On This Page – Quick Medical Summary
James, 51, was diagnosed with Stage III melanoma after a mole on his back changed shape over three months. His oncologist at MD Anderson presented him with five different treatment paths — not one. Two years later, after combination immunotherapy, James is in complete remission.
His story reflects the revolution in melanoma treatment options that has transformed outcomes since 2015 — and accelerated dramatically in 2026.
If you or someone you love has just received a melanoma diagnosis, here is what you need to know:
Melanoma treatment options in 2026 include surgery, immunotherapy, targeted therapy, radiation, and emerging mRNA vaccines. The right approach depends on your stage, BRAF mutation status, and overall health. Early-stage melanoma is cured by surgery alone in up to 99% of cases. Advanced melanoma now achieves response rates above 85% with combination checkpoint immunotherapy.
How Doctors Choose Your Melanoma Treatment in 2026
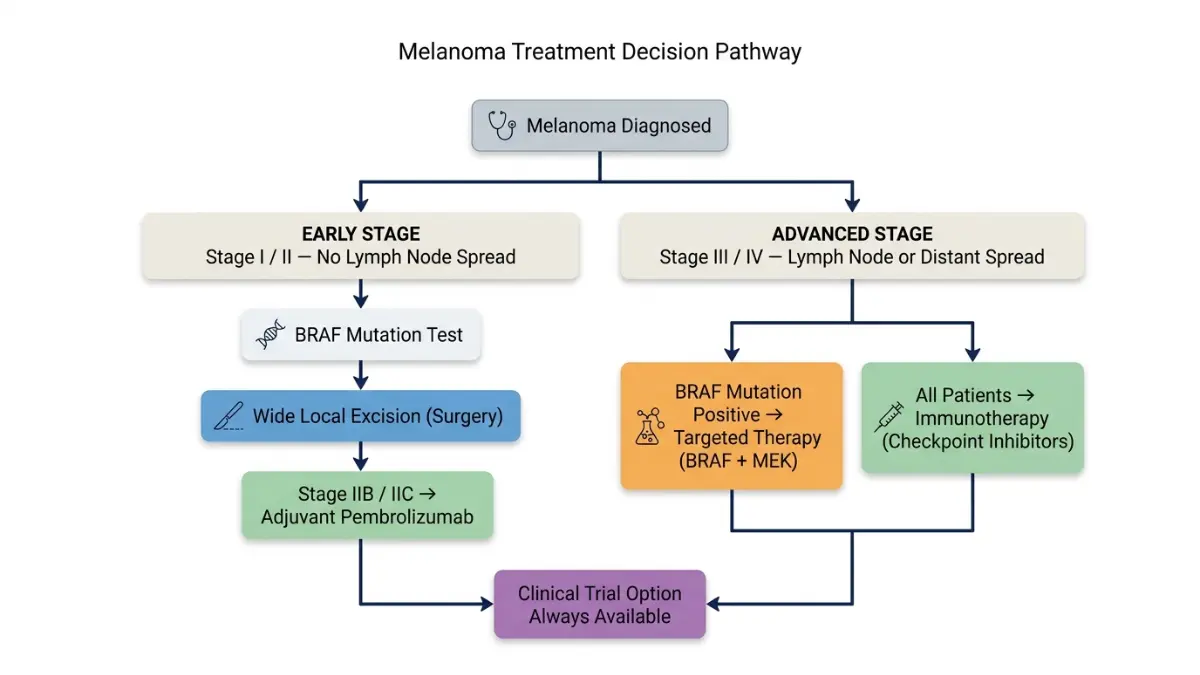
Not all melanoma treatments are created equal — and no two treatment plans are identical. Your oncologist will base every decision on three core factors:
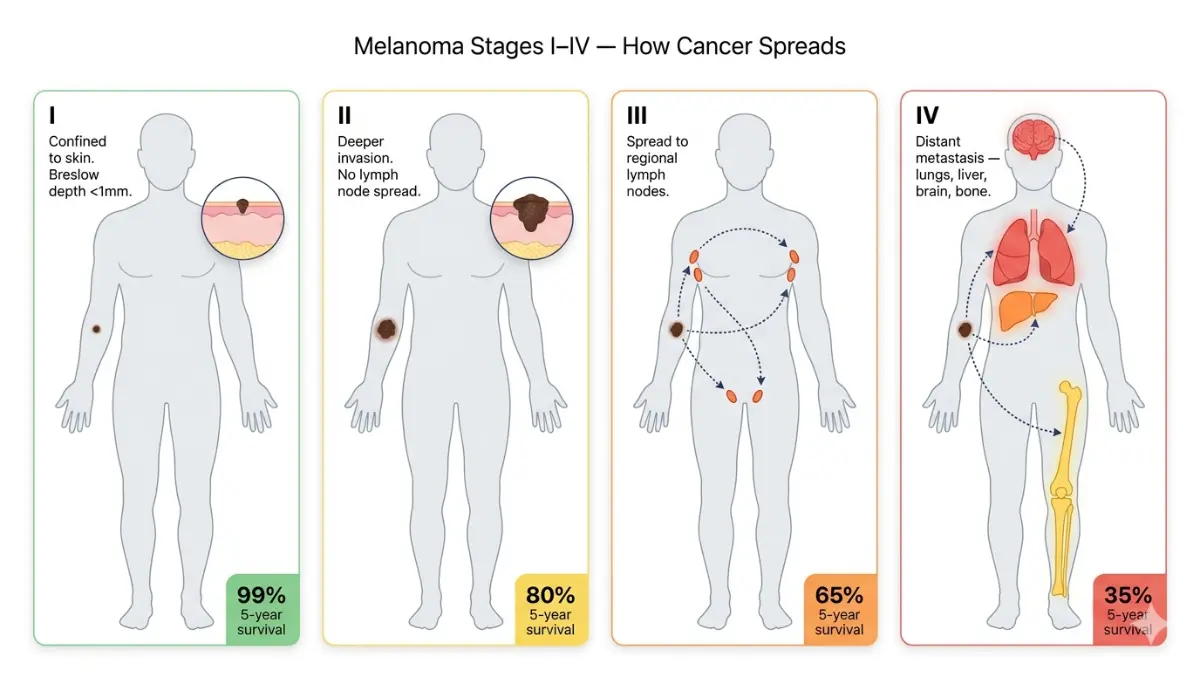
- Stage — how far the melanoma has spread (learn about melanoma stages and what each one means for your prognosis)
- BRAF mutation status — approximately 50% of cutaneous melanomas carry a BRAF V600 mutation, which unlocks an entirely different treatment category
- Overall health — your fitness for surgery, immune system strength, and organ function
Why BRAF testing now matters from Stage IIB onwards: Both the ESMO 2024 Clinical Practice Guidelines and the NCCN 2025–2026 Melanoma Guidelines now recommend BRAF V600 mutation testing starting at Stage IIB. This single blood and biopsy result determines whether targeted therapy is an option alongside immunotherapy.
Quick Treatment Pathway at a Glance
| Melanoma Stage | Primary Approach | Additional Consideration |
|---|---|---|
| Stage 0–I | Surgery (WLE) | Observation only |
| Stage II | Surgery + possible adjuvant therapy | BRAF test from IIB |
| Stage III | Surgery + immunotherapy | Targeted therapy if BRAF+ |
| Stage IV | Combination immunotherapy or targeted therapy | TIL therapy, clinical trials |
💡 What This Means For You: Before any treatment begins, ask your oncologist for a BRAF mutation test. This single result can completely change your treatment plan.
If you have a family history of melanoma, use our Genetic Risk Assessment Tool to understand your hereditary risk profile before your next dermatology appointment.
Surgery — The First-Line Standard for Melanoma Treatment
For early-stage melanoma, surgery is the most effective melanoma treatment option available — and often the only one needed.
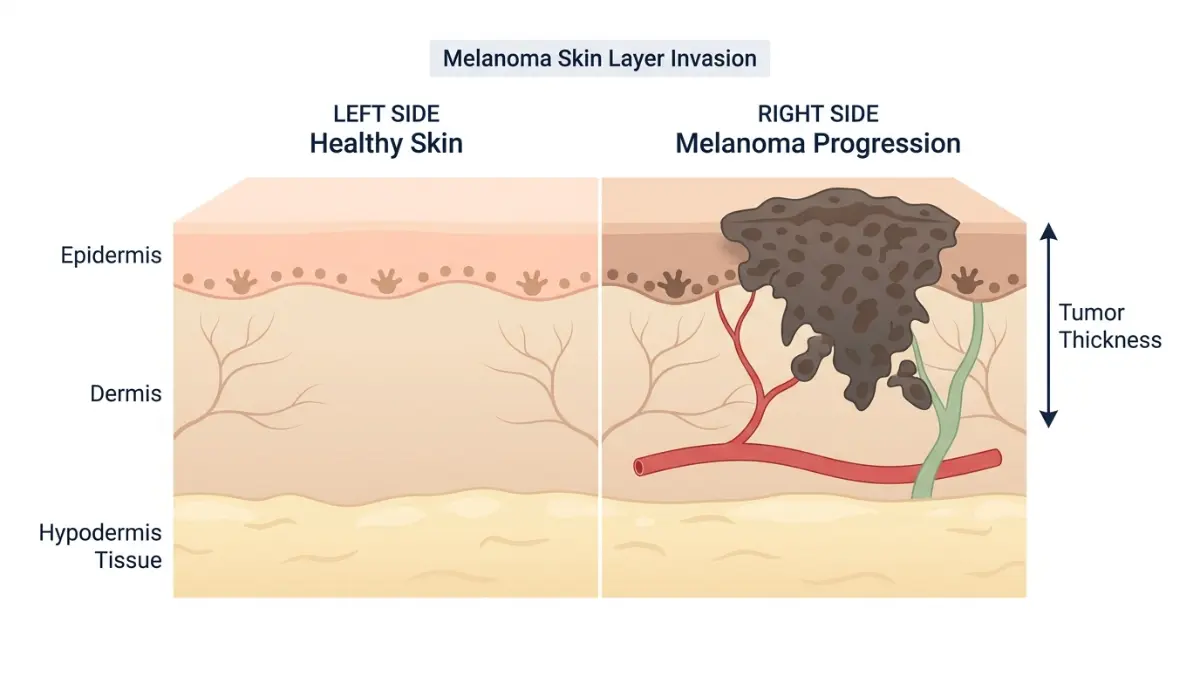
Wide Local Excision (WLE)
WLE is the standard procedure for all stages. The surgeon removes the melanoma plus a margin of healthy tissue. Margin width increases with tumor thickness (Breslow depth): 1 cm for thin melanomas, up to 2 cm for thicker tumors.
Stage 0–II melanoma is cured by surgery alone in 85–99% of cases, according to the National Cancer Institute’s melanoma treatment guidelines.
Sentinel Lymph Node Biopsy (SLNB)
SLNB is recommended for tumors thicker than 0.8 mm or with high-risk features. It identifies whether cancer has reached the nearest lymph nodes. You can read our detailed guide on sentinel lymph node biopsy to understand exactly what to expect before, during, and after the procedure.
2024–2026 Update: CLND No Longer Standard
Complete Lymph Node Dissection (CLND) has been largely replaced by active surveillance with ultrasound in patients with micrometastatic disease in lymph nodes. This change reduces lymphedema risk without compromising survival.
Side effects of surgery: wound healing time, temporary swelling, and in rare cases, lymphedema (fluid buildup in the limbs).
Melanoma Immunotherapy — FDA-Approved Options & 2026 Survival Data
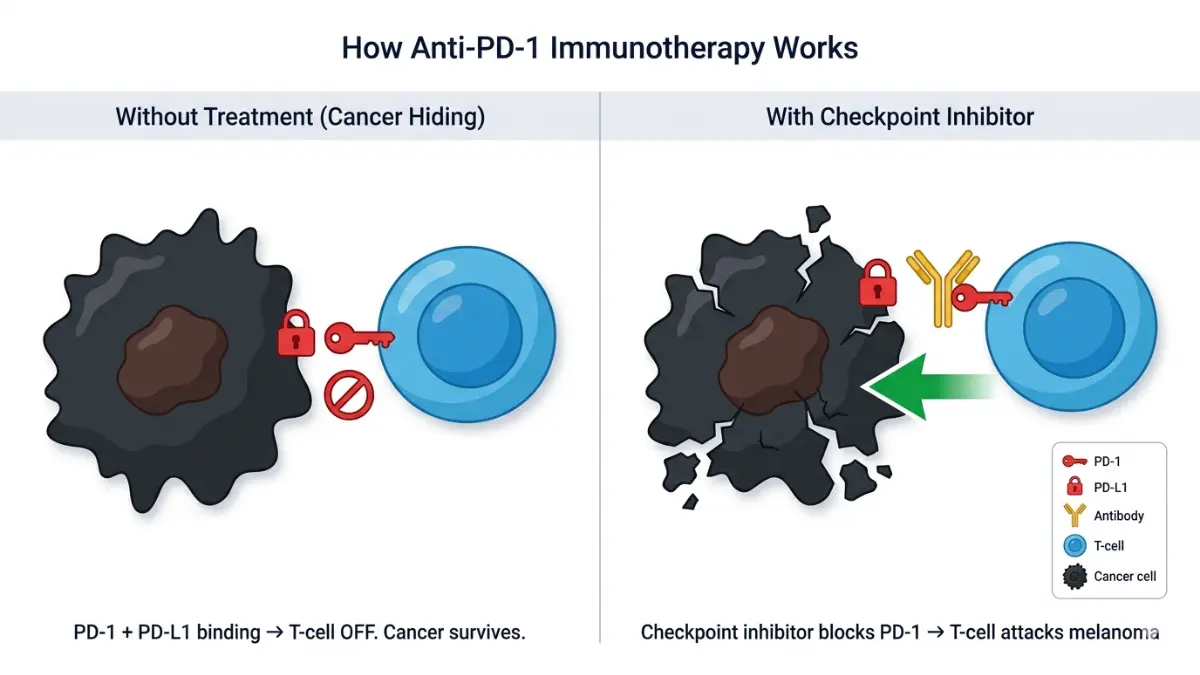
Immunotherapy has fundamentally redefined advanced melanoma treatment. It works by removing the molecular “brakes” that cancer cells use to hide from your immune system. For comprehensive background on how these drugs work, visit our guide on how immunotherapy works.
Checkpoint Inhibitors (Anti-PD-1 / Anti-CTLA-4 / Anti-LAG-3)
These are the backbone of Stage III and IV melanoma treatment in 2026. The Melanoma Research Alliance classifies currently approved options as follows:
| Drug (Brand) | Mechanism | Key Data |
|---|---|---|
| Pembrolizumab (Keytruda) | Anti-PD-1 | Approved Stage III adjuvant + Stage IV |
| Nivolumab (Opdivo) | Anti-PD-1 | First-line Stage IV; adjuvant Stage III |
| Nivolumab + Ipilimumab (Yervoy) | PD-1 + CTLA-4 | >50% of patients alive at 5 years |
| Relatlimab + Nivolumab (Opdualag) | LAG-3 + PD-1 | FDA-approved 2022; improved PFS vs. nivolumab alone |
The combination of nivolumab + ipilimumab remains one of the most powerful first-line options for Stage IV melanoma. In the pivotal trial, more than half of patients treated with this combination were still alive five years later — a milestone unthinkable a decade ago, per NCI research advances.
TIL Therapy — The 2024 FDA Breakthrough
Lifileucel (AMTAGVI) became the first cellular immunotherapy approved for metastatic melanoma in February 2024. It is designed for patients who have already failed PD-1 therapy.
The process:
- A patient’s tumor-infiltrating lymphocytes (T cells) are extracted
- Expanded in the lab to billions of cells
- Reinfused into the patient after lymphodepletion
Response rate: ~36% in patients with refractory Stage IV melanoma — a significant achievement in a population with very few options remaining.
T-VEC (Talimogene Laherparepvec)
T-VEC is an oncolytic virus therapy injected directly into accessible tumors. It is best suited for Stage IIIB–IVM1a patients with injectable lesions that cannot be surgically removed.
2026 Update: A next-generation oncolytic virus, vusolimogene oderparepvec (RPI), received an FDA review date of April 2026 after achieving a 32.9% objective response rate in trials — including shrinkage of tumors that were never directly injected.
💡 What This Means For You: If your melanoma is Stage III or IV, combination checkpoint immunotherapy — not chemotherapy — is the standard of care in 2026. Ask your oncologist about Opdualag or nivolumab + ipilimumab as first-line options.
If you want to track treatment-related symptoms at home, our Symptom Checker can help you log and identify patterns before your next oncology appointment.
BRAF & MEK Targeted Therapy — For BRAF-Mutated Melanoma
Targeted therapy for melanoma applies to approximately 50% of patients with cutaneous melanoma — specifically those whose tumors carry a BRAF V600 mutation (V600E or V600K).
FDA-Approved BRAF + MEK Inhibitor Combinations
| Combination | Brand Names | Key Benefit |
|---|---|---|
| Dabrafenib + Trametinib | Tafinlar + Mekinist | First approved combo; strong response rate |
| Vemurafenib + Cobimetinib | Zelboraf + Cotellic | Well-established for Stage IV |
| Encorafenib + Binimetinib | Braftovi + Mektovi | Improved tolerability; fewer febrile events |
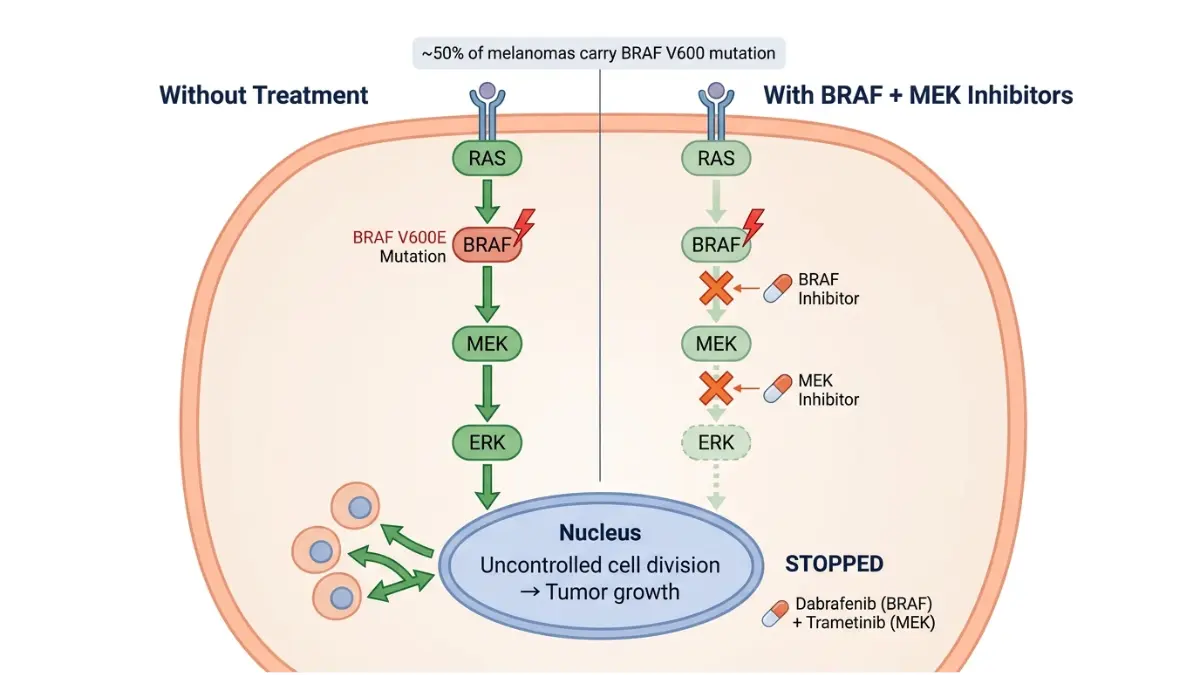
Why combination BRAF + MEK is standard: using a BRAF inhibitor alone accelerates resistance. Adding a MEK inhibitor delays this and improves overall survival.
The Critical Challenge: Most patients develop resistance within 9–12 months. Oncologists are now studying whether sequencing targeted therapy before immunotherapy (or vice versa) improves long-term outcomes — several Phase III trials are currently answering this.
Common side effects: fever, rash, joint pain, photosensitivity, and fatigue. These differ meaningfully from immunotherapy side effects and are typically more manageable with dose adjustments.
New Melanoma Treatments in 2026 — Vaccines, Cell Therapy & Clinical Trials
The melanoma treatment landscape in 2026 includes three genuinely novel approaches that no competitor article covers comprehensively.
Personalized mRNA Cancer Vaccine (mRNA-4157 / V940)
This is the most anticipated development in melanoma research. The mRNA-4157 vaccine — developed using the same platform as COVID-19 vaccines — is personalized to each patient’s tumor mutations.
Phase IIb results (KEYNOTE-942 trial): mRNA-4157 combined with pembrolizumab reduced recurrence risk by 44% compared to pembrolizumab alone in high-risk Stage III/IV patients after surgery. Full Phase III data is expected in 2027–2028.
A recent review published on PubMed/NIH highlights this as among the most promising adjuvant data in melanoma history.
Bispecific Antibodies & TCR Therapies
Tebentafusp-tebn (Kimmtrak) — approved in 2022 — is the first T-cell receptor therapy and the first bispecific T-cell engager approved for a solid tumor. It is specifically for uveal (eye) melanoma. Next-generation bispecific antibodies are in Phase I/II trials for cutaneous melanoma.
Fecal Microbiome Transplant (FMT) as Immunotherapy Booster
Emerging 2025 data shows that gut microbiome composition directly influences checkpoint inhibitor response rates. FMT is not yet standard care, but trials are enrolling at major cancer centers in the US and Europe.
Should You Consider a Clinical Trial?
According to the AIM at Melanoma Foundation, “If you aren’t considering clinical trials, you aren’t considering all your treatment options.” This is especially true for Stage III/IV patients who have progressed after first-line therapy. Find open US trials at ClinicalTrials.gov.
💡 What This Means For You: The mRNA melanoma vaccine is not yet FDA-approved, but Phase III trials are enrolling. Ask your oncologist whether you qualify for KEYNOTE-942 or a related trial.
For up-to-date data on how survival rates differ by stage, read our deep-dive on melanoma survival rate by stage.
Melanoma Treatment by Stage — Decision Guide, Side Effects & Costs
Stage-by-Stage Quick Reference Table
| Stage | Primary Treatment | 5-Year Survival (USA 2026) |
|---|---|---|
| Stage 0 (in situ) | Wide Local Excision | ~99% |
| Stage I | WLE ± SLNB | 98–99% |
| Stage II | WLE + SLNB; adjuvant pembrolizumab (IIB/IIC) | 65–90% |
| Stage III | Surgery + adjuvant immunotherapy | 40–78% |
| Stage IV | Combination immunotherapy / BRAF+MEK; TIL therapy | 20–35% |
Source: Skin Cancer Foundation — Melanoma Treatment Overview
Common Side Effects: Immunotherapy vs. Targeted Therapy
Immunotherapy (immune-related adverse events / irAEs):
- Fatigue, skin rash, colitis (bowel inflammation)
- Thyroid dysfunction — monitor with regular TSH testing; use our Blood Sugar Converter alongside thyroid tracking if on steroids
- Most irAEs are manageable with corticosteroids and dose holds
Targeted Therapy (BRAF+MEK):
- Fever, joint pain, photosensitivity, elevated liver enzymes
- Generally more predictable and dose-adjustable than immunotherapy irAEs
Maintaining strength and muscle mass during treatment is critical. Use our Protein Intake Calculator to ensure adequate daily protein intake, and our Sleep Calculator to optimize recovery sleep during treatment cycles.
Financial Reality for US Patients in 2026
Melanoma treatment costs are significant — and under-discussed:
| Treatment | Monthly Cost (Without Insurance) |
|---|---|
| Pembrolizumab (Keytruda) | ~$15,000–$20,000/month |
| Nivolumab + Ipilimumab | ~$25,000–$35,000/month |
| BRAF+MEK combo | ~$10,000–$18,000/month |
| TIL therapy (Lifileucel) | ~$500,000+ (one-time, inpatient) |
| Clinical trial participation | Drug cost: $0 |
Patient assistance programs:
- Merck’s Merck Access Program (MAP) — for Keytruda
- Bristol-Myers Squibb’s BMS Access Support — for Opdivo and Yervoy
- CancerCare Financial Assistance — copay assistance, transport, counseling
For Stage IV outcomes and what drives survival differences, our article on Stage 4 melanoma survival and therapy provides the most current data.
After Melanoma Treatment: Monitoring & Survivorship
Active surveillance after treatment is essential. Recurrence is most common in the first 2–3 years after completing therapy.
Standard follow-up schedule:
- Every 3–6 months for the first 2 years — full skin exam + lymph node check + imaging (CT or PET-CT by stage)
- Annually from year 3 onwards
5–8% of melanoma survivors develop a second primary melanoma. Daily SPF 50+ sunscreen, protective clothing, and annual full-body skin checks are non-negotiable. For a complete understanding of how melanoma is diagnosed during follow-up, including what dermoscopy and imaging look for, read our detailed guide.
Stay informed about emerging diagnostic tools — our article on melanoma AI screening and survival in 2026 covers how machine learning is changing early detection.
Frequently Asked Questions About Melanoma Treatment Options
1. What is the most effective melanoma treatment in 2026?
For Stage III/IV: combination nivolumab + ipilimumab immunotherapy. For Stage I/II: wide local excision surgery, which achieves cure rates up to 99%.
2. Can melanoma be completely cured?
Yes. Stage 0–I melanoma has a 98–99% cure rate with surgery. Even Stage IV outcomes have improved dramatically — approximately 35% of patients survive 5+ years, up from under 10% in 2010.
3. What is the first treatment for Stage 4 melanoma?
Combination immunotherapy (nivolumab + ipilimumab) or BRAF+MEK targeted therapy if BRAF-mutated — determined by your oncologist after full molecular profiling.
4. How long does melanoma treatment last?
Surgery: days to weeks recovery. Adjuvant immunotherapy: typically 12–18 months of cycles. Targeted therapy: continuous until disease progression.
5. Is melanoma immunotherapy covered by insurance in the US?
FDA-approved immunotherapies are generally covered under most US insurance plans. Patient assistance programs exist to cover gaps. Confirm with your insurer before starting.
6. What is TIL therapy for melanoma?
Tumor-Infiltrating Lymphocyte (TIL) therapy, brand name Lifileucel (AMTAGVI), is a cellular immunotherapy FDA-approved in 2024 for patients who have failed prior PD-1 therapy.
7. What does a BRAF mutation mean for my melanoma treatment?
Approximately 50% of melanomas carry the BRAF V600 mutation. If positive, you qualify for BRAF+MEK inhibitor combination therapy — a fast-acting targeted option especially useful when rapid tumor shrinkage is needed.
8. Is there a melanoma vaccine available in 2026?
The personalized mRNA vaccine (mRNA-4157/V940 + pembrolizumab) is currently in Phase III trials — not yet FDA-approved. Phase IIb data showed a 44% reduction in recurrence risk. Ask your oncologist about eligibility.
9. What are the side effects of melanoma immunotherapy?
Immune-related adverse events (irAEs) include fatigue, rash, colitis, thyroid dysfunction, and in rare cases, hepatitis or pneumonitis. Most are manageable with corticosteroids and treatment holds.
10. Can melanoma spread to the brain, and how is it treated?
Yes — brain metastases affect approximately 40–60% of Stage IV melanoma patients. Treatment combines stereotactic radiosurgery (SRS) with checkpoint immunotherapy. Outcomes have improved significantly since 2015.
11. How often should I be monitored after melanoma treatment ends?
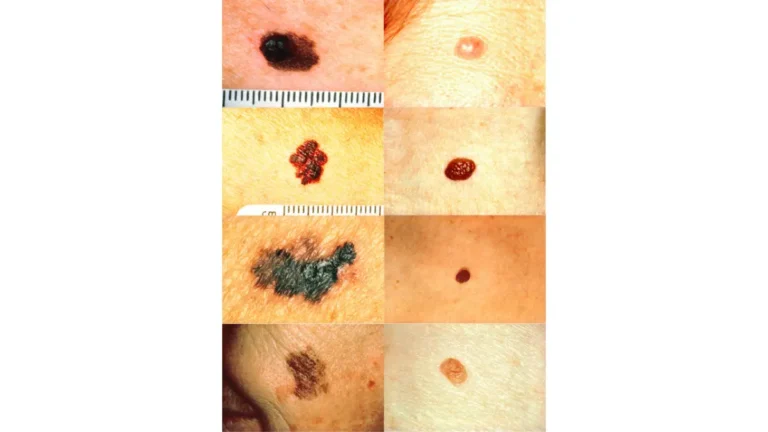
Every 3–6 months for the first 2 years, including full skin examination and imaging by stage. From year 3, annual checks are standard. Report any new or changing moles immediately using the ABCDE warning signs guide.
Sources: NCI Melanoma Treatment PDQ · NCI Skin Cancer Research · Skin Cancer Foundation · Melanoma Research Alliance · AIM at Melanoma Foundation · ClinicalTrials.gov · NIH/PMC Immunotherapy Review · CancerCare
This article is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a board-certified oncologist or dermatologist for personalized guidance. Treatment guidelines evolve rapidly — verify current standards with your healthcare provider.
🔗 Continue Reading:
- Melanoma Stages: What Each One Means for Your Treatment
- Melanoma Survival Rate by Stage — 2026 Data
- How Is Melanoma Diagnosed? Every Test Explained
- Melanoma Warning Signs & Symptoms
- Complete Melanoma Guide: Symptoms, Stages & Treatment
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.