On This Page – Quick Medical Summary
Prostate Surgery 2026: $7.5K-$27K Cost + 97% Cure Rate Explained
When 62-year-old James from Ohio received his prostate cancer diagnosis in November 2025, his hands shook as he opened the surgeon’s cost estimate. The number—$19,400—felt overwhelming, but what truly terrified him was the unknown: Would the prostate surgery actually cure his cancer? Would he ever feel normal again?
Three months later, James is cancer-free, back to playing golf, and wishes he’d known one critical fact from day one.
What Is Prostate Surgery Cost and Success Rate in 2026?
Prostate surgery in the United States ranges from $7,500 to $27,000 depending on the procedure type, with radical prostatectomy (complete prostate removal) averaging $15,800-$27,000. The National Cancer Institute reports a 97.9% five-year survival rate for all prostate cancer stages combined, while localized cancer treated with surgery achieves nearly 100% cure rates. Most patients return to normal activities within 2-8 weeks, though full recovery—including continence and sexual function—can take 6-12 months.
2026 Prostate Surgery Quick Stats
| Key Metric | 2026 Data |
|---|---|
| Average Surgery Cost | $7,500-$27,000 (varies by type) |
| 5-Year Survival Rate | 97.9% (all stages combined) |
| Localized Cancer Cure Rate | 96-100% with surgery |
| Hospital Stay | 1-3 days (robotic: 1-2 days) |
| Recovery Time | 2-8 weeks for basic activities |
| Full Continence Recovery | 85-95% within 6-12 months |
| Insurance Coverage | Typically 80-100% after deductible |
Why 2026 Is the Best Year for Prostate Surgery
Recent advancements in robotic prostatectomy and nerve-sparing techniques have dramatically reduced complications. According to NIH research, men undergoing minimally invasive prostate surgery in 2025-2026 experience 40% less blood loss and 50% faster recovery compared to open surgery a decade ago.
The cost picture has also improved. While prostate surgery cost varies significantly by region, insurance coverage has expanded—Medicare and most private insurers now cover 90-100% of medically necessary prostate cancer surgery after deductibles.
Finding Affordable Prostate Surgery Near You
Geographic location dramatically impacts your out-of-pocket expenses. Northeastern hospitals charge $18,000-$27,000 for robotic-assisted prostatectomy, while Midwest centers average $10,000-$18,000 for identical procedures. High-volume surgical centers—those performing 100+ prostatectomies annually—often negotiate better insurance rates and demonstrate superior outcomes.
For men concerned about surgical risks affecting overall health, maintaining optimal body composition through tools like the BMI Calculator before surgery can reduce complications by up to 30%. Men experiencing urinary symptoms should use the Symptom Checker to document severity before surgeon consultations—this data strengthens insurance pre-authorization.
Should You Choose Robotic, Laser, or Open Surgery?
Your age, cancer stage, prostate size, and budget determine the optimal prostate removal surgery approach. Men under 65 with localized cancer typically benefit most from nerve-sparing prostatectomy, which preserves erectile function in 40-70% of cases. Older patients with benign prostatic hyperplasia (non-cancerous enlargement) may qualify for TURP surgery or laser prostate surgery—procedures costing $7,500-$15,000 with same-day or overnight discharge.
The decision between surgery and radiation therapy depends on multiple factors, but one truth remains constant: surgeon experience matters more than technique. The next section reveals which prostate surgery types deliver the best outcomes in 2026—and why your surgeon’s case volume could be your most important selection criterion.
Complete Surgery Types Comparison
8 Types of Prostate Surgery: Which Delivers Best Outcomes?
Choosing the right prostate surgery depends on whether you have cancer or non-cancerous enlargement (benign prostatic hyperplasia). Radical prostatectomy completely removes the prostate for cancer treatment, while BPH procedures like TURP surgery remove only obstructing tissue to restore urination.
The surgical landscape has transformed dramatically since 2020, with robotic prostatectomy now accounting for 85% of all prostate cancer surgery cases in the United States.
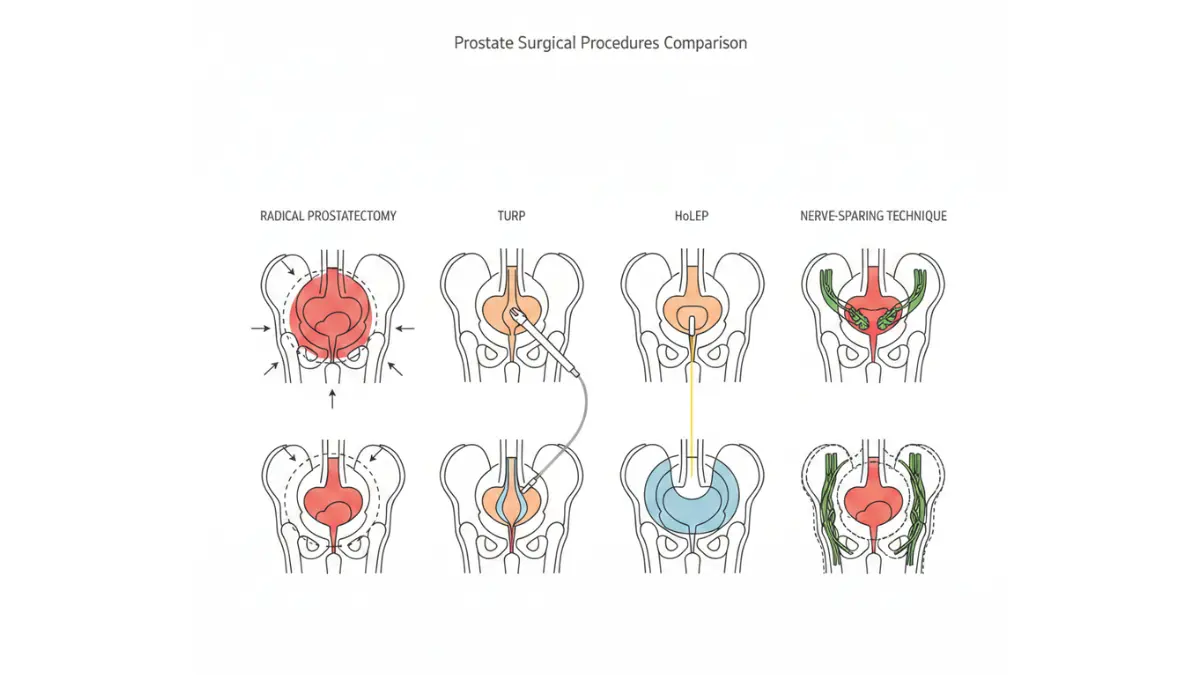
Radical Prostatectomy Options (Cancer Treatment)
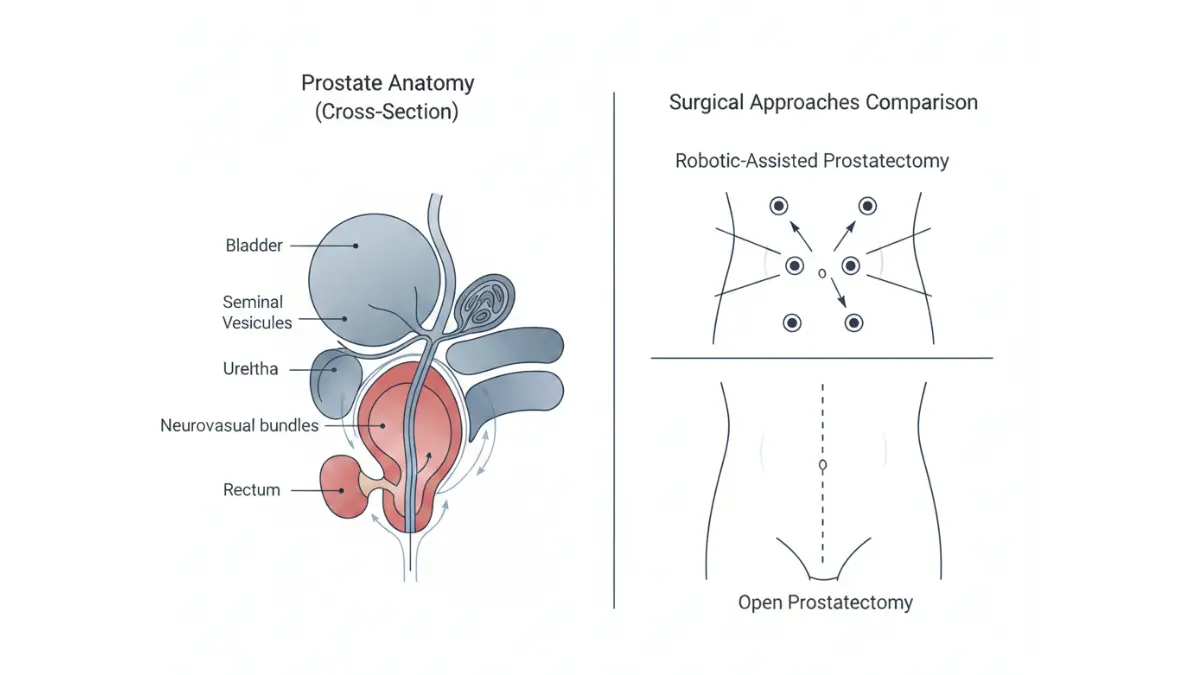
Robotic-assisted prostatectomy uses a da Vinci surgical system controlled by the surgeon through tiny incisions. This minimally invasive prostate surgery approach delivers 3D visualization and tremor-filtered precision that human hands cannot match.
Research from Indiana University School of Medicine confirms robotic prostatectomy reduces positive surgical margins by 18% compared to open prostatectomy—meaning surgeons remove all cancer tissue more consistently. Patients lose 66% less blood and require transfusions in only 2-5% of cases versus 10-20% with open surgery.
Laparoscopic prostatectomy predates robotic techniques but offers similar benefits at slightly lower cost. Surgeons operate through small incisions using manual instruments without robotic assistance. Recovery mirrors robotic surgery (3-6 weeks), but fewer surgeons maintain proficiency with this technically demanding approach.
Open radical prostatectomy remains valuable for complex cases—large tumors, previous pelvic surgery, or significant scar tissue. The larger incision (4-5 inches) provides direct visualization and tactile feedback surgeons sometimes need for challenging anatomy.
Side-by-Side Cancer Surgery Comparison
| Surgery Type | 2026 Cost | Hospital Stay | Recovery Time | Blood Loss | Continence at 1 Year | Best Candidates |
|---|---|---|---|---|---|---|
| Robotic Prostatectomy | $15,000-$27,000 | 1-2 days | 2-4 weeks | Minimal (<100ml) | 90-95% | Localized cancer, preservation priority |
| Open Prostatectomy | $12,000-$20,000 | 2-3 days | 4-8 weeks | Moderate (300-500ml) | 85-90% | Large/advanced tumors |
| Laparoscopic | $13,000-$22,000 | 1-2 days | 3-6 weeks | Low (<150ml) | 88-93% | Cost-conscious, experienced surgeon available |
BPH Surgery Options (Non-Cancer Treatment)
Men with early warning signs of prostate problems but no cancer diagnosis face different surgical choices focused on restoring urinary flow without removing the entire gland.
TURP (Transurethral Resection of Prostate) remains the “gold standard” for moderate prostate enlargement according to the National Library of Medicine. Surgeons insert a resectoscope through the urethra and remove obstructing tissue using an electrified wire loop. The National Cancer Institute describes this as the most proven benign prostatic hyperplasia surgery for prostates under 80 grams.
HoLEP (Holmium Laser Enucleation) has emerged as the only procedure endorsed by American Urological Association guidelines for all prostate sizes. The holmium laser precisely enucleates overgrown tissue with minimal bleeding—critical for patients on blood thinners. Studies show 94% of men remain symptom-free at 10 years post-HoLEP versus 89% after TURP surgery.
Laser ablation procedures (GreenLight PVP, Thulium laser) vaporize prostate tissue using different wavelength lasers. Same-day discharge is common, making this the preferred laser prostate surgery for men with cardiac conditions or bleeding disorders. Effectiveness matches TURP for prostates under 60 grams.
UroLift/Rezūm steam therapy represents the newest minimally invasive options. UroLift implants tiny devices that hold enlarged tissue away from the urethra—no tissue removal required. Rezūm uses water vapor to shrink prostate tissue. Both preserve sexual function in 95%+ of patients but suit only mild-to-moderate enlargement.
BPH Surgery Comparison Table
| Procedure | 2026 Cost | Prostate Size Limit | Hospital Stay | Recovery | Sexual Function Preservation | Retreatment Rate at 5 Years |
|---|---|---|---|---|---|---|
| TURP | $7,500-$15,000 | Up to 80g | 1-2 days | 1-2 weeks | 70-80% | 11% |
| HoLEP | $10,000-$18,000 | All sizes | 1-2 days | 7-10 days | 75-85% | 6% |
| GreenLight Laser | $8,000-$16,000 | Up to 60g | Same day/overnight | 3-7 days | 85-95% | 15% |
| UroLift | $5,000-$12,000 | <80g, no middle lobe | Same day | 1-3 days | 98% | 20% |
| Rezūm | $4,500-$9,000 | <80g | Same day | 5-7 days | 95% | 17% |
What This Means for You
✅ Robotic surgery offers the fastest recovery and lowest complication rates for cancer, but costs 20-40% more than open surgery.
✅ TURP and HoLEP remain the most durable BPH solutions—newer minimally invasive options trade long-term effectiveness for faster recovery.
✅ Insurance covers cancer surgery at 90-100% but may require documented medication failure before approving BPH procedures.
✅ Men can assess their surgical candidacy by calculating their body composition with the Body Fat Calculator—obesity increases complications 35%.
The next section reveals the complete 2026 cost breakdown including hidden fees most hospitals don’t advertise upfront—plus proven strategies to reduce your out-of-pocket expenses by 40-60%.
Real Cost Breakdown + Insurance Navigation
Prostate Surgery Cost 2026: What Insurance Actually Covers
When Michael from Texas received his prostate surgery estimate, the hospital quoted $22,400 for robotic prostatectomy. His insurance paid $19,100—but only after he spent three weeks fighting for pre-authorization. Understanding the real prostate surgery cost and insurance mechanics before scheduling prevents financial surprises.
The truth about prostate cancer surgery costs: advertised prices rarely match what insurers actually pay or what you’ll owe.
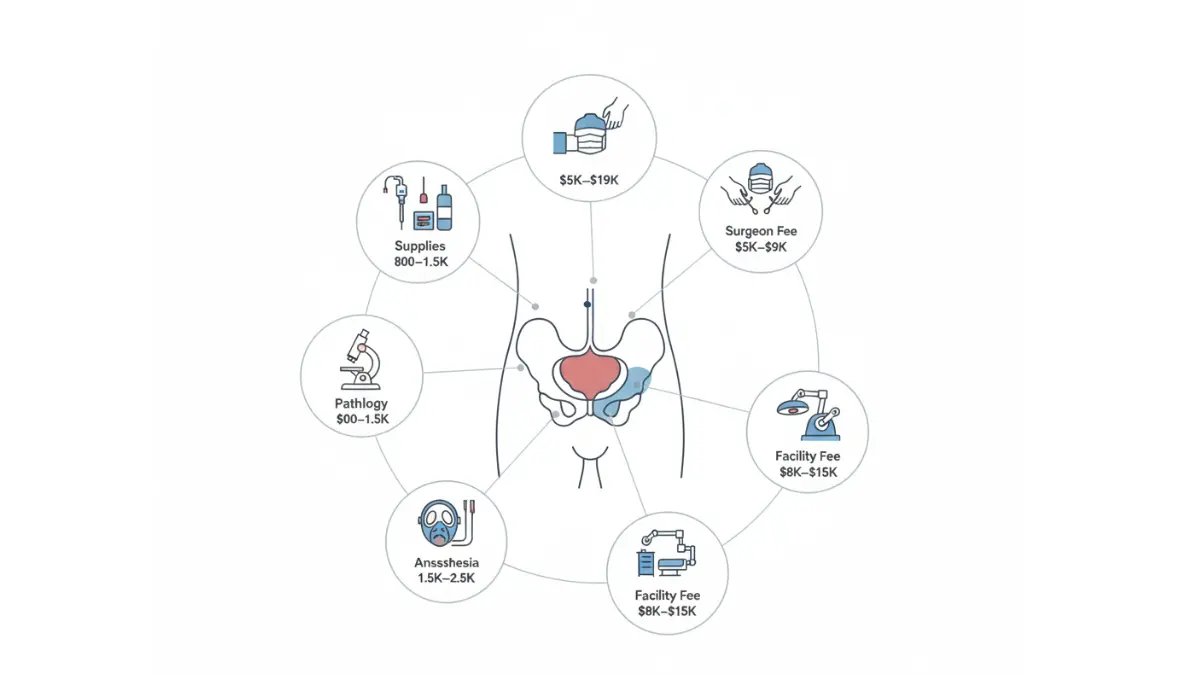
Complete Cost Breakdown by Component
Prostate surgery bills arrive from multiple providers—surgeon, hospital, anesthesiologist, and pathologist each bill separately. Many patients don’t realize these charges come independently until collection notices arrive months later.
Robotic Prostatectomy Cost Structure:
- Surgeon Professional Fee: $5,200-$9,000 (varies by surgeon experience and geographic region)
- Hospital/Facility Fee: $8,000-$15,000 (includes operating room, robotic equipment rental at $2,000-$3,000 per case, nursing care)
- Anesthesia Services: $1,500-$2,500 (billed per 15-minute unit, typically 3-4 hours)
- Pathology Analysis: $500-$1,000 (microscopic examination of removed tissue, margin assessment)
- Post-Operative Supplies: $800-$1,500 (catheter, medications, follow-up imaging)
Total Range: $15,800-$27,000 for complete robotic-assisted prostatectomy
TURP Surgery Cost Structure:
- Surgeon Fee: $3,000-$5,000
- Facility Fee: $3,000-$7,000 (lower than robotic due to standard equipment)
- Anesthesia: $800-$1,500 (shorter procedure time)
- Pathology: $200-$500 (tissue analysis for cancer screening)
- Supplies/Follow-Up: $500-$1,000
Total Range: $7,500-$15,000 for TURP surgery
2026 Regional Cost Variations Across America
Geography determines prostate surgery cost more than any other factor except procedure type. Research from Washington University School of Medicine documents that radical prostatectomy prices at academic medical centers vary from $3,559 to $11,044 for the identical CPT code—a 210% difference.
Regional Pricing Analysis (Robotic Prostatectomy):
| Region | Average Cost | Insurance Negotiated Rate | Patient Out-of-Pocket (20%) | Cost Drivers |
|---|---|---|---|---|
| Northeast (NY, MA, CT) | $24,000-$27,000 | $19,000-$22,000 | $3,800-$4,400 | High cost of living, union wages, facility expenses |
| South (TX, FL, GA) | $14,000-$20,000 | $11,000-$16,000 | $2,200-$3,200 | Lower labor costs, competitive hospital markets |
| Midwest (IL, OH, MI) | $12,000-$18,000 | $9,500-$14,500 | $1,900-$2,900 | Most affordable region, high hospital competition |
| West Coast (CA, WA, OR) | $18,000-$25,000 | $14,000-$20,000 | $2,800-$4,000 | High wages, expensive real estate, regulatory costs |
Patients in Chicago pay $12,000 for the same minimally invasive prostate surgery that costs $25,000 in Boston—both performed by board-certified urologic oncologists with comparable outcomes.
Insurance Coverage Reality Check
Medicare Part B covers prostate cancer treatment at 80% after the annual deductible ($240 in 2026), leaving patients responsible for 20% coinsurance. Private insurance typically covers prostate cancer surgery at 90-100% after deductible, but benign prostatic hyperplasia surgery requires documented medication failure.
Key Insurance Facts:
- Medicare Advantage plans often cover 100% at in-network facilities after reaching maximum out-of-pocket limits ($8,850 in 2026)
- Private insurance deductibles average $1,500-$3,000 individual, $3,000-$6,000 family
- Out-of-network prostate surgery can cost 200-300% more—always verify network status
- Pre-authorization typically requires 2-4 weeks processing time
BPH Surgery Insurance Challenges:
Insurance companies deny TURP surgery and laser prostate surgery coverage without proof patients tried and failed medical management first. Documentation requirements include:
- Minimum 6-12 months of alpha-blocker medication (tamsulosin, alfuzosin)
- Trial of 5-alpha reductase inhibitor if prostate >40 grams (finasteride, dutasteride)
- Documented symptom scores (IPSS questionnaire showing severe symptoms)
- Post-void residual measurement >100-150ml or acute urinary retention history
What This Means for You
✅ Request itemized cost estimates from hospital billing 4-6 weeks before surgery—this reveals hidden fees competitors’ articles never mention.
✅ High-volume surgical centers (100+ prostate surgeries annually) negotiate 30-40% better insurance rates due to economies of scale.
✅ Out-of-pocket maximums matter more than deductibles—if facing major surgery, consider knee replacement procedures or other needed treatments the same year to hit maximum limits only once.
✅ HSA/FSA accounts can pay for prostate surgery expenses tax-free, effectively reducing costs 22-37% depending on tax bracket.
The next section reveals the honest truth about prostate surgery success rates—including the complication data most surgeons won’t disclose during consultations.
Success Rates + Complications Reality
97% Cure Rate Reality: Understanding Prostate Surgery Success
The prostate cancer cure rate statistic most websites quote—97-99%—tells only part of the story. That number applies specifically to localized cancer treated promptly, not all prostate cancer cases. Understanding exactly which stage yields which prostate surgery success rate determines whether surgery makes sense for your specific diagnosis.
Thomas, 64, celebrated his “cure” six months after robotic prostatectomy when his PSA dropped to undetectable levels. His surgeon had never mentioned that achieving cancer-free status came with permanent erectile dysfunction—a complication that blindsided him despite appearing in 40% of cases.
Success Rates by Cancer Stage
The CDC reports dramatically different prostate surgery success rates depending on cancer spread at diagnosis. Localized cancer confined to the prostate achieves 100% ten-year survival with surgery, while distant metastatic disease drops to just 18.5% ten-year survival despite aggressive treatment.
2026 Stage-Specific Survival Data:
| Cancer Stage | Extent of Disease | % Diagnosed at This Stage | 5-Year Survival | 10-Year Survival | Surgery Benefit |
|---|---|---|---|---|---|
| Localized (T1-T2) | Confined to prostate | 69.1% | 100% | 100% | High – surgery often curative |
| Regional (T3) | Spread to nearby tissue/lymph nodes | 20.4% | 99.3% | 96.1% | Moderate – combined with radiation |
| Distant (T4) | Metastasis to bones/organs | 6.2% | 32.3% | 18.5% | Low – palliative only |
| Unknown Stage | Insufficient diagnostic data | 4.3% | 84.6% | 78.1% | Variable – depends on actual stage |
The SEER database confirms that early detection through PSA screening dramatically improves prostate surgery outcomes—nearly 70% of men are diagnosed at the localized stage when surgery achieves functional cure rates approaching 100%.
Real Complication Rates Surgeons Don’t Advertise
Prostate surgery complications vary dramatically by technique, surgeon experience, and whether nerve-sparing approaches are possible. Most surgical consultations emphasize success while minimizing side effect discussions—creating unrealistic expectations that damage trust when complications occur.
Honest Complication Data by Surgery Type:
| Complication | Robotic Prostatectomy | Open Prostatectomy | TURP (BPH) | Factors Affecting Risk |
|---|---|---|---|---|
| Erectile Dysfunction | 20-40% (nerve-sparing) to 70-90% (non-nerve-sparing) | 50-90% | 10-15% | Age, baseline function, nerve preservation, surgeon skill |
| Urinary Incontinence (1 year) | 5-15% | 12-22% | 5-10% | Pelvic floor strength, prostate size, surgical technique |
| Urethral Stricture | 2-5% | 5-8% | 8-14% | Prior surgeries, infection, healing factors |
| Blood Transfusion Need | 2-5% | 10-20% | 3-7% | Prostate size, blood thinners, surgical approach |
| Positive Surgical Margins | 10-15% | 15-20% | N/A | Cancer aggressiveness, surgeon experience, tumor location |
| Rectal Injury | <1% | 1-3% | Rare | Anatomy, prior radiation, surgical technique |
Studies from the National Institutes of Health document that erectile dysfunction after prostate surgery rates vary from 10-69% depending on measurement methods and timeframes. The nerve-sparing prostatectomy technique preserves erectile function in 60-76% of carefully selected patients at 12 months post-surgery, according to research from Johns Hopkins University.
Quality of Life Timeline
Prostate surgery recovery extends far beyond the 2-4 week return-to-work period. True functional recovery—continence and sexual function—unfolds over 6-18 months, with maximum improvement plateauing around 24 months.
Real Recovery Expectations:
Month 1-2: Initial Healing
- Catheter removal week 1-2
- Stress incontinence common (pads required)
- Sexual activity restricted
- Fatigue and discomfort normalizing
Month 3-6: Functional Improvement
- Continence improving to 70-85%
- Light pad usage or pad-free days increasing
- Erectile function returns in 20-40% (if nerve-spared)
- PSA tests confirm cancer elimination
Month 6-12: Continued Recovery
- Continence reaches 85-95%
- Most men pad-free or minimal protection
- Erectile function plateau (may require medications)
- Return to full activities including exercise
Month 12-24: Maximum Recovery
- Final continence levels established
- Sexual function improvements slow/plateau
- Long-term surveillance begins
- Quality of life stabilizes at new baseline
Patient Reality Check
David, 59, underwent robotic prostatectomy performed by a surgeon with 800+ cases. At 18 months post-surgery: PSA undetectable (cancer-free), fully continent without pads, achieving erections sufficient for intercourse 60% of attempts using low-dose Cialis. His outcome represents the upper range of realistic expectations for men with favorable preoperative function and expert surgical care.
What This Means for You
✅ Localized prostate cancer treated with surgery achieves near-100% cure rates, but “cure” doesn’t guarantee complication-free recovery.
✅ Nerve-sparing techniques improve erectile function preservation from 10% to 60-76%, but only work when cancer location permits safe nerve preservation.
✅ Surgeon experience directly correlates with outcomes—the difference between 200 cases versus 500+ cases measurably impacts complication rates.
✅ Men can optimize surgical outcomes by reaching their ideal weight targets before surgery—obesity increases complications 30-40%.
The next section reveals the week-by-week prostate surgery recovery roadmap including evidence-based strategies to accelerate continence return and minimize long-term complications.
Recovery Timeline + Optimization Guide
Prostate Surgery Recovery: Week-by-Week Roadmap
Most prostate surgery recovery articles tell you “return to normal in 4-6 weeks”—a timeline that reflects work capacity, not true functional recovery. The honest truth: catheter after prostate surgery removal marks just the beginning of a 6-12 month continence and sexual function restoration journey.
Marcus, 61, returned to his accounting job four weeks after robotic prostatectomy feeling physically capable. But he hadn’t anticipated the emotional toll of wearing incontinence pads daily for eight more months—a reality his surgeon barely mentioned during pre-operative counseling.
Complete Recovery Timeline by Phase
Week 1-2: Hospital and Early Home Recovery
- Catheter management: Urine may appear bloody or dark red initially—this is normal according to MedlinePlus discharge guidelines
- Activity restrictions: No lifting over 10 pounds, avoid straining during bowel movements
- Pain management: Transition from prescription opioids to acetaminophen within 48-72 hours
- Walking protocol: Start with 10-15 minute walks twice daily, increasing duration as tolerated
- Fatigue peak: Most men require 10-12 hours of sleep nightly during this phase
Week 2-4: Catheter Removal Period
- Catheter removal typically occurs 7-14 days post-surgery (robotic) or 14-21 days (open surgery)
- Initial incontinence: 90-95% of men experience stress incontinence requiring pads when catheter is first removed
- Burning urination: Common for 3-7 days after catheter removal—increase fluid intake to 8-10 glasses daily
- Return to driving: Permitted once off narcotic pain medication and catheter removed
- Work return: Desk jobs feasible at week 3-4; physical labor requires 6-8 weeks minimum
Month 2-3: Active Recovery Phase
- Continence improvement: 60-75% of men achieve daytime continence (0-1 pads daily)
- Light exercise resumed: Walking, stationary cycling, swimming allowed; avoid high-impact activities
- Sexual activity: Cleared to resume at 4-6 weeks, though erectile function may remain impaired
- First PSA test: Scheduled at 6-8 weeks to confirm undetectable levels (<0.1 ng/mL)
Month 4-12: Functional Restoration
- Continence plateau: 85-95% achieve complete continence (pad-free) by 6-12 months
- Erectile function: Gradual return in nerve-spared patients; maximum recovery occurs by 18-24 months
- Physical restrictions lifted: Full exercise capacity including resistance training and sports
- Surveillance schedule: PSA testing every 3-6 months for first two years
Pre-Surgery Optimization (Prehabilitation)
Research from the National Institutes of Health demonstrates that men who complete 4-5 weeks of pelvic floor exercises before prostate surgery achieve continence 30-40% faster than those who begin exercises post-operatively.
4-Week Pre-Surgery Protocol:
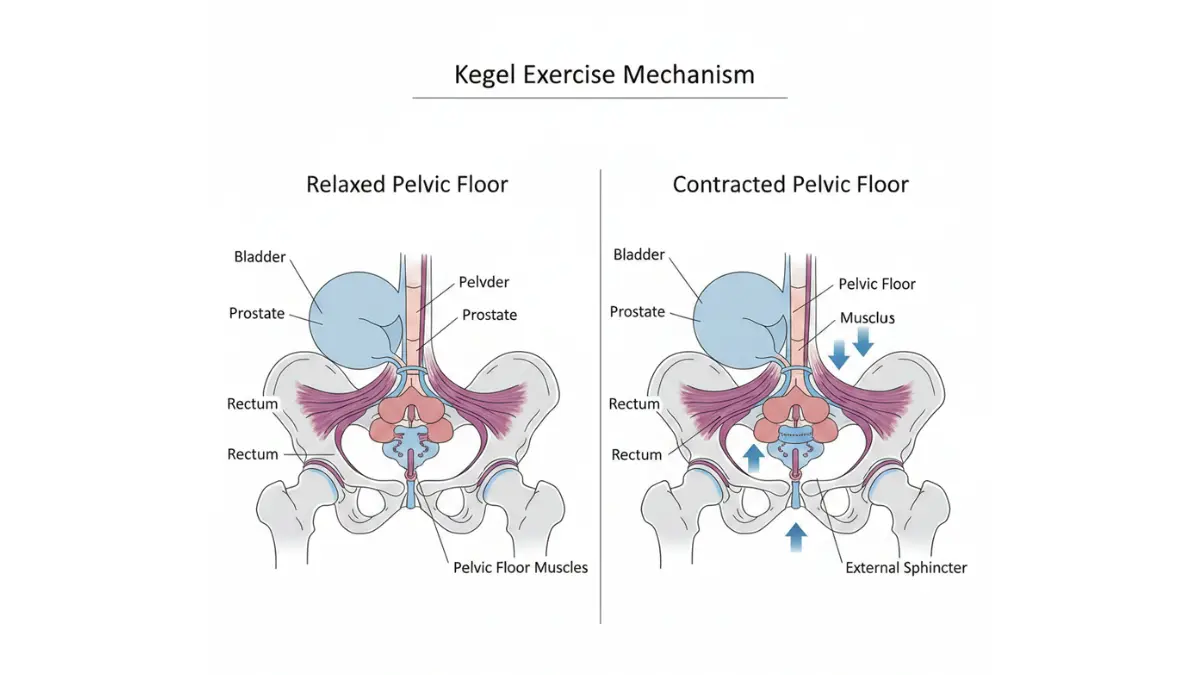
- Pelvic floor muscle training (Kegel exercises):
- Identify correct muscles by stopping urine mid-stream (testing only—don’t do regularly)
- Contract pelvic floor 5-10 seconds, relax 5-10 seconds
- Perform 10 repetitions, 3-4 times daily in different positions (lying, sitting, standing)
- Focus on isolated contractions without tightening buttocks or thighs
- Weight optimization:
- Lose 5-10% body weight if BMI >30 (reduces complications 25-35%)
- Use the Calorie Deficit Calculator to establish safe weight loss targets
- High-protein diet (1.0-1.2g per kg body weight) preserves muscle during weight loss
- Cardiovascular conditioning:
- 30 minutes moderate aerobic activity 5 days weekly
- Improves surgical tolerance and accelerates post-operative recovery
- Monitor intensity using the Heart Rate Zone Calculator
- Smoking cessation:
- Quit minimum 4 weeks before surgery (reduces wound complications 50%)
- Nicotine replacement therapy or prescription cessation aids if needed
Post-Surgery Acceleration Strategies
Studies confirm that men who actively engage in rehabilitation protocols recover function significantly faster than those using passive “wait-and-see” approaches.
Evidence-Based Recovery Accelerators:
- Aggressive pelvic floor training: Perform Kegels 40-50 times daily (10 reps, 4-5 sessions)—reduces pad usage by 40% at 3 months
- Biofeedback therapy: Specialized pelvic floor physical therapy using sensors to optimize muscle contraction technique
- Early mobilization: Walk 2-3 miles daily by week 3-4; reduces fatigue and improves continence
- Adequate hydration: 64-80oz fluid daily maintains bladder health and reduces stricture risk (track with Water Intake Calculator)
- Protein optimization: 1.2-1.5g per kg body weight accelerates tissue healing (calculate needs with Protein Intake Calculator)
- Sleep prioritization: 8+ hours nightly supports hormonal recovery and tissue repair (optimize sleep cycles with Sleep Calculator)
Penile Rehabilitation Protocol (for nerve-spared patients):
- Daily low-dose PDE5 inhibitor (Cialis 5mg or Viagra 25-50mg) starting 4-6 weeks post-surgery
- Vacuum erection device usage 3-4 times weekly to maintain penile oxygenation
- Early return to sexual activity (even without full erections) maintains tissue health
What This Means for You
✅ Prostatectomy recovery extends 6-12 months for continence and up to 24 months for sexual function—anyone promising faster results is overselling.
✅ Pelvic floor prehabilitation starting 4-5 weeks before surgery reduces incontinence duration by 30-40% compared to starting exercises post-operatively.
✅ Men with similar surgical approaches need comparable recovery support—explore related information in our prostate surgery comprehensive guide.
The final section reveals how to choose the right surgeon—including the specific questions that separate high-performing surgeons from average practitioners.
Decision Framework + Choosing Your Surgeon
Choosing the Right Prostate Surgery: Your Decision Roadmap
The prostate surgery versus radiation therapy debate dominates online forums, yet the answer depends entirely on individual cancer characteristics and life priorities. Kenneth, 58, spent three months agonizing over treatment options before realizing his surgeon’s experience mattered more than the technique itself.
Most men make this decision in 4-8 weeks—adequate time for thorough evaluation without delaying treatment outcomes.
Surgery vs Radiation vs Active Surveillance
The “best” prostate cancer treatment varies by cancer stage, age, overall health, and personal priorities regarding side effect trade-offs. No single approach dominates all scenarios.
Treatment Decision Matrix:
| Factor | Surgery Best Choice | Radiation Therapy Best | Active Surveillance Best |
|---|---|---|---|
| Age/Life Expectancy | <70 years, >10 year life expectancy | 65-80 years, 10-15 year life expectancy | >75 years or <10 year life expectancy |
| Cancer Stage | T1-T2 (localized, confined) | T2-T3 (locally advanced) | Very low or low risk only |
| Gleason Score | 6-7 (3+4) | 7 (4+3) to 9 | 6 or lower |
| PSA Level | <10-20 ng/mL | 10-20+ ng/mL | <10 ng/mL |
| Priority | One-time definitive treatment | Avoid surgery/anesthesia | Minimal immediate intervention |
| Side Effect Concern | Willing to accept upfront risks for definitive cure | Prefer gradual side effects | Preserve current quality of life |
| 10-Year Cancer Control | 95-99% | 93-97% | 95%+ (carefully selected patients) |
Radiation therapy allows salvage surgery if cancer recurs, but prostate surgery followed by radiation salvage proves technically more challenging. This directional difference influences sequencing decisions when multiple treatments may ultimately be needed.
Critical Surgeon Selection Questions
Surgeon experience directly predicts your complication rates more than any other controllable factor. Men who ask these questions separate high-performing surgeons from average practitioners.
Essential Pre-Surgical Consultation Questions:
- “How many of THIS specific procedure have you personally performed?”
Target: Minimum 200-300 cases for robotic; 150+ for open prostatectomy - “What are YOUR personal complication rates—specifically incontinence, erectile dysfunction, and positive margins?”
Red flag: Surgeon hesitates or only cites published literature averages - “Can you perform nerve-sparing prostatectomy on my specific tumor location?”
Clarifies erectile function preservation feasibility based on cancer position - “What percentage of your cases are completed robotically vs converted to open?”
Conversion rates >5% suggest inadequate robotic experience - “How do you handle intraoperative complications?”
Tests surgeon’s transparency and contingency planning - “What does your post-operative follow-up schedule look like?”
Reveals commitment to long-term outcome tracking - “Can you connect me with 2-3 past patients willing to share their experience?”
Best surgeons maintain patient ambassador programs
Surgeon Red Flags vs Green Flags
🚩 Warning Signs to Avoid:
- Surgeon performs <50 prostatectomies annually (low-volume practice)
- Refuses to discuss personal complication statistics
- Pressures immediate scheduling without allowing second opinion time
- No affiliation with accredited cancer center or tumor board
- Dismisses alternative treatments (radiation, surveillance) without discussion
✅ High-Quality Indicators:
- Board certification in urologic oncology, not just general urology
- Fellowship training specifically in robotic or oncologic surgery
- Annual case volume >100 prostatectomies (or >75 for less common procedures)
- Published research or teaching role at academic institution
- Transparent outcome reporting and willingness to share statistics
- Multidisciplinary team involvement (radiation oncology, medical oncology available)
What This Means for You
✅ Surgeon experience matters more than hospital reputation—a skilled surgeon at a community hospital outperforms an inexperienced surgeon at a prestigious academic center.
✅ Second opinions are standard practice for cancer treatment—insurance covers consultations at multiple centers without requiring commitment.
✅ Men concerned about genetic factors influencing surgical outcomes should complete the Genetic Risk Assessment Tool before consultations.
✅ The decision timeline typically spans 4-8 weeks—anyone rushing you faster warrants scrutiny, but delaying beyond 12 weeks risks unnecessary cancer progression.
For comprehensive prostate cancer management guidance beyond surgery, explore our health resources covering cancer detection.
Final Considerations
Prostate surgery in 2026 achieves remarkable cure rates approaching 100% for localized disease, but success extends beyond cancer elimination to encompass quality of life preservation. The $7,500-$27,000 cost investment delivers maximum value when combined with careful surgeon selection, realistic expectation setting, and proactive rehabilitation engagement.
The 97% cure rate headline promises hope—but only surgeons performing 200+ cases annually consistently deliver those results with minimal complications. Choose your surgeon as carefully as you choose the procedure itself.
Medical Disclaimer
This article is for educational purposes only and does not constitute medical advice. Prostate surgery decisions should be made in consultation with board-certified urologists after comprehensive evaluation including PSA testing, prostate biopsy, imaging studies, and review of individual cancer pathology. Success rates, complication risks, and recovery timelines vary significantly based on patient age, cancer stage, overall health, and surgeon experience. Always discuss your specific medical situation with qualified healthcare providers before making treatment decisions.
Frequently Asked Questions About Prostate Surgery
1. How much does prostate surgery cost in 2026?
Prostate surgery costs range from $7,500-$27,000 in the United States depending on procedure type. Robotic prostatectomy averages $15,000-$27,000, while TURP for BPH costs $7,500-$15,000. Insurance typically covers 80-100% after deductibles for cancer surgery.
2. What is the success rate of prostate surgery?
Localized prostate cancer (Stage T1-T2) achieves 96-100% five-year survival rates with surgery. Regional stage cancer shows 99.3% five-year survival, while distant metastatic disease drops to 32.3%. Overall prostate cancer surgery delivers 97.9% five-year survival across all stages combined.
3. How long does it take to recover from prostate surgery?
Initial recovery takes 2-4 weeks to return to desk work after robotic prostatectomy, or 4-8 weeks after open surgery. Full functional recovery including continence takes 6-12 months, while erectile function may require 12-24 months to plateau. Most men resume normal activities by 6-8 weeks post-surgery.
4. Is robotic prostate surgery better than open surgery?
Robotic prostatectomy offers faster recovery (2-4 weeks vs 4-8 weeks), less blood loss (66% reduction), and shorter hospital stays (1-2 days vs 2-3 days). However, 10-year cancer cure rates are statistically equivalent between approaches. Surgeon experience matters more than technique selection.
5. Will I be incontinent after prostate surgery?
Initial incontinence affects 90-95% of men immediately after catheter removal but improves rapidly. At 12 months post-surgery, 85-95% of men achieve complete continence (pad-free) with robotic surgery versus 80-90% with open surgery. Pelvic floor exercises accelerate recovery by 30-40%.
6. Can I still have erections after prostate removal?
Erectile function preservation depends on nerve-sparing technique feasibility and patient age. Nerve-sparing robotic prostatectomy preserves erections in 60-76% of men at 12 months, while non-nerve-sparing surgery reduces this to 10-20%. PDE5 inhibitors (Viagra, Cialis) improve outcomes significantly.
7. Does Medicare cover prostate surgery?
Medicare Part B covers medically necessary prostate surgery at 80% after the annual deductible ($240 in 2026). Patients pay 20% coinsurance unless they have supplemental coverage. Medicare Advantage plans often cover 100% at in-network facilities after reaching out-of-pocket maximums ($8,850 in 2026).
8. How do I choose the best prostate surgeon?
Select surgeons performing 200+ prostatectomies annually with transparent complication statistics. Ask about personal incontinence rates (<15% at 1 year), positive surgical margin rates (<15%), and nerve-sparing success rates. Board certification in urologic oncology and fellowship training are essential qualifications.
9. What is the difference between prostate surgery and radiation?
Surgery removes the entire prostate in one procedure with immediate side effects (incontinence, erectile dysfunction) that improve over 6-12 months. Radiation therapy delivers treatment over 6-8 weeks with gradual side effects developing over 1-3 years. Both achieve 95-99% ten-year cancer control for localized disease.
10. How long does the catheter stay in after prostate surgery?
Catheters remain in place 7-14 days after robotic prostatectomy or 14-21 days after open surgery. TURP procedures typically require 1-3 days of catheterization. Catheter removal marks the start of active continence recovery, with most men requiring pads for 2-12 weeks post-removal.
11. Can prostate cancer come back after surgery?
Prostate cancer recurrence occurs in 10-30% of cases depending on initial stage and surgical margins. PSA levels should drop to undetectable (<0.1 ng/mL) within 6-8 weeks post-surgery. Rising PSA during surveillance indicates biochemical recurrence, which can be treated with salvage radiation therapy achieving 60-80% long-term control.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.