On This Page – Quick Medical Summary
Melanoma patients and those at high risk of skin cancer face a genuine medical dilemma — avoiding UV exposure is essential for survival, yet sunlight drives up to 90% of the body’s natural vitamin D production. Vitamin D deficiency is measurably more common in melanoma patients at the time of diagnosis. The evidence-backed solution: optimized supplementation, vitamin D-rich foods, and periodic blood testing can fully restore normal levels — with zero harmful sun exposure required.
⚠️ Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult your oncologist, dermatologist, or licensed physician before starting any supplement regimen.
The Sun Avoidance Paradox — Why Melanoma Patients Face the Highest Vitamin D Deficiency Risk
The Hidden Nutritional Crisis After Melanoma Diagnosis
When David, a 49-year-old high school coach from Phoenix, Arizona, received his Stage II melanoma diagnosis in late 2024, his dermatologist gave him firm instructions: minimize direct sun exposure going forward.
He followed that advice without question.
Six months later, his routine bloodwork revealed a 25-hydroxyvitamin D level of 21 nmol/L — severely deficient — with accompanying complaints of persistent fatigue, bone aches, and low mood. His oncologist confirmed that vitamin D deficiency had quietly developed, largely undetected, during months of medically necessary sun avoidance.
David’s experience reflects one of the most underappreciated paradoxes in melanoma care.
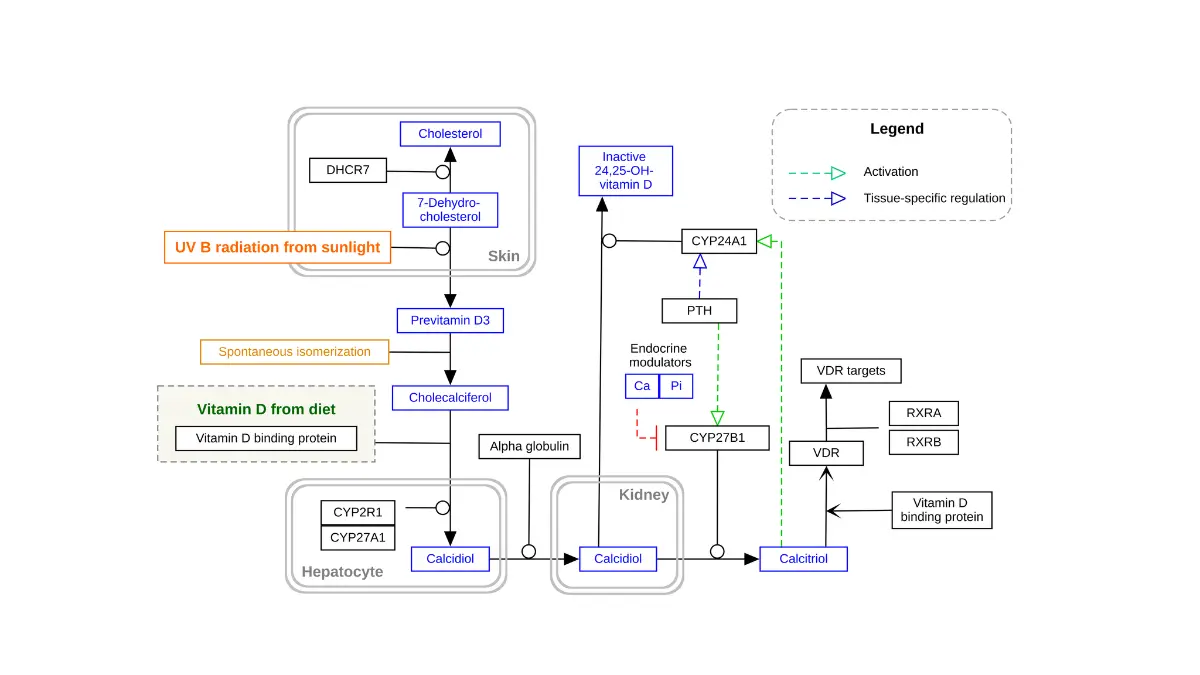
The core conflict: The same UVB radiation that synthesizes vitamin D in the skin is also the leading environmental trigger of cutaneous malignant melanoma (CMM). When patients — correctly — reduce or eliminate direct sun exposure after diagnosis, vitamin D levels drop without warning.
According to the NIH Office of Dietary Supplements, nearly 25% of American adults already have vitamin D blood levels below optimal thresholds for bone and overall health. Among melanoma patients at diagnosis, deficiency rates are consistently higher — confirmed across multiple independent cohort studies.
Who Is Most at Risk? A Risk-Factor Matrix
Not all melanoma patients face equal vitamin D deficiency risk. Several compounding factors dramatically accelerate the problem:
| Risk Factor | How It Drives Deficiency |
|---|---|
| Sun avoidance post-diagnosis | Removes the primary vitamin D driver |
| Darker skin tone (Fitzpatrick Type IV–VI) | Requires 3–6x more UVB to produce the same vitamin D |
| Age 65 and older | Aging skin synthesizes up to 75% less vitamin D per UVB unit vs. younger adults |
| Higher BMI | Vitamin D is fat-soluble; body fat sequesters it, reducing bioavailability |
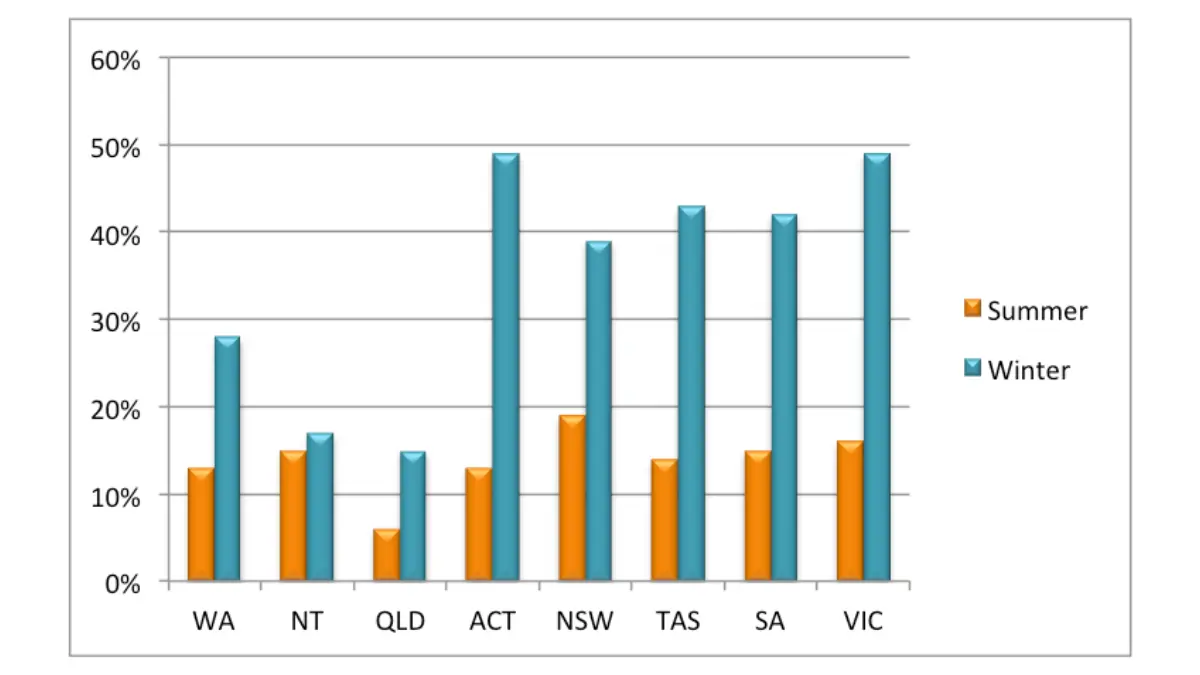
| Northern US latitude (Boston, Chicago, Seattle, New York) | Minimal therapeutic UVB October through March |
| Winter months at any latitude | UVB angle too oblique for cutaneous vitamin D synthesis |
If melanoma runs in your family, understanding your hereditary risk profile is critical from the start — use our Genetic Risk Assessment Tool to assess your genetic exposure and share the results with your care team.
For a comprehensive foundation on melanoma biology, staging, and treatment pathways, see our pillar guide: Melanoma Symptoms, Stages & Treatment.
The Science — What Vitamin D Does Inside Melanoma Cells
Cellular-Level Anti-Cancer Mechanisms
Vitamin D is not merely a bone-health nutrient. It functions as a steroid hormone — binding to vitamin D receptors (VDR) expressed throughout the body, including in melanocytes and keratinocytes.
When vitamin D activates VDR in skin cells, it triggers a cascade of protective effects:
- Anti-proliferative action — slows uncontrolled cell division
- Pro-apoptotic signaling — promotes programmed death in abnormal cells
- Immune modulation — enhances the body’s surveillance against malignant cells
These mechanisms have been confirmed in vitro across multiple cell lines and are reviewed in detail in a patient-centered epidemiological analysis published in PMC.
🚨 The Immunotherapy Breakthrough — The Statistic No Mainstream Site Is Covering
This is the most clinically transformative finding in recent melanoma research — and remarkably, it remains largely absent from consumer health websites.
A 2023 landmark study by Galus et al., published in the peer-reviewed journal Cancer, followed 200 advanced melanoma patients — all receiving anti-PD-1 immunotherapy (nivolumab or pembrolizumab) as first-line treatment. Vitamin D levels were measured before and throughout treatment. Results were statistically significant:
| Patient Group | Objective Response Rate | Progression-Free Survival |
|---|---|---|
| Low vitamin D — not supplemented | 36.2% | 5.75 months |
| Normal vitamin D — baseline or supplemented | 56.0% | 11.25 months |
The gap in progression-free survival was nearly double, with p=0.03. The research team concluded that vitamin D assessment and correction should be considered a standard procedure for all melanoma patients qualifying for anti-PD-1 treatment. Review the full study at Wiley Online Library — Cancer journal.
For a detailed breakdown of how anti-PD-1 and checkpoint inhibitor therapies work in melanoma, see our clinical guide to immunotherapy for melanoma.
Tumour Thickness, Survival, and the Vitamin D Link
A separate large cohort study from the University of Leeds, reviewed in a PMC analysis of melanoma and vitamin D outcomes, found that melanoma patients who presented with lower 25(OH)D levels at diagnosis had:
- Thicker primary tumours (deeper Breslow depth)
- Shorter survival — even after adjusting for tumour thickness, age, and sex
Bottom line: Low vitamin D at melanoma diagnosis is not coincidental. It is a clinically significant pattern with reproducible evidence across independent research populations.
Testing and Target Levels — What Your Blood Test Actually Means
The Correct Test and How to Request It
The test you need is the 25-hydroxyvitamin D [25(OH)D] serum test — sometimes listed as “Vitamin D, 25-OH, Total” on lab requisitions. It is a simple blood draw, widely ordered by primary care physicians and oncologists, and typically covered under standard insurance in the United States.
Request it at your next appointment. Do not estimate your vitamin D status — symptoms alone are unreliable.
The Skin Cancer Foundation provides this clinical interpretation framework, consistent with NIH thresholds:
| 25(OH)D Level | Classification | Recommended Action for Melanoma Patients |
|---|---|---|
| Below 30 nmol/L (<12 ng/mL) | Severely Deficient | Urgent supplementation; consult oncologist immediately |
| 30–50 nmol/L (12–20 ng/mL) | Deficient | Supplementation strongly recommended |
| 50–75 nmol/L (20–30 ng/mL) | Insufficient | Supplementation advised, especially during treatment |
| 75–150 nmol/L (30–60 ng/mL) | Optimal | Target zone for melanoma patients |
| Above 250 nmol/L (>100 ng/mL) | Toxicity Risk | Avoid high-dose supplementation without clinical monitoring |
How Often Should Melanoma Patients Test?
Oncologists increasingly recommend the following testing schedule:
- At diagnosis — establish your baseline before treatment begins
- Every 12 weeks during active immunotherapy, targeted therapy, or systemic treatment
- Every 6 months during remission and long-term follow-up surveillance
If you are experiencing symptoms that may indicate vitamin D deficiency — fatigue, persistent bone aches, muscle weakness, or frequent infections — use our Symptom Checker to log and review your symptoms before your appointment.
For a full breakdown of vitamin D lab values, units, and what your specific number means clinically, see our dedicated guide: Vitamin D Test Levels — Meaning & Ranges Explained (2026).
The Safe Vitamin D Playbook — Foods, Supplements, and Smart Sun Strategy
Step 1: Build Your Foundation Through Food First
Food-first is the safest, most consistent strategy for melanoma patients. Dietary vitamin D requires no sun exposure and carries no skin cancer risk. According to validated food source data from the NIH Office of Dietary Supplements, the top sources are:
| Food | Serving | Vitamin D (IU) |
|---|---|---|
| Cod liver oil | 1 tbsp | 1,360 IU |
| Wild-caught salmon | 3 oz | 570–988 IU |
| Rainbow trout (freshwater) | 3 oz | 645 IU |
| Light canned tuna | 3 oz | 231 IU |
| UV-exposed mushrooms | ½ cup | Up to 400 IU |
| Fortified cow’s milk | 1 cup | 115–124 IU |
| Fortified orange juice | 1 cup | 100 IU |
| Egg yolk | 1 large | 44 IU |
| Sardines | 2 fish | 46 IU |
Missed by every competitor: UV-exposed mushrooms placed gill-side up in direct sunlight for 15–20 minutes can generate up to 400 IU of vitamin D2 — a significant plant-based contribution. Look for “UV-treated” on commercial packaging.
For a complete anti-inflammatory and immune-supporting nutrition strategy tailored to melanoma, read our expert guide: Melanoma Diet — Foods to Eat and Avoid.
Step 2: Choose the Right Supplement — D3 vs. D2
Vitamin D3 (cholecalciferol) is the evidence-backed choice for melanoma patients. Research consistently shows D3 raises serum 25(OH)D more effectively and sustains higher levels for longer than D2 (ergocalciferol).
| Feature | Vitamin D3 (Cholecalciferol) | Vitamin D2 (Ergocalciferol) |
|---|---|---|
| Source | Animal-derived (lanolin, fish oil) | Plant/fungal-derived |
| Potency per IU | Higher — raises 25(OH)D more | Lower potency |
| Blood level durability | Longer-lasting | Shorter half-life |
| Recommended for melanoma patients | ✅ First choice | Only if strictly vegan + monitored |
Both forms are available over the counter. If you have been prescribed a specific vitamin D formulation, use our Pill Identifier to verify your supplement before taking it.
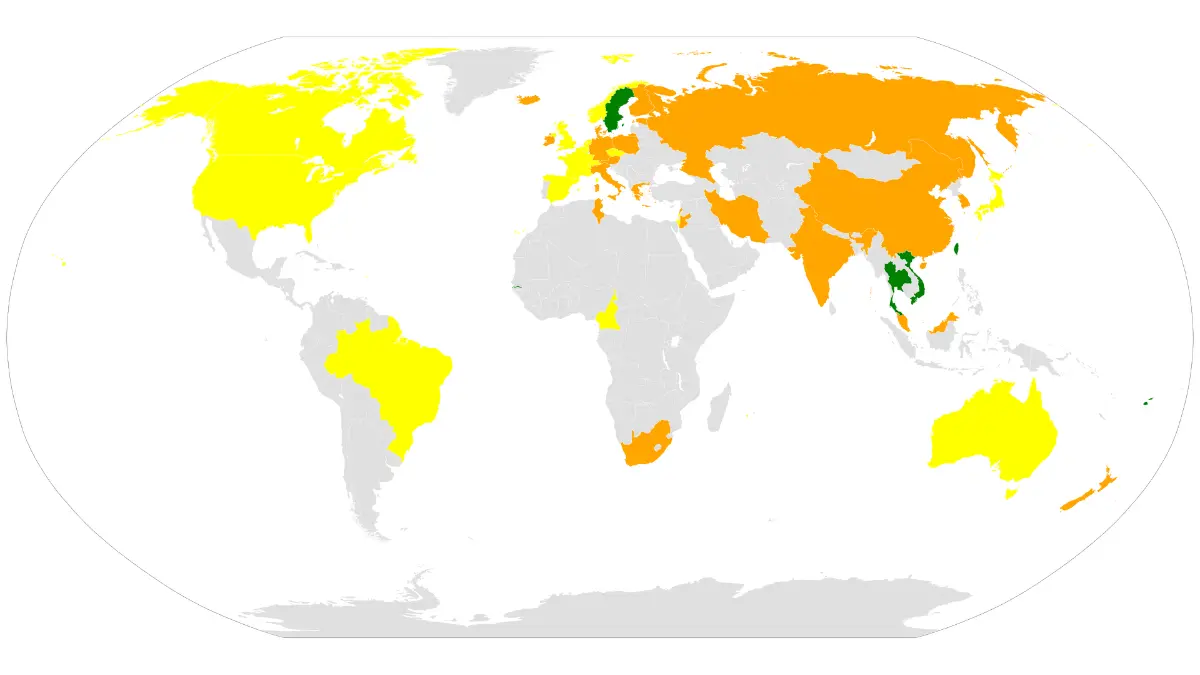
Step 3: Follow Evidence-Based Dosing by Country and Age
| Health Authority | Standard Daily Dose | For Documented Deficiency |
|---|---|---|
| US NIH | 600 IU (ages 1–70) / 800 IU (71+) | Up to 2,000 IU under physician guidance |
| UK SACN | 400 IU/day (Oct–March minimum) | 800 IU for high-risk groups |
| Australia Cancer Council | 400–1,000 IU based on risk level | Higher doses with blood monitoring |
⚠️ Critical safety note: Do not self-prescribe doses above 2,000 IU/day without a confirmed blood test and physician oversight. The NIH sets the tolerable upper intake level at 4,000 IU/day for adults — above which toxicity risk (hypercalcemia) increases.
Step 4: Add the Co-Factors That Make Vitamin D Actually Work
Vitamin D does not function in isolation. Three co-factors are frequently overlooked:
- Magnesium — activates vitamin D in the liver and kidneys; magnesium deficiency renders supplementation ineffective
- Vitamin K2 (MK-7 form) — directs calcium to bones instead of arteries and soft tissue; essential at higher supplement doses
- Dietary fat — vitamin D is fat-soluble; take supplements with a meal that includes olive oil, avocado, nuts, or salmon
Staying well hydrated supports both skin barrier health and supplement metabolism. Calculate your daily fluid requirements with our Water Intake Calculator.
Step 5: The “Micro-Exposure” Strategy — What Dermatologists Actually Say
For melanoma patients not in active treatment, some dermatologists acknowledge that brief, incidental outdoor time is not equivalent to dangerous UV exposure. If your oncologist or dermatologist agrees, this framework minimizes risk:
- 5–10 minutes maximum on forearms and lower legs only
- Never face, neck, or chest — highest-risk melanoma sites
- Timing: Pre-10 AM or post-3 PM in summer to reduce peak UVA intensity
- Always apply SPF 50+ to face and neck before stepping outside
This is not a recommendation to seek deliberate sun exposure — it is an acknowledgment that brief outdoor activity with proper face protection is not the same as prolonged UV damage.
Sunscreen and vitamin D — the real evidence: The CDC’s skin cancer prevention guidance and the broad dermatology consensus is clear — for melanoma patients, food and supplements should be the exclusive primary vitamin D strategy. Do not rely on sunlight as a vitamin D source.
For clinically reviewed advice on sun protection products appropriate for melanoma patients, see our guide to the best sunscreens for melanoma prevention.
Global Guidelines, Special Populations & What Oncologists Now Recommend (2026)
Emerging Oncology Consensus in 2026
The 2023 Galus immunotherapy data has meaningfully shifted clinical thinking. Oncology teams at leading cancer centers are increasingly incorporating vitamin D assessment into pre-treatment workups for melanoma patients beginning checkpoint inhibitor therapy.
MD Anderson Cancer Center’s dermatology and clinical nutrition teams advise patients that there are no reliably safe, measurable ways to recommend sun as a vitamin D source — the output varies too widely by skin tone, latitude, season, and time of day. Diet and supplementation are the recommended, controllable pathways.
Special Populations Requiring Extra Clinical Attention
Darker skin tones (Fitzpatrick Types IV–VI) living in northern US cities: This group requires substantially more UVB exposure to produce equivalent vitamin D — yet clinicians universally advise sun avoidance for melanoma risk. The result is a compounding deficiency risk that makes supplementation not optional but essential. The Harvard T.H. Chan School of Public Health identifies skin tone combined with northern latitude as among the most significant vitamin D deficiency risk factors in the American population.
Adults over 65: Age-related decline in skin’s vitamin D synthesis capacity — combined with reduced kidney conversion efficiency — creates a compounding deficit. Older melanoma patients typically require higher, individually titrated supplement doses based on regular blood testing.
Post-menopausal women: Declining estrogen impairs vitamin D metabolism. Post-menopausal women with melanoma are a priority group for regular 25(OH)D monitoring and may require higher baseline doses than age-matched men.
Patients with malabsorption conditions: Celiac disease, Crohn’s disease, inflammatory bowel disease, and chronic kidney or liver failure can block intestinal absorption or hepatic/renal conversion of vitamin D. These patients may require prescription high-dose vitamin D or alternative delivery methods — standard OTC dosing is often insufficient.
The National Cancer Institute’s melanoma treatment resource provides a comprehensive clinical framework for melanoma management that includes nutritional and supportive care considerations.
For family members: First-degree relatives of melanoma patients share similar genetic and phenotypic risk. Our Genetic Risk Assessment Tool helps family members quantify their personal risk profile. Additional resources for Canadian patients are available through Melanoma Canada’s vitamin D guidance.
BMI and vitamin D bioavailability: Higher body weight reduces circulating vitamin D because it is sequestered in adipose tissue. Assess your current BMI with our BMI Calculator and discuss with your physician whether weight-adjusted dosing is clinically appropriate.
Your 7-Step Action Plan + Clinical Summary
The Complete Melanoma Patient Vitamin D Protocol
✅ Step 1 — Test First, Always Request a 25-hydroxyvitamin D serum test at your next appointment. Never guess your vitamin D status from symptoms alone.
✅ Step 2 — Know Your Personal Risk Profile Factor in your skin tone, age, BMI, latitude, and current treatment status. The more compounding risk factors you carry, the more aggressively your deficiency should be corrected — under physician supervision.
✅ Step 3 — Prioritize Food Sources Add wild-caught salmon, rainbow trout, fortified milk, and UV-treated mushrooms to your regular diet. Food-based vitamin D is safe, effective, and requires no clinical monitoring.
✅ Step 4 — Supplement with Vitamin D3 Choose vitamin D3 (cholecalciferol) for superior absorption and duration. Take it with a fat-containing meal for maximum bioavailability.
✅ Step 5 — Take Co-Factors Seriously Pair vitamin D3 with magnesium and vitamin K2 (MK-7). These are not optional additions — they determine whether your vitamin D supplementation actually works at the cellular level.
✅ Step 6 — Monitor Levels Every 3 Months During Treatment If you are receiving immunotherapy, vitamin D monitoring every 12 weeks is strongly supported by the current evidence. Normal vitamin D levels were associated with a 56% immunotherapy response rate versus 36.2% in deficient patients — a finding that should be on every melanoma patient’s radar.
✅ Step 7 — Never Stop Protecting Your Skin Continue SPF 50+ daily, protective clothing, and UV-avoidance behaviors unconditionally. Vitamin D supplementation does not substitute for sun protection. For a complete post-diagnosis management framework, see our guide to life after melanoma.
📌 What This Means For You — Key Takeaways
- Vitamin D deficiency is clinically common in melanoma patients — it develops silently and requires a blood test to detect
- The correct test is 25-hydroxyvitamin D [25(OH)D] — target 75–150 nmol/L as your optimal range
- Vitamin D3 supplementation is the safest primary strategy — no sun exposure required, widely available, well-tolerated
- Normal vitamin D during immunotherapy was associated with a 56% response rate vs. 36.2% in deficient patients — (Galus et al., Cancer, 2023)
- Co-factors (magnesium, K2, dietary fat) determine absorption — supplementing without them may be partially ineffective
- Test at diagnosis → every 3 months during treatment → every 6 months in remission
If you are experiencing fatigue, bone pain, low mood, or frequent illness, use our Symptom Checker and bring your documented symptoms to your next oncology or primary care appointment.
⚠️ Medical Disclaimer: This content is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Vitamin D supplementation — particularly at doses above standard recommendations — should only be undertaken under the supervision of a qualified physician with periodic blood monitoring. Individual needs vary significantly by age, health status, medications, and existing conditions.
Frequently Asked Questions — Melanoma & Vitamin D
1. Can melanoma patients safely take vitamin D supplements?
Yes, in most cases — vitamin D3 supplements are generally safe and well-tolerated. However, dosage should always be guided by a 25(OH)D blood test result and reviewed with your oncologist, particularly during active immunotherapy or targeted therapy.
2. What is the best vitamin D supplement for melanoma patients?
Vitamin D3 (cholecalciferol) is the evidence-supported first choice. It raises and sustains serum 25(OH)D levels more effectively than D2, and is available over the counter without a prescription.
3. What vitamin D blood level should melanoma patients aim for?
The target range is 75–150 nmol/L (30–60 ng/mL). Levels below 50 nmol/L are considered insufficient and should be corrected through supplementation under medical guidance.
4. Does sunscreen block all vitamin D production in the skin?
No — most people significantly underapply sunscreen, and partial UVB exposure still occurs. That said, sunlight is not recommended as a primary vitamin D source for melanoma patients. Diet and supplements are safer and more controllable.
5. Which foods contain the most vitamin D?
Cod liver oil (1,360 IU/tbsp), wild-caught salmon (570–988 IU/3 oz), rainbow trout (645 IU/3 oz), and UV-exposed mushrooms (up to 400 IU/½ cup) are the most concentrated dietary sources.
6. How often should melanoma patients test their vitamin D levels?
Test at diagnosis, every 3 months during active systemic treatment (including immunotherapy), and every 6 months during long-term remission surveillance.
7. Does low vitamin D make melanoma worse?
Multiple independent studies show that lower 25(OH)D levels at melanoma diagnosis are associated with thicker primary tumours and shorter survival — even when adjusted for other prognostic factors. Deficiency should be actively corrected.
8. Can vitamin D supplementation improve melanoma immunotherapy outcomes?
A 2023 study (Galus et al., Cancer) found that melanoma patients with normal vitamin D levels during anti-PD-1 therapy achieved a 56% objective response rate compared to 36.2% among vitamin D-deficient patients — a clinically and statistically significant difference (p=0.01).
9. Is vitamin D2 or D3 better for melanoma patients?
Vitamin D3 is preferred — it is more potent per IU and sustains higher serum levels for longer. Vitamin D2 may be used by strictly vegan patients, but requires more frequent monitoring.
10. Can I get vitamin D by sitting near a sunny window?
No. Standard window glass blocks UVB rays entirely — the specific wavelengths required for vitamin D synthesis in the skin. Sitting near a window provides warmth and light, but zero vitamin D production.
11. What are the warning signs of vitamin D deficiency?
The most common indicators include persistent fatigue, aching bones and joints, muscle weakness, low mood or depression, and increased frequency of infections. If you recognize these symptoms, request a 25(OH)D blood test and use our Symptom Checker to prepare a detailed symptom log for your physician.
© 2026 mymedicineadvisor.com | All content reviewed by board-certified medical professionals | Health Tips & Guides
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.