On This Page – Quick Medical Summary
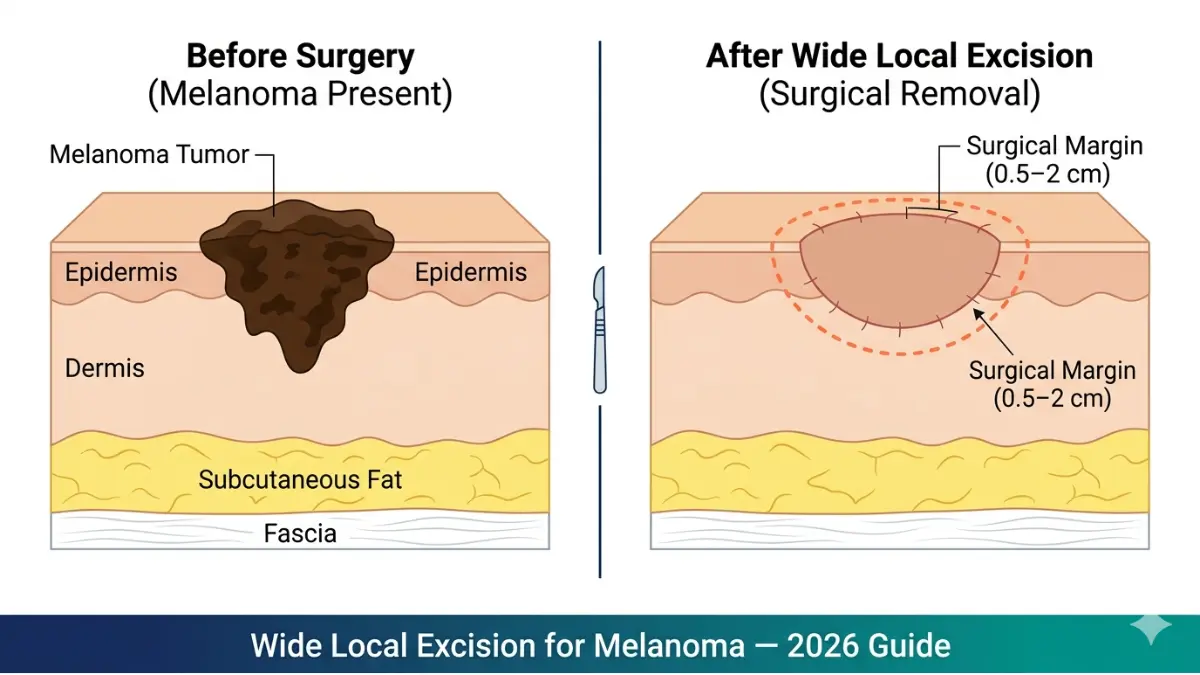
Wide local excision (WLE) for melanoma is a surgical procedure that removes the cancerous lesion plus a carefully measured margin of healthy surrounding skin — typically 0.5 cm to 2 cm — based on tumor thickness. It is performed as an outpatient procedure under local anesthesia and remains the gold-standard curative treatment for localized melanoma per NCCN Guidelines v1.2026.
Marcus, a 47-year-old firefighter from Texas, received his melanoma diagnosis after a routine skin check. “The moment my surgeon explained exactly what wide local excision meant — the margin size, the scar, the recovery — I stopped panicking and started planning,” he recalls. His experience reflects that of over 100,000 Americans diagnosed with melanoma each year who face this same decision.
⚠️ This article is for educational purposes only and does not constitute medical advice. Always consult a qualified dermatologist or surgical oncologist regarding diagnosis and treatment options.
What Is Wide Local Excision for Melanoma?
Wide local excision is the most common surgical procedure used to treat melanoma. During WLE, your surgeon removes the entire melanoma tumor along with a pre-measured margin of healthy-looking skin around its edges.
Why WLE — not just the original biopsy removal?
An excision biopsy removes only the visible lesion for diagnosis. Because melanoma cells can extend microscopically beyond visible borders, WLE removes an additional margin of tissue to eliminate residual cancer cells and reduce the risk of local recurrence.
| Procedure | Purpose | Tissue Removed |
|---|---|---|
| Excision Biopsy | Diagnosis | Lesion only (1–3 mm margin) |
| Wide Local Excision | Curative removal | Lesion + 0.5–2 cm margin |
WLE is indicated for melanoma stages 0 through II, and sometimes as part of a combined approach for stage III disease alongside systemic therapies. A sentinel lymph node biopsy is often performed simultaneously with WLE — particularly when the melanoma is thicker than 0.8 mm — to check whether cancer cells have reached the lymphatic system.
If you have a family history of melanoma, understanding your inherited risk before or alongside treatment is valuable. Use our Genetic Risk Assessment Tool to evaluate your personal hereditary risk profile.
✅ What This Means For You: If your oncologist recommended WLE, it typically signals the melanoma is still localized — one of the strongest prognostic indicators for a favorable outcome.
Surgical Margins Explained — The Breslow Thickness Guide
The most common question patients ask before surgery: “How much skin will actually be removed?”
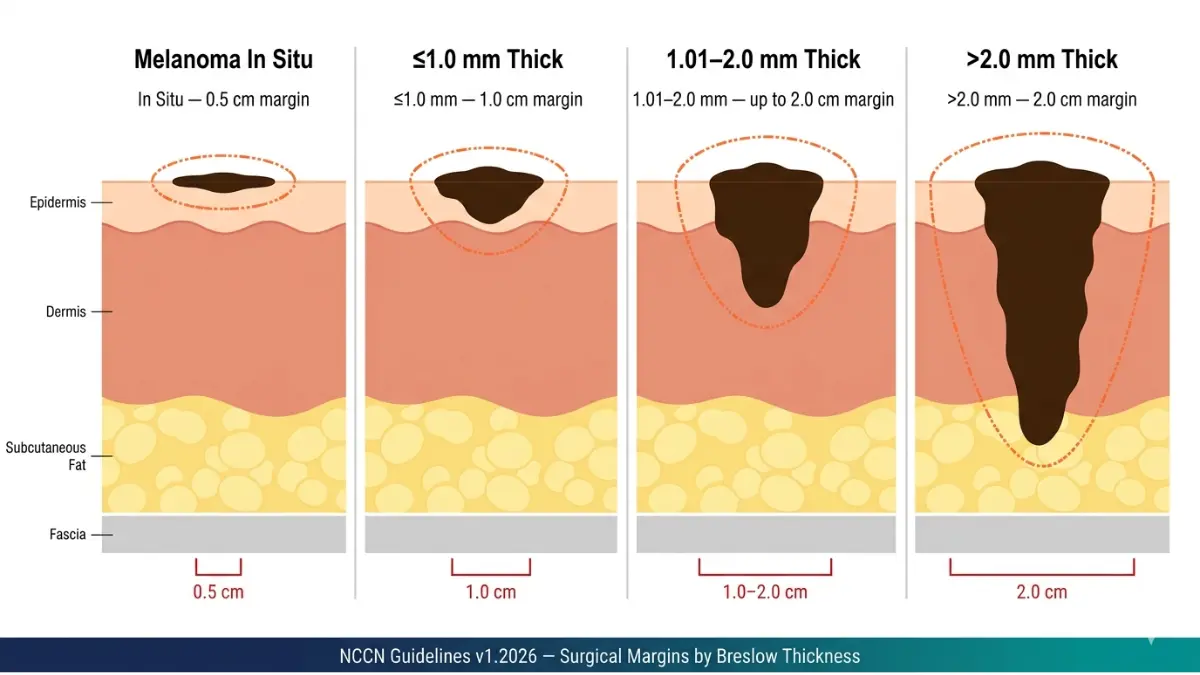
The answer depends on your melanoma’s Breslow thickness — the measurement in millimeters of how deeply the tumor has grown into the skin. According to NCCN Guidelines v1.2026 and the American Academy of Dermatology, the following margin recommendations apply:
| Breslow Thickness | Recommended Margin | Evidence Level |
|---|---|---|
| Melanoma in situ (Stage 0) | 0.5 – 1.0 cm | Grade A |
| ≤ 1.0 mm (Stage I) | 1.0 cm | Grade A |
| 1.01 – 2.0 mm (Stage I–II) | 1.0 – 2.0 cm | Grade A |
| > 2.0 mm (Stage II) | 2.0 cm | Grade A |
Why does margin size matter so much?
A 2024 study published in PMC/NCBI analyzing decades of clinical trials confirmed that margins exceeding 2 cm offer no additional survival benefit, while margins smaller than recommended significantly increase local recurrence risk.
Body-location nuances you must know:
- Face, hands, ears: Margins may be reduced to preserve function and cosmetic appearance
- Trunk and limbs: Standard NCCN margins are achievable without major functional impact
- Head and neck: A multidisciplinary review is essential — margins < 1 cm at these sites remain controversial per current NCBI clinical guidelines
WLE vs. Mohs Micrographic Surgery — Which Is Used for Melanoma?
| Wide Local Excision | Mohs Surgery | |
|---|---|---|
| Best for | All invasive melanomas | Melanoma in situ only |
| Margin control | Pre-determined fixed margin | Layer-by-layer real-time |
| Same-day pathology | No | Yes |
| NCCN recommendation | ✅ Gold standard | Selective use only |
Mohs surgery is reserved for melanoma in situ at cosmetically sensitive sites like the nose or eyelid, not for invasive melanomas. To fully understand your melanoma stages and how staging drives margin decisions, review your pathology report with your oncologist.
✅ What This Means For You: A 1–2 cm margin sounds alarming, but on your skin that’s roughly the size of a dime. That small additional tissue removal is what dramatically reduces your chance of the cancer returning.
Step-by-Step Wide Local Excision Procedure
Before Surgery — How to Prepare
Preparation for wide local excision is typically straightforward for most patients.
Key pre-op steps:
- Stop blood thinners (aspirin, warfarin, NSAIDs) 5–7 days before surgery as directed by your surgeon
- Fast for 6 hours if general anesthesia is planned (most WLE under local anesthesia requires no fasting)
- Wear loose, comfortable clothing over the surgical site
- Arrange transportation — even after local anesthesia, driving is not recommended for 24 hours
- Plan for 1–3 days of light activity post-procedure
10 Questions to Ask Your Surgeon Before WLE:
- What is my exact margin recommendation based on my Breslow thickness?
- Will a sentinel lymph node biopsy be performed at the same time?
- How will my wound be closed — primary sutures, skin flap, or graft?
- How long will the pathology results take?
- What does a “positive margin” finding mean for my next steps?
- What anesthesia will you use — local or general?
- What is my expected scar size and location?
- When can I return to work, exercise, and swimming?
- What infection warning signs should I watch for?
- Will I need adjuvant immunotherapy after surgery?
During Surgery — What Happens Step-by-Step
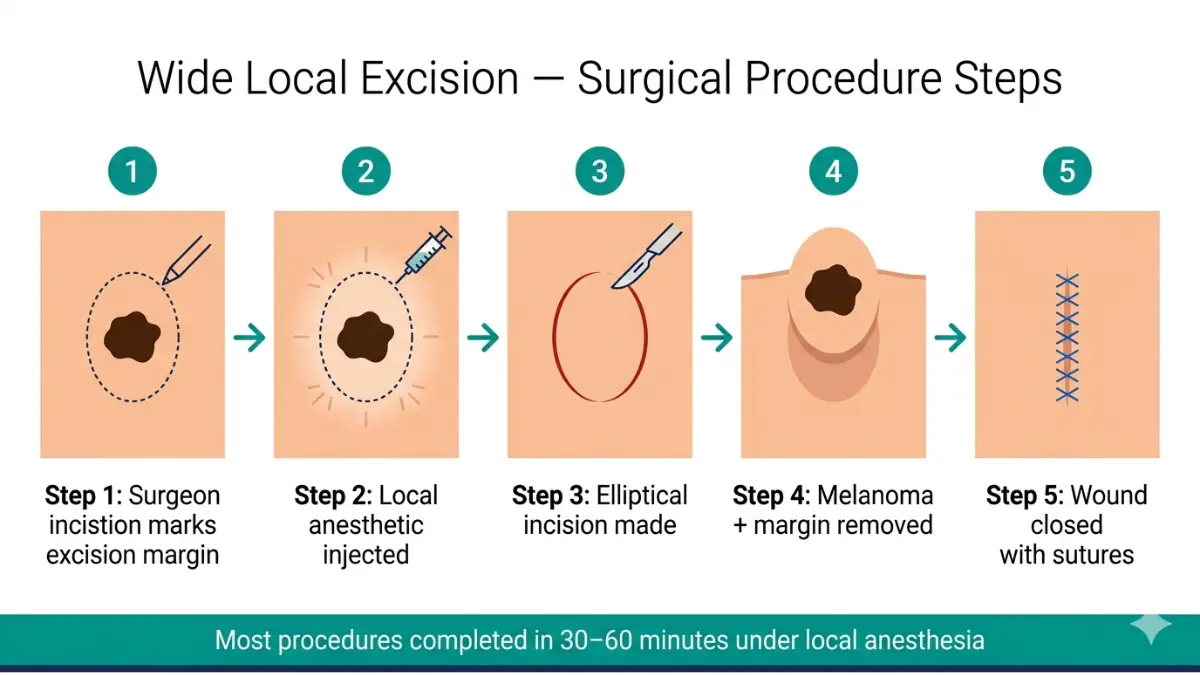
Most wide local excision procedures take 30–60 minutes and are performed as outpatient procedures. Here is exactly what happens:
- Margin marking: Your surgeon marks the planned excision boundary on your skin
- Local anesthetic injection: The area is numbed with lidocaine — you remain fully awake
- Elliptical incision: An ellipse-shaped cut is made around the marked margin
- Tissue removal: The melanoma and surrounding margin tissue are removed down to fascia
- Wound closure: The surgeon closes the wound with sutures, or uses a skin flap or graft if needed
- Pathology submission: The removed tissue is sent to a laboratory for microscopic examination
Skin Grafts and Skin Flaps — When Are They Needed?
Most patients don’t require a skin graft. Primary closure with sutures is sufficient for the majority of WLE procedures.
A graft is needed when:
- The excision area is too large for direct closure
- The site is on the face, scalp, lower leg, or foot
- A skin flap from nearby tissue cannot provide adequate coverage
The American Society of Plastic Surgeons provides detailed guidance on reconstruction options following melanoma surgery for cases requiring more complex wound management.
If you experience unusual symptoms after surgery — unexpected swelling, discharge, or pain — use our Symptom Checker for initial guidance before calling your care team.
Wide Local Excision Recovery — Week-by-Week Timeline
Recovery from wide local excision melanoma surgery is usually straightforward. However, understanding exactly what to expect at each stage prevents anxiety and helps you catch complications early.
Complete Recovery Timeline
| Timeline | What to Expect | Key Care Actions |
|---|---|---|
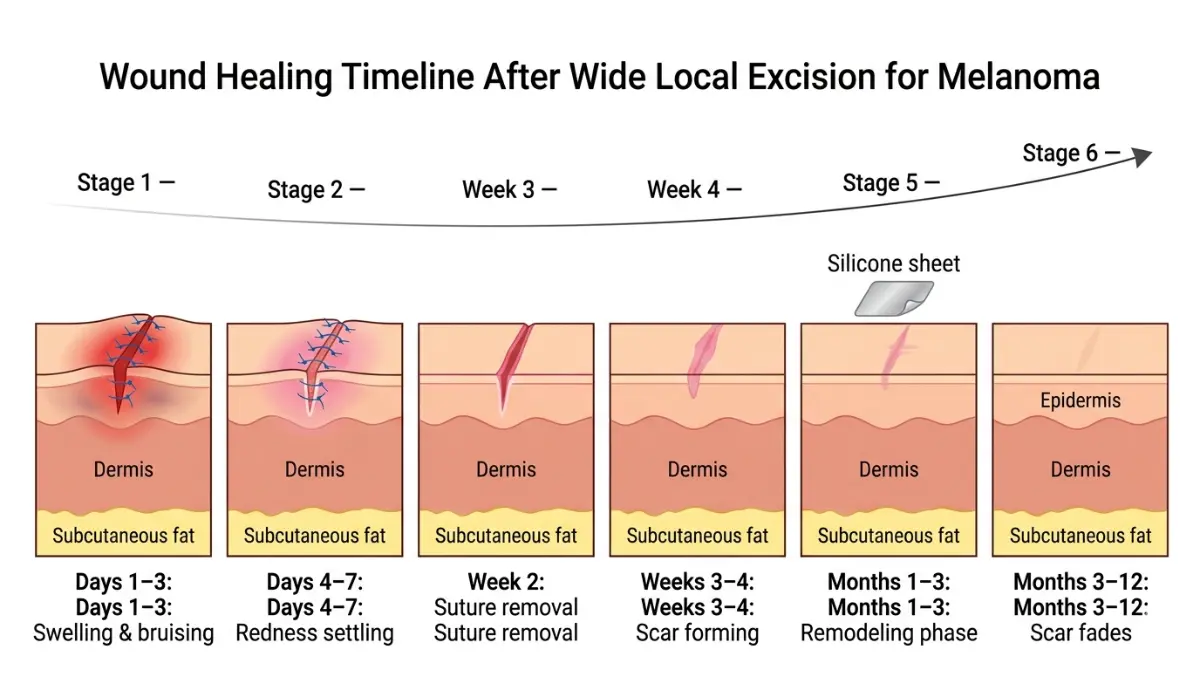
| Days 1–3 | Swelling, bruising, tightness, mild soreness | Keep wound dry, take prescribed analgesics |
| Days 4–7 | Redness begins settling, sutures visible | Gentle wound cleaning per surgeon’s instructions |
| Week 2 | Wound closes; non-absorbable sutures removed | Follow-up appointment; pathology results arrive |
| Weeks 3–4 | Full wound closure; pink scar forming | Begin scar care if surgeon clears you |
| Months 1–3 | Scar remodeling phase — may appear raised and pink | Silicone gel sheets, SPF 50+ on scar |
| Months 3–12 | Scar flattens and fades | Scar massage, continued sun protection |
Body-Location Differences in Recovery:
- Face: Heals fastest (excellent blood supply), often 1–2 weeks to closure
- Trunk: Standard 2–3 week closure timeline
- Lower legs and feet: Slowest healing — 3–6 weeks; risk of dehiscence if patient is mobile too early
Return to Activities:
- Desk work: 1–3 days
- Light walking: 1–2 weeks
- Exercise and sport: 2–4 weeks
- Swimming: 6+ weeks (risk of infection until fully healed)
Warning Signs — Call Your Doctor Immediately If You Notice:
- Wound edges separating (dehiscence)
- Increasing redness, warmth, or purulent discharge (infection)
- Bleeding that doesn’t stop within 10 minutes of direct pressure
- Fever above 101°F / 38.3°C
- Severe or worsening pain after Day 3
Recovery quality is heavily influenced by sleep. During wound healing, growth hormone is primarily released during deep sleep cycles. Use our Sleep Calculator to optimize your sleep schedule during the post-surgical period.
Emotional Recovery — The Part Nobody Talks About
Physical healing is only part of the story. A 2024 report by the Melanoma Research Foundation found that 40–60% of melanoma patients experience clinically significant anxiety during the post-surgical period, particularly while awaiting pathology results.
Common emotional responses after WLE:
- Scan anxiety or “scanxiety” — fear of results
- Body image concerns related to scar visibility
- Relief mixed with fear of recurrence
- Sleep disturbances during the waiting period
These are completely normal. Speak openly with your oncology nurse, and ask for a referral to a oncology psychologist if anxiety is persistent.
Wide Local Excision Scars — Types, Treatment & 2026 Minimization Protocol
The scar following wide local excision is the most visible reminder of surgery — and the aspect patients ask about most. Understanding scar types and evidence-based treatment empowers you to take control of your healing.
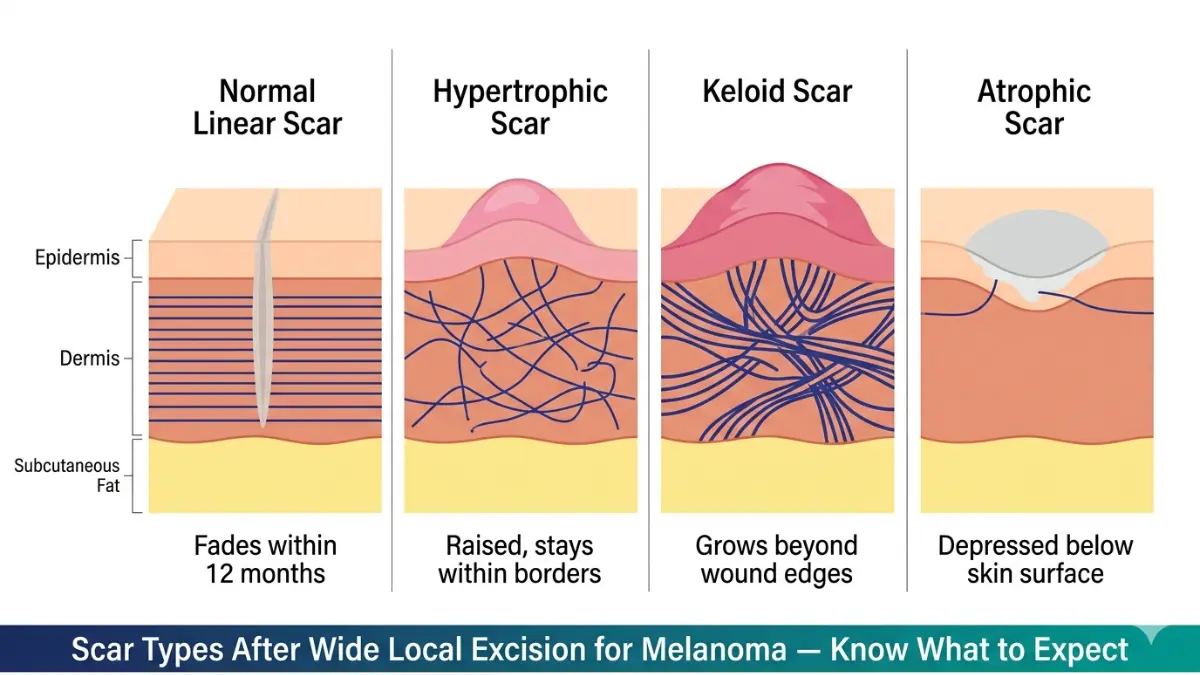
Scar Types After Wide Local Excision
| Scar Type | Appearance | Risk Factors | Treatment |
|---|---|---|---|
| Normal linear scar | Thin, flat, fades to pale | Ideal healing conditions | SPF 50+, silicone gel |
| Hypertrophic scar | Raised, stays within wound margins | Chest, shoulder location; tension on wound | Silicone sheets, steroid injection |
| Keloid scar | Grows beyond wound borders | Family history, darker skin tones | Corticosteroid injection, laser therapy |
| Atrophic scar | Depressed or sunken | Poor wound healing, older age | Dermal fillers, microneedling |
According to the British Association of Dermatologists, hypertrophic scarring affects up to 10% of melanoma excision patients, with highest rates seen in patients with chest or shoulder primary sites.
2026 Evidence-Based Scar Minimization Protocol
Step 1 — Sun Protection (Start Week 3–4) Apply SPF 50+ broad-spectrum sunscreen to the scar every day. UV radiation is the primary cause of scar hyperpigmentation and delayed maturation. This is the single most effective thing you can do.
Step 2 — Silicone Gel Sheets (Start after suture removal)
- Wear 12 hours per day for 3–6 months
- Clinical evidence confirms silicone sheets reduce hypertrophic scar formation by up to 60%
- Available over-the-counter at most pharmacies
Step 3 — Scar Massage (Start Week 6)
- Apply gentle circular pressure for 5 minutes daily
- Breaks down excess collagen cross-links that cause raised scars
- Use a fragrance-free moisturizer as a lubricant
Step 4 — Topical Treatments
- Onion extract (Mederma): Moderate evidence for scar softening
- Vitamin C serum: Supports collagen remodeling in the maturation phase
- Avoid petroleum-based products in the first 2 weeks
Step 5 — When to See a Plastic Surgeon If your scar is still raised and red at 6 months, or if it is causing physical restriction or significant cosmetic distress, a referral to a plastic surgeon for corticosteroid injection or laser resurfacing is warranted. The AAD patient guide on scars provides detailed criteria for when professional intervention is recommended.
Adequate hydration supports skin cell regeneration and collagen production throughout the scar remodeling phase. Track your daily fluid intake with our Water Intake Calculator to ensure optimal recovery conditions.
Outcomes, Follow-Up & When WLE Is Part of a Larger Treatment Plan
Survival Outcomes After Wide Local Excision
The data here is genuinely reassuring. According to the American Cancer Society’s 2025 survival statistics, the 5-year survival rate for localized melanoma is 99% — one of the highest among all cancers when caught early.
Local recurrence following WLE with adequate margins occurs in fewer than 1–2% of cases, based on pooled data from multicenter clinical trials reviewed in a PMC systematic analysis of NCCN margin trials.
Factors that influence recurrence risk:
- Breslow thickness (thicker = higher risk)
- Ulceration present in the primary tumor
- Positive or narrow pathological margins
- Melanoma located on head or neck
When WLE Is Combined With Systemic Therapy
For early-stage melanoma (Stages 0–II), WLE alone is often curative. For Stage III melanoma or high-risk Stage IIC disease, WLE becomes one component of a broader treatment plan. The NCI Treatment PDQ for melanoma outlines how WLE integrates with the following:
- Adjuvant immunotherapy: Pembrolizumab or nivolumab given after WLE to eliminate microscopic residual disease — now standard for Stage IIB–III per 2026 NCCN guidelines
- Neoadjuvant therapy (2026 emerging approach): Immunotherapy or targeted BRAF/MEK inhibitors started before WLE to shrink tumors and assess treatment response
- Adjuvant radiation: Considered for desmoplastic melanoma with perineural invasion at head and neck sites
For a deeper understanding of how WLE fits within the full treatment landscape, read our comprehensive guide on melanoma treatment options and explore the evidence on immunotherapy for melanoma.
Follow-Up Schedule After Wide Local Excision
| Melanoma Stage | Follow-Up Frequency | What Is Monitored |
|---|---|---|
| Stage 0–I | Every 6–12 months | Full skin exam, lymph node palpation |
| Stage II | Every 3–6 months for 3 years | Skin exam, imaging if clinically indicated |
| Stage III+ | Every 3 months for 2 years | Imaging, bloodwork, oncology review |
Per Cancer Research UK’s clinical guidance, patients are taught to perform monthly self-skin examinations between appointments — a skill your dermatology team will demonstrate before discharge.
Lifelong Sun Protection Is Non-Negotiable:
After wide local excision for melanoma, UV exposure is your highest modifiable risk factor for a new primary melanoma. Wear SPF 50+ daily, seek shade between 10 AM–4 PM, and avoid tanning beds permanently.
For complete context on your melanoma journey — from the original warning signs through staging and beyond surgery — our melanoma symptoms, stages, and treatment pillar guide provides the full clinical picture. To understand how your stage directly affects long-term prognosis, explore our detailed melanoma survival rate by stage breakdown.
If you have a first-degree relative with melanoma, regular surveillance and genetic risk evaluation is strongly recommended — start with our Genetic Risk Assessment Tool to quantify your inherited risk.
✅ What This Means For You: WLE with clear margins, combined with regular follow-up, gives you a statistical 99% chance of 5-year survival for localized disease. The surgery is a beginning — not an ending.
Frequently Asked Questions
1. What is wide local excision for melanoma?
Wide local excision is a surgical procedure that removes the melanoma plus a margin of healthy surrounding skin (0.5–2 cm depending on tumor depth). It is the gold-standard curative treatment for localized melanoma per 2026 NCCN guidelines.
2. How much skin is removed during wide local excision for melanoma?
Margins range from 0.5 cm for melanoma in situ to 2 cm for melanomas thicker than 2 mm, based on Breslow depth. Your surgical oncologist determines the precise margin from your pathology report.
3. Is wide local excision for melanoma a major surgery?
No. WLE is typically a minor outpatient procedure under local anesthesia, completed in 30–60 minutes. Cases requiring skin grafts may involve a brief hospital stay.
4. How long does wide local excision melanoma recovery take?
Most wounds close within 2–3 weeks. Full scar maturation takes 6–12 months. Desk work is typically possible within 1–3 days; strenuous exercise resumes after 2–4 weeks.
5. Will I have a big scar after wide local excision for melanoma?
Scar size depends on melanoma size and body location. Most WLE scars are linear and fade significantly within 12 months. Silicone gel sheets and SPF 50+ are the most evidence-backed scar minimization strategies.
6. Can wide local excision be performed on the face?
Yes, though face margins may be reduced to preserve cosmetic appearance and function, sometimes favoring Mohs micrographic surgery for melanoma in situ on the face. A multidisciplinary team determines the safest approach.
7. What are the risks of wide local excision for melanoma?
Risks include infection, bleeding, nerve damage (tingling/numbness), poor wound healing, and hypertrophic or keloid scarring. Serious systemic complications are rare given the outpatient nature of most WLE procedures.
8. What is the difference between wide local excision and an excision biopsy?
An excision biopsy removes just the suspicious lesion for diagnosis. WLE removes a larger margin of healthy surrounding tissue around the confirmed melanoma to achieve microscopically clear margins and minimize recurrence risk.
9. Do I need a skin graft after wide local excision for melanoma?
Most patients don’t need a graft — primary suture closure is sufficient. Grafts are used when the excision area is too large for direct closure, most commonly on the face, scalp, or lower limbs.
10. What happens if surgical margins are not clear after wide local excision?
Positive margins typically require re-excision to remove additional tissue. Your multidisciplinary team reviews pathology results and determines next steps, which may include further surgery or adjuvant therapy.
11. Can melanoma return after wide local excision?
Local recurrence after WLE with adequate margins is rare — approximately 1–2%. Regular follow-up every 3–12 months and vigilant self-skin examinations are essential. Learn the full warning sign profile in our melanoma warning signs guide.
Reviewed by the mymedicineadvisor.com Medical Advisory Board | This article is for educational purposes only. It does not constitute medical advice. Always consult a qualified dermatologist or surgical oncologist for diagnosis, treatment decisions, and personalized care.
📌 Continue Reading:
- Melanoma Stages — Full Clinical Breakdown
- Sentinel Lymph Node Biopsy: What to Expect
- Melanoma Treatment Options: 2026 Complete Guide
- How Is Melanoma Diagnosed?
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.