On This Page – Quick Medical Summary
Watching the weight fall away — your own or a loved one’s — is one of the most frightening parts of pancreatic cancer. It often happens fast, and eating more rarely stops it. That is not a personal failing; it is biology, and understanding it is the first step toward managing it.
This guide explains why pancreatic cancer weight loss happens and what genuinely helps. If you are newly diagnosed, start with how common it is and why it occurs. If you are a caregiver, the sections on nutrition support and warning signs matter most. If you are worried about unexplained weight loss and your own risk, the section on weight loss as an early sign — especially with new-onset diabetes — is for you. For the bigger picture, see our pillar guide to understanding pancreatic cancer from first signs to treatment.
ℹ️ Medical Disclaimer: This article is educational and not a substitute for professional medical advice, diagnosis, or treatment. Pancreatic cancer, exocrine pancreatic insufficiency, enzyme replacement therapy, and the medications mentioned here must be managed by your own care team. Consult a board-certified oncologist or gastroenterologist before acting on anything here, and seek urgent care for the warning signs below.
How common is weight loss in pancreatic cancer?
Weight loss affects the large majority of people with pancreatic cancer, often before any other clue. Across studies, around 85% of patients show a measurable drop in body weight, sometimes at the moment of diagnosis. If this is happening, you are in the majority — it is expected, not a sign you did something wrong.
📊 Clinical Data Point: About 85% of pancreatic cancer patients experience a reduction in body weight, often by the time of diagnosis. — Source: peer-reviewed review, Pancreatic Cancer and Cachexia: Metabolic Mechanisms, 2020.
Weight loss versus cancer cachexia
Ordinary weight loss can sometimes be reversed by eating more; cancer cachexia — a wasting of muscle and fat driven by the cancer itself — usually cannot. It affects up to 80% of pancreatic cancer patients, among the highest of any cancer type, and one study found 71% met the formal definition.
The broader context
Pancreatic cancer itself is relatively uncommon — about 67,530 new U.S. cases are projected for 2026 in national incidence and survival data. Within the disease, weight loss is the rule, sitting alongside other symptoms of pancreatic cancer such as jaundice and abdominal pain.
Why does pancreatic cancer cause weight loss?
Pancreatic cancer causes weight loss through four overlapping mechanisms: cancer cachexia, poor digestion from exocrine pancreatic insufficiency, reduced food intake, and the tumor’s own high energy use. Usually more than one is at work, which is why eating more alone rarely reverses it.
Cancer cachexia: the body’s wasting response
🔬 How It Works: In cachexia, the tumor and immune system release inflammatory cytokines such as IL-6 and TNF-α that switch the body into a breakdown state. TNF-α drives muscle breakdown directly through the cell’s protein-disposal system while resting energy use climbs — so muscle and fat are lost even when calorie intake looks adequate.
The key insight: cachexia is metabolic, not simply eating too little. By definition, it is a wasting syndrome that standard nutrition alone cannot fully reverse.
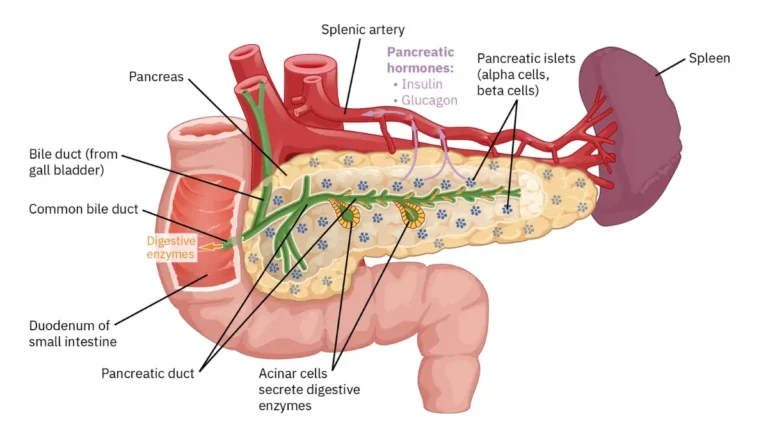
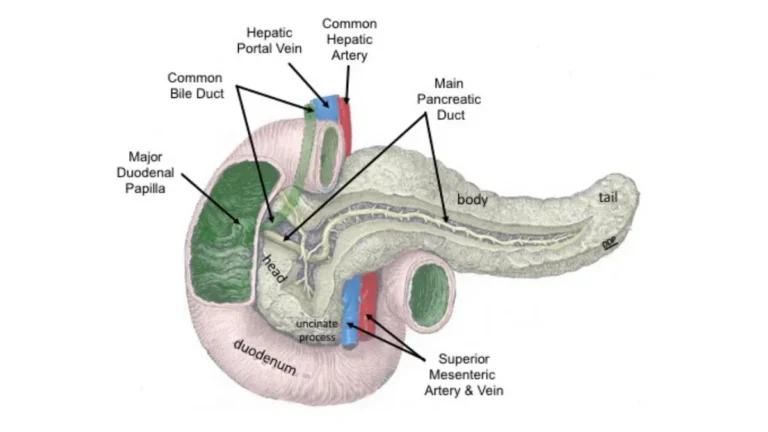
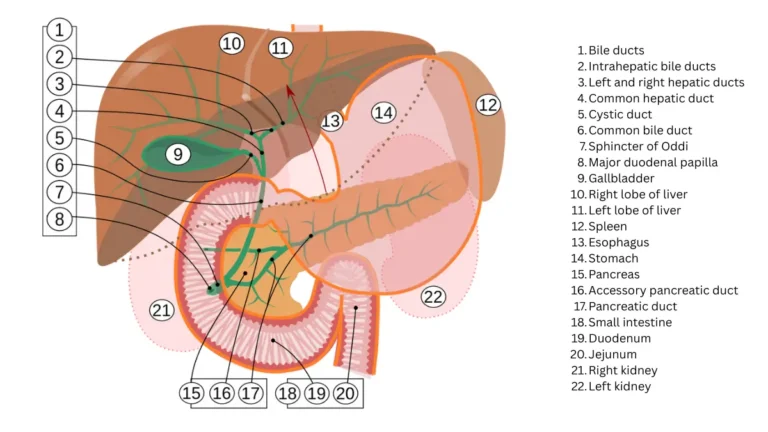
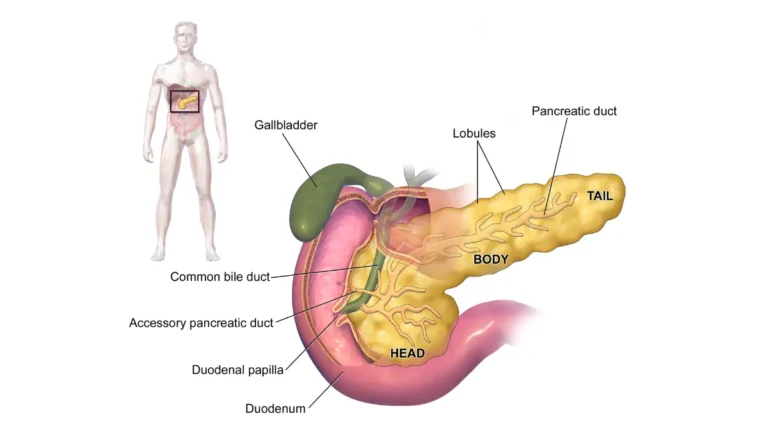
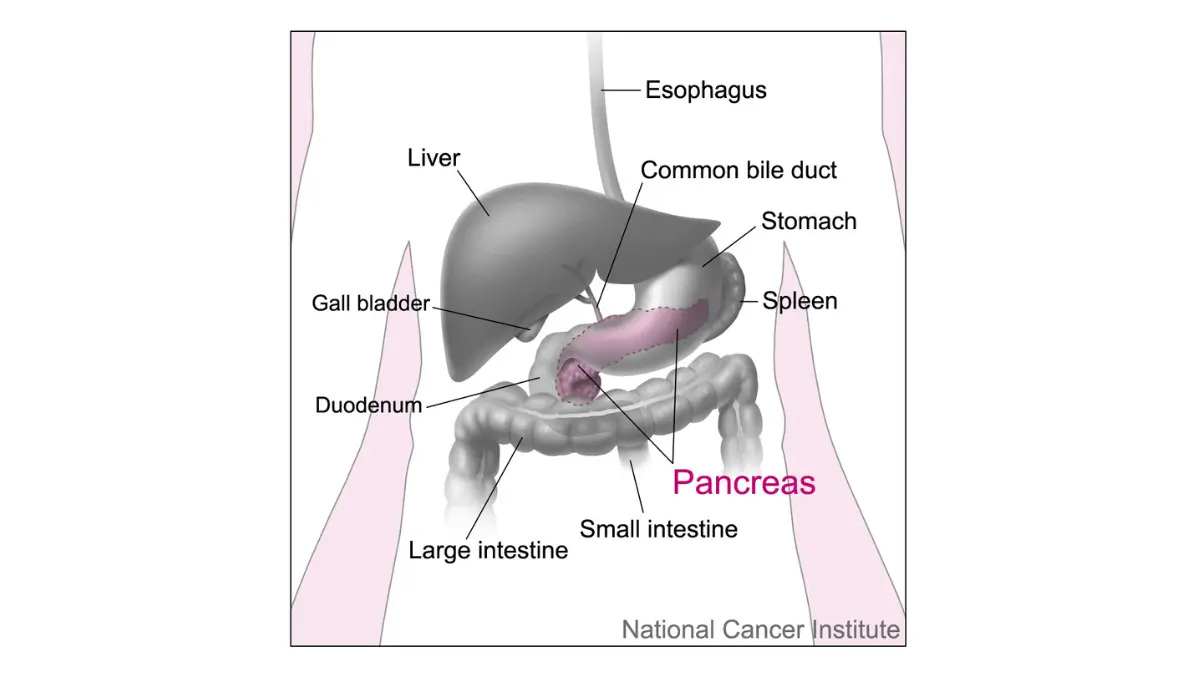
Exocrine pancreatic insufficiency: when food isn’t broken down
The pancreas makes the enzymes that digest fat, protein, and carbohydrate. When a tumor blocks the pancreatic duct or destroys working tissue, those enzymes no longer reach the gut — exocrine pancreatic insufficiency, or EPI. Food then passes through partly undigested, and stools may turn pale, oily, bulky, and hard to flush. EPI affects 66–92% of patients, and overt maldigestion typically appears only after about 90% of enzyme output is lost — so it can be advanced before it is obvious.
Reduced intake and the tumor’s metabolism
Appetite loss is common, sometimes with a specific aversion to meat; nausea, early fullness, and treatment-related taste changes cut intake further, while the tumor consumes energy and nutrients rapidly. In advanced disease, anorexia affects around 83% of patients.
| Driver | What happens in the body | What it can feel like | Key clinical detail |
|---|---|---|---|
| Cancer cachexia | Inflammatory signals break down muscle and fat; energy use rises | Steady muscle and weight loss despite eating | Metabolic — not reversed by calories alone |
| Exocrine pancreatic insufficiency | Tumor blocks or destroys enzyme-producing tissue, so food isn’t digested | Pale, oily, floating stools; bloating | Often advanced before symptoms show |
| Reduced food intake | Appetite loss, nausea, early fullness, taste changes | Eating less; feeling full fast; meat aversion | Treatment side effects can add to this |
| Tumor metabolism | The cancer consumes energy and nutrients rapidly | Ongoing depletion even with some eating | Compounds the other three drivers |
Sources: peer-reviewed reviews in the Journal of Cachexia, Sarcopenia and Muscle (2024) and Nutrients (2025); EPI prevalence from a systematic review/meta-analysis (2020). See citations in text.
Can weight loss be an early sign of pancreatic cancer?
Unexplained weight loss can be an early sign of pancreatic cancer, especially alongside new-onset diabetes in an older adult who is not trying to lose weight. On its own it has many causes, most of them not cancer — but one specific pattern is worth raising with a doctor.
Most new diabetes is ordinary type 2: fewer than 1 in 100 new-diabetes cases are caused by cancer. Yet about 1 in 4 people later diagnosed with pancreatic cancer were first diagnosed with diabetes.
📊 Clinical Data Point: About 1 in 4 people with pancreatic cancer were first diagnosed with diabetes; fewer than 1 in 100 new-onset diabetes cases are caused by cancer. — Source: NCI research on new-onset diabetes as an early sign, 2021.
The pattern that matters is three features together: older age, rapidly rising blood sugar, and unintentional weight loss. Research links recent-onset diabetes plus weight loss to roughly a six-fold higher risk of pancreatic cancer.
⚠️ Clinical Warning: New-onset diabetes with unexplained weight loss in someone over 60 — especially at a healthy weight beforehand and not dieting — warrants prompt evaluation. UK NICE guidance recommends abdominal imaging in exactly this situation.
✅ Patient Action: If you have developed diabetes recently and are losing weight without trying, ask your primary care doctor or a gastroenterologist: “Should I have abdominal imaging to rule out a pancreatic cause?” You can also review new-onset diabetes and pancreatic cancer and the earliest signs of pancreatic cancer beforehand.
What helps with pancreatic cancer weight loss?
Weight loss in pancreatic cancer can often be slowed or stabilized, even if not always fully reversed. The most effective steps target the specific causes — replacing missing enzymes, expert nutrition support, and making each bite count.
Pancreatic enzyme replacement therapy (PERT)
If EPI is part of the picture, pancreatic enzyme replacement therapy (PERT) supplies the enzymes the pancreas can no longer deliver, so food is absorbed instead of passing through. In advanced disease, PERT is linked to weight gain and, in a pooled analysis, a survival benefit of roughly 3.8 months — yet it is often under-prescribed.
📊 Clinical Data Point: In advanced pancreatic cancer, enzyme replacement therapy was associated with a survival benefit of about 3.8 months (95% CI 1.4–6.2). — Source: systematic review and meta-analysis of enzyme replacement therapy, 2020.
⚠️ Clinical Warning: Enzyme doses are individualized and must be set by your prescriber — not started or adjusted on your own.
✅ Patient Action: Ask your oncology team: “Could exocrine pancreatic insufficiency be contributing to this weight loss, and would enzyme replacement therapy help?”
Work with an oncology dietitian
This is the single highest-value referral, because unmanaged malnutrition can itself progress to cachexia. A dietitian sets individualized calorie and protein targets. You can estimate everyday protein needs as a starting point, but cancer-related needs are often higher — treat any calculator as a conversation-starter, not a plan.
Practical eating strategies
National Cancer Institute guidance offers evidence-based tips for appetite and weight loss during cancer: small, frequent, high-calorie and high-protein meals; protein first while appetite is strongest; smoothies or oral nutrition supplements when solids are hard; and the largest meal whenever appetite peaks, not by the clock.
When is weight loss a warning sign to call your team?
Some changes alongside weight loss need prompt medical attention rather than a wait-and-see approach.
Red-flag symptoms
- Inability to keep food or fluids down, or persistent vomiting
- New or worsening jaundice — yellowing of the skin or eyes — which can signal a blocked bile duct
- Rapid, ongoing weight loss with weakness or dehydration, such as dizziness, dark urine, or passing little urine
- Severe or worsening abdominal or back pain
A tumor blocking the stomach’s outlet occurs in about 5–10% of newly diagnosed cases, causing nausea, vomiting, and worsening intake. Yellowing of the skin or eyes is covered in our guide to jaundice as a pancreatic cancer warning sign.
⚠️ Clinical Warning: If you cannot keep food or fluids down, develop yellowing of the skin or eyes, or are losing weight rapidly with signs of dehydration, contact your care team promptly or seek urgent care.
Why acting early matters
Unmanaged malnutrition reduces the body’s ability to tolerate chemotherapy and stay on schedule. Addressing weight loss early helps protect those treatment options.
✅ Patient Action: Keep a weekly weight log, bring it to appointments, and report a fast drop right away rather than waiting for the next scheduled visit.
What does weight loss mean for pancreatic cancer outcomes?
It is natural to wonder what weight loss means for the road ahead. The honest answer: it matters, but it is not the whole story, and it is partly within your control.
Weight loss, cachexia, and survival
In a systematic review of pancreatic and colorectal cancer, weight loss or cachexia was linked to poorer survival in nearly two-thirds of studies, and in one pancreatic cohort more severe loss tracked with shorter median survival — 12 versus 16 months. Overall, pancreatic cancer’s 5-year relative survival is about 13%, but markedly higher when the cancer is found while still confined to the pancreas.
📊 Clinical Data Point: Pancreatic cancer 5-year relative survival is about 13% overall and about 44% for localized disease. — Source: American Cancer Society survival statistics by stage, 2026, drawing on NCI SEER data.
These figures describe large populations, not individuals.
Why managing it still matters
Because it is partly modifiable: enzyme replacement and nutrition support are linked to weight gain, better treatment tolerance, and a measurable survival benefit. It is one of the few levers genuinely within reach.
Frequently asked questions about pancreatic cancer weight loss
1. How much weight do pancreatic cancer patients usually lose?
Most lose weight: around 85% show a measurable drop, often present by diagnosis, and up to 80% develop cancer cachexia — a wasting of muscle and fat. Near the end of life, average loss can reach roughly a quarter of pre-illness weight. The amount varies widely with tumor location and stage.
2. Why can’t eating more reverse pancreatic cancer weight loss?
Because two main drivers aren’t fixed by calories alone. Cancer cachexia is a metabolic state that breaks down muscle and fat regardless of how much you eat, and exocrine pancreatic insufficiency leaves food partly undigested. Both usually need targeted treatment — such as enzyme replacement and dietitian support — not simply more food.
3. What is cancer cachexia in simple terms?
Cancer cachexia is a wasting syndrome in which the cancer and immune system drive ongoing loss of muscle and fat, along with weakness and appetite loss. It can continue even when you eat well, because it is metabolic rather than purely nutritional, and standard nutrition alone usually cannot fully reverse it.
4. Can weight loss be the first sign of pancreatic cancer?
It can. Unexplained weight loss is a recognized early symptom, and about 1 in 4 people with pancreatic cancer were first diagnosed with diabetes. That said, most weight loss has other, more common causes, so see a doctor to identify yours rather than assuming the worst.
5. Does new-onset diabetes with weight loss always mean cancer?
No. Fewer than 1 in 100 new diabetes cases are caused by cancer. But new diabetes combined with unintentional weight loss in someone older and not dieting is a pattern worth checking, and guidelines suggest abdominal imaging. Ask your doctor whether that evaluation is appropriate for your situation.
6. What is PERT, and can it help with weight loss?
Pancreatic enzyme replacement therapy (PERT) supplies the digestive enzymes a damaged pancreas can no longer make, so food is absorbed instead of wasted. In advanced disease it is linked to weight gain and a modest survival benefit. Dosing is individualized, so ask your prescriber whether it is right for you.
7. What foods help during pancreatic cancer treatment?
Small, frequent, high-calorie and high-protein meals help most — eat protein first while your appetite is strongest, and use smoothies or oral nutrition supplements when solid food is hard. An oncology dietitian can tailor this to your needs, which is the most effective single step; ask your team for a referral.
8. Can pancreatic cancer weight loss be slowed or stopped?
Often yes — it can frequently be slowed or stabilized, even if not always reversed. Replacing enzymes, working with a dietitian, and concentrating calories together address the main causes. Starting early, before significant muscle is lost, gives the best chance of holding weight. Discuss a plan with your care team.
9. When is weight loss a medical emergency?
Contact your care team promptly if you cannot keep food or fluids down, develop new yellowing of the skin or eyes, or lose weight rapidly with signs of dehydration such as dizziness and dark urine. These can signal a blockage or dehydration that needs urgent medical attention rather than waiting.
10. Does losing weight mean the cancer is worse?
Not necessarily, but it is worth taking seriously. Weight loss and cachexia are linked to poorer outcomes in roughly two-thirds of studies, and more severe loss tracks with shorter survival. It is also partly modifiable, so managing it is genuinely worthwhile. Discuss any rapid change with your care team.
11. Should I see a dietitian for pancreatic cancer weight loss?
Yes — an oncology dietitian is one of the highest-value referrals available. Unmanaged malnutrition can progress to cachexia and reduce your ability to tolerate treatment. A dietitian sets individualized calorie and protein targets and adjusts them as your needs change. Ask your oncology team for a referral.
Key takeaways
Pancreatic cancer weight loss happens for real, identifiable reasons — cancer cachexia, poor digestion from enzyme loss, reduced intake, and the tumor’s high energy demand — usually several at once. That is why eating more alone rarely fixes it, and why it is never a personal failing.
The encouraging part is how much is within reach. Replacing missing enzymes, partnering with an oncology dietitian, and concentrating calories and protein can slow or steady the loss and help the body tolerate treatment. Two steps matter most: ask your team whether enzyme replacement and a dietitian referral are right for you, and act promptly on the warning signs above. You do not have to navigate this alone.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Internal Medicine (2010); Clinical Pharmacology (2013) Experience: 15 years | Location: San Francisco, California Education: BS Molecular Biology, Caltech (2000); MD/PhD, UCSF School of Medicine (2007);…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.