On This Page – Quick Medical Summary
Can you actually prevent lung cancer from developing?
Your clinical profile determines where to start. If you are a current or former smoker evaluating your risk, Section 3 and Section 5 address you directly. If you want to know whether you qualify for annual lung cancer screening, go to Section 4. If you have never smoked but work in a high-exposure industry or have a recently diagnosed family member, start with Section 6 and Section 3. If you are a caregiver, Section 7 is written for you.
In my oncology practice, the question patients ask before any treatment conversation is: Could this have been prevented? The clinical answer is that lung cancer prevention operates on two parallel tracks — primary prevention through carcinogen exposure reduction, and secondary prevention through early detection. Understanding what lung cancer is and how it develops at the cellular level clarifies why each strategy below targets a different point in that process.
If you have noticed unexplained changes in your breathing, persistent cough, or energy levels alongside any of the risk factors discussed here, use our symptom checker to evaluate what you are experiencing before reading further.
ℹ️ Medical Disclaimer: The diagnostic criteria, screening eligibility thresholds, treatment options, smoking cessation medications, radon action thresholds, and insurance coverage information discussed in this article reflect current clinical guidelines and are provided for educational purposes only. Individual screening eligibility determinations, treatment decisions, and medication choices depend on factors including patient history, comorbidities, prior exposures, and specialist assessment. Consult a board-certified oncologist, pulmonologist, or internal medicine physician before acting on any clinical information in this article. This article does not constitute a medical diagnosis, a prescription recommendation, or a coverage determination for any individual patient.
What actually reduces your lung cancer risk, according to the evidence
The most clinically validated strategies to prevent lung cancer, ranked by strength of evidence, are:
- Smoking cessation — the single highest-impact intervention, with risk reduction beginning within years of quitting and continuing for more than a decade post-cessation
- Annual low-dose CT (LDCT) screening for eligible adults — the only imaging approach proven to reduce lung cancer mortality in high-risk populations in randomized clinical trial data
- Home radon testing and mitigation — the second-leading cause of lung cancer operates silently in millions of US households and is directly addressable
- Occupational carcinogen reduction — respiratory protective equipment, NIOSH-compliant controls, and surveillance for workers in asbestos, silica, and diesel exhaust environments
- Sustained air quality management — limiting prolonged PM2.5 exposure and ensuring adequate indoor kitchen ventilation
Physical activity and plant-forward dietary patterns show modestly protective associations in observational data. They support pulmonary health — but they do not substitute for the top three interventions above.
📊 Clinical Data Point: Cigarette smoking is the leading attributable cause of lung cancer in the United States — responsible for the substantial majority of all diagnoses. Source: National Cancer Institute, 2026 — verify the current attributable fraction against the NCI lung cancer prevention patient guide at publish time. (Flag: confirm 2026-specific figure at publish)
To combine prevention with awareness of early changes, review early warning signs of lung cancer — prevention and symptom recognition reinforce each other before a diagnosis occurs. (Editor: insert confirmed cluster URL)
What puts you at highest risk for lung cancer — and how much each factor matters
Risk for lung cancer compounds across multiple simultaneous exposures — and understanding the hierarchy determines which prevention actions are most urgent for your specific profile.
How your smoking history determines your risk level
Pack-year history is the primary clinical tool for quantifying tobacco exposure: packs smoked per day multiplied by years smoked. One pack per day for 20 years equals 20 pack-years — as does two packs per day for 10 years. This calculation matters directly for LDCT screening eligibility, which Section 4 covers in full.
Current smokers carry the highest absolute risk. Former smokers who quit retain an elevated risk for more than a decade post-cessation — which is why USPSTF criteria extend LDCT eligibility to anyone who quit within the past 15 years.
The non-smoking risk factors most patients overlook
Radon gas is the second-leading cause of lung cancer in the United States, responsible for a meaningful share of annual diagnoses — particularly among lifetime non-smokers. Secondhand smoke contains more than 70 documented carcinogens and elevates lung cancer risk in household and workplace contacts who have never smoked. IARC Group 1 occupational lung carcinogens include asbestos (both chrysotile and amphibole fiber types), diesel exhaust particulates, crystalline silica, arsenic compounds, and beryllium — all confirmed human lung carcinogens in working populations.
🔬 How It Works: Radon gas decays into radioactive particles that emit alpha radiation directly inside the airway cells lining the lungs. Unlike tobacco carcinogens — which require metabolic activation by liver enzymes before damaging DNA — radon decay products cause immediate double-strand DNA breaks on cellular contact. This is why radon and active smoking together are a particularly dangerous combination: two independent carcinogenic mechanisms operating on the same tissue simultaneously.
Does family history or genetics increase your risk?
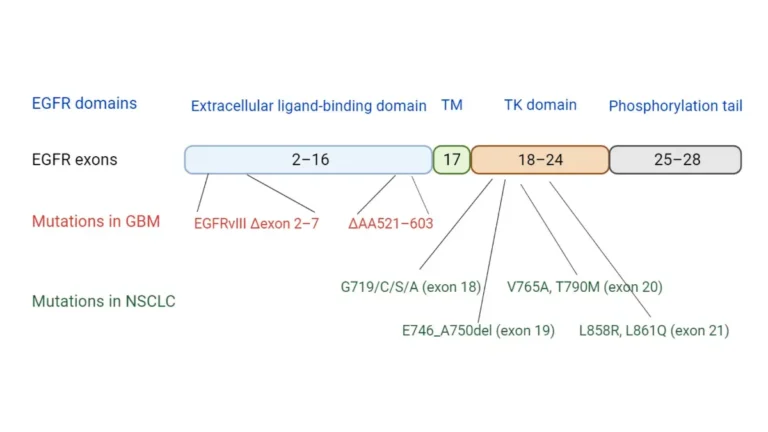
Most familial clustering of lung cancer reflects shared environmental exposures — household smoking and radon levels — rather than true Mendelian inheritance. A small subset of never-smokers carries germline variants in carcinogen metabolism genes (including CYP1A1 and GSTM1 polymorphisms) that modestly elevate susceptibility. EGFR mutations are commonly identified in lung tumor tissue, particularly in adenocarcinoma among never-smoking women — but these are typically acquired somatic mutations, not inherited germline variants.
Use our genetic risk assessment tool to map your personal risk factors before your next appointment.
✅ Patient Action: If you have worked in asbestos insulation, shipbuilding, underground mining, demolition, or foundry operations for five or more cumulative years, ask a board-certified occupational medicine physician: “Based on my cumulative exposure history, do I qualify for enhanced lung cancer surveillance beyond standard USPSTF screening criteria?”
Do you qualify for lung cancer screening — and how do you get it covered?
Annual LDCT screening is the most powerful secondary prevention tool for high-risk adults — and the section most patients who quit smoking in the past decade need most urgently.
The USPSTF criteria that determine whether you qualify
| Eligibility Criterion | Qualifying Threshold | Insurance Coverage Standard | Your Next Step |
|---|---|---|---|
| Age | 50 to 80 years | ACA-compliant plans: covered without cost-sharing | Confirm your age falls within this range |
| Pack-year history | 20 or more pack-years | Same | Calculate: (packs/day) × (years smoked) |
| Smoking status | Currently smoking OR quit within the past 15 years | Same | Confirm your quit date if applicable |
| All three criteria met | Proceed to referral | Medicare: verify 2026 CMS coverage status at publish | Request LDCT referral from your PCP |
📊 Clinical Data Point: The USPSTF recommends annual low-dose CT screening for qualifying adults as a Grade B preventive recommendation. Source: U.S. Preventive Services Task Force — verify the current USPSTF lung cancer screening recommendation at publish time. (Flag: confirm whether the 2021 recommendation has been updated in a 2026 statement before citing eligibility thresholds)
What low-dose CT screening actually involves
LDCT uses approximately one-fifth of the radiation dose of a standard diagnostic chest CT — roughly equivalent to the background radiation exposure of a transcontinental flight. The scan takes under 10 minutes, requires only a brief breath-hold, involves no intravenous contrast, and carries no recovery period.
🩺 Physician Note: The single most common barrier I encounter to LDCT access is not insurance — it is the belief that quitting smoking “reset” a patient’s screening eligibility. It did not. Current USPSTF criteria explicitly include anyone who quit within the past 15 years and meets the age and pack-year thresholds. I have had patients who quit 11 years earlier walk into my office certain they no longer qualified. If you quit between one and fifteen years ago and are between 50 and 80, this appointment conversation is not optional.
How to get your first screening appointment scheduled
- Calculate your pack-year history — (packs per day) × (years smoked) = your pack-year total
- Confirm all three eligibility criteria — age 50–80, 20+ pack-years, currently smoking or quit within 15 years
- Request an LDCT referral from your primary care physician — bring your calculated pack-year total to the appointment
- Verify your insurance coverage — ACA-compliant plans must cover qualifying adults without cost-sharing; confirm your plan’s specific prior authorization process
- Schedule at an ACR-accredited lung cancer screening center — accreditation ensures the facility follows established nodule management protocols
✅ Patient Action: Before your next PCP appointment, calculate your pack-year total: packs smoked per day multiplied by years smoked. Bring that number and ask specifically: “Based on my pack-year history, age, and quit date, do I qualify for annual LDCT screening covered without cost-sharing by my insurance plan?” That single question, answered correctly, is the clinical gateway to this intervention.
If you meet eligibility criteria, review what to expect from a lung cancer screening appointment before you schedule. (Editor: insert confirmed cluster URL)
How quitting smoking changes your lung cancer risk — and what the evidence shows
Quitting smoking is the highest-impact single action available to prevent lung cancer — at any age, after any number of years of tobacco use.

How quickly does lung cancer risk drop after quitting?
Smoking cessation begins reducing lung cancer risk within the first years after the final cigarette. Risk continues declining over the following decade, approaching — but not fully reaching — a lifetime never-smoker’s baseline after 15 or more years of abstinence. This progressive risk reduction is the clinical basis for the USPSTF’s 15-year quit window in LDCT screening eligibility criteria.
Two facts must be held simultaneously: quitting is never too late to produce meaningful risk reduction, and cessation does not immediately eliminate LDCT screening eligibility for those who meet the criteria. These are complementary truths, not contradictory ones.
📊 Clinical Data Point: Smoking cessation progressively reduces lung cancer risk in the years following quitting. Source: CDC tobacco surveillance data, 2026 — verify the current CDC evidence base for cessation and lung cancer risk reduction at publish time. (Flag: confirm 2026 CDC cessation risk-reduction data before citing any specific percentage)
Which cessation treatments have the strongest clinical evidence?
Varenicline (Chantix — also available in generic form) is an FDA-approved partial agonist at the α4β2 nicotinic acetylcholine receptor. It reduces nicotine withdrawal symptoms while simultaneously blocking the reward response from continued smoking. Randomized controlled trial data consistently identify varenicline as achieving the highest 12-week continuous abstinence rates among single-agent cessation pharmacotherapy options. Bupropion SR (Wellbutrin SR) is the second FDA-approved oral cessation medication, acting through dopaminergic and noradrenergic modulation. Nicotine replacement therapy (NRT) — available over the counter in patch, gum, and lozenge forms — can be combined with varenicline or bupropion for enhanced efficacy in patients who have failed monotherapy.
⚠️ Clinical Warning: Varenicline requires a physician prescription and a full medication review before starting. Verify the current 2026 FDA prescribing label for varenicline at publish time — labeling requirements, including any neuropsychiatric monitoring guidance, can be updated by the FDA between article review cycles. Do not characterize current labeling requirements from any pre-2026 source.
✅ Patient Action: At your cessation consultation, ask your physician: “Of varenicline, bupropion, and combination NRT, which has the strongest evidence for my specific history — and are there contraindications given my current medications and any psychiatric history?” This question moves the conversation from a generic prescription to an individualized clinical decision.
If you are monitoring your weight during the cessation process, use our BMI calculator to track changes through your quit timeline.
Hidden exposures at home and work that raise your lung cancer risk
Environmental and occupational carcinogens are the most underaddressed lung cancer risk category among patients who have already quit smoking — or who have never smoked at all.
Radon — the lung cancer risk hiding in your home
Radon seeps through foundation cracks from uranium-bearing soil and accumulates in basements and lowest-floor living areas. The EPA sets 4 pCi/L as the action level for mitigation but considers any level above 2 pCi/L a meaningful reduction target for extended-occupancy spaces. EPA-certified short-term test kits — exposed for 48–96 hours and mailed to a certified laboratory — provide an accurate baseline reading.
📊 Clinical Data Point: Radon is the second-leading cause of lung cancer in the United States. Source: EPA, 2026 — verify the current EPA radon risk estimates and action level guidance at publish time. (Flag: confirm 2026 EPA attributable death estimate at publish)
🔬 How It Works: Inhaled radon decays into radioactive polonium-210, which emits alpha radiation directly against the cells lining the airways. No metabolic activation is required — the ionizing damage to DNA is immediate on cellular contact. Sub-slab depressurization systems, installed by a certified radon mitigation contractor, can reduce indoor radon levels by up to 99% in most residential structures. Testing costs less than $30. Mitigation averages $800–$2,500. The risk reduction is clinically significant.

Occupational carcinogens — who is most at risk at work?
| IARC Group 1 Carcinogen | Primary Exposure Sector | Lung Cancer Mechanism |
|---|---|---|
| Asbestos (chrysotile + amphibole fibers) | Construction, shipbuilding, insulation | Direct fiber embedding → chronic inflammation → malignant transformation |
| Diesel exhaust particulates | Trucking, mining, construction | PM2.5 penetration → oxidative DNA damage in airway cells |
| Crystalline silica | Mining, quarrying, foundry work | Silicotic fibrosis → inflammatory carcinogenesis |
| Arsenic compounds | Smelting, pesticide manufacturing | Direct DNA adduct formation |
| Beryllium | Aerospace, nuclear, electronics manufacturing | Immune-mediated chronic disease → secondary malignancy risk |
✅ Patient Action: If you have worked in any sector in the table above for five or more cumulative years, ask a board-certified occupational medicine physician: “Based on my specific exposure history, do I qualify for enhanced lung cancer surveillance — and should this exposure history be formally documented in my medical record before I leave your office today?”
Air quality, secondhand smoke, and other environmental factors
Fine particulate matter (PM2.5), classified by the IARC as a Group 1 human carcinogen, penetrates deep into the alveolar sacs and drives oxidative stress and chronic airway inflammation. Indoor cooking fumes — particularly from high-heat cooking in poorly ventilated kitchens — have been specifically linked to EGFR-mutant adenocarcinoma in never-smoking women in multiple large population cohorts. Dedicated kitchen exhaust ventilation and minimizing prolonged outdoor exposure during high-pollution air quality days are actionable steps available to every household.
What I tell my high-risk patients about lung cancer prevention
I have had this conversation hundreds of times. The version that changes outcomes is always the same.
The one conversation that changes the outcome
Every high-risk patient who arrives at my practice — whether they are still smoking, quit years ago, or never smoked but worked in the wrong building for twenty years — has what I call a prevention window. It is the period between the moment a risk factor is first recognized and the moment a radiographic finding makes that conversation moot. In that window, action changes outcomes. What I have learned after years of this work is that what closes the window is almost never a lack of information. It is a lack of someone sitting across from a patient and saying clearly: your risk is real, your options are specific, and there is something concrete you can do today.
The question every high-risk patient should ask their doctor
The single most important question you can bring to your next physician appointment is this: “Based on my age, pack-year history, and any occupational or household exposures I have had, do I qualify for annual low-dose CT screening?” That question — answered honestly and completely — closes more prevention windows than any supplement, dietary intervention, or general wellness advice I have ever seen deployed.
For patients who receive a lung cancer diagnosis despite prevention efforts, understanding treatment options available if lung cancer is detected early is the critical conversation that follows. (Editor: insert confirmed cluster URL)
Frequently asked questions about how to prevent lung cancer
Q1: What is the best way to prevent lung cancer?
The strongest evidence supports three strategies to prevent lung cancer: quitting smoking at any age, annual LDCT screening for eligible adults, and home radon testing and mitigation. No single measure guarantees prevention — but combining cessation with annual screening provides the greatest risk reduction for high-risk adults. Consult a board-certified oncologist to map these strategies to your specific exposure profile.
Q2: Can you prevent lung cancer if you smoke?
Smoking cessation reduces lung cancer risk at every age, even after decades of tobacco use. Risk decreases measurably in the years following quitting but never fully returns to a never-smoker’s baseline. Full cessation — not reduction or switching to e-cigarettes — carries the strongest clinical evidence. Consult a board-certified internal medicine physician about FDA-approved cessation medications available to you now.
Q3: What foods help prevent lung cancer?
No specific food prevents lung cancer. Diets high in cruciferous vegetables and low in processed meat are associated with modestly reduced risk in observational studies, not clinical trials. Dietary changes should complement — not replace — evidence-based prevention strategies like cessation and LDCT screening. A board-certified oncologist or registered dietitian can provide personalized nutritional guidance for your situation.
Q4: Does quitting smoking lower lung cancer risk?
Quitting smoking meaningfully lowers lung cancer risk, with measurable reduction beginning within the first years of cessation and continuing over the following decade. Former smokers who quit within the past 15 years remain LDCT screening-eligible under current USPSTF criteria. The earlier the cessation, the greater the long-term benefit. Consult a board-certified pulmonologist to confirm your current screening eligibility and residual risk.
Q5: What are the biggest risk factors for lung cancer?
The largest risk factor is cigarette smoking — responsible for the majority of US lung cancer diagnoses. Radon gas is the second-leading cause, followed by secondhand smoke and occupational exposures to asbestos, diesel exhaust particulates, and crystalline silica. Never-smokers can develop lung cancer through combined radon, environmental, and occupational carcinogen exposures without any smoking history involved.
Q6: How does radon cause lung cancer?
Radon is a naturally occurring radioactive gas that decays into alpha particles capable of direct DNA double-strand breaks in airway cells. Unlike tobacco carcinogens requiring metabolic activation, alpha radiation damages DNA on immediate cellular contact. Test your home with an EPA-certified kit and mitigate any level above 4 pCi/L — the EPA’s established action threshold — to reduce lung cancer risk from radon.
Q7: What is LDCT lung cancer screening?
Low-dose CT screening is an annual imaging test using a fraction of the radiation of a standard chest CT to detect early lung tumors before symptoms develop. It is the only imaging approach proven to reduce lung cancer mortality in high-risk adults in randomized clinical trial data. The scan takes under 15 minutes with no contrast dye or recovery period. Consult a board-certified pulmonologist to confirm whether you qualify.
Q8: Who should get screened for lung cancer?
Current USPSTF criteria recommend annual LDCT for adults aged 50 to 80 with a 20+ pack-year smoking history who currently smoke or quit within the past 15 years. Under ACA-compliant insurance plans, qualifying adults receive LDCT without cost-sharing. Adults with significant occupational exposures may also benefit from enhanced surveillance discussions with a specialist. Consult a board-certified pulmonologist to verify your eligibility against current 2026 USPSTF guidelines.
Q9: Can secondhand smoke cause lung cancer?
Secondhand smoke is a documented cause of lung cancer in non-smokers, containing more than 70 known carcinogens including benzene and polycyclic aromatic hydrocarbons. Extended household or workplace exposure elevates lung cancer risk meaningfully compared to unexposed non-smokers. Smoke-free environments at home and in the workplace are the most direct prevention measure against secondhand smoke exposure — particularly for children in the household.
Q10: Are there genetic factors in lung cancer?
Most family history of lung cancer reflects shared environmental exposures — primarily smoking and radon — rather than inherited genetic mutations. A small subset of never-smokers carries germline variants affecting carcinogen metabolism or DNA repair that modestly elevate susceptibility. EGFR mutations commonly found in lung tumors are typically acquired somatic mutations, not inherited. Discuss genetic risk assessment with a board-certified oncologist if multiple first-degree relatives have been diagnosed.
Q11: How much does radon contribute to lung cancer in the US?
Radon is the second-leading cause of lung cancer in the United States, responsible for a significant share of annual diagnoses — particularly among non-smokers with no smoking history. The EPA sets 4 pCi/L as the residential action level for mitigation. Home testing with an EPA-certified kit is the only way to assess your personal exposure level and take targeted action to prevent lung cancer from this source.
Q12: Can exercise reduce lung cancer risk?
Higher physical activity levels are associated with modestly reduced lung cancer risk in large population studies, independent of smoking history or body weight. The mechanism likely involves improved pulmonary function and reduced systemic inflammation. While the evidence is not definitive, regular aerobic activity supports overall pulmonary health as part of a broader prevention strategy. Consult your primary care physician before beginning a new exercise regimen if respiratory conditions are present.
Q13: What occupational exposures increase lung cancer risk?
IARC Group 1 occupational lung carcinogens include asbestos, diesel exhaust particulates, crystalline silica, arsenic compounds, and beryllium. Workers in construction, shipbuilding, mining, and demolition carry the highest documented cumulative exposure burden. Respiratory protective equipment and OSHA compliance reduce — but do not eliminate — exposure risk. Consult a board-certified occupational medicine physician for a formal cumulative exposure assessment and personalized surveillance plan.
Q14: Is there a vaccine for lung cancer?
No FDA-approved lung cancer vaccine currently exists in the United States. CIMAvax-EGF, an investigational therapeutic vaccine targeting epidermal growth factor, has entered early-phase US clinical trials but has not received FDA approval. Prevention of lung cancer currently relies on carcinogen avoidance, smoking cessation, and annual LDCT screening — not vaccination. Patients interested in investigational options can review active studies at clinicaltrials.gov.
Q15: How effective is smoking cessation at preventing lung cancer?
Smoking cessation is the single most effective lung cancer prevention strategy available. Risk reduction begins within years of quitting and continues for more than a decade post-cessation. Former smokers who meet age and pack-year criteria remain LDCT screening-eligible for up to 15 years post-cessation under current USPSTF guidelines. Consult a board-certified internal medicine physician about FDA-approved cessation pharmacotherapy options including varenicline and bupropion.
Q16: Does air pollution cause lung cancer?
Outdoor air pollution — classified by the IARC as a Group 1 human carcinogen — contributes to lung cancer risk through fine particulate matter (PM2.5) that penetrates deep into alveolar tissue. Indoor cooking fumes in poorly ventilated kitchens carry similar documented carcinogenic risk, particularly for never-smoking women. Limiting prolonged exposure to high-pollution outdoor environments and maintaining dedicated kitchen exhaust ventilation are actionable prevention steps.
Q17: What vitamins or supplements prevent lung cancer?
No supplement prevents lung cancer. High-dose beta-carotene is clinically contraindicated for active smokers and asbestos-exposed workers — clinical trial evidence demonstrates it increases lung cancer risk in these specific groups. Vitamin E and retinol supplements have both failed to demonstrate preventive benefit in large randomized controlled trials. Consult a board-certified oncologist before starting any supplement regimen marketed toward lung cancer prevention.
Take the next clinical step
Prevention works. Cessation works. Screening works. Radon mitigation works. These are not aspirational statements — they are conclusions from decades of clinical trial data and population surveillance. The gap between a high-risk profile and a lung cancer diagnosis is not inevitable.
Three actions are available to you this week: confirm your LDCT screening eligibility with a physician, test your home’s radon level with an EPA-certified kit, and schedule a cessation consultation if you are currently smoking. The most powerful next step is not a dietary overhaul or a supplement — it is a single honest conversation with a board-certified physician who can map your specific exposure history to the intervention with the strongest evidence behind it.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…

Board Certifications: Internal Medicine (1996); Pulmonary Disease (1999); Critical Care Medicine (1999); Sleep Medicine (2005) Experience: 29 years | Location: Sydney, Australia Education: MBBS, University of Sydney (1993);…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.