On This Page – Quick Medical Summary
Marcus Rodriguez, 44, was told his melanoma had spread to his lungs and liver. Two rounds of pembrolizumab had failed. In February 2024, he became one of the first patients to receive FDA-approved TIL cell therapy at a major cancer center. Fourteen months later, his scans show no evidence of disease.
His story is not an outlier. It is where medicine now stands.
Stage 4 melanoma — also called metastatic melanoma — means cancer has spread through the bloodstream or lymphatic system to distant organs. The 5-year survival rate is now 35–52%, compared to under 10% before 2011. Here is everything you need to know about prognosis, treatment options, and your immediate action plan.
📌 Disclaimer: This article is for educational purposes only and does not constitute medical advice. All treatment decisions for stage 4 melanoma should be made in consultation with a board-certified oncologist.
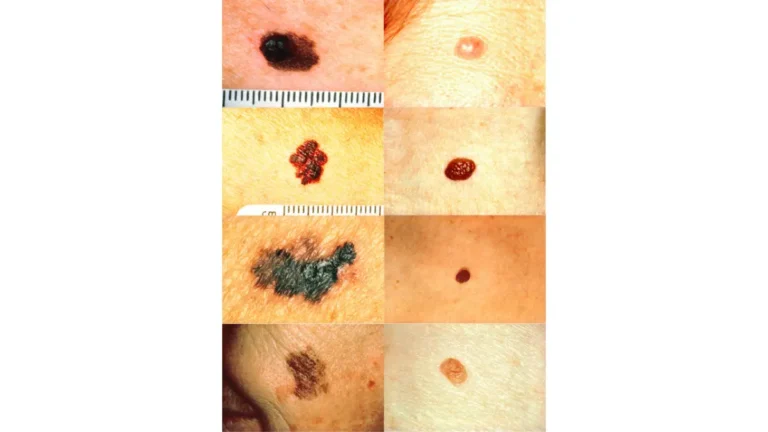
What Is Stage 4 Melanoma? Sub-Stages, Spread Sites & Diagnosis
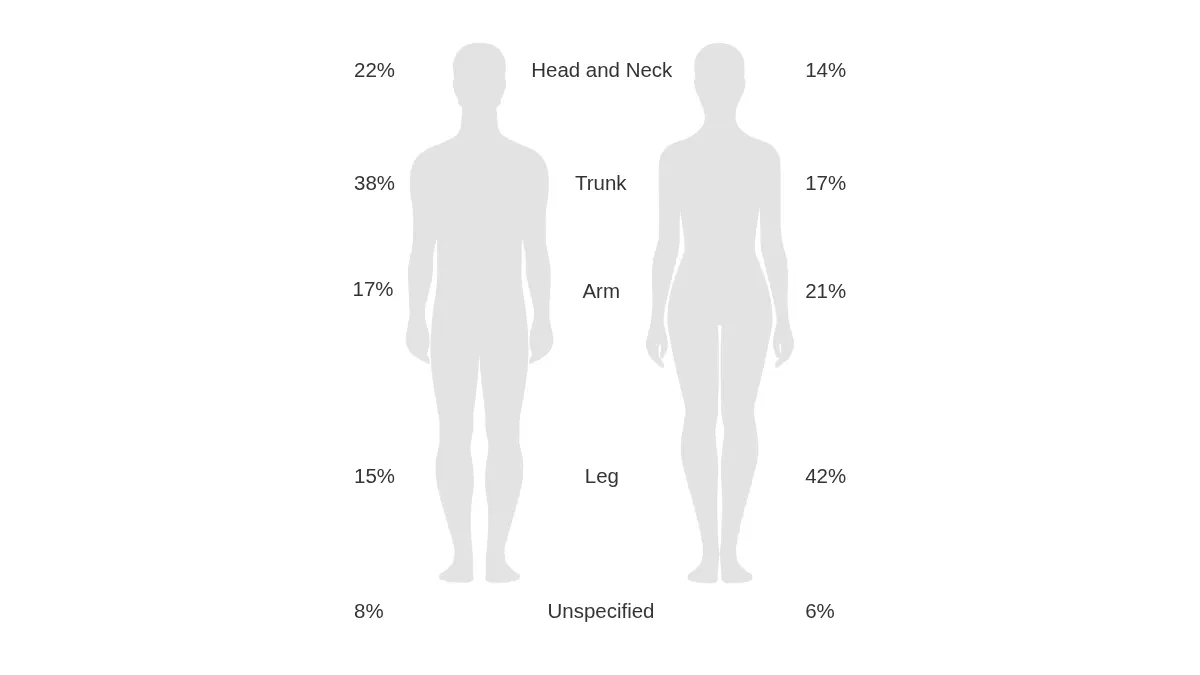
Stage 4 melanoma, clinically classified as distant metastatic melanoma, means the cancer has traveled beyond the original skin site and regional lymph nodes to other parts of the body. Common spread sites include the lungs, liver, brain, bone, gastrointestinal tract, and distant skin.
Use our Symptom Checker if you are monitoring unexplained symptoms that may warrant urgent evaluation.
The M1a–M1d Sub-Stages: Why Your Specific Sub-Stage Changes Everything
Most competitors report “stage 4” as a single category — that is clinically inaccurate and misleading. The AJCC 8th Edition staging system divides stage 4 into four sub-stages based on metastasis location, each carrying significantly different survival outcomes:
| Sub-Stage | Metastasis Location | 5-Year Survival (2026) |
|---|---|---|
| M1a | Distant skin, subcutaneous tissue, or distant lymph nodes | ~62% |
| M1b | Lungs only | ~53% |
| M1c | Other distant organs (liver, bone, GI tract, adrenal gland) | ~33% |
| M1d | Brain metastases (with or without other sites) | ~19–27% |
Source: SEER 2021 data; AJCC 8th Edition; CheckMate 067 long-term follow-up
Always ask your oncologist: “What is my exact M sub-stage — M1a, M1b, M1c, or M1d?” The difference in prognosis between M1a and M1d is significant, and your treatment protocol will differ accordingly.
Adapted from Wikimedia Commons, licensed under CC BY 4.0
How Is Stage 4 Melanoma Diagnosed?
Diagnosis requires a combination of imaging and molecular testing. Key workup components include:
- CT scan of chest, abdomen, and pelvis — identifies visceral metastases
- MRI of the brain — required in all new metastatic melanoma diagnoses
- PET-CT scan — full-body metabolic assessment
- Tissue biopsy of a metastatic site — confirms histology
- BRAF V600E/K mutation testing — determines targeted therapy eligibility (mandatory)
- PD-L1 expression testing — predicts immunotherapy response
- LDH (lactate dehydrogenase) blood test — elevated LDH correlates with higher tumor burden and poorer prognosis
For a complete review of all staging criteria and classifications, see our full melanoma stages guide.
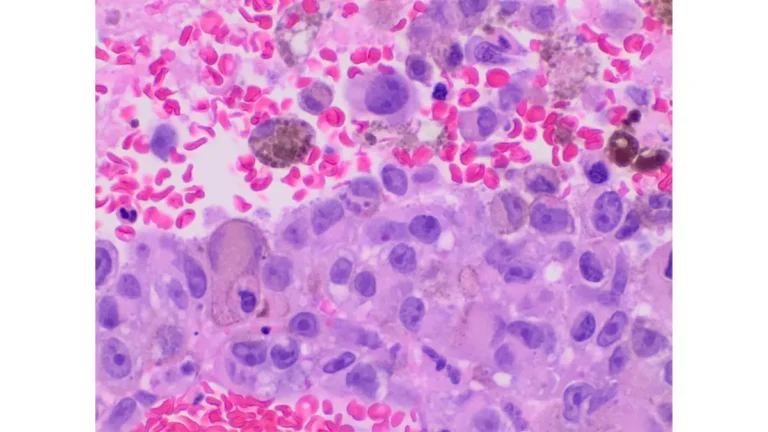
Stage 4 Melanoma Prognosis — The Real 2026 Numbers
A decade ago, a stage 4 melanoma diagnosis meant a median survival of just 8–9 months. That reality has fundamentally changed.
5-Year and 10-Year Survival Data (2026 Update)
According to the SEER database, the 5-year relative survival rate for distant-stage melanoma (diagnosed 2015–2021) is 34.6% as a population baseline. However, that number does not reflect current treatment protocols.
Updated 2026 clinical data tells a more encouraging story:
| Data Source | 5-Year Survival | Notes |
|---|---|---|
| SEER 2021 (population baseline) | 34.6% | Includes all treatments, all sub-stages |
| CheckMate 067 (nivo + ipi combo) | ~52% | Combination immunotherapy, 5-year follow-up |
| KEYNOTE-006 (pembrolizumab) | ~45% | Anti-PD-1 monotherapy |
| TIL therapy (lifileucel) responders | ~51% estimated | Post-checkpoint failure patients |
The 10-year data is where the real hope lies. Research published by Dana-Farber Cancer Institute in 2024 showed that approximately 50% of combination immunotherapy responders remained alive and cancer-free at 10 years — data no competitor currently presents to patients.
For a comprehensive breakdown of survival statistics at every stage, read our melanoma survival rate by stage guide.
Factors That Influence Your Individual Stage 4 Melanoma Prognosis
Your prognosis is not a fixed number. Key variables include:
- BRAF mutation status — positive mutation opens targeted therapy pathways with ~70% initial response rates
- LDH levels — elevated LDH at diagnosis correlates with shorter survival
- Number and location of metastases — oligometastatic disease (few sites) carries better outcomes
- ECOG performance status — patients with better functional status tolerate and respond to treatment more effectively
- Brain metastases — M1d patients benefit from specialized protocols combining SRS and immunotherapy
What This Means For You: Your prognosis is shaped by sub-stage, mutation profile, treatment center, and the therapies you receive — not by a population average from years ago.
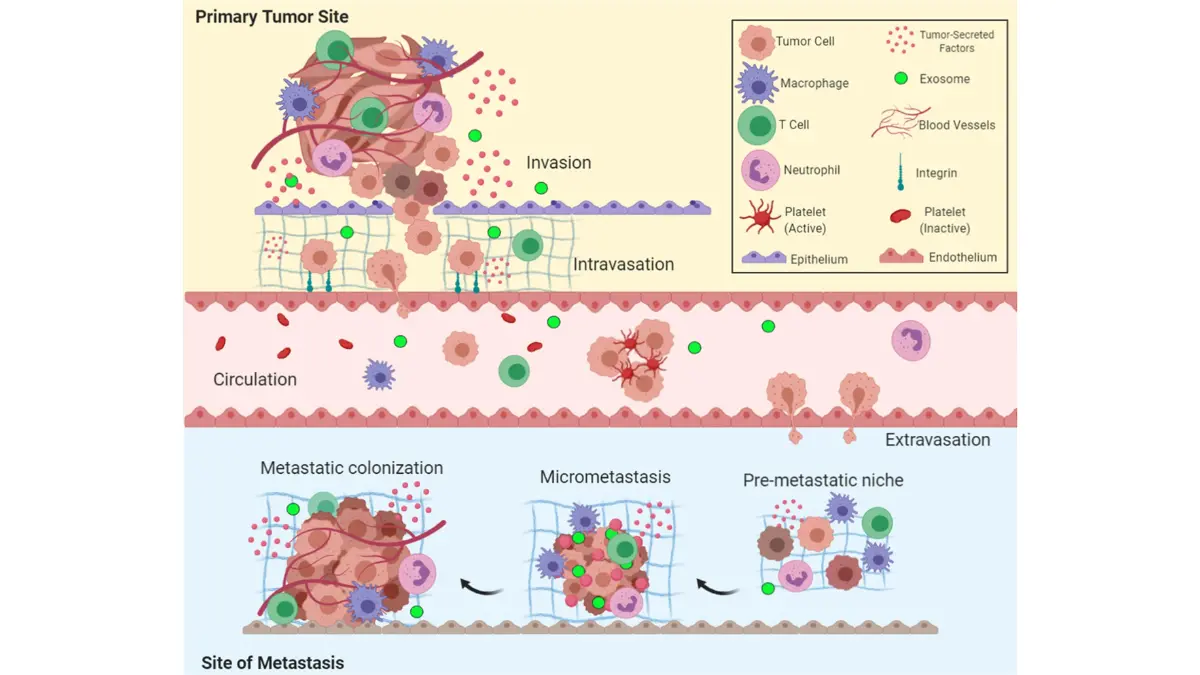
Adapted from Wikimedia Commons, licensed under CC BY-SA 4.0
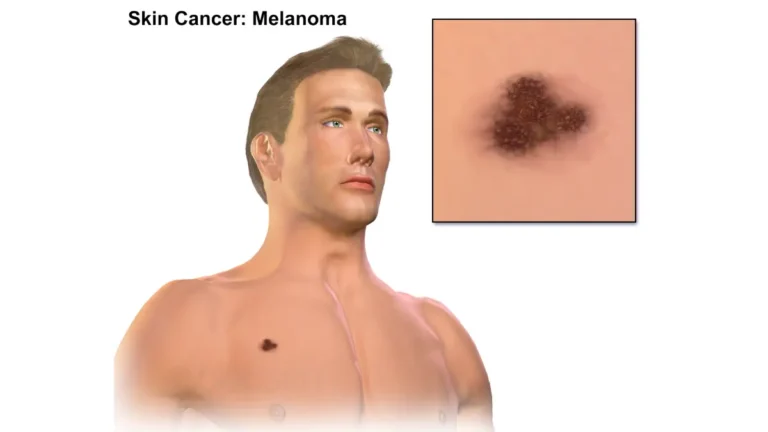
Stage 4 Melanoma Treatment Options in 2026 — The Complete Decision Tree
Treatment for stage 4 melanoma has shifted from chemotherapy to precision immunotherapy and targeted therapy. Here is the current treatment landscape, organized by clinical pathway.
First-Line Treatment: Immunotherapy Checkpoint Inhibitors
For most patients, combination immunotherapy is the international gold standard first-line treatment. The NCI’s melanoma treatment guidelines currently recommend:
- Nivolumab + Ipilimumab (Opdivo + Yervoy) — blocks PD-1 and CTLA-4 pathways simultaneously; ~58% objective response rate; confirmed as the best overall first-line option by the DREAMseq Phase III trial
- Pembrolizumab (Keytruda) — anti-PD-1 monotherapy; preferred for elderly patients or lower-burden disease; ~45% ORR
- Nivolumab + Relatlimab (Opdualag) — approved 2022; blocks LAG-3 protein; better tolerability profile than ipi+nivo
For a deep dive on how immune checkpoint therapy works at a cellular level, read our immunotherapy for melanoma guide.
Key side effects to monitor: immune-related colitis, hepatitis, pneumonitis, and endocrinopathies. Report any new symptoms to your oncologist immediately.
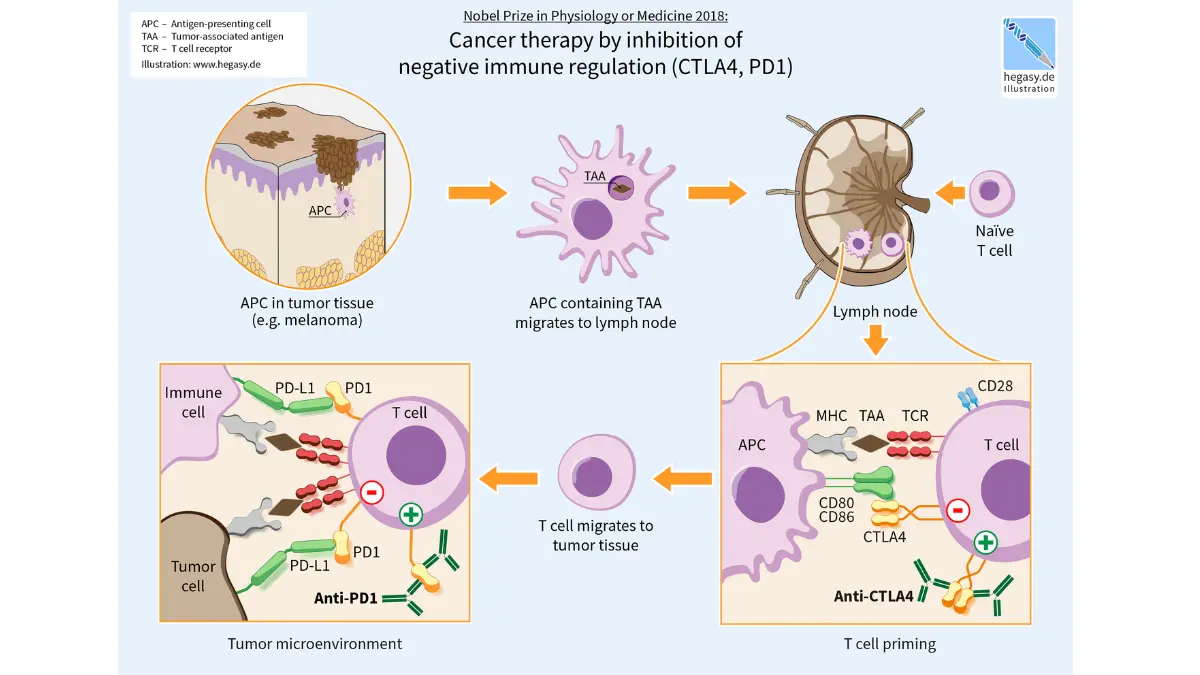
Adapted from Wikimedia Commons, licensed under CC BY-SA 4.0
BRAF-Mutated Stage 4 Melanoma: Targeted Therapy Options
Approximately 50% of melanoma patients carry a BRAF V600 mutation. For these patients, targeted BRAF + MEK inhibitor combinations produce high initial response rates. According to ASCO’s most recent educational guidance, the approved combinations include:
- Dabrafenib + Trametinib (Tafinlar + Mekinist) — ~70% initial ORR
- Encorafenib + Binimetinib (Braftovi + Mektovi) — comparable efficacy with favorable tolerability
Critical sequencing guidance from DREAMseq (Phase III): Starting ipi+nivo first, then switching to BRAF/MEK inhibitors on progression, produced a 20% absolute improvement in 2-year overall survival (72% vs. 52%) compared to the reverse sequence. For most BRAF+ patients, immunotherapy should come first.
For complete BRAF mutation treatment options, see our BRAF targeted therapy for melanoma article.
TIL Therapy (Lifileucel/Amtagvi) — The 2024 FDA Breakthrough
In February 2024, the FDA approved lifileucel (Amtagvi) as the first cell therapy to treat a solid tumor — a landmark moment for stage 4 melanoma patients who have progressed on checkpoint inhibitors.
How it works:
- Surgeons remove a small metastatic tumor
- Tumor-infiltrating lymphocytes (TIL cells) are extracted and multiplied by billions in a laboratory
- Patient receives lymphodepleting chemotherapy to prepare the immune system
- Expanded TIL cells are reinfused in a single treatment
Outcomes: ~31% overall response rate in treatment-refractory patients; some patients achieve complete remission. For the full TIL therapy patient story and clinical data, read our stage 4 melanoma survival and TIL therapy guide.
Memorial Sloan Kettering’s TIL therapy program has treated dozens of patients since approval, with outcomes consistent with trial data.
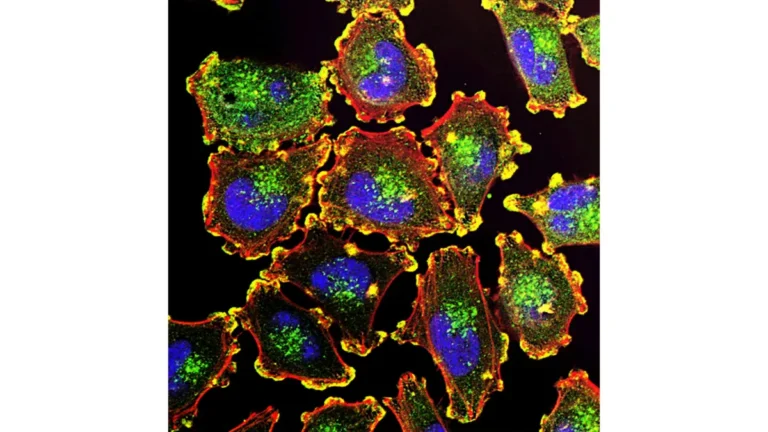
Brain Metastases (M1d): Specialized Treatment Protocol
Brain metastases represent the most challenging sub-stage. The current standard of care combines:
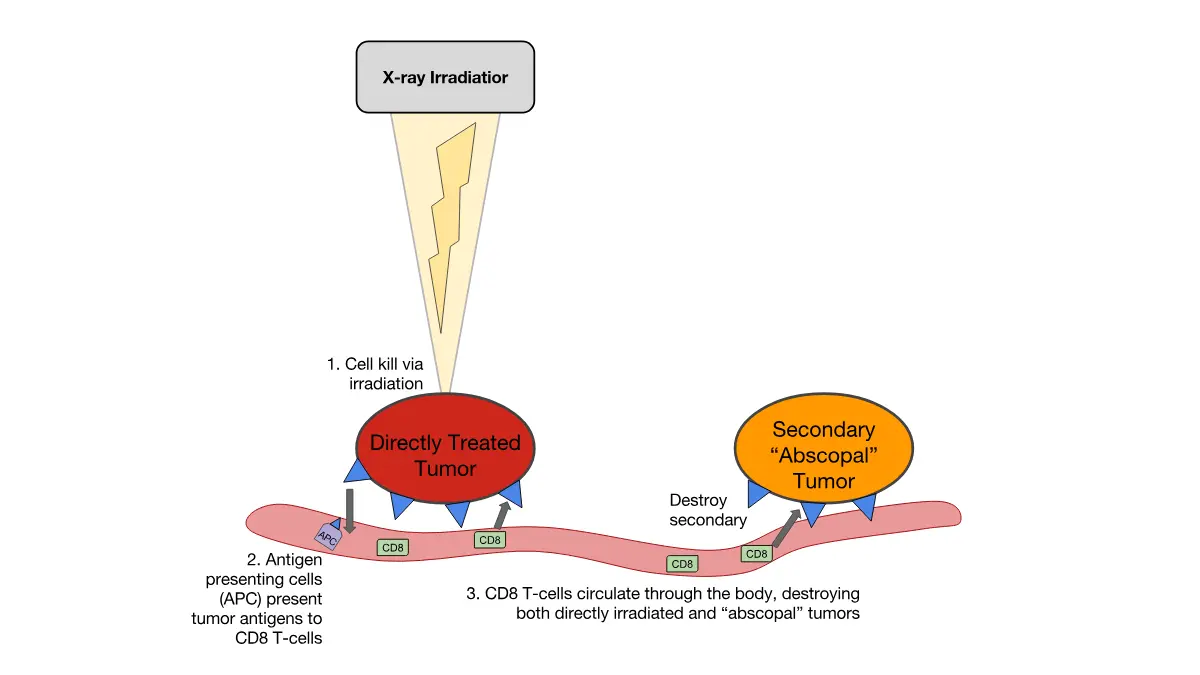
- Stereotactic Radiosurgery (SRS) — precision radiation to individual brain lesions
- Concurrent immunotherapy — nivo+ipi has shown improved intracranial response vs. either treatment alone
- Whole-brain radiation (WBRT) — now largely avoided due to neurocognitive side effects; reserved for leptomeningeal disease
Adapted from Wikimedia Commons, National Cancer Institute image — United States Government Work, Public Domain. No copyright restriction applies to this image.
Treatment Comparison at a Glance
| Treatment | Best Candidate | ORR | Key Side Effects |
|---|---|---|---|
| Nivo + Ipi | Most first-line patients | ~58% | Colitis, hepatitis, immune toxicity |
| Pembrolizumab | Low-burden/elderly | ~45% | Fatigue, rash, hypothyroidism |
| BRAF + MEK inhibitors | BRAF V600+ only | ~70% initial | Fever, skin rash, joint pain |
| TIL therapy (lifileucel) | Post-checkpoint failure | ~31% | Cytokine release, neutropenia |
| T-VEC injection | Accessible lesions only | ~26% | Local inflammation |
Clinical Trials & Emerging Therapies — What’s Coming in 2026–2028
For patients whose cancer has progressed on standard treatments, clinical trials are not a last resort — they are a legitimate first-line consideration. You can search active melanoma trials by sub-stage, mutation status, and location at ClinicalTrials.gov.
For a curated overview of all active studies, see our melanoma clinical trials 2026 guide.
mRNA Cancer Vaccine (mRNA-4157 + Pembrolizumab)
The most anticipated development in metastatic melanoma treatment is the personalized mRNA cancer vaccine. Phase IIb data from the KEYNOTE-942 trial showed mRNA-4157 combined with pembrolizumab reduced recurrence risk by approximately 44% compared to pembrolizumab alone in high-risk Stage III/IV patients after surgery.
The full Phase III trial (KEYNOTE-942/mRNA-4157-P201) is actively enrolling. Results are expected in 2027–2028. If confirmed, this could become a standard adjuvant option for stage 4 melanoma.
Other Emerging Approaches
- LAG-3 + PD-1 combinations beyond Opdualag — multiple Phase II trials ongoing
- Gut microbiome modulation — fecal microbiota transplants combined with checkpoint inhibitors are showing early signal in immunotherapy non-responders
- CAR-T cell therapy in solid tumors — exploratory but progressing toward Phase II
- Tumor-agnostic targeted therapies — for NRAS, c-KIT, and NF1-mutated melanomas without BRAF alteration
Action Step: Ask your oncologist at every appointment: “Am I eligible for any open clinical trials right now?” Every FDA-approved treatment today began in a trial someone else enrolled in.
Stage 4 Melanoma Patient Guide — Your First 30 Days
The first 30 days after a stage 4 diagnosis are the most critical for setting up optimal care. Most patients do not know what to request — or in what order. Here is your evidence-based action checklist.
Immediate Action Checklist (Days 1–30)
- Request molecular tumor profiling within Week 1 — BRAF V600E/K, NRAS, c-KIT, and PD-L1 expression testing. Use our Genetic Risk Assessment Tool to document your hereditary cancer risk factors before your first oncology appointment.
- Seek a second opinion at an NCI-Designated Cancer Center — these centers have dedicated melanoma tumor boards that review complex cases weekly. Find a center near you at cancer.gov.
- Ask specifically about clinical trial eligibility — use ClinicalTrials.gov filtered to your sub-stage and mutation status.
- Build your multidisciplinary team — medical oncologist, dermatologic oncologist, radiologist, and palliative care specialist from the start.
- Review financial assistance options immediately (see Section 6 below).
- Track your nutrition — patients with adequate protein intake tolerate immunotherapy better. Calculate your daily protein needs with our Protein Intake Calculator.
- Prioritize sleep quality — sleep disruption amplifies treatment-related fatigue and impairs immune function. Our Sleep Calculator can help you establish an optimal recovery schedule.
- Monitor body weight during treatment — unintentional weight loss during immunotherapy is a warning sign. Use our Weight Loss Calculator to track trends and share data with your care team.
7 Questions to Ask Your Oncologist at Your First Appointment
- What is my exact AJCC M sub-stage (M1a, M1b, M1c, or M1d)?
- Do I have a BRAF V600E or V600K mutation?
- What is my PD-L1 expression level?
- Should I begin with immunotherapy or BRAF-targeted therapy, and why?
- Am I eligible for any open clinical trials right now?
- What are the most likely Grade 3–4 side effects I should monitor for?
- What does my imaging surveillance schedule look like for the first two years?
Quality of Life, Nutrition & Mental Health During Treatment
Treatment for metastatic melanoma is intensive. Patients who actively manage nutrition, sleep, and mental health consistently report better treatment tolerance and quality-of-life scores.
- Nutrition: Maintain adequate calories and protein. Immunotherapy can suppress appetite — work with a registered dietitian.
- Mental health: Anxiety and depression affect 30–40% of metastatic cancer patients. The American Cancer Society’s cancer support groups and CancerCare counseling are both free resources.
- Exercise: Light to moderate physical activity (walking 20–30 minutes daily) is supported by evidence to improve fatigue and mood during immunotherapy.
Stage 4 Melanoma Treatment Costs & Financial Assistance in 2026
This section addresses what virtually no competitor covers — the real financial impact of stage 4 melanoma treatment. Drug costs without insurance are substantial, but assistance programs exist for most approved therapies.
2026 Drug Cost Reference Table
| Treatment | Annual Cost (Uninsured) | Patient Assistance Program |
|---|---|---|
| Pembrolizumab (Keytruda) | ~$190,000 | Merck Access Program |
| Nivolumab + Ipilimumab | ~$285,000 | BMS Patient Assistance Foundation |
| Dabrafenib + Trametinib | ~$160,000 | Novartis Patient Assistance Program |
| Lifileucel (Amtagvi) | ~$515,000 (one-time) | Iovance Biotherapeutics Support |
| TIL therapy (total program) | $150,000–$515,000 | Center-specific grants available |
Where to Get Financial Help
- CancerCare Financial Assistance — free counseling and co-pay grants for cancer patients
- NeedyMeds.org — tracks manufacturer patient assistance programs by drug name
- Clinical trials — drug costs are $0 to the patient in most Phase II and III trials
- Medicare/Medicaid — oncology drug coverage under Part B and Part D varies by treatment setting; ask your oncology billing coordinator about “medical necessity” documentation requirements
Frequently Asked Questions About Stage 4 Melanoma
1. What is stage 4 melanoma?
Stage 4 melanoma (metastatic melanoma) means cancer has spread to distant organs, skin, or lymph nodes beyond the primary site. It is classified into four sub-stages: M1a through M1d.
2. What is the stage 4 melanoma survival rate in 2026?
The 5-year survival rate ranges from 35% (population baseline) to 52% with combination immunotherapy. Some 10-year data now shows approximately 50% survival in checkpoint inhibitor responders.
3. Can stage 4 melanoma be cured?
Long-term remission — functionally equivalent to a cure — is achievable. Studies show 20–30% of stage 4 patients treated with checkpoint inhibitors remain disease-free beyond 10 years.
4. What is the best treatment for stage 4 melanoma in 2026?
For most patients, nivolumab + ipilimumab (combination immunotherapy) is the first-line gold standard. For BRAF V600-positive patients, BRAF + MEK inhibitors may be sequenced in after immunotherapy.
5. What is TIL therapy for melanoma?
TIL (tumor-infiltrating lymphocyte) therapy uses immune cells harvested from your own tumor, multiplied in a laboratory, and reinfused in a single treatment. Lifileucel (Amtagvi) received FDA approval in February 2024.
6. How long can you live with stage 4 melanoma?
Highly variable and improving. Some patients achieve decade-long remission. Prognosis depends on sub-stage, BRAF status, LDH levels, and treatment received.
7. Does a BRAF mutation affect stage 4 melanoma prognosis?
Yes. BRAF V600 mutation (present in ~50% of patients) unlocks access to targeted BRAF + MEK inhibitor therapies with ~70% initial response rates, meaningfully improving short-term outcomes.
8. What is the difference between M1a and M1d melanoma?
M1a involves distant skin or lymph nodes (~62% 5-year survival); M1d involves brain metastases (~19–27% 5-year survival). Sub-stage dramatically changes both prognosis and treatment approach.
9. What should I ask my oncologist first after a stage 4 melanoma diagnosis?
Start with three questions: What is my M sub-stage? Do I have a BRAF mutation? Am I eligible for clinical trials? The answers determine your entire treatment pathway.
10. Are clinical trials worth considering for stage 4 melanoma?
Yes — especially for patients who have progressed on standard therapy. Trials provide access to cutting-edge drugs at no cost and have produced every major breakthrough in melanoma over the past decade.
11. What financial assistance exists for stage 4 melanoma treatment?
Merck, BMS, Novartis, and Iovance all offer patient assistance programs. CancerCare provides free co-pay grants and counseling. Patients enrolled in clinical trials pay $0 for the trial drug.
Related Reading on MyMedicineAdvisor.com:
- Melanoma Survival Rate by Stage: 2026 Complete Data →
- Immunotherapy for Melanoma: How It Works →
- BRAF Targeted Therapy for Melanoma →
- Melanoma Clinical Trials 2026 →
📌 This article is for educational purposes only and does not constitute medical advice. Treatment decisions for stage 4 melanoma must be made in consultation with a board-certified oncologist. Information is current as of April 2026 and reflects FDA approvals, NCCN guidelines, and clinical trial data available at the time of publication.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.