On This Page – Quick Medical Summary
One blistering sunburn before age 18 doubles your lifetime melanoma risk. By 2026, melanoma accounts for over 100,000 new U.S. diagnoses annually — and the majority are directly linked to UV-induced DNA damage from sunburns. This article tells you exactly what that means for your skin, your health, and your future.
The Alarming Truth About Sunburn and Melanoma Risk
Marcus, a 34-year-old construction supervisor from Phoenix, Arizona, had no family history of skin cancer. What he did have were three blistering sunburns before the age of 16 — the kind where skin swells, bubbles, and peels away in sheets. At 31, a routine dermatology visit revealed a Stage II melanoma on his left shoulder. His dermatologist’s words stopped him cold: “Those childhood burns were almost certainly contributing factors.”
Marcus’s story is not rare. It is increasingly common.
According to the American Cancer Society, people who have had five or more blistering sunburns in their lifetime face an 80% higher melanoma risk compared to those who have never blistered. That figure is not theoretical — it is drawn from decades of epidemiological data tracking real patients.
2026 Global Snapshot
| Country | New Melanoma Cases (Est. 2026) | Trend |
|---|---|---|
| United States | ~106,000 | ↑ 3% YoY |
| Australia | ~18,000 | ↑ 2% YoY |
| United Kingdom | ~17,500 | ↑ 4% YoY |
| Canada | ~9,800 | ↑ 2.5% YoY |
Melanoma is the 5th most common cancer in the United States. It is also among the most preventable — because its primary driver, UV radiation from sunburn, is within your control.
What makes sunburn melanoma risk so dangerous is the delay. You may have burned at 14 and not develop melanoma until your 40s. This latency period fools people into thinking old sunburns no longer matter. They do.
If you’re concerned about your personal cancer risk factors, our Genetic Risk Assessment Tool can help you understand inherited vulnerabilities alongside environmental triggers like UV exposure.
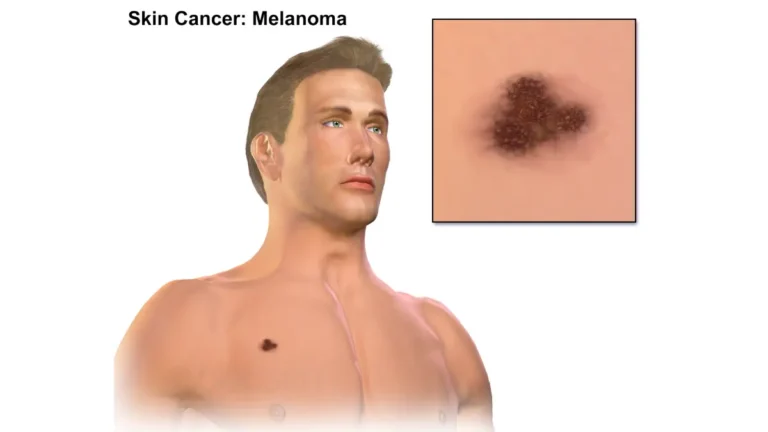
How Sunburn Actually Creates Melanoma Risk — The Science
Understanding why a sunburn raises your melanoma risk requires understanding what UV radiation does inside your skin cells.
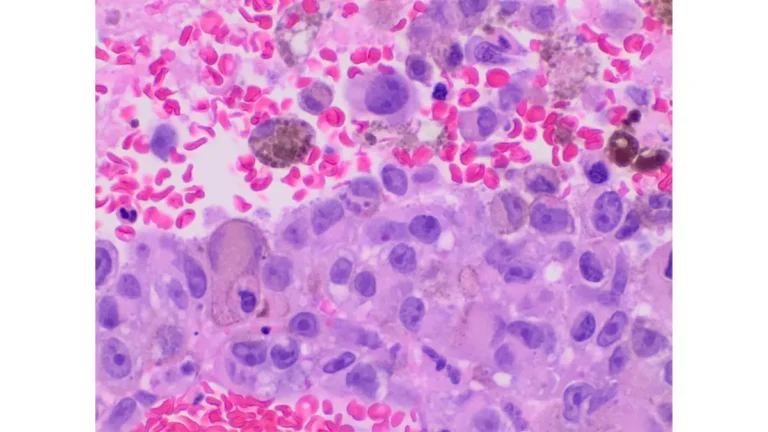
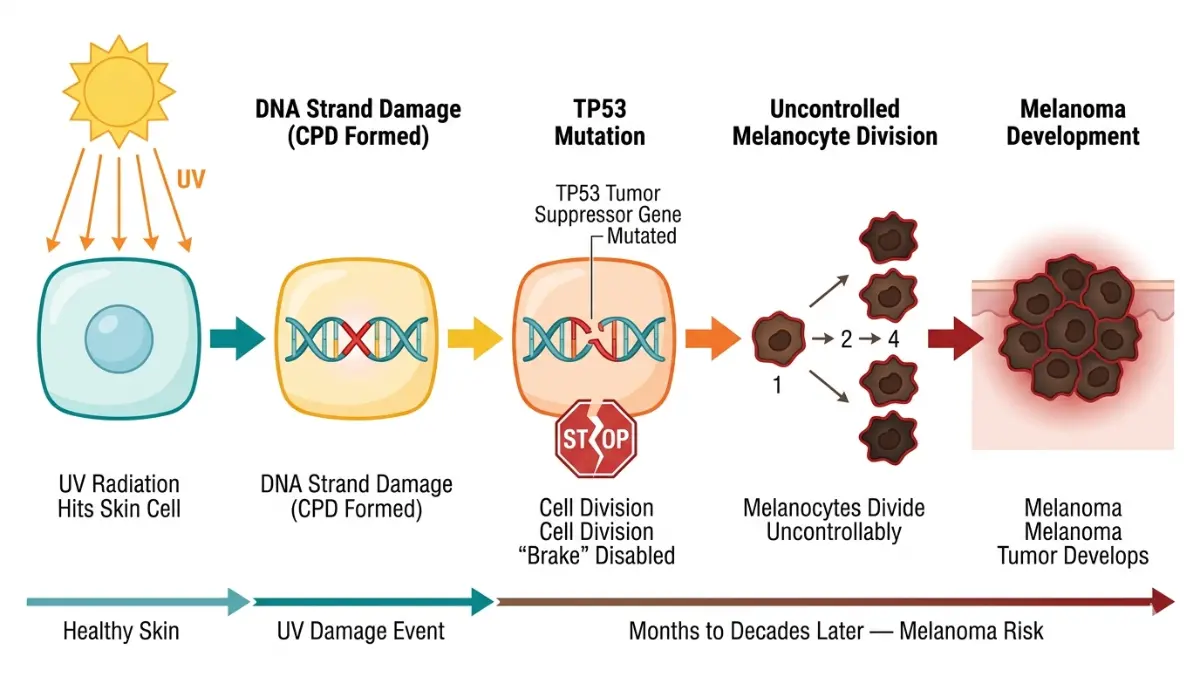
The DNA Damage Cascade
Within 15 minutes of unprotected UV exposure, ultraviolet radiation begins damaging the DNA inside your skin cells. Specifically, it creates abnormal bonds between adjacent DNA bases called cyclobutane pyrimidine dimers (CPDs). These are essentially kinks in your DNA strand that, if not repaired correctly, become permanent mutations.
Your body has repair mechanisms — but they aren’t perfect. When UV exposure is intense (a blistering burn), the volume of damage overwhelms the repair systems. Mutations accumulate in the TP53 tumor suppressor gene, the gene responsible for halting abnormal cell growth. Once this “brake” is broken, abnormal melanocytes — the pigment-producing cells — can begin dividing uncontrollably.
This process is called photocarcinogenesis, and it is the direct biological bridge between your sunburn and melanoma risk. As documented by the National Cancer Institute, UV radiation is classified as a Group 1 carcinogen — the highest possible risk classification.
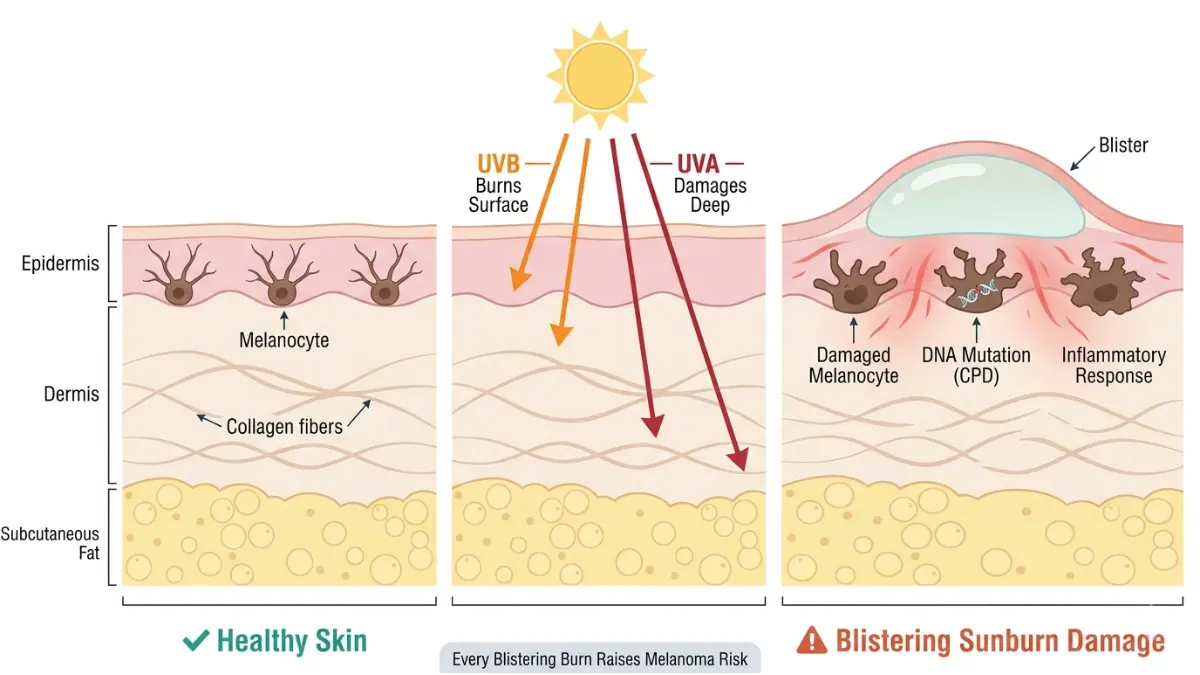
Why Blistering Burns Are Categorically Different
Not all sunburns carry equal melanoma risk. A blistering burn represents epidermal destruction — the outer skin layer is so severely damaged that fluid-filled blisters form as an emergency inflammatory response.
At this level of damage:
- Melanocytes experience direct trauma, not just surface DNA damage
- The dermal-epidermal junction is disrupted, creating unstable cellular environments
- Inflammatory cytokines flood the area, suppressing local immune surveillance
UVA vs. UVB — both matter:
- UVB (shorter wavelength) causes visible burning and direct DNA strand breaks
- UVA (longer wavelength) penetrates deeper, oxidizes DNA indirectly, and ages skin at the cellular level
Both wavelengths contribute to sunburn melanoma risk. Tanning beds emit both — which is why tanning bed use dramatically elevates melanoma risk, particularly when started before age 35.
Cumulative vs. Single-Event Risk
| Blistering Burn Count | Lifetime Melanoma Risk Multiplier |
|---|---|
| 0 blistering burns | Baseline (1×) |
| 1–2 blistering burns | ~1.5–2× |
| 3–4 blistering burns | ~2.5–3× |
| 5+ blistering burns | ~4–5× (up to 80% higher) |
Source: American Cancer Society, Epidemiology Research 2024
The cumulative model is critical. Every blistering sunburn adds to your total mutation load — the lifetime accumulation of DNA errors that eventually tips toward malignancy. This is why understanding what causes melanoma goes far beyond a single bad beach day.
Your Personal Sunburn Melanoma Risk Profile
Not every person who blisters develops melanoma. Your individual risk depends on a combination of genetic, environmental, and behavioral factors.
The 9 Major Risk Amplifiers
- Fair skin (Fitzpatrick Type I or II — always burns, rarely tans)
- History of 2+ blistering sunburns, especially before age 20
- More than 50 moles on the body
- Family history of melanoma in a first-degree relative — melanoma has a significant hereditary component
- Tanning bed use before age 35
- Living at high altitude or low latitude (closer to the equator or higher elevation = more UV)
- Immunosuppression (organ transplant recipients, HIV, long-term steroid use)
- Outdoor occupation (farmers, construction workers, lifeguards)
- Prior history of any skin cancer
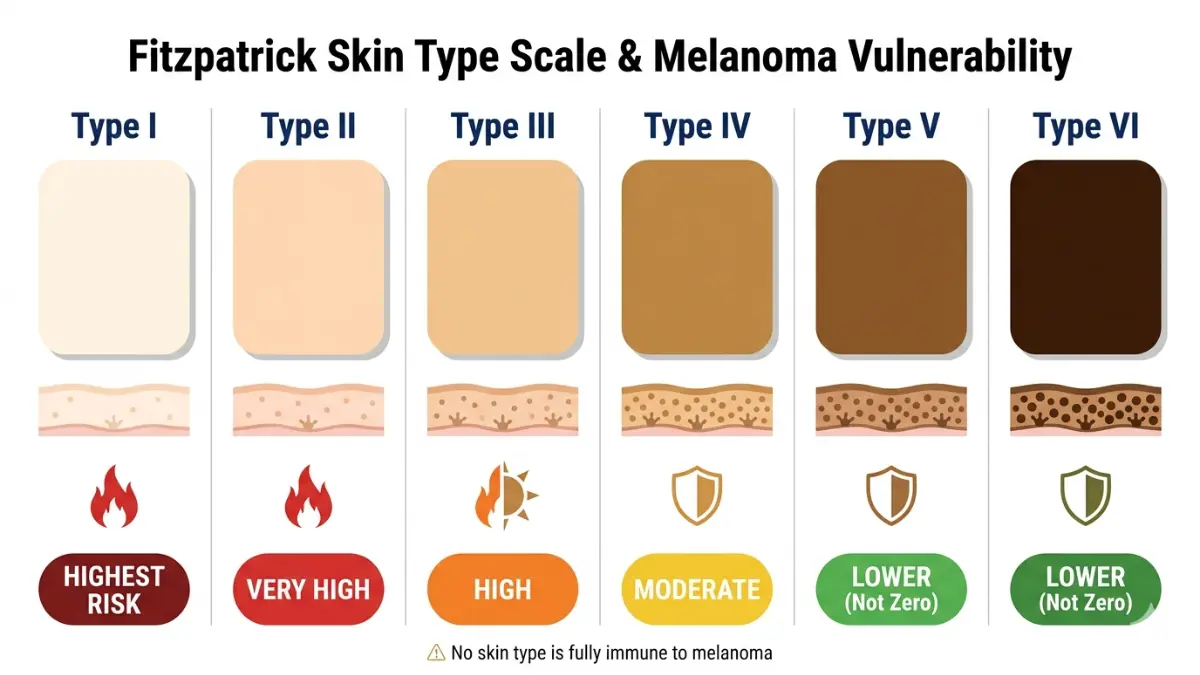
Fitzpatrick Skin Type and Melanoma Vulnerability
| Fitzpatrick Type | Description | Burns Easily? | Melanoma Risk |
|---|---|---|---|
| Type I | Very fair, freckled | Always burns | Highest |
| Type II | Fair, light hair/eyes | Usually burns | Very High |
| Type III | Medium, occasionally burns | Burns moderately | High |
| Type IV | Olive skin | Rarely burns | Moderate |
| Type V–VI | Brown to dark skin | Almost never burns | Lower (not zero) |
Important: Dark-skinned individuals are not immune to sunburn melanoma risk. Melanoma in people with Type V–VI skin is often diagnosed later at more advanced stages because awareness is lower — making education critical across all skin tones.
Childhood Sunburns: A Special Category of Danger
Research published in peer-reviewed dermatology literature consistently shows that blistering burns sustained before age 20 carry disproportionately higher melanoma risk than equivalent burns in adulthood. This is because:
- Developing skin has more rapidly dividing cells (higher mutation vulnerability)
- Decades of latency remain ahead for mutations to accumulate
- Immune surveillance in children has not yet fully matured
For parents: A child’s single severe blistering sunburn is a serious medical event. Prevent it with the same urgency you would any other injury.
If you’ve noticed a changing mole or new skin lesion after years of sun exposure, use our Symptom Checker as an initial assessment step before scheduling your dermatologist consultation.
Warning Signs — When a Sunburn Scar Becomes a Melanoma Red Flag
Recognizing melanoma early is the single most powerful factor in survival. A Stage I melanoma has a ~97% five-year survival rate. Stage IV drops below 30%.
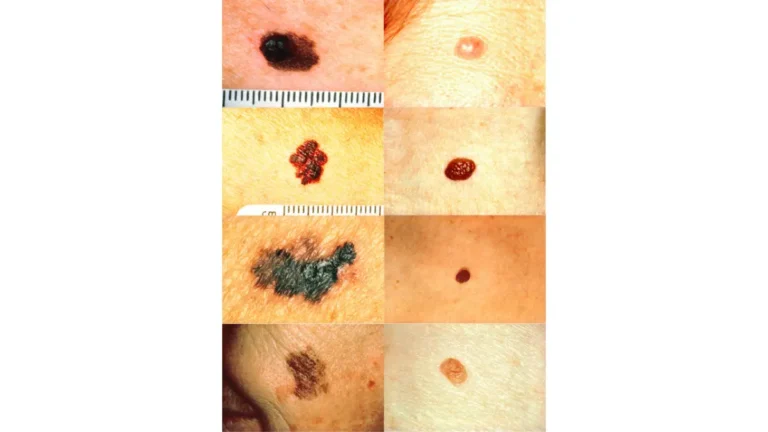
The ABCDE Rule — Updated 2026 Clinical Criteria
Dermatologists worldwide use the ABCDE framework to assess suspicious lesions. Memorize this — it could save your life:
| Letter | Stands For | What to Look For |
|---|---|---|
| A | Asymmetry | One half doesn’t match the other |
| B | Border | Irregular, ragged, notched, or blurred edges |
| C | Color | Multiple shades — tan, brown, black, red, or white within one lesion |
| D | Diameter | Larger than 6mm (the size of a pencil eraser) |
| E | Evolving | ANY change in size, shape, color, or new bleeding/itching/crusting |
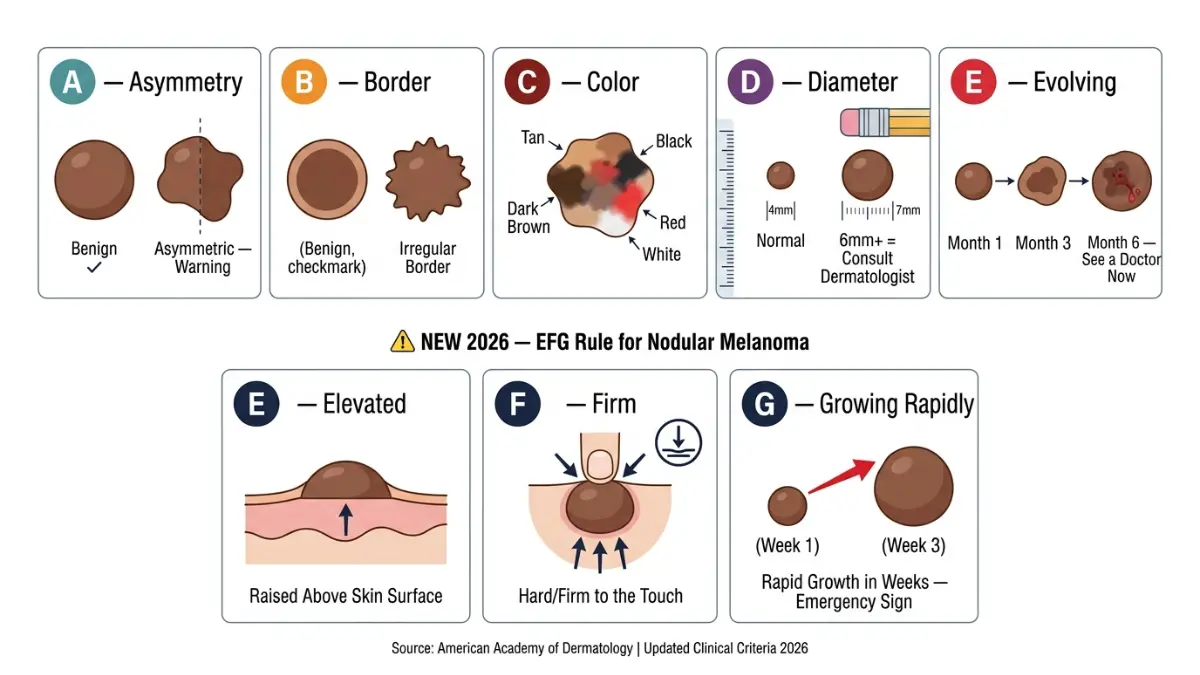
2026 Addition — The EFG Rule (for nodular melanoma, the fastest-growing type):
- E — Elevated (raised above surrounding skin)
- F — Firm to the touch
- G — Growing rapidly (over weeks, not months)
For a visual guide to the full ABCDE warning system, see our dedicated guide on melanoma warning signs and ABCDE mole checks.
How Long After a Sunburn Can Melanoma Develop?
This is one of the most-asked questions — and one of the most misunderstood.
There is no fixed timeline. The latency period between UV-induced DNA damage and the emergence of detectable melanoma can range from months to decades. This explains why:
- A 45-year-old may develop melanoma from burns sustained at age 12
- A 28-year-old may develop melanoma after repeated tanning bed use in their early 20s
| Time After Sun Damage | What You May Notice | Recommended Action |
|---|---|---|
| Days 1–7 | Redness, blistering, peeling | Cool compresses, hydration, monitor |
| Weeks 2–6 | Post-inflammatory darkening | Normal — watch for ABCDE changes |
| 3–12 months | New or changing mole | Dermatologist consult — don’t wait |
| Years to decades | Melanoma may emerge | Annual full-body skin exam, every year |
As outlined in comprehensive melanoma warning signs and symptom guides, new lesions appearing on previously sun-damaged skin deserve immediate professional evaluation — not watchful waiting.
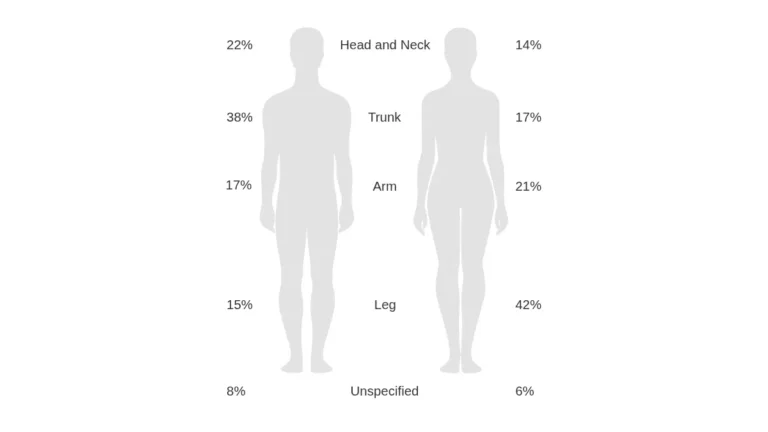
According to the Mayo Clinic’s melanoma resource, melanoma can develop anywhere on the body — including areas that have never been directly sun-exposed, though UV damage significantly raises risk on exposed sites.
The CDC’s skin cancer data reinforces that early detection through regular self-examination and professional screening remains the most effective intervention available today.
Evidence-Based Protection — How to Break the Sunburn-to-Melanoma Cycle
Prevention is not complicated. It is, however, non-negotiable for anyone serious about reducing their sunburn melanoma risk.
The Sunscreen Truth — SPF Numbers Decoded
Most Americans significantly misunderstand SPF values:
| SPF Level | UVB Rays Blocked | UVA Protection | Reapplication Needed? |
|---|---|---|---|
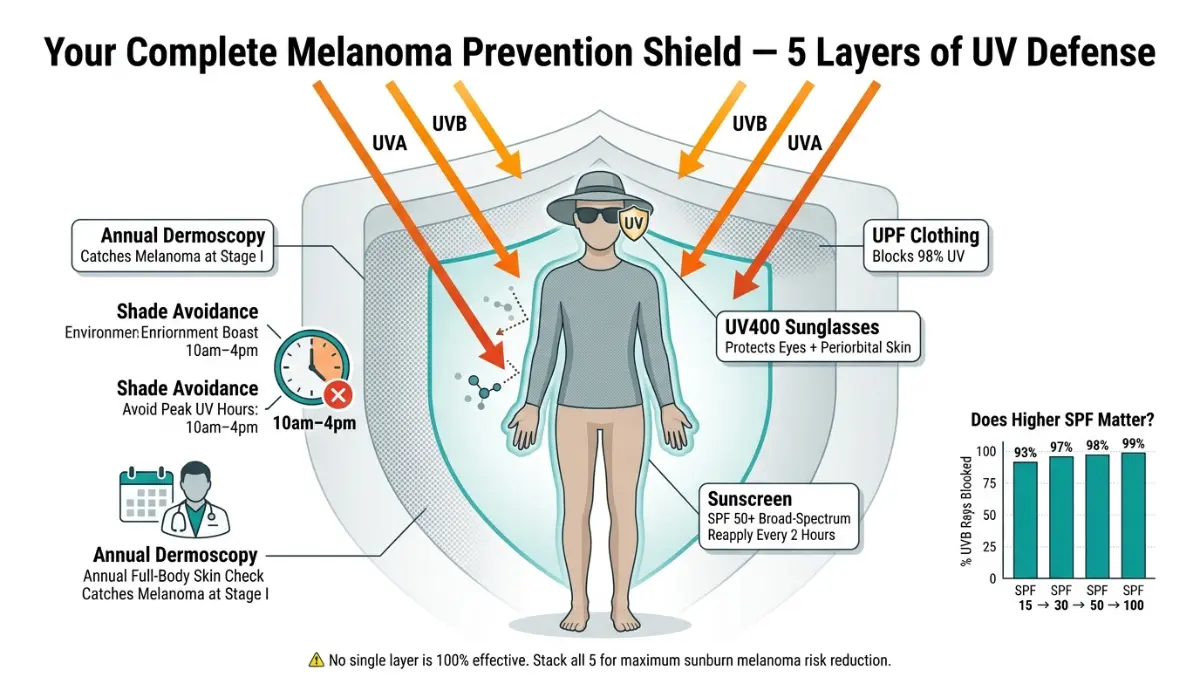
| SPF 15 | 93% | Partial (if broad-spectrum) | Every 2 hours |
| SPF 30 | 97% | Partial (if broad-spectrum) | Every 2 hours |
| SPF 50 | 98% | Good (if broad-spectrum) | Every 2 hours |
| SPF 100 | 99% | Good (if broad-spectrum) | Every 2 hours |
Key rules:
- Always choose broad-spectrum (protects against both UVA and UVB)
- Apply 1 ounce (shot glass amount) for full-body coverage
- Reapply every 2 hours outdoors — or immediately after swimming or sweating
- Mineral sunscreens (zinc oxide, titanium dioxide) sit on top of skin and block physically; chemical sunscreens absorb UV and convert it to heat — both are effective when applied correctly
The Full UV Protection Protocol
- ☀️ Avoid peak UV hours: 10am–4pm — UV index is highest during this window
- 👕 UPF 50+ clothing provides more reliable coverage than sunscreen alone
- 🕶️ UV-blocking sunglasses protect against ocular melanoma and periorbital skin damage
- 🌳 Seek shade actively — don’t rely on cloud cover; UV penetrates overcast skies
- 🔁 Reapply sunscreen even on cloudy days and even after light physical activity
After any sun exposure, hydrating properly is essential for skin repair. Dehydration slows cellular recovery — use our Water Intake Calculator to ensure you’re meeting your daily hydration needs.
Emerging Photoprotection: 2026 Evidence Updates
Three evidence-backed additions to your prevention toolkit:
1. Nicotinamide (Vitamin B3) A landmark study supported by the National Cancer Institute’s melanoma prevention research found that oral nicotinamide (500mg twice daily) reduced new non-melanoma skin cancers by 23% in high-risk patients. Emerging evidence suggests benefits for melanoma prevention too.
2. Polypodium leucotomos extract A fern-derived oral antioxidant shown in multiple trials to reduce UV-induced erythema and oxidative DNA damage. Not a sunscreen replacement — a complement.
3. Topical DNA repair enzymes T4N5 liposome-based topical lotions are FDA-cleared for high-risk patients. They introduce bacterial DNA repair enzymes (photolyase) directly into sun-damaged skin post-exposure.
The World Health Organization’s ultraviolet radiation guidance classifies UV as a Group 1 carcinogen and recommends a multi-layer approach to photoprotection — consistent with the protocol outlined above.
For comprehensive skin health guidance, explore our Health Tips resource hub — covering everything from sun protection to dermatology-grade skincare.
From Diagnosis to Survival — What Happens If Melanoma Is Found
If a suspicious lesion is identified, early and accurate diagnosis is everything.
Diagnostic Tools in 2026
- Dermoscopy: Magnified, polarized light examination of pigmented lesions — the first-line tool
- Reflectance confocal microscopy (RCM): Non-invasive cellular-level imaging
- AI-assisted dermatoscopy: FDA-cleared algorithms now match or exceed expert dermatologist accuracy in controlled trials
- Excisional biopsy: The gold standard — lesion is surgically removed and pathologically analyzed
- Sentinel lymph node biopsy: Determines if melanoma has begun spreading regionally
Melanoma Staging and Survival Rates (2026 Data)
| Stage | Description | 5-Year Survival Rate |
|---|---|---|
| Stage 0 (In situ) | Confined entirely to epidermis | ~99% |
| Stage I | Thin tumor, no spread | 92–98% |
| Stage II | Thicker tumor, no lymph node spread | 65–85% |
| Stage III | Spread to regional lymph nodes | 40–78% |
| Stage IV | Distant metastasis (organs, brain) | 15–30% |
Source: American Cancer Society SEER Database, 2025–2026
Treatment Advances in 2026
Immunotherapy has transformed melanoma treatment. Checkpoint inhibitors — particularly pembrolizumab (Keytruda) and nivolumab (Opdivo) — have produced durable remissions in Stage III–IV patients previously considered untreatable. As detailed in our guide to melanoma symptoms, stages, and treatment options, the landscape has shifted dramatically since 2018.
Targeted therapy (BRAF + MEK inhibitor combinations like dabrafenib/trametinib) is effective for the ~50% of melanomas carrying BRAF V600E mutations.
CAR-T cell therapy for melanoma is currently in Phase II trials, with early results showing promise for treatment-resistant Stage IV cases.
The American Academy of Dermatology’s melanoma patient guide recommends annual full-body skin exams for any adult with a history of blistering sunburns — a recommendation our advisory board fully endorses.
For a complete picture of your skin cancer risk beyond melanoma, our skin cancer warning signs guide covers all major subtypes including basal cell and squamous cell carcinoma.
🔑 Final Thought: Melanoma caught at Stage I is nearly always curable. Every sunburn you prevent today is a melanoma you may never have to fight. Your skin remembers every burn. Make sure your future self doesn’t have to.
Frequently Asked Questions
1. Does one blistering sunburn cause melanoma?
A single blistering sunburn significantly raises your risk — doubling it if it occurs before age 18. It doesn’t guarantee melanoma, but it creates real, measurable biological vulnerability.
2. How many sunburns does it take to get melanoma?
Research shows five or more lifetime blistering sunburns raises melanoma risk by up to 80%. However, even one severe burn in childhood is clinically significant.
3. Can you get melanoma years after a sunburn?
Yes. The latency period between UV damage and diagnosable melanoma is often 10–30 years. Burns you had as a teenager can cause melanoma in your 40s or 50s.
4. Is peeling after sunburn a sign of cancer?
Peeling itself is normal — it is your body shedding UV-damaged cells. However, monitor the area over the following months for any ABCDE changes in moles or new lesions.
5. What does early melanoma look like after sun damage?
Early melanoma often appears as a flat, asymmetric spot with irregular borders and multiple colors. It may evolve from an existing mole or appear as a brand-new lesion.
6. Does sunscreen prevent melanoma risk from sunburns?
Broad-spectrum SPF 30+ applied correctly and reapplied every 2 hours significantly reduces sunburn melanoma risk. No sunscreen offers 100% protection — layered protection is essential.
7. Are childhood sunburns more dangerous for melanoma?
Yes. Burns before age 20 carry disproportionately higher risk due to rapidly dividing cells, longer latency window, and developing immune systems.
8. Can dark-skinned people get melanoma from sunburns?
Yes. Fitzpatrick Type V–VI individuals have lower — but not zero — sunburn melanoma risk. They are often diagnosed at more advanced stages due to lower awareness.
9. How long after sun exposure can melanoma develop?
Anywhere from several months to several decades. Consistent annual skin checks are the only reliable way to catch it early regardless of how long ago the sun damage occurred.
10. What is the difference between sunburn and early melanoma?
Sunburn resolves within 1–2 weeks. Melanoma is a persistent, evolving lesion that does not fade. Any spot that changes over weeks or months — rather than healing — warrants urgent dermatological evaluation.
11. Should I see a doctor after every severe sunburn?
After a severe blistering sunburn, monitor the affected area closely for 6–12 months. Book a full-body skin check with a dermatologist annually if you have had multiple blistering burns or other risk factors.
🔗 Related Reading from mymedicineadvisor.com
- What Causes Melanoma? Full Risk Factor Guide
- Is Melanoma Hereditary? Genetic Risk Explained
- Melanoma Statistics 2026: U.S. and Global Data
- Tanning Beds and Melanoma Risk
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.