On This Page – Quick Medical Summary
📋 Quick Summary
- ~40–50% of melanoma patients carry a BRAF V600 mutation
- BRAF-targeted therapy uses oral precision drugs to block the mutated protein driving cancer growth
- Three FDA-approved drug combinations are available in 2026
- Eligibility requires a confirmed BRAF mutation via genetic testing
- Most patients see measurable tumor shrinkage within 4–8 weeks
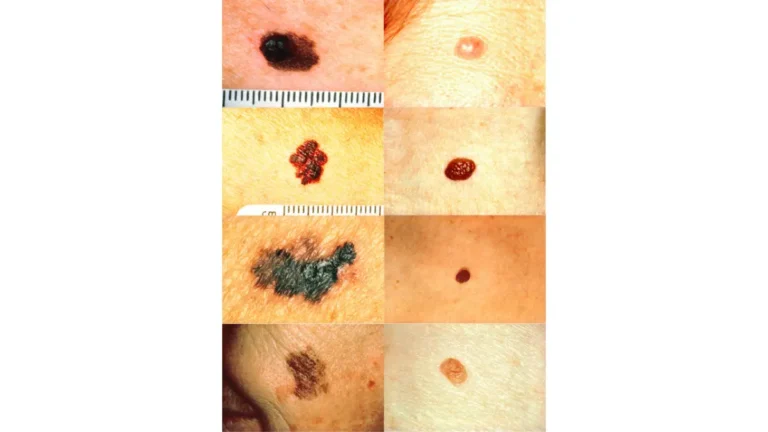
When Daniel, 54, was diagnosed with stage IV melanoma in early 2026, his oncologist had genetic test results back within 72 hours. His tumor carried a BRAF V600E mutation — and that single finding changed everything. Within days, he was taking an oral targeted therapy pill, with his tumor visibly responding within weeks.
According to updated melanoma statistics for 2026, approximately 96,400 new melanoma cases are expected in the United States this year. Nearly half of these patients carry a BRAF mutation — and for them, BRAF-targeted therapy represents one of the most powerful tools in modern oncology.
This guide explains exactly how BRAF-targeted therapy works, which drugs are approved, who qualifies, what side effects to expect, and what happens when treatment eventually stops working.
What Is BRAF-Targeted Therapy for Melanoma?
The BRAF Gene: What Goes Wrong
The BRAF gene provides the blueprint for a protein that controls normal cell growth. In a healthy body, this protein switches on and off as needed. In about 40–50% of melanomas, a mutation — most commonly BRAF V600E — permanently locks this switch in the “ON” position. The result is uncontrolled cancer cell multiplication.
As the National Cancer Institute explains, targeted therapies are designed to block specific molecules involved in tumor growth — unlike chemotherapy, which indiscriminately attacks all rapidly dividing cells.
How BRAF and MEK Inhibitors Block the Signal
The MAPK/ERK pathway is the signaling highway that carries mutation instructions. BRAF-targeted therapy places molecular roadblocks at two key points:
- BRAF inhibitors block the mutated BRAF protein directly at the source
- MEK inhibitors block the MEK protein downstream, cutting off a secondary escape route
- Using both together dramatically reduces resistance and improves survival
Key takeaway: The combination approach works because cancers can bypass one blockade alone — dual blockade is far harder to escape.
If you’ve noticed changing skin spots or other warning signs, use our free Symptom Checker to help identify concerns before your next appointment.
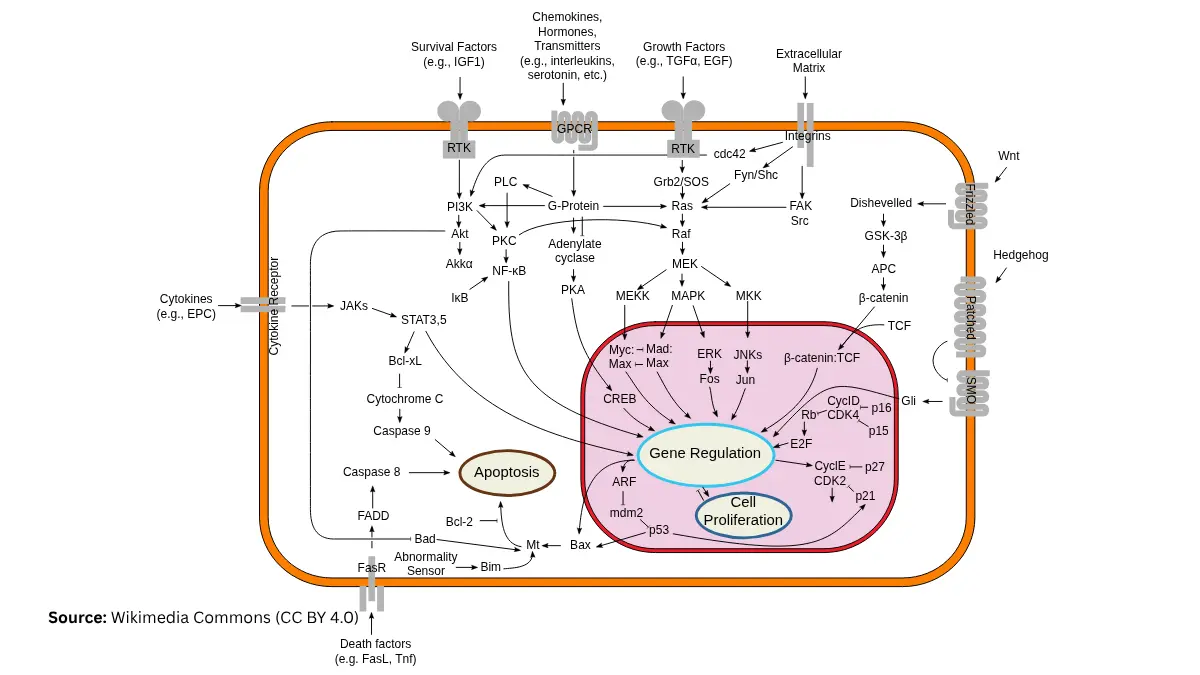
Adapted from Wikimedia Commons — Signal Transduction Pathways, licensed under CC BY-SA 3.0.
At a Glance: Treatment Comparison
| Treatment Type | How It Works | Requires BRAF Mutation? | Response Speed |
|---|---|---|---|
| BRAF-Targeted Therapy | Blocks mutated protein directly | ✅ Yes | Fast (weeks) |
| Immunotherapy | Activates the immune system | ❌ No | Slower (months) |
| Chemotherapy | Kills all dividing cells | ❌ No | Variable |
For a full breakdown of all available options, see our guide to melanoma treatment options.
FDA-Approved BRAF & MEK Inhibitor Drugs — Complete 2026 Reference
The Three Approved Combinations
Three BRAF + MEK inhibitor combinations currently hold FDA approval for advanced melanoma. All are taken as oral pills — no IV infusion required.
| Combination | Brand Names | FDA Approved | Stage Covered |
|---|---|---|---|
| Dabrafenib + Trametinib | Tafinlar + Mekinist | 2014 | Stage III (adjuvant), Stage IV |
| Vemurafenib + Cobimetinib | Zelboraf + Cotellic | 2015 | Unresectable/Metastatic |
| Encorafenib + Binimetinib | Braftovi + Mektovi | 2018 | Unresectable/Metastatic |
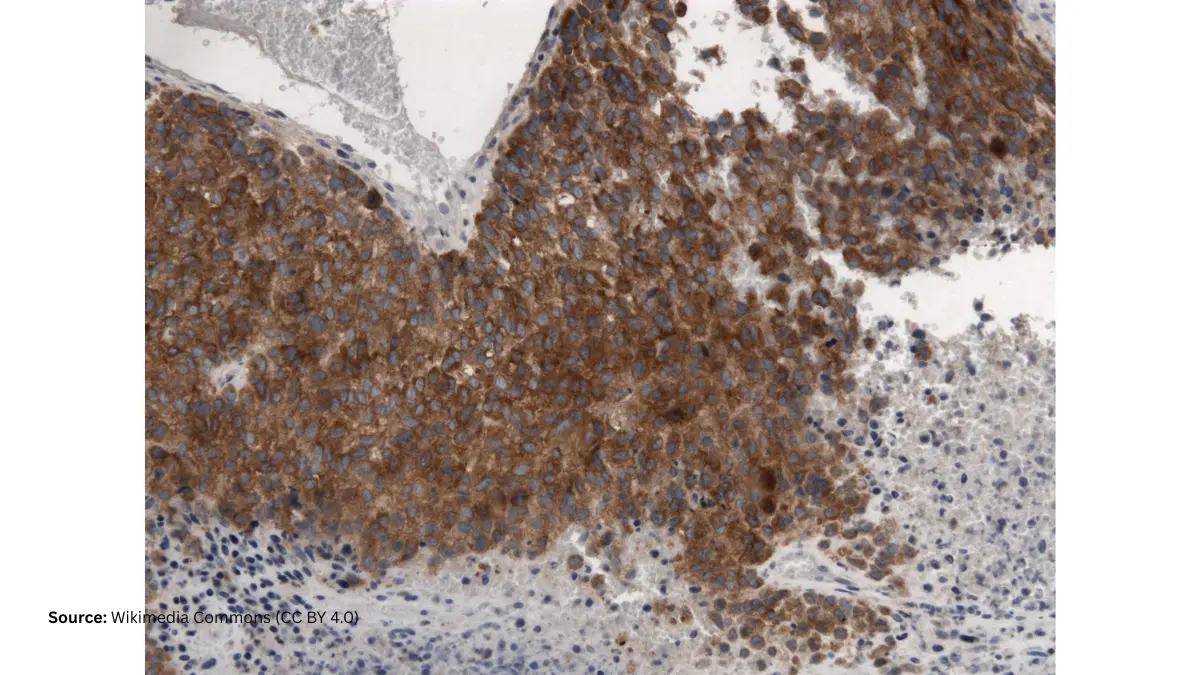
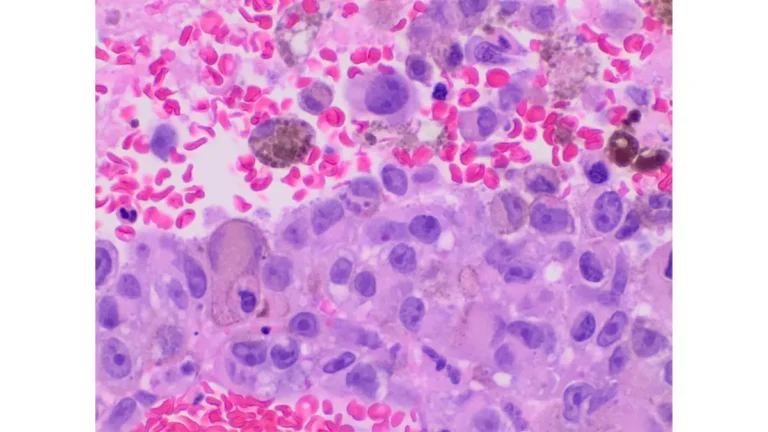
Adapted from Wikimedia Commons — BRAF V600E Mutant Melanoma, licensed under CC BY-SA 4.0.
Which Combination Performs Best?
The 2018 COLUMBUS trial showed encorafenib + binimetinib achieved a median progression-free survival of 14.9 months — the longest of the three combinations. It also causes significantly less fever and photosensitivity than older regimens.
A 2023 clinical management review published in PMC (NIH) confirms no direct head-to-head comparison exists between the three, but encorafenib + binimetinib is increasingly preferred due to its tolerability profile.
The American Cancer Society’s targeted therapy guide offers additional context on each drug’s approved indications.
How Fast Does BRAF Therapy Work?
This is one of the most searched patient questions — and most competitors skip it entirely.
- Tumor shrinkage typically begins within 4–8 weeks
- Measurable response confirmed by imaging at 3 months in most cases
- Fewer than 5% of BRAF-positive patients fail to respond at all
- Median duration of response: 12–17 months with combination therapy
Adjuvant Use After Surgery — An Overlooked Option
Dabrafenib + trametinib is also FDA-approved as adjuvant therapy for resected stage III melanoma. This means it can reduce recurrence risk even after surgery, when no visible tumor remains. For more on how melanoma is diagnosed and staged before treatment decisions are made, see our full diagnostic guide.
Who Qualifies for BRAF-Targeted Therapy? Full 2026 Eligibility Guide
Step 1 — Genetic Testing: The Gating Requirement
BRAF-targeted therapy only works if your tumor has a confirmed BRAF mutation. Your oncologist will order genetic testing from:
- A tumor biopsy (tissue sample — most common)
- A liquid biopsy (blood-based circulating tumor DNA — increasingly available in 2026)
Results typically take 5–10 business days. Understanding your melanoma blood tests and biomarkers can help you prepare better questions for your oncologist.
Use our Genetic Risk Assessment Tool to evaluate your broader hereditary cancer risk factors before your next appointment.
BRAF Positive vs. BRAF Negative — What Each Means
- BRAF Positive: Mutation confirmed → eligible for BRAF-targeted therapy
- BRAF Negative (Wild Type): No mutation → targeted therapy will not work; immunotherapy is recommended
2026 Eligibility Checklist
| Eligibility Criterion | Status |
|---|---|
| Confirmed BRAF V600E or V600K mutation | ✅ Eligible |
| BRAF negative (wild-type) tumor | ❌ Not eligible for BRAF therapy |
| Stage III melanoma (unresectable) | ✅ Eligible |
| Stage IV (metastatic) melanoma | ✅ Eligible |
| Stage I–II (early, fully resected) | 🔄 Not typically indicated |
| Prior BRAF therapy with acquired resistance | ⚠️ Specialist evaluation required |
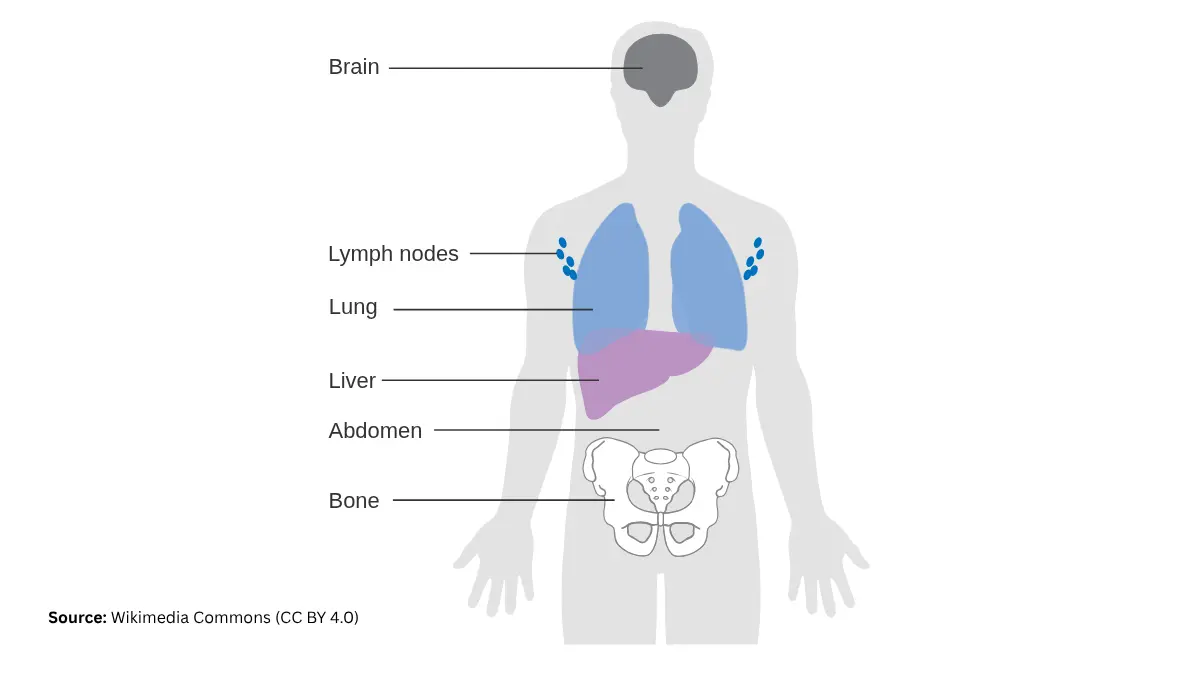
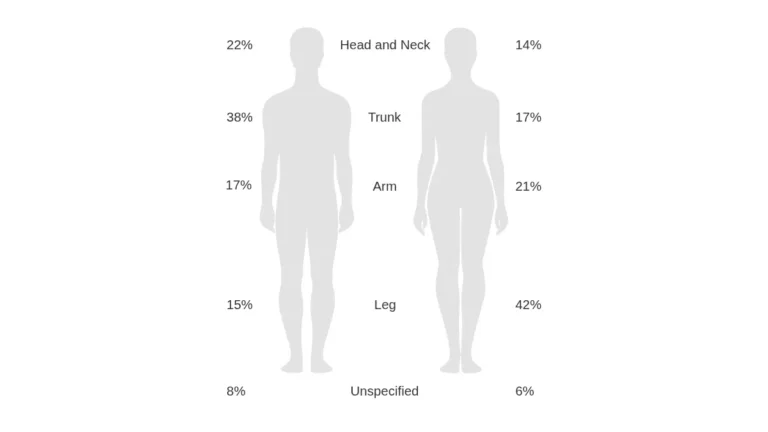
Adapted from Wikimedia Commons — Melanoma Spread Diagram (CRUK 312), licensed under CC BY-SA 4.0.
Special Cases: Rare Mutations, Brain Metastases, Elderly Patients
About 10–20% of BRAF-mutant melanomas carry the V600K mutation (vs. the more common V600E). Most approved combinations cover both. Rare non-V600 mutations (3–14% of cases) may require enrollment in clinical trials.
Patients with treated brain metastases may still qualify. Those with very high LDH levels are often considered for immunotherapy first. Knowing your melanoma stage precisely is essential before discussing eligibility with your specialist.
BRAF Therapy Side Effects — Complete Severity Guide & Management Plan
Common Side Effects (Occurring in >20% of Patients)
All BRAF-targeted therapy combinations cause side effects. Most are manageable with close monitoring — but patients must see their oncologist regularly. The NCI’s side effects management resource provides the most up-to-date clinical guidance on reporting and grading adverse events.
| Side Effect | Frequency | Severity | Management |
|---|---|---|---|
| Fatigue | Very common | Mild–Moderate | Paced activity; optimizing sleep with our Sleep Calculator can help |
| Fever / Pyrexia | Common (dabrafenib) | Moderate | Contact oncologist same day |
| Rash / Dry Skin | Common | Mild | Topical treatment; strict sun avoidance |
| Nausea / Diarrhea | Common | Mild | Dietary adjustment; stay well hydrated |
| Joint / Muscle Pain | Common | Mild–Moderate | Light activity; notify oncologist if severe |
| Secondary Squamous Cell Carcinoma | ~15–20% | Moderate | Skin checks every 8 weeks; removable surgically |
| Heart Rhythm Abnormalities | Rare | Serious | Regular ECG monitoring throughout treatment |
| Liver Enzyme Elevation | Occasional | Moderate | Monthly liver function tests |
| Vision Changes (Retinopathy) | Rare | Serious | Ophthalmology referral; dose modification |
| Photosensitivity | Common (vemurafenib combo) | Moderate | Encorafenib combo significantly reduces this risk |
Key takeaway: The encorafenib + binimetinib combination has the most favorable side effect profile in 2026 — particularly regarding fever and severe photosensitivity.
Recommended Monitoring Schedule
- Every 4 weeks: Liver function tests (LFTs), complete blood count, symptom review
- Every 8 weeks: Dermatology skin check for secondary cancers
- Every 3 months: Tumor imaging (CT/PET scan)
- Ongoing: Cardiac monitoring, ophthalmology review
Adequate hydration supports tolerability during treatment. Use our Water Intake Calculator to set personalized daily fluid goals based on your weight and activity level.
BRAF Therapy vs. Immunotherapy — The 2026 Sequencing Evidence
What the DREAMseq Trial Proved
The landmark DREAMseq trial (NCI) answered one of oncology’s most debated questions: for BRAF-positive patients, should you start with targeted therapy or immunotherapy?
The 2026 consensus answer: start with immunotherapy, in most cases.
- Immunotherapy first: 72% of patients alive at 2 years
- BRAF therapy first: 52% of patients alive at 2 years
The survival gap was so significant the trial’s safety board stopped it early. The European SECOMBIT trial independently confirmed this: immunotherapy-first delivered 64% 3-year survival vs. 53% with BRAF therapy first.
For a complete breakdown of immunotherapy options and how they compare, see our dedicated guide on immunotherapy for melanoma.
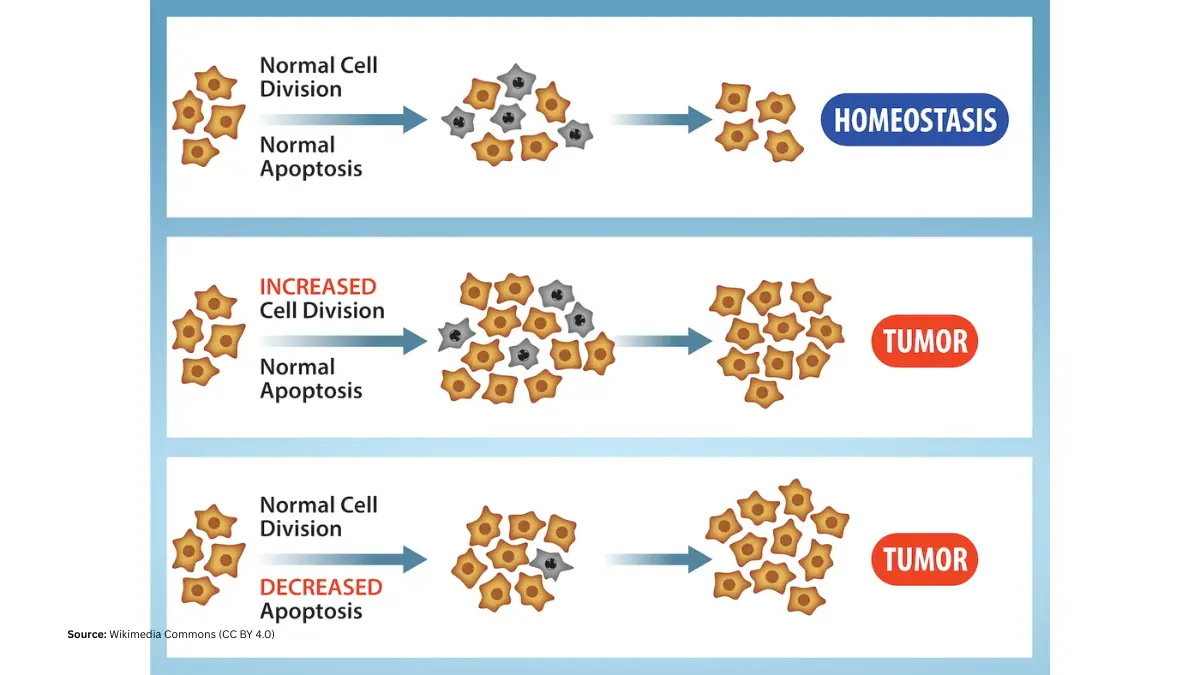
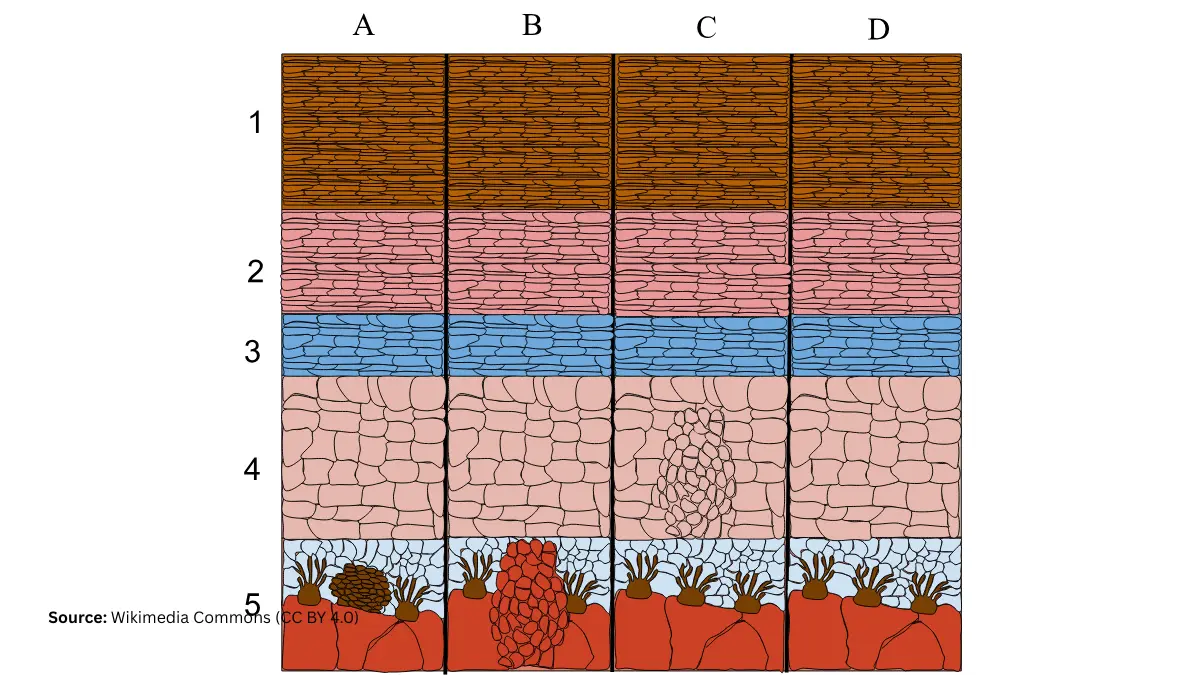
Adapted from OpenStax Biology 2e, Chapter 10.4 — Cancer and the Cell Cycle (Figure 10.15), licensed under CC BY 4.0.
When BRAF Therapy First Still Makes Sense
Immunotherapy-first is not universal. BRAF-targeted therapy remains the preferred first choice when:
- Rapid disease progression demands a fast tumor response (BRAF therapy works in weeks, not months)
- High tumor burden or elevated LDH makes immunotherapy response less predictable
- Patient cannot tolerate immune-related adverse events (autoimmune side effects)
- Rapid cytoreduction needed before or alongside brain metastasis management
The Melanoma Research Alliance’s patient-facing resource provides plain-English detail on these clinical distinctions.
2026 Sequencing Decision Framework
| Patient Situation | Recommended First-Line |
|---|---|
| Slow progression, low LDH | Immunotherapy first |
| Rapid progression, high tumor burden | BRAF-targeted therapy |
| Elderly / cannot tolerate immunotherapy | BRAF therapy often preferred |
| Brain metastases (previously treated) | Discuss both options with specialist |
| Strong desire for oral (not IV) treatment | BRAF therapy preferred |
When BRAF Therapy Stops Working: Acquired Resistance
Most patients develop resistance to BRAF-targeted therapy within 12–18 months. Cancer cells find alternative MAPK pathway escape routes. This is not a treatment failure — it is an expected biological event that your oncologist plans for from day one.
Options after resistance include:
- Switching to checkpoint immunotherapy
- Enrollment in clinical trials for triple BRAF + MEK + ERK combination regimens
- Re-challenge protocols in select cases
Understanding long-term melanoma survival rates by stage helps patients set informed expectations throughout the treatment journey.
Cost, Insurance Coverage & Emerging BRAF Treatments (2026)
How Much Does BRAF Therapy Cost in the United States?
BRAF + MEK inhibitor combinations are among the most expensive cancer drugs available. Monthly drug costs in the US typically range from $12,000 to $20,000+ without insurance. Most major commercial insurance plans and Medicare Part D cover these medications — but prior authorization is almost always required.
Patient Assistance Programs (2026)
| Program | Drug(s) Covered | How to Access |
|---|---|---|
| Novartis Patient Assistance | Tafinlar, Mekinist | novartis.com |
| Pfizer RxPathways | Zelboraf | pfizer.com |
| Array/Pfizer Oncology Support | Braftovi, Mektovi | pfizeroncolology.com |
| NeedyMeds Database | Multiple BRAF drugs | needymeds.org |
What’s Coming: Emerging BRAF Treatments in 2026
The field of BRAF-targeted therapy is advancing rapidly. Key developments this year include:
- Triple combinations (BRAF + MEK + ERK inhibitors) now in Phase II/III trials
- Next-generation BRAF inhibitors targeting rare non-V600 mutations
- BRAF therapy + immunotherapy combinations — early Phase II data is promising
- Resistance reversal agents targeting ERK5, CD73, and ALDH1A1 pathways
Browse active BRAF melanoma clinical trials at ClinicalTrials.gov to find studies you may currently be eligible for.
A 2024 landmark review in Frontiers in Oncology via PMC identifies ERK5 inhibition and CD73 targeting as the two most promising next-generation strategies for patients who develop resistance to existing BRAF-targeted therapy regimens.
Frequently Asked Questions
1. What is BRAF-targeted therapy for melanoma?
BRAF-targeted therapy uses precision oral drugs — BRAF inhibitors and MEK inhibitors — to block the mutated BRAF protein driving melanoma cell growth. It is effective only for patients whose tumors test positive for a BRAF V600 mutation.
2. Who is eligible for BRAF-targeted therapy?
Patients with stage III (unresectable) or stage IV melanoma who have a confirmed BRAF V600E or V600K mutation. Genetic testing of a tumor or blood sample is required before treatment can begin.
3. How do I know if my melanoma is BRAF positive?
Your oncologist orders a BRAF mutation test using a tumor biopsy sample or, increasingly, a liquid biopsy (blood draw). Results typically return within 5–10 business days.
4. What drugs are used in BRAF-targeted therapy for melanoma?
Three FDA-approved oral combinations: dabrafenib + trametinib, vemurafenib + cobimetinib, and encorafenib + binimetinib.
5. How fast does BRAF therapy work?
Most patients see measurable tumor shrinkage within 4–8 weeks. The overall response rate exceeds 60–70% in BRAF-positive patients receiving combination therapy.
6. What are the most common BRAF inhibitor side effects?
Fatigue, rash, fever (especially with dabrafenib regimens), nausea, joint pain, and photosensitivity. Approximately 15–20% develop secondary squamous cell skin cancers, which are typically treated by surgical removal.
7. Is BRAF therapy better than immunotherapy for melanoma?
For most BRAF-positive patients in 2026, immunotherapy first delivers better long-term survival (72% vs. 52% at 2 years, per DREAMseq). BRAF therapy first is preferred for rapidly progressing disease.
8. What happens when BRAF therapy stops working?
Most patients develop acquired resistance within 12–18 months. Options include switching to immunotherapy, enrolling in clinical trials, or exploring triple-combination regimens.
9. Can BRAF therapy be used after surgery (adjuvant)?
Yes. Dabrafenib + trametinib is FDA-approved as adjuvant therapy for resected stage III melanoma to reduce recurrence risk.
10. How long is BRAF-targeted therapy taken?
There is no fixed duration. Treatment continues until disease progression, unacceptable toxicity, or a clinical decision to transition to another modality.
11. Is a BRAF mutation inherited from parents?
No. BRAF mutations in melanoma are somatic — they occur only in tumor cells and are not passed down through families. They are not related to inherited hereditary cancer syndromes.
⚕️ Medical Disclaimer: This content is for educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. All drug data reflects FDA-approved indications and peer-reviewed clinical evidence as of April 2026. Consult a board-certified oncologist for individual guidance.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.