On This Page – Quick Medical Summary
What are lung cancer complications?
Lung cancer complications are health problems that arise either from the tumor itself or from the treatments used to manage it. They range from manageable symptoms addressed in an outpatient clinic to emergencies requiring immediate intervention.
Not every patient develops every complication. Your specific risk depends on tumor type, stage, location, and which treatment is underway. Understanding what can go wrong — and how clinicians respond to each problem — gives you a decisive advantage before any symptom appears.
Find your section:
- Newly diagnosed and wanting an overview? Start here, then move to Section 2.
- Currently in treatment with a new symptom? Go directly to Section 4 for the emergency urgency guide.
- Caring for a family member at home? Section 6 is written specifically for you.
- Preparing for your next oncology appointment? Section 7 gives you the question your oncologist wants you to ask.
For a full breakdown of lung cancer staging, histology, and prognosis, see our complete guide to lung cancer.
ℹ️ Medical Disclaimer: The diagnostic criteria, treatment protocols, medication information, emergency management guidance, and caregiver recommendations discussed in this article reflect current clinical guidelines as of 2026 and are provided for educational purposes only. Individual diagnostic conclusions, treatment decisions, emergency response plans, and medication choices depend on factors including patient history, comorbidities, laboratory results, imaging findings, and specialist assessment. The insurance and coverage information discussed is general in nature and varies by plan and provider. Consult a board-certified oncologist, pulmonologist, or emergency physician before acting on any clinical information in this article. This disclaimer covers all regulated clinical activities discussed throughout — including diagnosis, treatment, medication, emergency procedures, and caregiver management protocols — and applies to all sections that follow.
The most common lung cancer complications
The most common lung cancer complications fall into two categories: those caused directly by the tumor and those caused by treatment. Understanding which category a symptom belongs to changes both the urgency of the response and which specialist manages it.
Complications caused by the tumor itself
| Complication | What It Means in Plain Language | Urgency Tier |
|---|---|---|
| Malignant pleural effusion | Fluid building between lung and chest wall | Urgent |
| Hemoptysis | Coughing up blood from the airways | Urgent to Emergent |
| SVC syndrome | Face and arm swelling from vein compression | Emergent |
| Hypercalcemia | Dangerously elevated blood calcium | Urgent to Emergent |
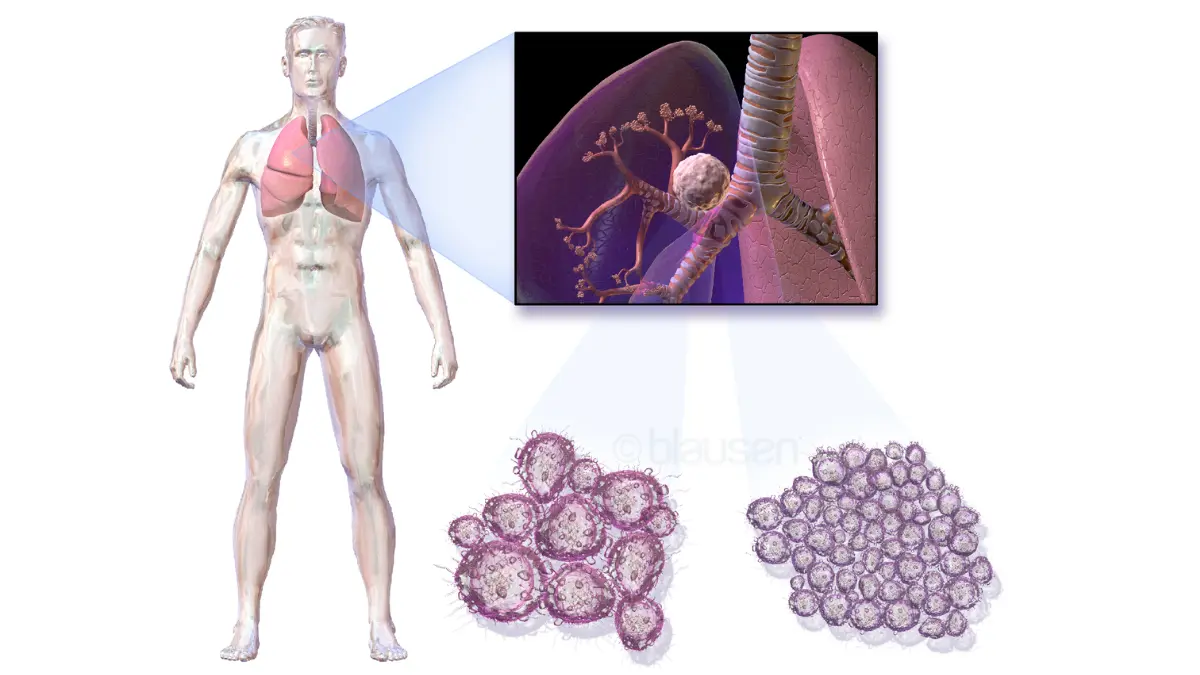
| Malignant airway obstruction | Tumor blocking a major airway | Emergent |
| Pericardial effusion | Fluid accumulating around the heart | Urgent to Emergent |
| Spinal cord compression | Tumor pressing on the spinal cord | Emergent |
| Paraneoplastic syndromes | Whole-body effects triggered by tumor signaling | Varies |
📊 Clinical Data Point: Malignant pleural effusion is one of the most frequently encountered complications in advanced non-small cell lung cancer — current incidence figures by stage are tracked in the American Cancer Society’s lung cancer statistics and data. Verify 2026 update at publish. — Source: ACS, 2026
Complications caused by lung cancer treatment
| Treatment Type | Primary Complications |
|---|---|
| Platinum-based chemotherapy | Neutropenia, peripheral neuropathy, VTE, fatigue |
| Immunotherapy (checkpoint inhibitors) | Immune pneumonitis, colitis, hepatitis, thyroid dysfunction |
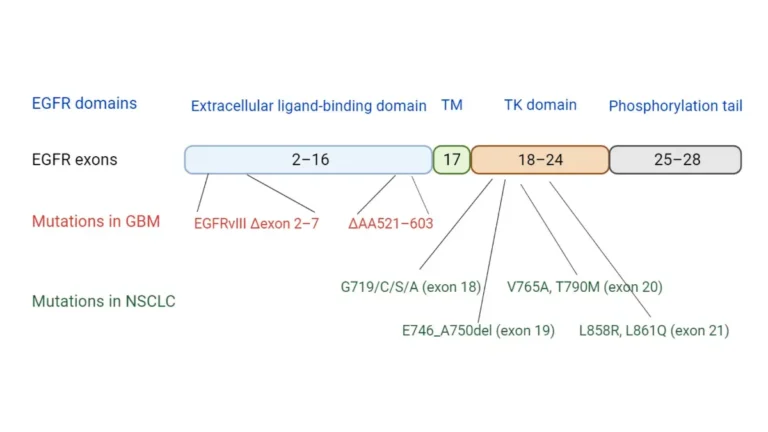
| Targeted therapy (EGFR/ALK/ROS1 inhibitors) | Skin toxicity, QTc prolongation, interstitial lung disease |
| Radiation therapy | Radiation pneumonitis, esophagitis, fatigue |
Some of these overlap with the early signs of lung cancer that prompted diagnosis — which makes distinguishing new symptoms from pre-existing ones clinically important.
Patients uncertain whether a new symptom represents a complication or a side effect can use our Symptom Checker to assess severity before calling their oncology team.
The most serious lung cancer complications explained
These complications demand specific — often urgent — medical intervention. Understanding the mechanism behind each one helps patients and caregivers respond with precision rather than panic.
Pleural effusion: fluid around the lung
🔬 How It Works: Tumor cells invading the pleura — the membrane lining the lung — trigger an inflammatory response that causes fluid to accumulate in the pleural space. This fluid compresses the lung, producing progressive dyspnea that worsens with activity and eventually occurs at rest.
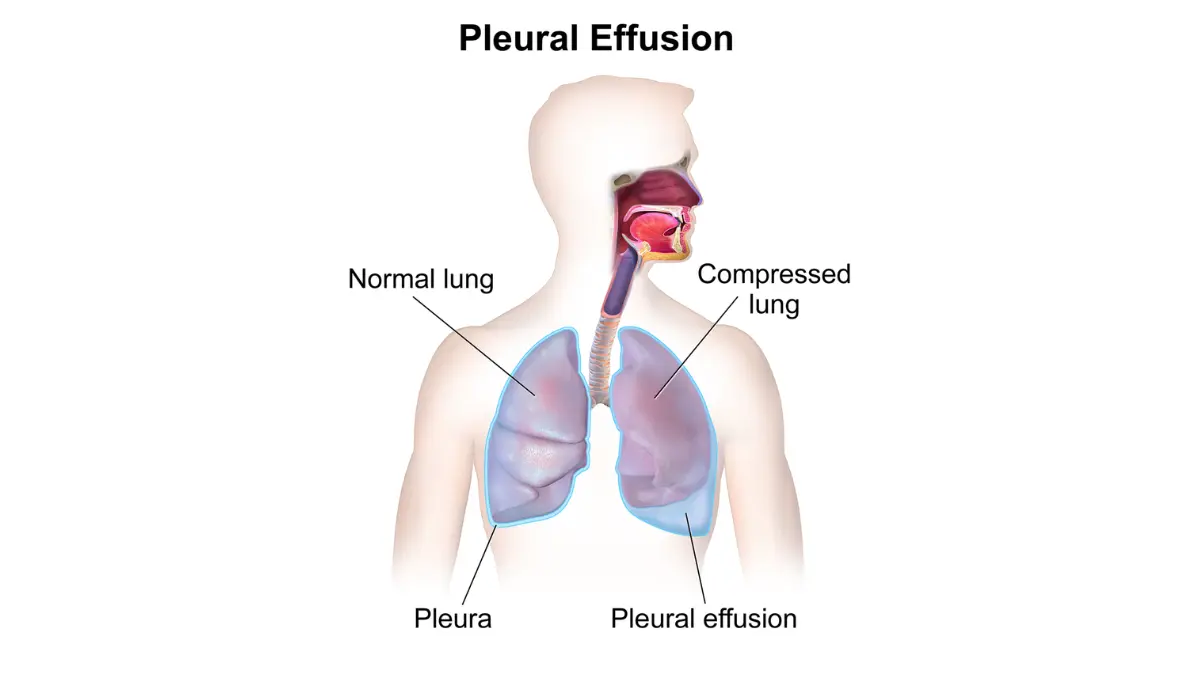
Diagnosis is confirmed by CT scan or chest X-ray. Treatment starts with thoracentesis (needle drainage of the pleural fluid). For recurrent effusions, pleurodesis — a procedure that seals the pleural space permanently — prevents re-accumulation.
SVC syndrome and cardiac tamponade: when the tumor compresses vital structures
Superior vena cava (SVC) syndrome occurs when a tumor mass or enlarged lymph nodes compress the superior vena cava — the large vein returning blood from the upper body to the heart. This causes facial swelling, arm edema, dilated neck and chest veins, and progressively worsening shortness of breath that can become a vascular emergency within hours.
⚠️ Clinical Warning: Early SVC syndrome presents subtly — a shirt collar that suddenly feels tight, mild facial puffiness on waking. By the time visible edema appears across the upper chest and arms, obstruction is typically significant and requires emergent CT with contrast imaging. Cardiac tamponade — pericardial fluid compressing cardiac output — can cause sudden cardiovascular collapse and is confirmed by emergent echocardiogram.

🩺 Physician Note: “In my clinical practice, hypercalcemia is frequently the first sign of occult bone metastasis in squamous cell carcinoma patients. They describe profound fatigue, confusion, and constipation that they attribute to chemotherapy — and a routine metabolic panel then returns a critically elevated calcium level. This is not a complication to wait on.” — Dr. Nathaniel J. Hargrove, MD (Oncology)
Blood clots and pulmonary embolism: lung cancer’s hidden vascular threat
Venous thromboembolism (VTE) — including deep vein thrombosis and pulmonary embolism — is among the most underrecognized complications of lung cancer.
📊 Clinical Data Point: Lung cancer patients carry substantially elevated VTE risk compared to the general population, driven by tumor-induced hypercoagulability, immobility during treatment, and central venous catheter use. Confirm current 2026 incidence data from NCI at publish. — Source: NCI lung cancer clinical summary, 2026
Management involves low-molecular-weight heparin (LMWH) anticoagulation; direct oral anticoagulants are considered for eligible patients. For detail on recognizing blood clot symptoms, see our guide to blood clot symptoms, causes, and treatment.
Paraneoplastic syndromes, SIADH, and hypercalcemia: when the tumor signals the whole body
🔬 How It Works: Some lung tumors secrete biologically active hormones or trigger immune responses affecting organs far from the chest. In small cell lung cancer (SCLC), neuroendocrine tumor cells frequently secrete antidiuretic hormone (ADH) ectopically — causing SIADH and life-threatening hyponatremia. In squamous cell carcinoma, tumor cells secrete PTHrP (parathyroid hormone-related protein), producing hypercalcemia even without bone metastasis. These two syndromes require different laboratory confirmation and different management protocols.
✅ Patient Action: If you develop unexplained confusion, severe constipation, excessive thirst, or progressive muscle weakness during lung cancer treatment, ask your oncologist to check serum sodium and serum calcium immediately. Consult a board-certified oncologist or endocrinologist if sodium is below 130 mEq/L or calcium exceeds 12 mg/dL — both are treatable if identified early.
Several of these complications are first detected during the lung cancer diagnostic workup, before treatment begins.
When is a lung cancer complication a medical emergency?
Not every lung cancer complication is an emergency — but some are. The three-tier framework below, based on NCCN clinical practice guidelines (2026), tells you exactly which symptoms require a 911 call, which require a same-day oncology call, and which can be monitored at home.
Go to the emergency room immediately — these complications cannot wait
- Sudden heavy hemoptysis (significant blood volume from the lungs) — possible ruptured vessel near the tumor; requires bronchoscopy and bronchial artery embolization, not treatable in urgent care.
- Rapidly progressive facial and arm swelling with dilated chest veins — possible SVC syndrome; requires emergent CT with contrast and possible endovascular stenting.
- New shortness of breath with hypotension and muffled heart sounds — possible cardiac tamponade; requires emergent echocardiogram and pericardiocentesis.
- Sudden leg weakness, loss of bladder or bowel control, or severe mid-back pain worsening when lying flat — possible spinal cord compression; requires emergency MRI within hours.
- Sudden confusion, severe agitation, or altered mental status — possible hypercalcemic crisis or brain metastasis; requires immediate metabolic panel and neurological evaluation.
📊 Clinical Data Point: Spinal cord compression from vertebral metastasis requires corticosteroid initiation within hours and decompressive intervention within 24 hours to prevent permanent neurological deficit. Verify exact treatment window threshold against 2026 NCCN guidelines at publish. — Source: NCCN Clinical Practice Guidelines in Oncology, 2026
⚠️ Clinical Warning: Do not go to an urgent care center for any of the five emergencies above. These complications require emergency imaging, specialist consultation, and interventional procedures that urgent care facilities cannot provide.
🩺 Physician Note: “I advise every lung cancer patient and caregiver: go directly to the emergency department — not urgent care — for sudden heavy coughing of blood. The source is frequently a vascular erosion adjacent to the tumor requiring bronchoscopic evaluation and bronchial artery embolization. That is not a ‘wait and see’ symptom.” — Dr. Nathaniel J. Hargrove, MD (Oncology)
Call your oncologist today — same-day urgency signs
- New hemoptysis that is blood-streaked but small in volume — still a new symptom requiring same-day evaluation
- SpO₂ below 90% at rest on a home pulse oximeter
- Fever above 100.4°F (38°C) in a patient currently on chemotherapy — neutropenic fever protocol
- New localized spine tenderness in a patient with known bone metastases
- New shortness of breath that does not resolve after 30 minutes of rest
Monitor at home — manageable complications with watchful waiting guidance
Mild fatigue, mild nausea, mild peripheral tingling, and mild radiation skin changes are managed at home with supportive care. The escalation threshold is absolute: if any “mild” symptom worsens over 24 hours or triggers any same-day call signs listed above, contact the oncology team that day.
✅ Patient Action: Ask your oncology team for a written complication response protocol — including after-hours contact and 911 triggers — specific to your treatment plan. Consult your board-certified oncologist or emergency physician immediately for any sudden neurological symptom: leg weakness, bowel or bladder loss, or severe back pain worsening at rest.
Complications caused by lung cancer treatment
Treatment-related complications arise from the mechanism of therapy itself. Each modality creates a distinct risk profile — and the specialist who manages the complication depends on which treatment caused it.
Chemotherapy complications: neutropenia, neuropathy, and VTE risk
Platinum-based chemotherapy (cisplatin, carboplatin) carries three primary complication risks: neutropenia (low white blood cell count requiring G-CSF support with filgrastim in high-risk patients), peripheral neuropathy (dose-limiting numbness and tingling in the hands and feet), and VTE (venous clot formation managed with LMWH anticoagulation). Baseline complete blood count monitoring before each cycle is standard protocol.
Checkpoint inhibitor toxicity: when immunotherapy attacks healthy tissue
🔬 How It Works: Immune checkpoint inhibitors — including pembrolizumab and nivolumab — work by releasing suppression of the immune system’s anti-tumor response. In some patients, this causes the immune system to attack healthy tissue, producing immune-related adverse events (irAEs) affecting the lungs (pneumonitis), gut (colitis), liver (hepatitis), and thyroid gland (dysfunction requiring hormone replacement).
📊 Clinical Data Point: Grade 3 or higher irAEs occur in a clinically significant proportion of checkpoint inhibitor patients — confirm current 2026 incidence rates from NCCN immunotherapy toxicity management guidelines at publish. Grade 3+ pneumonitis requires immediate drug hold and corticosteroids — Source: NCCN Guidelines, 2026
⚠️ Clinical Warning: New or worsening shortness of breath, dry cough, or fever during immunotherapy must be evaluated by your oncologist the same day. Immune checkpoint inhibitor pneumonitis can progress from Grade 1 to respiratory failure within 48–72 hours.
Targeted therapy side effects: EGFR, ALK, and ROS1 inhibitors
EGFR inhibitors such as osimertinib carry risks of skin rash, diarrhea, QTc prolongation, and a low but real signal for interstitial lung disease requiring treatment hold. ALK inhibitors such as alectinib require hepatotoxicity monitoring and photosensitivity precautions. Baseline cardiac monitoring and liver function testing are standard before starting any targeted agent.
Radiation therapy complications: acute and late effects
Radiation pneumonitis develops 6–12 weeks after thoracic radiation (acute phase) or 6–12 months later as irreversible fibrosis (late phase). Acute pneumonitis presents with dry cough, low-grade fever, and dyspnea corresponding to the radiation field on CT imaging and is managed with a corticosteroid taper per 2026 NCCN radiation toxicity protocols. Late-phase fibrosis may be permanent.
📊 Clinical Data Point: All checkpoint inhibitors and targeted agents named in this section carry current FDA approval for their specific lung cancer indications — verify approval status in the FDA drug approval database at publish. — Source: FDA, 2026
For a full comparison of treatment modalities and eligibility criteria by stage, see our guide to lung cancer treatment options.
✅ Patient Action: Before your next treatment cycle, ask your oncologist: “Given the specific agent I’m receiving, which treatment-related complication am I most at risk for, and what is the first symptom that should prompt me to call you immediately?” Consult a board-certified oncologist before independently stopping, holding, or modifying any cancer treatment.
A caregiver’s guide to managing lung cancer complications at home
Caregiving for someone with lung cancer means managing clinical uncertainty at home, often without medical training. These three protocols give you a framework built on the same logic your oncology team uses.
How to monitor lung cancer complications between oncology appointments
Check and record these daily:
- Oxygen saturation (SpO₂): SpO₂ below 90% on room air = call the oncology team immediately. SpO₂ below 85% = call 911.
- Temperature: Above 100.4°F (38°C) in a patient receiving chemotherapy = call the oncology team immediately — neutropenic fever is a medical emergency.
- New neurological changes: Any new confusion, leg weakness, or loss of bladder or bowel control = call 911.
- Facial or arm swelling: New swelling of the face, neck, or arms — especially with visible chest veins = call 911.
When to call the oncology team vs. when to call 911
Call 911 immediately for heavy hemoptysis, rapid facial or arm swelling, sudden leg weakness, loss of bladder or bowel control, and altered mental status.
Call the oncology team the same day for blood-streaked sputum (new), SpO₂ below 90%, fever in a patient on chemotherapy, new localized bone pain, and any new symptom your instinct tells you is wrong.
✅ Patient Action: Save the oncology after-hours nurse line number in your phone alongside 911. When you call, open with: “I’m calling about a lung cancer patient currently on [treatment name]. The new symptom is [describe]. It started [timeframe].” This framing triggers the correct clinical triage immediately. Consult a board-certified oncologist the same day any new warning sign appears — never wait for the next scheduled appointment.
Taking care of yourself while caring for someone with lung cancer
Caregiver fatigue is a real clinical concern — and disrupted sleep is one of its earliest signals. Our Sleep Calculator can help caregivers build a rest schedule that maintains alertness during extended caregiving periods. For more on how lung cancer-related exhaustion affects both patients and caregivers, see our guide to managing lung cancer fatigue.
What your oncologist wants you to know about lung cancer complications
How oncologists balance complication management with active cancer treatment
Complication management in lung cancer is not a binary decision between treating the cancer and treating the complication. It is a continuously recalibrated multidisciplinary tumor board judgment. A new pleural effusion mid-chemotherapy cycle may prompt a brief thoracentesis, then immediate continuation of treatment. A new Grade 3 immune pneumonitis on pembrolizumab requires immediate drug hold and high-dose corticosteroids. Both decisions follow 2026 NCCN guidelines and involve the oncologist, pulmonologist, and — when appropriate — the palliative care team working in parallel, not sequentially.
The one question patients forget to ask — and why it matters before a complication develops
Every lung cancer patient should schedule a dedicated conversation with their oncologist before a complication occurs and ask: “Given my specific tumor type, stage, and treatment plan, which complication concerns you most — and what is our protocol if it develops?”
This single conversation transforms an unknown clinical risk into a prepared response. It is the most underused tool in lung cancer management.
✅ Patient Action: Raise this question at your next appointment before any complication appears. Consult your board-certified oncologist to establish a written complication response protocol specific to your treatment — including the symptoms that trigger an ER visit, a same-day call, and home monitoring.
For resources on the psychological dimensions of managing a serious diagnosis, see our article on lung cancer and mental health.
Frequently asked questions about lung cancer complications
1. What are the most dangerous complications of lung cancer?
The most dangerous lung cancer complications include massive hemoptysis, rapidly progressive SVC syndrome, cardiac tamponade, spinal cord compression, and neutropenic sepsis in patients receiving chemotherapy. Each can become life-threatening within hours without emergency care. Your personal risk depends on tumor type, stage, and current treatment. Consult a board-certified oncologist to review your specific complication risk profile before symptoms develop.
2. Can lung cancer cause fluid around the lungs?
Yes. Malignant pleural effusion develops when tumor cells invade the pleura, triggering fluid accumulation that compresses the lung and causes progressive breathlessness. Diagnosis is confirmed by CT scan; treatment involves thoracentesis for immediate relief and pleurodesis for recurring effusions. Left untreated, significant effusion can cause respiratory failure. Consult a board-certified pulmonologist or thoracic surgeon about management options for your specific case.
3. What is superior vena cava (SVC) syndrome in lung cancer?
SVC syndrome in lung cancer occurs when a tumor or enlarged lymph nodes compress the superior vena cava, causing facial swelling, arm edema, dilated neck veins, and worsening dyspnea. Right-sided and centrally located tumors carry the highest risk. Treatment options include radiation therapy or endovascular stenting depending on tumor histology and urgency. Go directly to an emergency department if these symptoms develop acutely.
4. Does lung cancer increase the risk of blood clots?
Yes. Lung cancer elevates venous thromboembolism risk through tumor-induced hypercoagulability, treatment-related immobility, and central catheter use. Management typically involves low-molecular-weight heparin anticoagulation, with direct oral anticoagulants considered for eligible patients. Untreated pulmonary embolism can be fatal. Consult a board-certified oncologist or hematologist before starting or changing anticoagulation therapy during lung cancer treatment.
5. What are paraneoplastic syndromes and which occur with lung cancer?
Paraneoplastic syndromes are complications triggered by tumor-secreted hormones or immune signals rather than direct invasion. Common examples include SIADH (ectopic ADH secretion causing low sodium, seen in small cell lung cancer), PTHrP-mediated hypercalcemia (in squamous cell carcinoma), and Lambert-Eaton myasthenic syndrome (progressive muscle weakness, also in SCLC). Each requires specific laboratory testing for diagnosis. Consult a board-certified oncologist to determine which syndrome applies to your case.
6. Can lung cancer affect the heart?
Yes. Tumor invasion of the pericardium can cause pericardial effusion — fluid accumulation around the heart. When pressure on the cardiac chambers reaches a critical threshold, cardiac tamponade occurs: a life-threatening emergency marked by hypotension, muffled heart sounds, and acute dyspnea. Treatment is emergency pericardiocentesis. Go directly to an emergency department for sudden shortness of breath accompanied by low blood pressure or dizziness.
7. What happens when lung cancer spreads to the brain?
Brain metastasis from lung cancer causes morning headache, seizures, focal weakness, and cognitive changes. Treatment options include stereotactic radiosurgery, whole-brain radiation, dexamethasone for edema, and — in EGFR-mutated tumors — CNS-penetrant targeted therapy such as osimertinib. The optimal approach depends on metastasis number, location, and overall disease burden. Consult a board-certified oncologist and neuro-oncologist to determine the appropriate management plan.
8. How do doctors treat coughing up blood in lung cancer?
Hemoptysis management is graded by volume. Blood-streaked sputum warrants same-day oncology evaluation. Heavy active bleeding is a medical emergency requiring bronchoscopy for source identification and bronchial artery embolization for control. Palliative radiation can reduce bleeding from endobronchial tumors. Go directly to an emergency department — not urgent care — for any significant lung bleeding. Consult a board-certified pulmonologist or interventional radiologist for evaluation and management.
9. What signs indicate that lung cancer complications are worsening?
Escalating signs include rapidly worsening dyspnea over hours, new or increasing hemoptysis, progressive facial and arm swelling, new back pain with limb weakness, fever during chemotherapy, and sudden confusion or altered consciousness. Any of these changes warrants same-day oncology contact; the most acute presentations require 911. Contact your board-certified oncologist the same day any new warning sign appears during lung cancer treatment.
10. Can lung cancer cause bone pain, and what does it mean?
Bone metastasis causes localized pain typically worse at night and during activity. Common sites include vertebrae, ribs, pelvis, and femur. The primary clinical risks are pathologic fracture and — in the spine — spinal cord compression. Treatment includes bisphosphonates, denosumab, radiation therapy, and orthopedic stabilization for high-fracture-risk sites. Consult a board-certified oncologist to determine whether bone-protective therapy is appropriate for your current disease stage.
11. What is hypercalcemia in lung cancer and how is it treated?
Hypercalcemia occurs when tumor cells secrete PTHrP (in squamous cell carcinoma) or bone metastases release calcium into the bloodstream. Symptoms include fatigue, confusion, constipation, and excessive thirst. Serum calcium above 14 mg/dL constitutes a crisis requiring emergency IV fluids, bisphosphonates, and calcitonin for rapid reduction. Consult a board-certified oncologist or endocrinologist immediately if your calcium level is elevated on routine laboratory testing.
12. How does lung cancer affect breathing over time?
Lung cancer impairs breathing through airway obstruction, pleural effusion, parenchymal invasion, and treatment effects including radiation pneumonitis and targeted therapy–induced interstitial lung disease. Management depends on the specific mechanism — thoracentesis for effusion, bronchodilators for obstruction, corticosteroids for treatment-related inflammation, supplemental oxygen for sustained hypoxia. Consult a board-certified pulmonologist to identify the cause of worsening dyspnea and initiate the correct treatment.
13. What are the complications of late-stage lung cancer?
Late-stage lung cancer frequently produces malignant pleural effusion, brain metastasis, bone pain, hypercalcemia, cachexia, and progressive respiratory failure. The palliative care team specializes in managing these complications alongside or instead of active cancer treatment — providing symptom control without replacing oncology management. Consult a board-certified palliative care specialist and oncologist together to develop a comprehensive late-stage complication management plan.
14. Can lung cancer cause paralysis?
Spinal cord compression from vertebral metastasis causes progressive leg weakness, sensory loss, and bladder or bowel dysfunction. This is a medical emergency: corticosteroids must begin within hours and decompressive intervention — radiation or surgery — within 24 hours to prevent permanent paralysis. Go to an emergency department immediately for any new leg weakness, numbness, or sudden bowel or bladder change in a lung cancer patient.
15. How is radiation pneumonitis from lung cancer treatment managed?
Radiation pneumonitis develops 6–12 weeks post-treatment (acute) or 6–12 months later as irreversible fibrosis. Acute presentation includes dry cough, low-grade fever, and dyspnea within the radiation field on CT imaging. Management involves a corticosteroid taper per 2026 NCCN radiation toxicity protocols, bronchodilators, and treatment hold in severe cases. Consult your radiation oncologist at the first sign of new respiratory symptoms following thoracic radiation.
16. What are the most common complications of immunotherapy for lung cancer?
The most common complications of immunotherapy for lung cancer are immune-related adverse events: pneumonitis, colitis, hepatitis, and thyroid dysfunction. Grade 3 or higher irAEs require immediate drug hold and high-dose corticosteroids. Lower-grade events may be managed with dose modification and monitoring. Consult a board-certified oncologist immediately if you develop new dyspnea, severe diarrhea, or jaundice during checkpoint inhibitor therapy.
17. How do lung cancer complications affect survival?
The impact of lung cancer complications on survival depends on complication type and speed of treatment. Complications indicating advanced disease — brain metastasis, malignant pleural effusion at initial presentation — correlate with shorter median survival. Complications treated promptly — VTE managed with anticoagulation, pleural effusion controlled with pleurodesis — do not necessarily shorten survival. Consult a board-certified oncologist for a complication-specific prognosis discussion based on your stage and treatment plan.
Managing lung cancer complications: your next steps
Understanding the complications that can arise from lung cancer — and knowing in advance which ones require immediate emergency care, which require same-day oncology contact, and which can be monitored at home — is one of the most useful preparations any patient or caregiver can make.
This article was written by Dr. Nathaniel J. Hargrove, MD (Oncology) and reviewed by Dr. Serena V. Beaumont, MD (Immunotherapy) and Dr. Alicia M. Thornton, MD (Internal Medicine) — members of the mymedicineadvisor.com 54-member Global Medical Advisory Board. All clinical content reflects 2026 guidelines.
If you have questions about your personal complication risk profile, schedule a dedicated conversation with your board-certified oncologist before a complication develops — not after.
For a detailed breakdown of how stage, treatment response, and complication burden affect long-term outcomes, see our guide to lung cancer statistics and survival rates.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.