On This Page – Quick Medical Summary
What radiation therapy for lung cancer actually means for you
One of the first things my patients ask after a lung cancer diagnosis is whether radiation therapy will destroy healthy lung tissue permanently. It is a fair and important question — and the answer depends entirely on which technique is used and what stage of disease is being treated.
Radiation therapy is not a single treatment. It is a family of precise, technology-driven techniques, each designed for a different tumor location, stage, and patient profile. For some patients, it replaces surgery entirely. For others, it works alongside chemotherapy or immunotherapy. Understanding which type applies to you — and why — is the first step toward making an informed treatment decision.
If you are still learning about your diagnosis, our complete guide to understanding your lung cancer diagnosis explains staging, NSCLC versus SCLC classification, and how treatment plans are built from the ground up.
You can also use our Genetic Risk Assessment Tool to understand how hereditary factors may influence your cancer risk profile — a conversation worth having with your oncologist before treatment begins.
ℹ️ Medical Disclaimer: The diagnostic criteria, treatment techniques, dose schedules, drug names, side effect management protocols, and clinical trial data discussed in this article reflect current 2026 clinical guidelines and peer-reviewed evidence. This information is provided for educational purposes only. Individual treatment decisions — including choice of radiation technique, fractionation schedule, eligibility for SBRT versus IMRT, concurrent medication use, and management of treatment-related complications — depend on factors including tumor stage, tumor location (peripheral vs. central), pulmonary function, comorbidities, and multidisciplinary team assessment. Insurance coverage for specific radiation techniques varies by plan and eligibility status.
Consult a board-certified radiation oncologist before acting on any clinical information in this article. If you are experiencing symptoms you believe may be related to ongoing treatment, contact your oncology care team immediately.
How radiation therapy kills lung cancer cells
Radiation therapy destroys lung cancer cells by delivering high-energy ionizing radiation directly into the tumor, severing the DNA strands inside cancer cells and preventing them from dividing. Cancer cells divide rapidly and have weakened DNA repair mechanisms compared to healthy cells — which is exactly what makes them more vulnerable to this damage.
🔬 How It Works: When ionizing radiation enters a cancer cell, it causes what oncologists call a “double-strand DNA break” — it literally cuts both strands of the DNA helix simultaneously. A healthy cell can often repair single-strand breaks. A double-strand break in a rapidly dividing cancer cell is far harder to repair, and the cell typically dies during its next attempted division. This is why radiation is delivered in carefully planned doses rather than all at once — giving healthy surrounding tissue time to recover between sessions while the tumor accumulates lethal damage.
The difference between curative and palliative radiation for lung cancer
Not all radiation therapy for lung cancer is given with the same goal. Curative-intent radiation aims to eliminate the tumor entirely and is used for Stage I–III non-small cell lung cancer (NSCLC) when surgical resection is not possible or has been declined. Palliative-intent radiation targets metastatic sites — such as bone, brain, or adrenal glands — to relieve pain, neurological symptoms, or airway obstruction. It does not aim to eliminate the cancer but significantly improves quality of life.
Knowing which type your oncologist has recommended matters because it changes what success looks like and what side effects are worth tolerating.
✅ Patient Action: Ask your radiation oncologist directly: “Is this radiation being given with curative intent or palliative intent?” The answer changes the dose schedule, the number of sessions, and how to weigh side effects against expected benefit.
When radiation is combined with surgery or chemotherapy
For locally advanced Stage III NSCLC, radiation is almost never given alone. Concurrent chemoradiation — delivering platinum-based chemotherapy and IMRT simultaneously — is the standard protocol because the two treatments sensitize the cancer to each other, improving tumor response compared to either alone. Following chemoradiation, patients with unresectable Stage III NSCLC are typically evaluated for durvalumab consolidation immunotherapy.
For a full breakdown of how chemotherapy works alongside radiation, see our guide on lung cancer chemotherapy treatment protocols.
📊 Clinical Data Point: For patients receiving external beam radiation therapy (EBRT) for lung cancer, the ESTRO-EORTC 2026 expert guideline on radiotherapy target delineation established updated dose fractionation standards for NSCLC and SCLC, reinforcing the use of IMRT/VMAT with involved-field nodal irradiation and respiratory motion management as the current clinical benchmark. — Source: ESTRO-EORTC Expert Consensus Guideline, 2026.
For a deeper look at how NCI classifies and monitors radiation therapy use in cancer treatment, see the NCI’s overview of radiation therapy in cancer care.
SBRT and IMRT for lung cancer: what each technique does
Stereotactic body radiation therapy (SBRT) is a non-invasive, high-precision technique that delivers ablative — meaning tumor-destroying — doses of radiation to lung tumors in 1 to 5 sessions, making it the standard of care for medically inoperable early-stage NSCLC. It is also called SABR (stereotactic ablative radiotherapy) in some clinical settings. The two names refer to the same technique.
SBRT for lung cancer: how it works, who it’s for, and 2026 trial results
SBRT works by converging multiple precisely aimed radiation beams from different angles onto a single small target — the tumor — while sharply limiting dose to surrounding healthy lung tissue. Each session delivers a much higher dose per fraction than conventional radiation, which is why so few sessions are needed.
🔬 How It Works: At each SBRT session, a cone-beam CT (CBCT) scan is taken before radiation is delivered. This real-time image confirms that the tumor is exactly where the treatment plan predicts — accounting for any positional shift since the simulation. Only once the radiation oncologist or system confirms alignment is the beam activated. This image-guided radiation therapy (IGRT) process is what makes SBRT safe to use at high ablative doses.
📊 Clinical Data Point: A 2026 phase II randomized clinical trial reported by ASCO Post demonstrated that 30 Gy delivered in a single fraction achieved equivalent outcomes to 60 Gy in three fractions for peripheral early-stage NSCLC — including equivalent toxicity profiles, local failure rates, freedom from distant failure, progression-free survival, and overall survival. This finding supports a single-session SBRT protocol as a clinically valid option for eligible patients. — Source: 2026 SBRT single-fraction lung cancer trial results, ASCO Post, April 2026.
SBRT is appropriate for:
- Patients with peripheral Stage I or Stage II NSCLC who cannot tolerate thoracic surgery due to COPD, reduced pulmonary function, cardiac comorbidity, or advanced age
- Patients with medically operable early-stage NSCLC who prefer a non-surgical approach after multidisciplinary consultation
- Patients with limited oligometastatic disease to the lung in select protocols
SBRT is not automatically appropriate for central tumors — those located near the mainstem bronchus, trachea, esophagus, or major pulmonary vessels. Central location increases the risk of serious bronchial or vascular injury at ablative doses. Modified dosing or alternative techniques are used in these cases.
✅ Patient Action: Before assuming SBRT is your optimal approach, ask your radiation oncologist: “Is my tumor peripheral or central, and does its location change the dose schedule I would receive?” The peripheral-vs-central distinction is the single most important technical eligibility factor for standard SBRT protocols.
For radiation oncologists following ASTRO clinical eligibility and dosing criteria, see the ASTRO 2026 IMRT clinical guidelines.
IMRT for lung cancer: dose schedules and when it’s the right choice
Intensity-modulated radiation therapy (IMRT) uses computer-controlled beams that vary in intensity across the treatment field, conforming the dose tightly around the tumor while reducing exposure to adjacent heart, esophagus, and spinal cord. It is typically given in 30–33 daily fractions over 6–7 weeks, most commonly as part of concurrent chemoradiation for Stage II–III NSCLC.
VMAT (volumetric-modulated arc therapy) is an advanced delivery version of IMRT in which the radiation head rotates continuously around the patient, delivering the full treatment plan more efficiently. The 2026 ESTRO-EORTC guideline recommends IMRT or VMAT with involved-field nodal irradiation and 4D-CT simulation for respiratory motion management as the current standard in locally advanced NSCLC.
Can SBRT replace surgery for early-stage lung cancer?
For medically inoperable patients, SBRT is already the standard of care — not an experimental alternative to surgery. For medically operable patients, this is an active and evolving clinical question. Long-term follow-up data presented at major oncology meetings in 2025 and now reflected in 2026 clinical discussions shows 10-year overall survival with SBRT is comparable to surgical lobectomy for early-stage NSCLC, with SBRT carrying significantly fewer acute complications and a faster return to normal activity.
When durvalumab consolidation immunotherapy follows concurrent chemoradiation for unresectable Stage III NSCLC, the combination has become the established post-chemoradiation standard of care in eligible patients. See our detailed guide on lung cancer immunotherapy treatment options for how durvalumab works and who qualifies.
SBRT vs. IMRT vs. surgery: how doctors decide which to use
The treatment your oncologist recommends depends on three primary factors: tumor stage and location, your pulmonary function and surgical eligibility, and whether lymph nodes or adjacent structures are involved. No single technique is universally superior — each is the right choice under the right clinical conditions.
How tumor stage and location determine your radiation approach
| Technique | Best For | Dose Schedule | Sessions | Key Advantage | Best For Patient Profile |
|---|---|---|---|---|---|
| SBRT (peripheral) | Stage I–II NSCLC, medically inoperable | 30 Gy × 1 or 60 Gy × 3 | 1–5 | Non-surgical, minimal recovery time | Older adults, reduced lung function, surgical risk |
| SBRT (ultra-central) | Stage I–II NSCLC, central tumor, modified protocol | Modified — lower dose/fraction | 3–8 | Spares critical structures with adjusted fractionation | Patients with centrally located tumors |
| IMRT/VMAT + chemo | Stage II–III NSCLC, locally advanced | 60–66 Gy / 30–33 fractions (daily) or 45 Gy / 30 fractions (BID) | 30–33 | Covers nodal disease, concurrent chemosensitization | Patients with lymph node involvement |
| Surgical lobectomy | Stage I–II NSCLC, medically operable | N/A (surgical) | 1 procedure | Complete pathological staging, direct tissue removal | Patients with good pulmonary reserve and surgical fitness |
Source: ESTRO-EORTC Expert Guideline, 2026; ASTRO IMRT Model Policy, 2026.

🩺 Physician Note: “In my clinical practice, the decision between SBRT and surgery for an operable patient is never made by one physician alone. Every case I treat is reviewed by a multidisciplinary team that includes a thoracic surgeon, a medical oncologist, a pulmonologist, and myself as the radiation oncologist. A patient who walks in having been told they need surgery deserves to know that SBRT is a legitimate, evidence-supported alternative discussion — and a competent specialist will never make you feel pressured to skip that conversation.” — Dr. Nathaniel J. Hargrove, MD (Oncology)
What 2026 data shows about SBRT and surgery outcomes
📊 Clinical Data Point: A 2026 systematic review and meta-analysis published on PubMed evaluating SBRT for ultra-central lung malignancies reported pooled 1-year local control of 93% and 2-year local control of 84%, with pooled grade ≥3 toxicity of 9% and grade 5 (fatal) toxicity of 2%. These figures specifically apply to the more challenging ultra-central tumor location — outcomes for standard peripheral SBRT are generally more favorable. — Source: SBRT safety and local control meta-analysis, PubMed, 2026.
For a detailed comparison of surgical resection options, see our complete guide on lung cancer surgery: lobectomy, VATS, and recovery.
When radiation is combined with immunotherapy (durvalumab)
For unresectable Stage III NSCLC patients who complete concurrent chemoradiation without disease progression, durvalumab (the PACIFIC regimen) is the FDA-approved consolidation immunotherapy. It is given intravenously every 2 weeks for up to 12 months following chemoradiation. The combination significantly extends progression-free survival compared to chemoradiation alone.
Importantly, the addition of immunotherapy increases the risk of radiation pneumonitis — particularly in patients who already have underlying lung disease. This interaction is discussed in detail in the side effects section below.
✅ Patient Action: Ask your oncologist specifically: “Has my case been reviewed by a multidisciplinary tumor board including a radiation oncologist and thoracic surgeon?” This review is the NCCN standard of care for all lung cancer treatment decisions, and you have every right to request confirmation that it occurred.
What to expect during radiation therapy for lung cancer
For most patients, the word “radiation” triggers a fear of the procedure itself — what the machine looks like, whether it hurts, how long it takes. The reality is far more manageable than most patients expect before they arrive.
The simulation appointment: what actually happens
The simulation is a planning CT scan, not a treatment session. It is your longest appointment — typically 45 to 90 minutes — because the entire purpose is to map your tumor in three dimensions before a single dose is delivered.
During simulation, a 4D-CT scan captures images across your full breathing cycle to track exactly how your tumor moves as your lungs expand and contract. Tiny skin markings (either ink or small permanent tattoo dots) are placed to ensure your position is reproduced identically at every treatment session. You will lie still in a custom-built positioning mold designed specifically for your body. Nothing hurts. Nothing is injected unless contrast dye is needed for tumor visualization.
🩺 Physician Note: “I tell every patient at simulation: this is the appointment that determines the precision of everything that follows. We are not being slow — we are being exact. The 4D-CT lets us see your tumor breathing with you. When your real treatment begins, we already know exactly where it will be at every moment.” — Dr. Nathaniel J. Hargrove, MD (Oncology)
How many sessions you’ll have and how long each one takes
The number of sessions depends entirely on which technique your oncologist has recommended:
- Single-fraction SBRT (30 Gy): 1 session — approximately 30 to 60 minutes including setup and imaging
- Standard SBRT (60 Gy in 3 fractions): 3 sessions — typically delivered every other day over 1 week
- Extended SBRT (4–5 fractions): 1–2 weeks
- IMRT/VMAT with concurrent chemoradiation: 30–33 daily sessions — 6 to 7 weeks, Monday through Friday
- Palliative radiation: 1–10 sessions depending on symptom target
Each actual treatment delivery — once you are positioned — takes 10 to 20 minutes. The machine does not touch you. There is no sensation during beam delivery.
What to eat, avoid, and do on treatment days
Fatigue accumulates across a radiation course, particularly during a 6-week concurrent chemoradiation regimen. Maintaining adequate protein intake during treatment supports tissue repair and immune function.
Our Protein Intake Calculator can help you estimate your daily protein target based on your body weight and activity level — a practical tool to bring to your dietitian or oncology team.
Stay well-hydrated. Avoid smoking throughout treatment — smoking reduces tumor oxygenation and directly impairs radiation effectiveness. Avoid anti-inflammatory supplements (high-dose vitamin C, vitamin E, fish oil) without oncologist approval, as some may interfere with radiation-induced tumor cell death.
For understanding how radiation-related fatigue compares to other treatment-related fatigue patterns, see our guide on managing fatigue during lung cancer treatment.
Side effects of radiation therapy for lung cancer: what’s normal vs. urgent
Radiation pneumonitis is the side effect patients fear most — and the one most worth understanding precisely, because early recognition completely changes the outcome.
Common side effects during and immediately after treatment
Most side effects during a radiation course are mild to moderate and resolve within weeks of completing treatment. What you experience depends on the technique, dose, and area treated:
- Fatigue — affects nearly all patients; typically peaks in weeks 3–4 of a long course; managed with paced activity and adequate sleep
- Skin irritation at the treatment site — redness, mild tenderness; managed with fragrance-free moisturizers and avoiding sun exposure
- Esophagitis — soreness or difficulty swallowing, most common during concurrent chemoradiation targeting mediastinal nodes; managed with liquid diet adjustments and prescription pain relief if needed
- Dry cough — common during and after treatment; report to your care team if it worsens after treatment ends
- Temporary hair loss only in the treated area — body hair on the chest wall may thin; scalp hair is unaffected unless brain radiation is involved
Radiation pneumonitis: who gets it, how serious it is, and how it’s treated
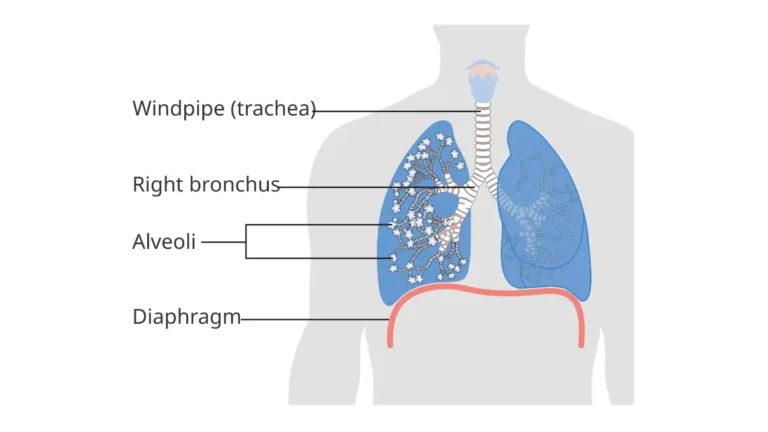
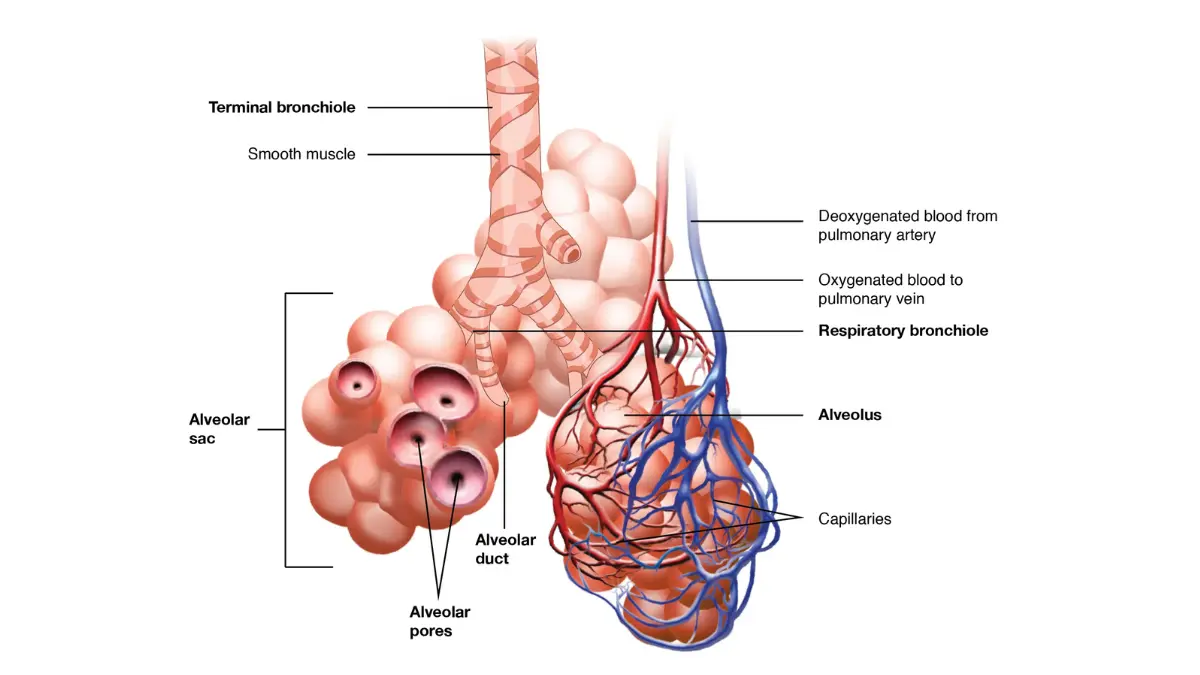
Radiation pneumonitis (RP) is an inflammatory reaction in the lung tissue that develops 4–12 weeks after completing radiation therapy, caused by radiation-induced damage to healthy alveolar cells surrounding the treated tumor. It is the most clinically significant acute complication of thoracic radiation.

📊 Clinical Data Point: A 2026 systematic review and meta-analysis published on PubMed reported pooled grade ≥3 toxicity of 9% and grade 5 (fatal) toxicity of 2% for SBRT in ultra-central lung tumors — a higher-risk subset. A 2026 study published in Nature Communications Medicine assessed pneumonitis risk specifically in patients receiving radiation plus immunotherapy, identifying this combination as carrying elevated RP risk requiring active monitoring. — Source: PubMed meta-analysis, 2026; Nature Communications Medicine, 2026.
Symptoms to recognize:
- New or worsening shortness of breath
- Dry, persistent cough that develops or worsens after treatment ends
- Low-grade fever (above 100.4°F)
- Chest tightness without a prior cardiac explanation
Treatment: When caught early, radiation pneumonitis responds well to oral corticosteroids (typically prednisone). The critical window is early — before the inflammatory cascade progresses to fibrosis.
⚠️ Clinical Warning: If you develop any combination of new shortness of breath, dry cough, and low-grade fever within 3 months of completing thoracic radiation, contact your radiation oncologist or oncology nurse line immediately — do not wait for your next scheduled appointment. Radiation pneumonitis treated early rarely becomes life-threatening. Treated late, it can progress to permanent radiation fibrosis that significantly reduces lung function.
The risk of radiation pneumonitis is meaningfully higher when durvalumab immunotherapy is added following chemoradiation. Patients on the PACIFIC regimen require active pulmonary monitoring throughout the consolidation phase.
If you are currently experiencing symptoms and want to document them before your next appointment, our Symptom Checker lets you log and track your symptoms in detail to share with your care team.
✅ Patient Action: Ask your oncologist: “Given my treatment protocol, what is my personal risk level for radiation pneumonitis, and what specific symptoms should send me to the phone immediately?” The threshold differs between a patient receiving palliative SBRT and one receiving concurrent chemoradiation followed by durvalumab.
Long-term side effects: what may persist after treatment ends
Radiation fibrosis is a long-term change in lung tissue — scarring that develops months to years after treatment — most commonly in the region that received the highest dose. Mild fibrosis often causes no symptoms. More significant fibrosis can reduce exercise tolerance and oxygen saturation.
To understand how your lung cancer treatment affects long-term prognosis and survival expectations, our guide on lung cancer prognosis and survival rates by stage provides a detailed breakdown matched to treatment type.
What your radiation oncologist wants you to know before you start
I have treated lung cancer patients with radiation for over two decades. The patients who navigate treatment most successfully share one thing in common: they arrive at their first radiation oncology appointment with specific questions — not generic fears.
The three questions every lung cancer patient should ask before radiation begins
Ask these three questions at your first radiation oncology consultation:
- “Is my tumor peripheral or central, and how does that change my SBRT dose schedule?” — The answer determines whether single-fraction, 3-fraction, or modified dosing applies to your case, and whether your tumor’s location increases your risk of serious side effects.
- “Has my case been reviewed by a multidisciplinary tumor board that includes a thoracic surgeon?” — NCCN guidelines require this for all lung cancer treatment decisions. If it has not happened, ask for it before consenting to treatment.
- “If I receive durvalumab after chemoradiation, what is my individual risk for radiation pneumonitis, and what monitoring protocol will you use?” — This question is especially important for patients with pre-existing COPD, reduced FEV1, or bilateral lung involvement.
For a full view of all lung cancer treatment modalities and how radiation fits into the overall plan, our guide on lung cancer treatment options compared gives the complete treatment decision framework.
Red flags that should send you back to your oncologist immediately
These symptoms require a same-day call — not a wait-and-see:
- Fever above 100.4°F combined with new or worsening shortness of breath at any point during or after treatment
- Coughing up blood (hemoptysis) — requires immediate evaluation regardless of treatment stage
- Sudden chest pain that is new, sharp, or radiating
- Neurological symptoms — sudden confusion, severe headache, vision changes — which may indicate brain metastasis requiring urgent imaging
- Oxygen saturation dropping below 94% on a home pulse oximeter🩺 Physician Note: “When a patient calls my office three weeks after finishing a radiation course and describes a new dry cough with mild shortness of breath and a 99.8°F fever, I do not reassure them over the phone. I bring them in that day. Radiation pneumonitis in the early inflammatory stage is very treatable. My job is to catch it before it becomes something I cannot reverse.” — Dr. Nathaniel J. Hargrove, MD (Oncology)
For a detailed breakdown of current FDA-approved drugs used in lung cancer treatment alongside radiation, including targeted therapy and immunotherapy agents, see our guide on FDA-approved lung cancer drugs and treatment options for 2026.
Radiation therapy for lung cancer: frequently asked questions
1. What is radiation therapy for lung cancer?
Radiation therapy for lung cancer delivers high-energy ionizing radiation directly into tumor tissue, breaking apart the DNA inside cancer cells and stopping them from dividing. It is used with curative intent for Stage I–III NSCLC and with palliative intent for metastatic disease. The two primary techniques — SBRT and IMRT — are used in different clinical situations based on tumor stage, location, and surgical eligibility. Consult a board-certified radiation oncologist to determine which approach applies to your case.
2. What is SBRT for lung cancer?
SBRT is a high-precision radiation technique that delivers ablative doses — typically 30 Gy in 1 session or 60 Gy in 3 sessions — to lung tumors with millimeter-level accuracy. It is the standard of care for medically inoperable early-stage NSCLC. A 2026 phase II randomized trial confirmed that single-fraction SBRT achieves equivalent outcomes to 3-fraction SBRT in peripheral tumors. Consult a board-certified radiation oncologist to confirm your tumor’s eligibility for the single-fraction protocol.
3. How many radiation sessions are needed for lung cancer?
The number of sessions depends on the technique: SBRT typically requires 1–5 sessions over 1–2 weeks, while IMRT for locally advanced NSCLC typically requires 30–33 daily sessions over 6–7 weeks. Palliative radiation therapy for metastatic sites may require as few as 1–5 sessions. Each actual treatment delivery takes 10–20 minutes once positioned. Consult a board-certified radiation oncologist to confirm your specific session count based on tumor stage and protocol.
4. Is SBRT better than surgery for early-stage lung cancer?
For medically inoperable patients with peripheral Stage I NSCLC, SBRT is the standard of care and achieves local control rates of 93% at 1 year based on 2026 meta-analysis data. For medically operable patients, 10-year overall survival with SBRT is comparable to surgical lobectomy, with fewer acute complications. The right choice depends on your surgical fitness, tumor location, and pulmonary function testing. Consult a board-certified thoracic surgeon and radiation oncologist together before deciding.
5. What is the difference between SBRT and IMRT?
SBRT delivers very high doses per session in 1–5 treatments — used for small, localized, early-stage tumors. IMRT delivers moderate doses across 30–33 daily sessions — used for larger, locally advanced tumors involving lymph nodes, often alongside concurrent chemotherapy. SBRT is not appropriate for all tumor locations or stages. IMRT covers a broader treatment volume. The choice is determined by tumor size, stage, nodal involvement, and your overall treatment plan.
6. What are the side effects of radiation therapy for lung cancer?
Common side effects include fatigue, mild skin irritation at the treatment site, dry cough, and esophagitis during concurrent chemoradiation. The most serious acute complication is radiation pneumonitis — lung inflammation developing 4–12 weeks post-treatment that affects a subset of patients and requires early corticosteroid treatment. Long-term effects may include radiation fibrosis in the treated region. Side effect severity varies by technique, dose, and tumor location.
7. What is radiation pneumonitis and how serious is it?
Radiation pneumonitis is an inflammatory reaction in the lung developing 4–12 weeks after thoracic radiation, caused by damage to healthy alveolar cells surrounding the tumor. A 2026 meta-analysis reported grade ≥3 toxicity in 9% of SBRT ultra-central cases and grade 5 toxicity in 2%. When caught early, it responds well to corticosteroids. Untreated, it can progress to permanent fibrosis. Consult a board-certified radiation oncologist immediately if you develop fever, worsening shortness of breath, or dry cough post-treatment.
8. Can radiation cure lung cancer?
Radiation therapy can achieve curative outcomes in early-stage NSCLC — particularly Stage I and II disease treated with SBRT, where local control rates exceed 90% at 1 year based on 2026 data. For Stage III locally advanced NSCLC treated with concurrent chemoradiation plus durvalumab, long-term disease control is achievable. Stage IV disease is not treated with curative-intent radiation. Whether radiation is curative for your specific case depends on stage, tumor biology, and overall treatment response.
9. What is IMRT for lung cancer?
IMRT is an external beam radiation technique that uses computer-controlled beams of varying intensity to deliver a precisely contoured radiation dose to locally advanced lung tumors while sparing the heart, esophagus, and spinal cord. It is typically delivered daily over 6–7 weeks and is almost always combined with concurrent platinum-based chemotherapy for Stage III NSCLC. VMAT is an advanced IMRT delivery method that reduces treatment time. Consult a board-certified radiation oncologist to determine IMRT eligibility based on your staging.
10. How long does radiation therapy for lung cancer last?
SBRT lasts 1–2 weeks (1–5 sessions). Concurrent chemoradiation with IMRT lasts 6–7 weeks (30–33 daily sessions). Palliative radiation for metastatic sites may be completed in 1–2 weeks. Each session takes 10–20 minutes of actual beam delivery, though total appointment time including setup and imaging is typically 30–60 minutes. Consult a board-certified radiation oncologist for your exact timeline based on technique and tumor protocol.
11. Can you eat normally during radiation treatment for lung cancer?
Most patients receiving SBRT eat normally throughout their 1–5 sessions. Patients undergoing concurrent chemoradiation over 6–7 weeks often develop esophagitis — soreness when swallowing — requiring soft or liquid diet adjustments mid-course. Adequate protein and hydration are clinically important throughout radiation therapy. Avoid high-dose antioxidant supplements (vitamin C, vitamin E, fish oil) during treatment without oncologist approval, as they may interfere with radiation-induced tumor cell death. Ask your oncology dietitian for a personalized plan.
12. What happens to your lungs after radiation therapy?
After radiation therapy, the treated area of the lung may develop radiation fibrosis — gradual scarring that typically stabilizes within 12–18 months post-treatment. Mild fibrosis is common on imaging but causes no symptoms in many patients. More extensive fibrosis can reduce exercise tolerance. Radiation pneumonitis, an acute inflammatory phase occurring 4–12 weeks post-treatment, precedes fibrosis in some patients. Serial CT imaging and pulmonary function testing track long-term lung changes.
13. What is the survival rate after radiation therapy for lung cancer?
Survival after radiation therapy for lung cancer varies significantly by stage and technique. SBRT for Stage I NSCLC achieves 1-year local control rates above 90% based on 2026 meta-analysis data. Stage III NSCLC treated with concurrent chemoradiation plus durvalumab demonstrates meaningful long-term progression-free survival improvement versus chemoradiation alone. Overall survival rates by lung cancer stage are detailed in our guide on lung cancer statistics and survival rates by stage. Consult a board-certified oncologist for your personal prognosis.
14. Does radiation therapy shrink lung tumors?
Yes — radiation therapy shrinks lung tumors by causing lethal DNA damage in cancer cells, triggering cell death during subsequent division attempts. Tumor shrinkage is typically visible on follow-up CT or PET-CT imaging performed 6–12 weeks after completing radiation therapy. SBRT often produces significant tumor volume reduction at ablative doses. The degree and speed of shrinkage depends on tumor size, histology, and radiation dose delivered. Ask your radiation oncologist when your first post-treatment imaging is scheduled.
15. How effective is SBRT for Stage I lung cancer?
SBRT is highly effective for peripheral Stage I NSCLC — the 2026 PubMed meta-analysis data reports 1-year local control of 93% even for the more technically challenging ultra-central cases. Peripheral Stage I tumors treated with standard SBRT protocols achieve even stronger local control. For medically inoperable patients, SBRT is considered the definitive curative-intent treatment. Consult a board-certified radiation oncologist to confirm Stage I eligibility and which dose fractionation — single-fraction or 3-fraction — applies to your tumor.
16. Can radiation therapy be combined with immunotherapy for lung cancer?
Yes — for unresectable Stage III NSCLC, durvalumab immunotherapy is administered following concurrent chemoradiation as the FDA-approved PACIFIC regimen. The combination extends progression-free survival significantly compared to chemoradiation alone. However, adding immunotherapy to radiation meaningfully increases the risk of radiation pneumonitis, per 2026 Nature Communications Medicine research. Patients receiving this combination require active pulmonary monitoring. Consult a board-certified medical oncologist and radiation oncologist together before starting this combination approach.
17. What should I ask my radiation oncologist before starting treatment?
Before starting radiation therapy for lung cancer, ask: (1) “Is my tumor peripheral or central, and which SBRT dose schedule applies?” (2) “Has my case been reviewed by a multidisciplinary tumor board including a thoracic surgeon?” (3) “What is my personal risk for radiation pneumonitis given my treatment plan and lung function?” (4) “When is my first post-treatment imaging scan, and what symptoms should prompt me to call before that date?” Writing down specific answers at that appointment significantly improves treatment decision-making.
Your next step after reading this guide
Understanding radiation therapy for lung cancer — which technique applies to you, what the sessions involve, and which side effects require urgent attention — puts you in a far stronger position for your next oncology appointment.
The three most important actions to take before that appointment: confirm your tumor has been staged and locationally classified (peripheral vs. central), verify your case has been reviewed by a multidisciplinary team, and write down the specific side effect threshold that should prompt an immediate call to your care team.
You are not navigating this alone. Our complete lung cancer treatment options guide covers the full treatment landscape — surgery, chemotherapy, targeted therapy, immunotherapy, and radiation — so you can see where your recommended approach fits within your overall plan.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.