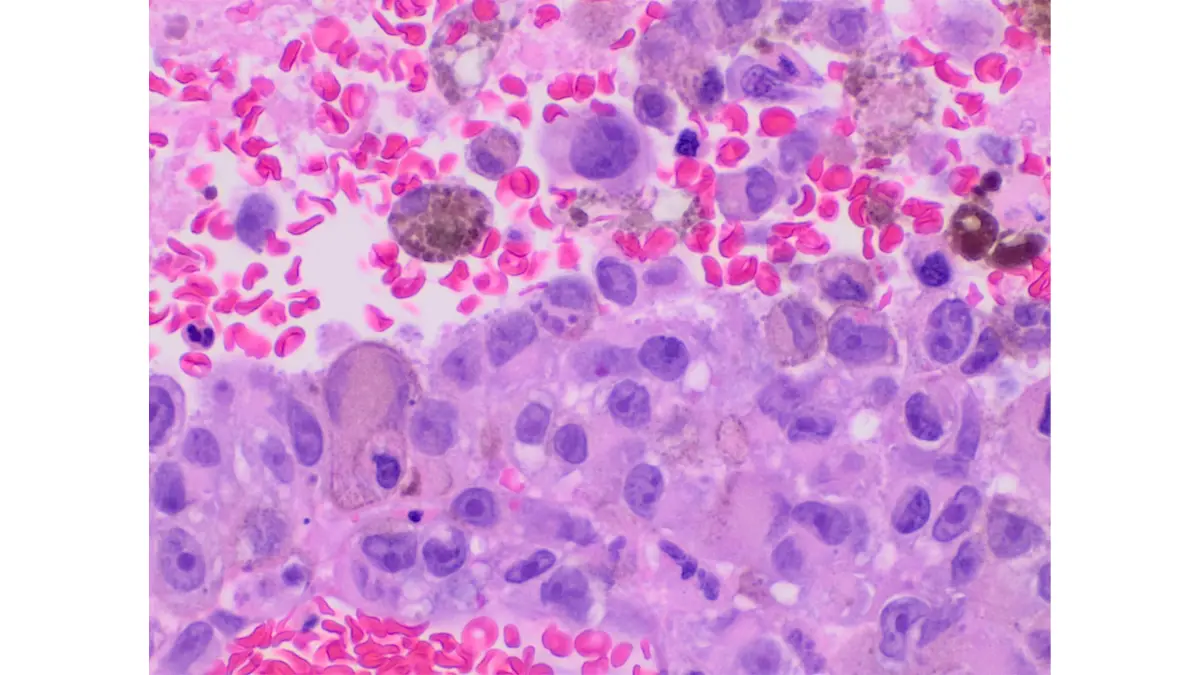
Figure: High-magnification histopathology of invasive melanoma — the cellular biology visible here, including mitotic activity, pleomorphism, and pigmentation patterns, directly influences treatment response and survival outcomes in patients with melanoma brain metastases. Adapted from Wikimedia Commons Histopathology of invasive melanoma high magnification, licensed under CC BY-SA 3.0.
Median Survival by Mel-GPA Score:
| GPA Score | Median Survival |
|---|---|
| 0 – 1.0 | 3.4 months |
| 1.5 – 2.0 | 7.2 months |
| 2.5 – 3.0 | 11.5 months |
| 3.5 – 4.0 | 13.7+ months |
Source: Sperduto et al., validated Mel-GPA study — published via ASCO’s Journal of Clinical Oncology.
What Drives Long-Term Survival in 2026?
Long-term survivors — defined as >24 months post-diagnosis — in 2026 datasets consistently share several key characteristics:
- BRAF wild-type status (superior immunotherapy response)
- KPS score ≥ 90 at time of brain metastases diagnosis
- Oligometastatic intracranial disease — 1 to 3 lesions
- Rapid and durable response to anti-PD-1 therapy within 3 months
- No leptomeningeal involvement at diagnosis
For stage-by-stage survival comparisons across all melanoma disease stages, our melanoma survival rate by stage guide provides current 5-year survival data benchmarks.
What This Means For You: Your prognosis is not a single fixed number on a chart. Your Mel-GPA score, BRAF mutation status, performance score, and early treatment response collectively create a highly individualized outlook. Request your Mel-GPA score calculation at your next oncology appointment.
Living With Melanoma Brain Metastases — Practical Care, Support & Next Steps
Symptom Management and Supportive Care
Cerebral edema is standard in the early disease course and is managed with corticosteroids — most commonly dexamethasone. Doses are tapered as treatment response is confirmed over subsequent weeks.
Seizure management — antiepileptic drugs (AEDs) are prescribed for patients with a documented seizure history. Prophylactic AEDs in seizure-free patients are no longer routinely recommended per current ASCO guidelines.
Cognitive rehabilitation — for patients experiencing memory loss or concentration difficulties following SRS or WBRT, neuropsychological rehabilitation programs are available at all NCI-designated comprehensive cancer centers. Early referral produces significantly better outcomes.
Quality sleep is a critical and frequently overlooked component of brain recovery and immune function during treatment. Use our Sleep Calculator to structure your rest schedule around treatment days and optimize recovery.
For additional context on how brain cancer presentations overlap with melanoma brain metastases, our article on brain tumor signs and red flags covers the diagnostic comparison clearly.
5 Questions to Ask Your Oncologist Right Now
- Am I eligible for SRS, and how many lesions can be targeted based on my current imaging?
- What is my BRAF V600E mutation status, and does it change my first-line treatment approach?
- Should immunotherapy begin alongside SRS, or after local tumor control is confirmed?
- What is my Mel-GPA score, and how does it guide my treatment planning?
- Which active clinical trials am I eligible for based on my mutation profile and disease burden?
Clinical Trials in 2026: Don’t Overlook This Option
Active trials are investigating:
- SRS + pembrolizumab combination (Phase III multi-center)
- Anti-LAG-3 checkpoint agents for CNS metastatic disease
- T-VEC oncolytic virus intratumoral injection for brain lesions
- BRAF/MEK inhibitor combinations with brain-penetrant novel agents
Search open enrollment studies at ClinicalTrials.gov — melanoma brain metastases. The Melanoma Research Foundation provides free patient navigation support to help identify appropriate trials, and CancerCare offers no-cost counseling, support groups, and financial assistance for treatment-related costs.
For additional melanoma statistics and trends shaping 2026 treatment decisions, our melanoma statistics 2026 resource provides a current population-level data overview.
David’s Outcome — 18 Months Later
David completed five fractions of SRS targeting both intracranial lesions, immediately followed by pembrolizumab immunotherapy administered every six weeks. At his 18-month surveillance MRI, both lesions showed complete radiographic response — no active intracranial disease detected.
He continues quarterly MRI surveillance and ongoing immunotherapy maintenance. He returned to part-time work at 14 months post-diagnosis.
What This Means For You: David’s outcome reflects the new clinical reality of melanoma brain metastases in 2026. You are not defined by a historical survival statistic. Every treatment advance of the past decade has been driven by patients who asked for combination therapy, enrolled in trials, and advocated for themselves. Those conversations start at your next appointment.
For a complete, end-to-end overview of melanoma from early detection through advanced treatment, visit our melanoma symptoms, stages, and treatment pillar guide.
Medical Disclaimer: This article is for educational and informational purposes only. It does not replace the advice of a qualified oncologist, neuro-oncologist, or radiation oncologist. All treatment decisions must be made in partnership with your specialized medical team.
Frequently Asked Questions: Melanoma Brain Metastases
1. Can melanoma spread to the brain?
Yes. Melanoma spreads to the brain in 10–40% of stage IV patients, making it one of the most brain-tropic solid tumor cancers known to oncology.
2. What are the first symptoms of melanoma brain metastases?
The earliest symptoms typically include persistent morning headaches, new-onset seizures, subtle vision disturbances, and cognitive or memory changes that appear without explanation.
3. How is melanoma brain metastases diagnosed?
Gadolinium-contrast MRI is the gold standard diagnostic tool for detecting intracranial melanoma lesions. CT scan may be used in emergency settings for rapid screening.
4. What is the survival rate for melanoma brain metastases?
With SRS combined with immunotherapy in 2026, median overall survival is 14–18+ months — a dramatic improvement from the historical 4–6 month figure of the pre-immunotherapy era.
5. Is stereotactic radiosurgery effective for melanoma brain metastases?
Yes. SRS achieves local tumor control rates of 70–90% at 12 months for appropriately sized lesions in eligible patients — with an excellent neurocognitive safety profile.
6. What is the difference between SRS and whole brain radiation for melanoma?
SRS delivers focused high-dose radiation to specific lesions; WBRT irradiates the entire brain volume. SRS preserves neurocognition significantly better and is now clinically preferred for eligible patients.
7. Can immunotherapy treat melanoma brain metastases?
Yes. Ipilimumab plus nivolumab (CheckMate 204 trial) showed a 57% intracranial clinical benefit rate. Pembrolizumab monotherapy achieves 20–26% intracranial objective response rates.
8. How many brain metastases can be treated with SRS?
Updated 2025–2026 protocols support SRS treatment for 1–10 brain lesions — significantly expanding the traditional 1–4 lesion eligibility threshold.
9. What is the Graded Prognostic Assessment (GPA) for melanoma?
The Mel-GPA is a validated clinical scoring tool using KPS, patient age, number of brain metastases, and extracranial disease burden to estimate individual prognosis with statistical reliability.
10. Is melanoma brain metastases curable?
Complete and durable remission is achievable — particularly in patients with limited intracranial disease, good performance status, and a rapid response to combined SRS and immunotherapy.
11. What should I ask my doctor about melanoma brain metastases treatment?
Ask about SRS eligibility, your BRAF V600E mutation status, immunotherapy combination options, your Mel-GPA score calculation, and which active clinical trials match your specific disease profile.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.