On This Page – Quick Medical Summary
Immunotherapy for melanoma works by removing the “brakes” cancer places on your immune system, allowing T cells to recognize and destroy tumor cells. As of 2026, five FDA-approved immunotherapy agents are available, with eligibility based on stage, mutation status, and overall health. Median survival for advanced melanoma has risen from 6 months (pre-2011) to nearly 6 years today.
⚠️ Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a board-certified oncologist before making any treatment decisions.
What Is Immunotherapy for Melanoma — And Why It Changed Everything
In 2019, Marcus D., a 54-year-old contractor from Phoenix, was diagnosed with Stage IV melanoma. His oncologist told him that just a decade earlier, his median survival would have been measured in months. After 18 months of pembrolizumab (Keytruda) infusions, his scans showed no evidence of disease (NED). His story is no longer rare.
Immunotherapy has fundamentally transformed melanoma outcomes. Before 2011, the standard of care — chemotherapy — produced a median overall survival of 6 to 9 months for metastatic melanoma. Today, landmark trials show median survival approaching 6 years for patients on combination immunotherapy, according to long-term follow-up data published in PMC/NCBI.
How It Differs from Chemotherapy and Targeted Therapy
Many patients ask: “Is immunotherapy the same as chemo?” No — and the difference matters enormously.
| Treatment Type | How It Works | Durability | Key Side Effects |
|---|---|---|---|
| Chemotherapy | Kills fast-growing cells (including healthy ones) | Short-term | Hair loss, nausea, low blood counts |
| Targeted Therapy | Blocks specific proteins (e.g., BRAF) | Can lose effectiveness over time | Skin rash, fever, joint pain |
| Immunotherapy | Trains YOUR immune system to find and kill cancer | Long-lasting “immunological memory” | Immune-related inflammation |
Key Takeaway: Immunotherapy works with your body’s natural defenses — it doesn’t replace them. This is why some patients achieve durable, long-lasting remissions that persist even after stopping treatment.
For a broader look at all available treatment paths, see our complete guide on melanoma treatment options and the full overview in our melanoma symptoms, stages & treatment pillar.
How Immunotherapy Actually Works Against Melanoma Cells
Understanding the biology makes the treatment decisions less overwhelming. Here’s the plain-language breakdown.
The Checkpoint Problem: How Cancer “Hides”
Your immune system has built-in brakes — called checkpoints — that prevent it from attacking your own healthy cells. Proteins like PD-1, CTLA-4, and LAG-3 act as these brakes.
Melanoma cells are clever. They hijack these checkpoint proteins to disguise themselves as “self” — essentially flipping the off switch on your T cells so they don’t attack the tumor.
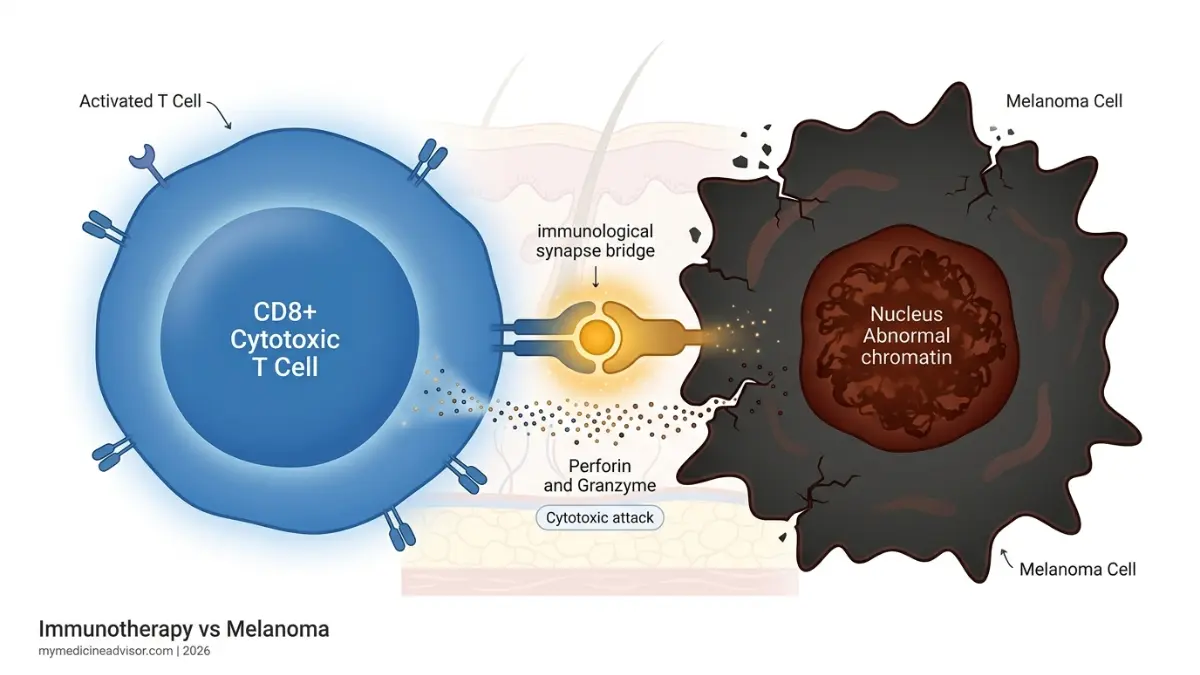
How Checkpoint Inhibitors “Release the Brakes”
Checkpoint inhibitor drugs work by blocking the off switch — unmasking the tumor so your immune cells can finally recognize and destroy it.
Think of it this way: Your T cells are trained attack dogs on a leash. Melanoma cells cut the leash release mechanism. Checkpoint inhibitors restore the release — unleashing your immune cells on the tumor.
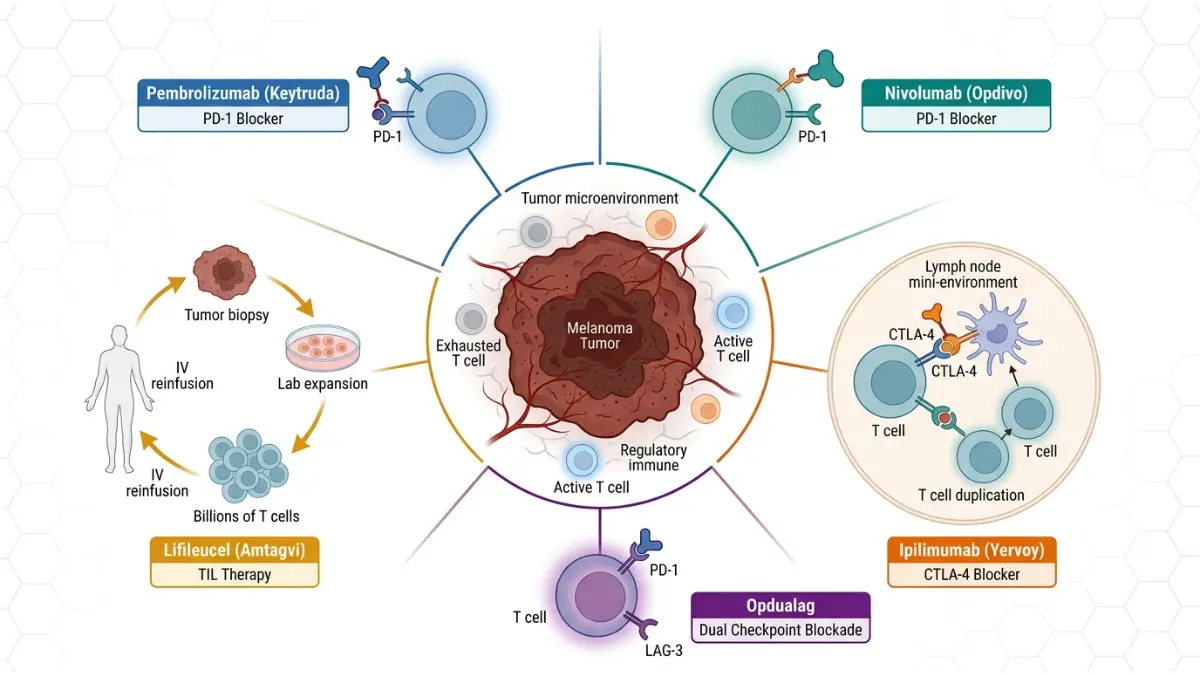
The 3 Key Immunotherapy Pathways in Melanoma
| Pathway Blocked | What It Does | Drugs That Target It |
|---|---|---|
| PD-1 | Prevents T cells from being “turned off” by tumor | Pembrolizumab (Keytruda), Nivolumab (Opdivo) |
| CTLA-4 | Amplifies T cell activation and proliferation | Ipilimumab (Yervoy) |
| LAG-3 | Overcomes a secondary immune resistance mechanism | Relatlimab (in Opdualag) |

Beyond Checkpoints: TIL Therapy (2024 FDA Approval)
In 2024, the FDA approved lifileucel (Amtagvi) — the first tumor-infiltrating lymphocyte (TIL) therapy for metastatic melanoma. Unlike checkpoint inhibitors, TIL therapy:
- Removes your own T cells that have already infiltrated the tumor
- Expands them into billions of cancer-fighting cells in a lab
- Reinfuses them back into your body as a supercharged immune force
This is a critical advancement, especially for patients whose cancer has stopped responding to checkpoint inhibitors, as covered in detail by Washington University Medicine’s coverage of this approval.
You can assess your personal cancer-related genetic risk factors using our Genetic Risk Assessment Tool.
All FDA-Approved Immunotherapy Drugs for Melanoma (2026 Master Guide)
The National Cancer Institute’s melanoma treatment PDQ lists five major immunotherapy agents currently approved for melanoma.
2026 FDA-Approved Melanoma Immunotherapy: Complete Comparison Table
| Drug (Brand) | Type | Pathway | Stages Approved | Administration | Approx. Response Rate |
|---|---|---|---|---|---|
| Pembrolizumab (Keytruda) | PD-1 inhibitor | PD-1 | Stage IIB–IV | IV infusion, every 3–6 wks | ~33–40% |
| Nivolumab (Opdivo) | PD-1 inhibitor | PD-1 | Stage III–IV | IV infusion, every 2–4 wks | ~32–40% |
| Ipilimumab (Yervoy) | CTLA-4 inhibitor | CTLA-4 | Stage III–IV | IV infusion, every 3 wks × 4 doses | ~10–15% (mono) |
| Nivolumab + Ipilimumab (Opdualag alternative) | Combo | PD-1 + CTLA-4 | Stage III–IV | IV infusion | ~57% (combo) |
| Relatlimab + Nivolumab (Opdualag) | LAG-3 + PD-1 combo | LAG-3 + PD-1 | Unresectable/metastatic | IV infusion | ~43% |
| Lifileucel (Amtagvi) | TIL therapy | Cellular | Post-checkpoint failure | One-time IV infusion | ~31% (heavily pretreated) |
Important: The combination of nivolumab + ipilimumab shows the highest 5-year survival rates (~52%), but also the highest rate of serious side effects. Your oncologist will weigh this tradeoff individually.
BRAF Testing: Why It Comes First
Before choosing between immunotherapy and targeted therapy, your oncologist will test your tumor for a BRAF V600 mutation. Approximately 50% of melanomas carry this mutation.
- BRAF-positive: You may have the option of BRAF/MEK inhibitors (dabrafenib + trametinib) or immunotherapy — or both in sequence
- BRAF-negative: Immunotherapy is typically the first-line treatment
Understanding your diagnosis starts with knowing your stage — review our guide to melanoma stages and learn how melanoma is diagnosed for full context.
You can cross-reference your medications using our free Pill Identifier tool to verify names and dosages.
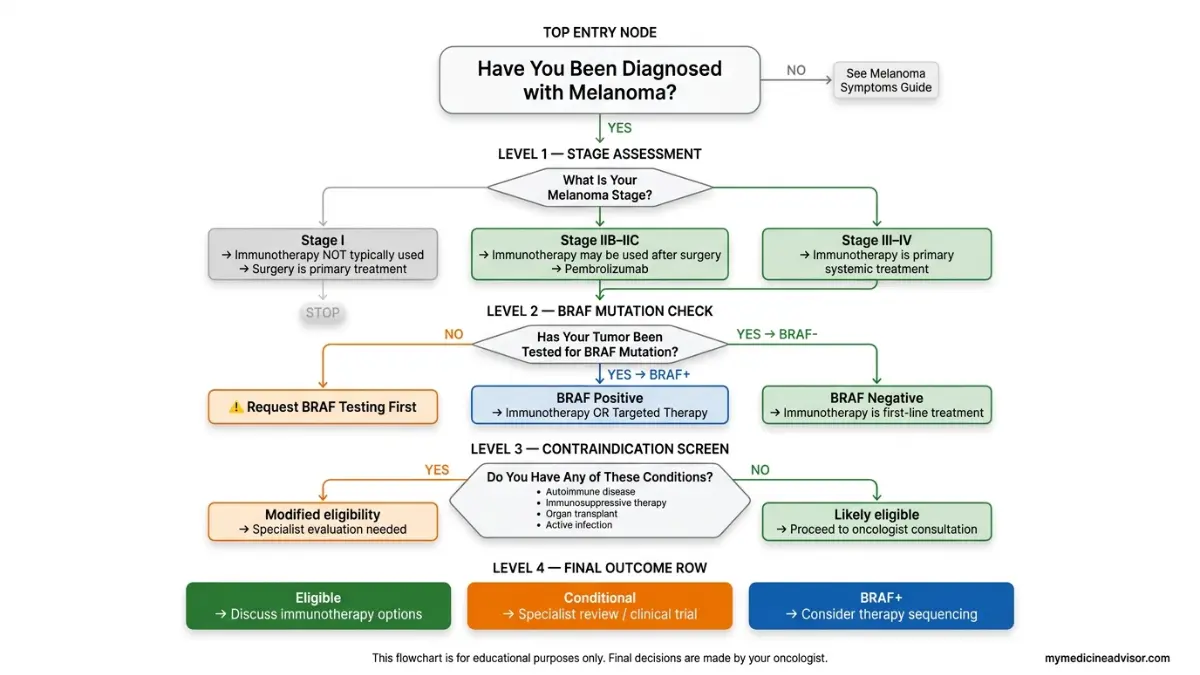
Who Is Eligible for Melanoma Immunotherapy?
This is the most critical question patients ask — and the most poorly answered by competitors. Here is the definitive eligibility breakdown for 2026.
Stage-by-Stage Eligibility Overview
| Stage | Immunotherapy Used? | Common Drug |
|---|---|---|
| Stage I | Not typically | — |
| Stage IIB–IIC | Yes — adjuvant (post-surgery) | Pembrolizumab |
| Stage III (resectable) | Yes — adjuvant | Pembrolizumab or Nivolumab |
| Stage III (unresectable) | Yes — systemic | Combo or mono |
| Stage IV (metastatic) | Yes — first-line | Combo or mono |
| Post-checkpoint failure | TIL therapy option | Lifileucel (Amtagvi) |
✅ The 8-Point Eligibility Self-Assessment Checklist
Bring this list to your next oncology appointment:
- ☐ Is my melanoma Stage IIB or higher?
- ☐ Have I had a BRAF mutation test on my tumor?
- ☐ Do I have any active autoimmune diseases (lupus, IBD, MS, rheumatoid arthritis)?
- ☐ Am I currently on immunosuppressive medications (prednisone, biologics)?
- ☐ Do I have adequate kidney, liver, and lung function (blood tests will confirm)?
- ☐ Is my performance status ECOG 0–1 (able to carry out normal activity)?
- ☐ Do I have untreated brain metastases? (May require radiation first)
- ☐ Have I had a prior organ transplant? (Significantly changes eligibility)
If you checked “yes” to items 3, 4, 7, or 8 — you may still qualify with modifications, but these require specialist evaluation. Ask about clinical trials as an alternative pathway.
Who May NOT Qualify (and Why)
Patients with the following conditions require extra caution before starting checkpoint inhibitors:
- Active autoimmune disease: Risk of triggering severe immune flares
- Solid organ transplant recipients: Immunotherapy can trigger organ rejection
- Active systemic infections: Including uncontrolled HIV
- Severe organ impairment: Poor liver or kidney function limits drug clearance
The Emerging ctDNA Blood Test (2026 Frontier)
One competitor gap none of the top-ranking sites addresses: circulating tumor DNA (ctDNA) testing is emerging as a powerful tool to determine which Stage III patients actually need adjuvant immunotherapy after surgery.
A ctDNA-negative result after surgery may indicate low recurrence risk — allowing some patients to avoid immunotherapy side effects entirely. Ask your oncologist if this test is available at your center.
For deeper insight into your personal risk profile, explore our melanoma blood tests and biomarkers guide and our full stage 4 melanoma survival and therapy breakdown.
Success Rates, Side Effects & What to Expect During Treatment
2026 Survival Data: What the Numbers Actually Mean
According to long-term immunotherapy trial data from PMC/NCBI, here is where survival outcomes stand in 2026:
| Treatment | 5-Year Overall Survival |
|---|---|
| Pembrolizumab (mono) | ~44–48% |
| Nivolumab (mono) | ~44% |
| Ipilimumab + Nivolumab (combo) | ~52% |
| Relatlimab + Nivolumab | Ongoing data (promising) |
| Lifileucel (post-checkpoint) | ~31% response rate (heavily pretreated) |
What This Means For You: Before 2011, a Stage IV melanoma diagnosis carried a median survival of 6–9 months. These numbers represent a generational transformation in outcomes. However, responses vary — approximately 40–50% of patients do not respond to first-line immunotherapy, which is why ongoing research and clinical trials remain critical.
For stage-specific survival data, see our comprehensive melanoma survival rate by stage guide.

Immune-Related Side Effects: 3-Tier Severity Guide
Because immunotherapy activates your entire immune system, it can cause inflammation in any organ. Here’s what to watch for:
Tier 1 — Minor (Manage at home, report at next visit):
- Fatigue, mild rash, itching
- Mild diarrhea (fewer than 4 extra stools/day)
- Low-grade fever
Tier 2 — Moderate (Call your oncology team within 24 hours):
- Colitis (abdominal cramping, bloody stool)
- Hepatitis (jaundice, dark urine, right-sided pain)
- Pneumonitis (new shortness of breath, dry cough)
- Thyroid dysfunction (unexpected fatigue, weight changes)
Tier 3 — Serious (Go to the Emergency Room immediately):
- Myocarditis (chest pain, racing heartbeat, shortness of breath)
- Severe pneumonitis (oxygen dependence)
- Neurological symptoms (confusion, weakness, vision changes)
- Adrenal crisis (extreme weakness, dizziness, low blood pressure)
Bold Rule: Most side effects are reversible with prompt corticosteroid treatment. The key is early reporting — don’t wait for your next scheduled appointment if something feels wrong.
The American Cancer Society’s immunotherapy side effect resource provides additional guidance on managing specific reactions.
Your First Infusion: A Step-by-Step Walkthrough
Patients consistently say knowing what to expect reduces anxiety dramatically. Here’s what actually happens:
- Pre-infusion bloodwork — Liver, kidney, thyroid, and CBC panels (30 min)
- Medical review — Nurse or physician reviews labs and symptoms before each dose
- IV placement — Standard IV line in arm, no port required for most patients
- Infusion duration — Pembrolizumab: 30 minutes | Nivolumab: 30–60 minutes | Combo: 30–60 minutes
- Observation period — 30–60 minutes post-infusion for any acute reactions
- Discharge — Most patients drive themselves home; fatigue may peak 24–72 hours later
What to bring: Insurance card, list of all current medications, a book or headphones — you’ll be seated comfortably in a recliner chair. You do not need to fast beforehand.
To support your overall health during treatment, track your daily hydration with our Water Intake Calculator, monitor cardiac wellness using our Heart Rate Zone Calculator, and manage fatigue by optimizing your rest with our Sleep Calculator.
Your Next Steps — Questions, Costs & Clinical Trials
10 Questions to Ask Your Oncologist Before Starting Immunotherapy
Print this list and bring it to your next appointment:
- What stage is my melanoma, and which immunotherapy approach applies to my case?
- Has my tumor been tested for BRAF mutations?
- Should I receive monotherapy or combination therapy — what are the tradeoffs for me personally?
- What side effects should I watch for in the first 48–72 hours after my first infusion?
- How will we measure whether the immunotherapy is working?
- Are there clinical trials I qualify for that might give me access to newer agents?
- What happens if my cancer doesn’t respond or progresses despite immunotherapy?
- Will immunotherapy interact with my existing health conditions or medications?
- What financial assistance programs are available for Keytruda, Opdivo, or Yervoy?
- Can I continue working, exercising, and traveling during treatment?
How Much Does Melanoma Immunotherapy Cost?
| Drug | Annual List Price (US) | Insurance Coverage | Patient Assistance |
|---|---|---|---|
| Pembrolizumab (Keytruda) | ~$150,000–$190,000/yr | Covered (Medicare, most private plans) | Merck Access Program |
| Nivolumab (Opdivo) | ~$150,000–$180,000/yr | Covered | Bristol Myers Squibb program |
| Ipilimumab (Yervoy) | ~$150,000/yr | Covered | Bristol Myers Squibb program |
| Lifileucel (Amtagvi) | ~$515,000 (one-time) | Accelerated coverage expanding | Iovance patient support |
Key Point: Most major insurance plans — including Medicare and Medicaid — cover FDA-approved melanoma immunotherapy. Out-of-pocket costs vary significantly based on your plan. Always ask your oncology billing team about copay assistance programs before assuming it’s unaffordable.
Also explore the sentinel lymph node biopsy guide to understand staging procedures that precede treatment decisions, and use our Symptom Checker to monitor any new or changing symptoms between appointments.
Clinical Trials: Access Treatments Before FDA Approval
As of April 2026, ClinicalTrials.gov lists 400+ active melanoma immunotherapy trials across the United States. These trials may offer:
- Access to next-generation LAG-3, TIM-3, and TIGIT inhibitors
- Novel combinations not yet commercially available
- Free treatment at qualifying centers
Ask your oncologist: “Is there an open trial I qualify for at this center or a nearby NCI-designated cancer center?”
The Cancer Research Institute’s melanoma immunotherapy clinical trial database also offers a patient-facing trial matching tool.
For context on how immunotherapy compares across cancer types, visit our broader guide on how immunotherapy works.
Frequently Asked Questions (FAQs)
1. What is the success rate of immunotherapy for melanoma?
The 5-year overall survival rate for combination checkpoint immunotherapy (nivolumab + ipilimumab) is approximately 52% for Stage IV melanoma — compared to less than 5% before 2011. Monotherapy with pembrolizumab or nivolumab yields 5-year survival rates of 44–48%.
2. Who qualifies for immunotherapy for melanoma?
Patients with Stage IIB through Stage IV melanoma are generally eligible. Eligibility depends on tumor stage, BRAF mutation status, organ function, and absence of contraindications like active autoimmune disease or organ transplant history.
3. What is the best immunotherapy drug for melanoma in 2026?
There is no single “best” drug — the choice depends on your stage, health, and risk tolerance. The combination of nivolumab + ipilimumab offers the highest survival benefit but also the highest side effect burden. Pembrolizumab is the most widely prescribed due to its favorable efficacy-to-side-effect profile.
4. How long does melanoma immunotherapy treatment last?
Most protocols run for up to 2 years, or until cancer progression or intolerable side effects. Many patients who achieve remission are observed off treatment, and some maintain durable responses years after stopping.
5. Can Stage 4 melanoma be cured with immunotherapy?
“Cure” is not the standard clinical language, but durable complete responses (no detectable cancer for 5+ years) are documented in approximately 15–20% of Stage IV patients on combination therapy. These are cases that would previously have been considered terminal.
6. What are the most common side effects of melanoma immunotherapy?
The most common include fatigue (30–50%), skin rash (30–40%), diarrhea/colitis (10–30%), and thyroid dysfunction (10–20%). Most are manageable with prompt medical attention.
7. Is pembrolizumab (Keytruda) approved for melanoma?
Yes. Pembrolizumab is FDA-approved for Stage IIB through Stage IV melanoma — including as adjuvant therapy after surgery and as first-line treatment for unresectable or metastatic disease.
8. Can you have immunotherapy if you have an autoimmune disease?
It depends on severity and type. Patients with mild, well-controlled autoimmune conditions may still qualify with close monitoring. Those with severe, active conditions (e.g., active lupus nephritis, active IBD flares) typically do not qualify due to risk of life-threatening immune flares.
9. What is TIL therapy and how is it different from checkpoint inhibitors?
TIL (tumor-infiltrating lymphocyte) therapy uses your own T cells that have already found the tumor — they are extracted, multiplied in a lab into billions of cells, then reinfused. Checkpoint inhibitors, by contrast, are drugs given IV that remove brakes on all T cells broadly. TIL therapy is more personalized and approved specifically for patients who have failed prior checkpoint treatment.
10. Does insurance cover melanoma immunotherapy?
Yes — FDA-approved melanoma immunotherapy drugs are covered by Medicare, Medicaid, and most major private insurers. Coverage requirements vary; your oncology team’s billing department can navigate prior authorizations and patient assistance programs.
11. How do I find a melanoma immunotherapy clinical trial near me?
Visit ClinicalTrials.gov and enter your location and melanoma stage. You can also ask your oncologist for referrals to NCI-designated cancer centers, which run the largest volume of trials.
Summary: Key Takeaways
- Immunotherapy has transformed Stage IV melanoma from a near-certain death sentence into a potentially manageable — and sometimes curable — disease.
- Five FDA-approved agents are available in 2026, ranging from PD-1 inhibitors to the newest TIL therapy (lifileucel).
- Eligibility depends on stage (IIB+), BRAF mutation status, organ function, and absence of severe autoimmune conditions.
- Side effects are serious but manageable — early reporting is the single most important thing a patient can do.
- Clinical trials remain the frontier — always ask if you qualify.
Related Reading:
Sources: NCI Cancer Treatment PDQ, PMC/NCBI Immunotherapy Review, American Cancer Society, Memorial Sloan Kettering Cancer Center, ClinicalTrials.gov, FDA Drug Approvals Database.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.