On This Page – Quick Medical Summary
If you or someone you love has just been handed a pancreatic cancer stage, the number can feel like a verdict. It isn’t one. A stage is a description — shorthand for how much cancer is present and where — and understanding what yours means is the first step toward clear decisions.
This guide is built for three situations. If you were just diagnosed and want to know what your stage describes, start with the stage-by-stage walkthrough below. If you are weighing treatment and wondering whether surgery is possible, the section on resectability matters most. If you are a caregiver or comparing survival numbers you found online, the statistics section explains what those figures do — and don’t — say about one person.
One thing to know up front: you will run into three different “staging languages.” Your pathology report may show a number from 0 to IV. The survival statistics online use a separate grouping — localized, regional, or distant. And your oncologist plans treatment around a third idea entirely: whether the tumor can be removed. This article connects all three, so nothing you read sends you to the wrong conclusion. For the wider picture, see our full guide to pancreatic cancer symptoms and stages.
ℹ️ Medical Disclaimer: This article is general health education — not medical advice — and does not diagnose disease, recommend treatment, or replace your care team. Pancreatic cancer staging, treatment decisions, survival estimates, and clinical-trial eligibility are individual to you and depend on findings only your doctors can interpret. Before acting on anything here, consult a board-certified medical oncologist or surgical oncologist who knows your case.
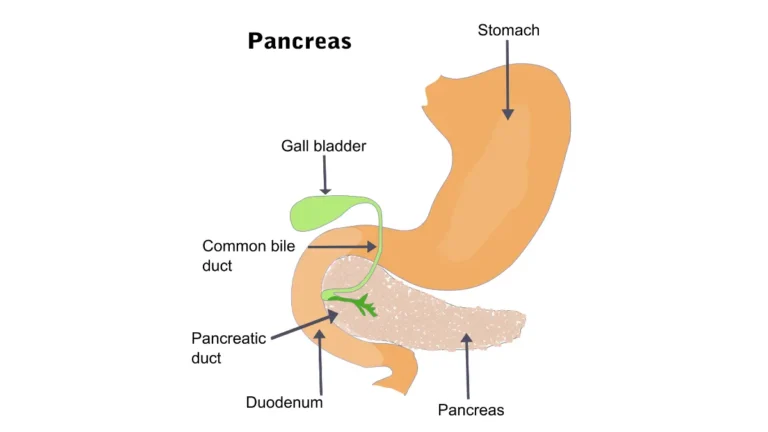
How pancreatic cancer is staged: the TNM system
Doctors describe pancreatic cancer using the TNM staging system from the American Joint Committee on Cancer, now in its 8th edition. It answers three questions and combines the answers into one overall stage.
What the T, N, and M mean
Each letter captures one part of the picture:
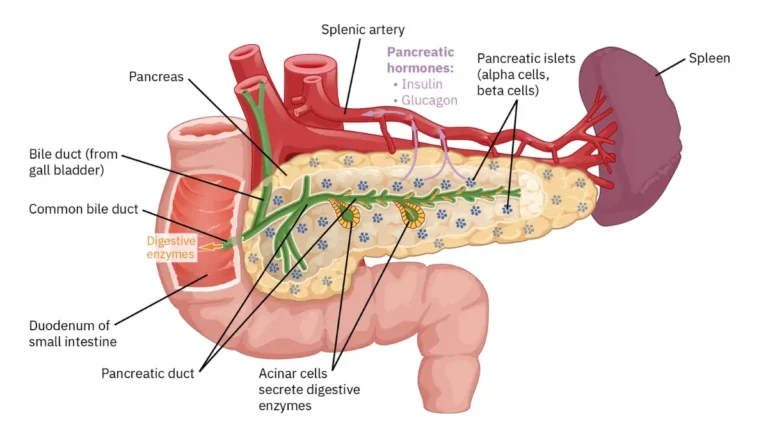
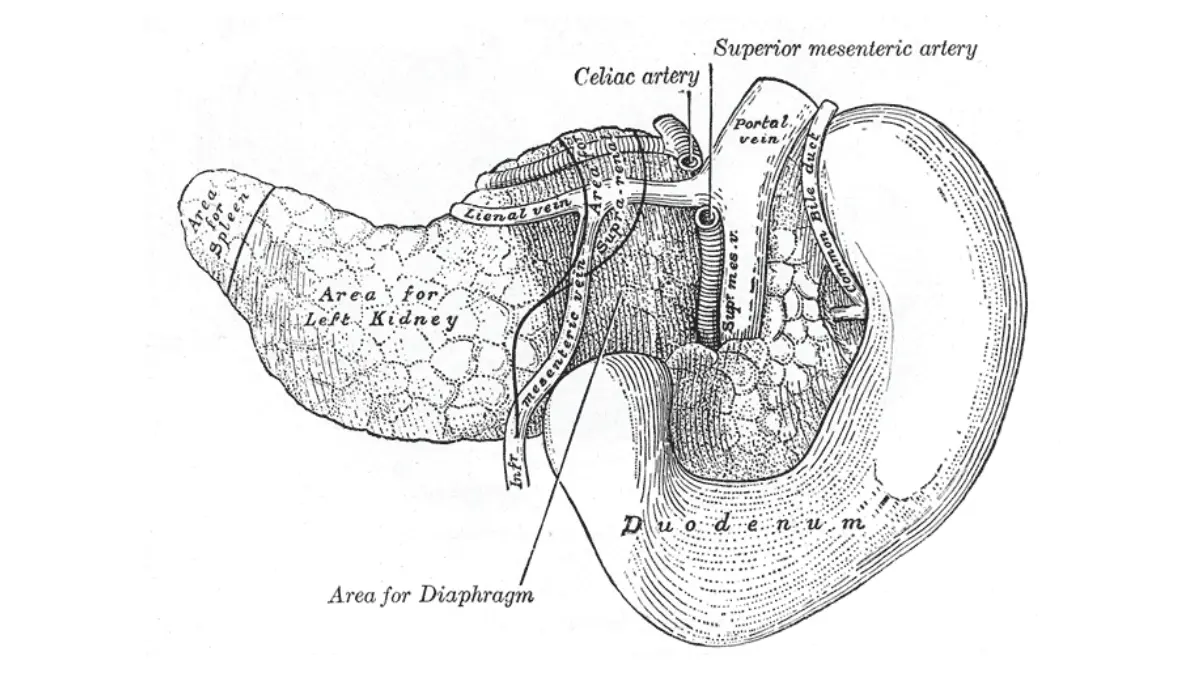
- T (tumor): how large the tumor is and whether it has grown into nearby arteries. T1 is 2 cm or smaller, T2 is larger than 2 up to 4 cm, T3 is larger than 4 cm, and T4 means the tumor involves major arteries — the celiac axis, superior mesenteric artery, or common hepatic artery — regardless of size.
- N (nodes): whether cancer has reached nearby lymph nodes. N0 is none, N1 is 1 to 3 nodes, N2 is 4 or more.
- M (metastasis): whether cancer has spread to distant organs. M0 is no; M1 is yes.
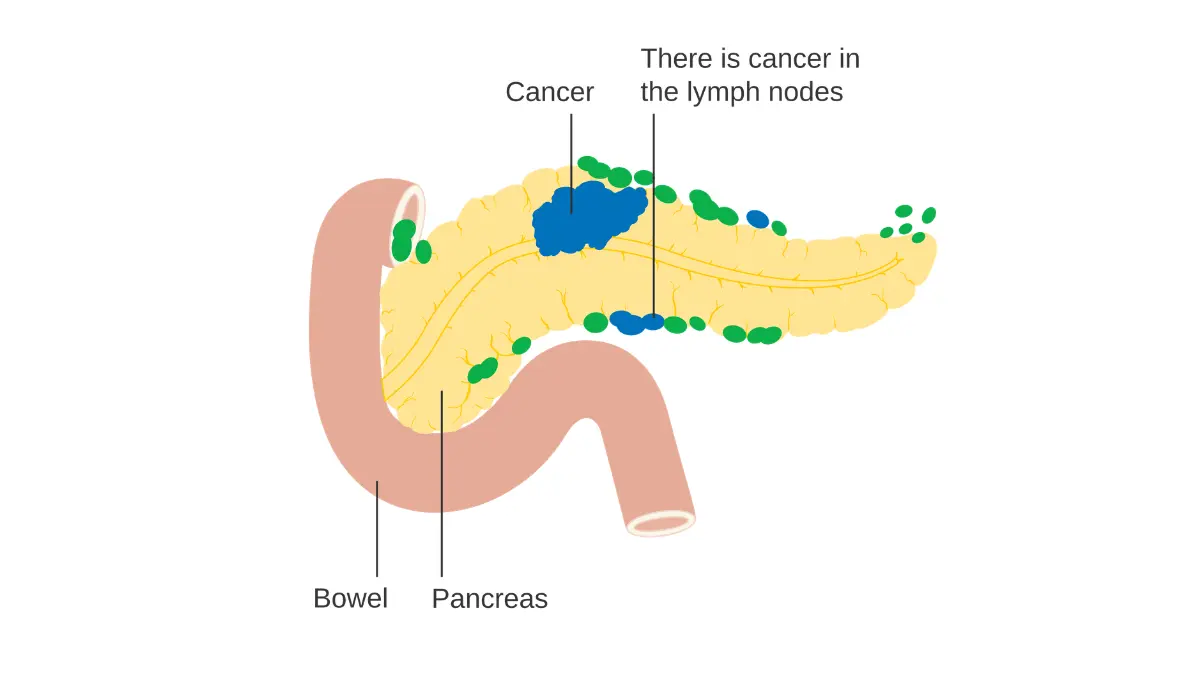
Adapted from Wikimedia Commons Diagram showing pancreatic cancer in the lymph nodes (N staging) CRUK 178, licensed under Creative Commons Attribution-Share Alike 4.0 International license.
🔬 How It Works: Your T, N, and M are combined into a single Roman-numeral stage through a step called stage grouping. Your team assigns each letter from imaging, biopsy, and — if you have surgery — the tissue removed, then maps that combination to a stage from 0 to IV.
Stages 0 through IV at a glance
In plain terms: stage 0 is confined to the duct lining; stages I and II are limited to or near the pancreas; stage III is locally advanced; and stage IV has spread to distant organs. The American Cancer Society’s staging overview lays out the full grouping table if you want to match your exact T, N, and M.
What each stage means, from stage 0 to stage 4
Your stage number is more useful once you know what it describes about the cancer itself.
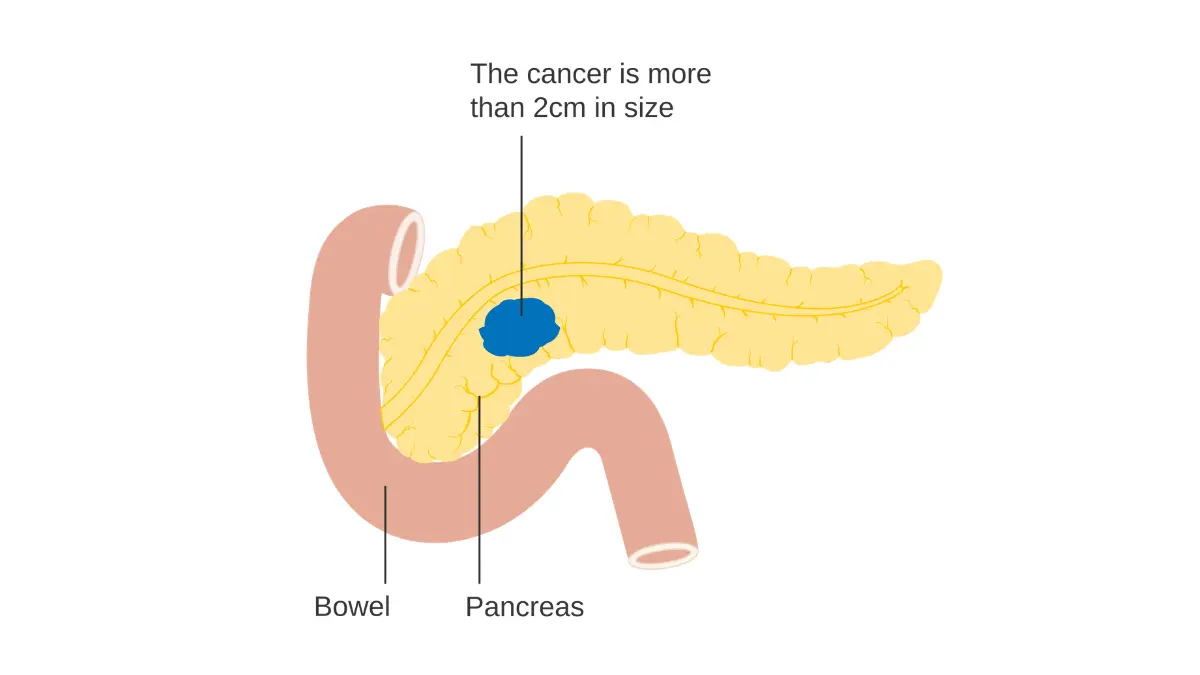
Adapted from Wikimedia Commons Diagram showing stage T2 cancer of the pancreas CRUK 254, licensed under Creative Commons Attribution-Share Alike 4.0 International license.
Stages 0, I, and II: confined or nearby
Stage 0 (carcinoma in situ) means abnormal cells sit only in the lining of the pancreatic duct and have not invaded deeper — it is rarely caught this early. Stage I is an invasive tumor still limited to the pancreas: IA is 2 cm or smaller, IB is larger. Stage II is either a tumor over 4 cm with no node involvement (IIA), or a tumor that has reached 1 to 3 nearby lymph nodes (IIB).
Stage III: locally advanced
Stage III means the cancer is locally advanced. Either the tumor has grown into major nearby arteries (T4), or it has spread to 4 or more regional lymph nodes — but it has not reached distant organs. Stage III tumors often fall into the “borderline resectable” or “unresectable” categories covered next.
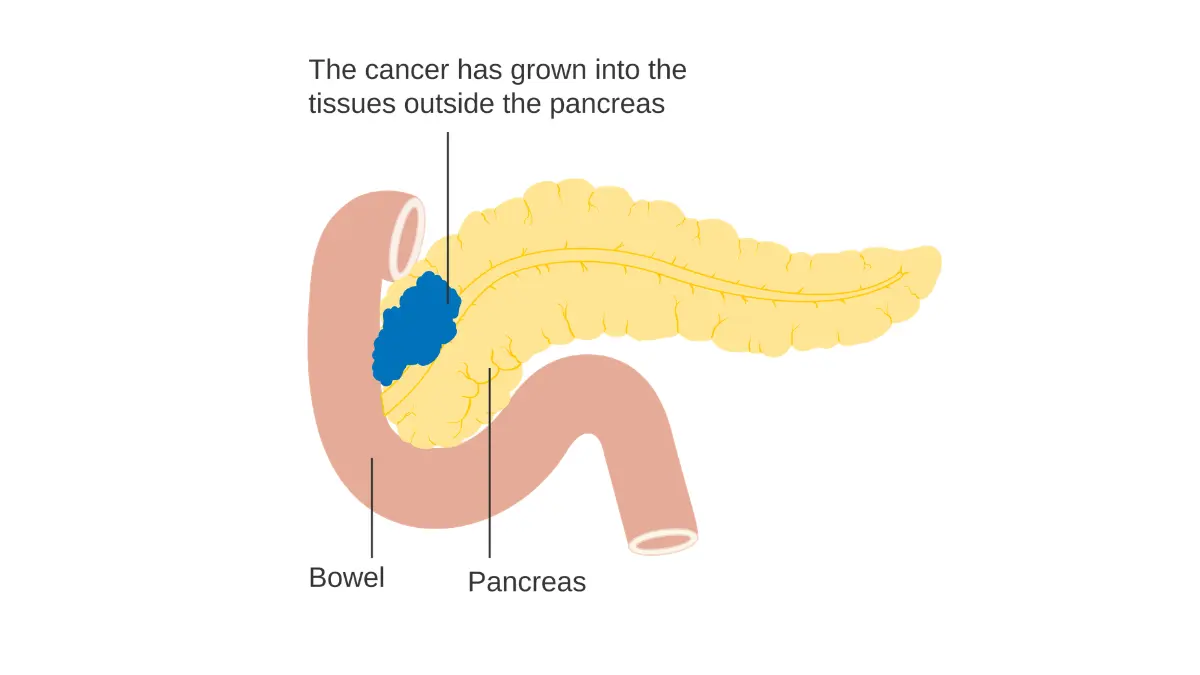
Adapted from Wikimedia Commons Diagram showing stage T3 cancer of the pancreas CRUK 261, licensed under
Stage IV: metastatic (often searched as “stage 4”)
Stage IV means the cancer has spread to distant parts of the body — most often the liver, the lining of the abdomen (peritoneum), or the lungs. It is the most advanced stage and the one most people mean when they search “stage 4.” A stage IV diagnosis is serious, but it describes where the cancer is — not a fixed timeline for any individual. Treatment here focuses on controlling the cancer, easing symptoms, and protecting quality of life, and the options have expanded in recent years.
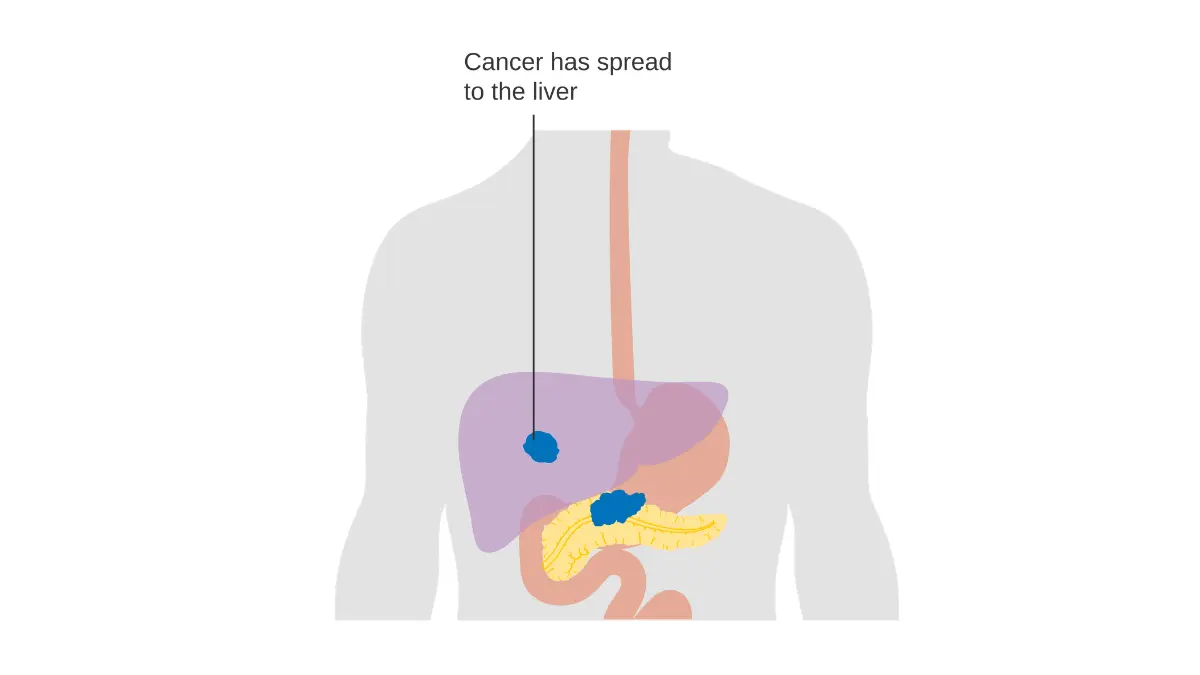
Adapted from Wikimedia Commons Diagram showing pancreatic cancer that has spread (M staging) CRUK 179, licensed under Creative Commons Attribution-Share Alike 4.0 International license.
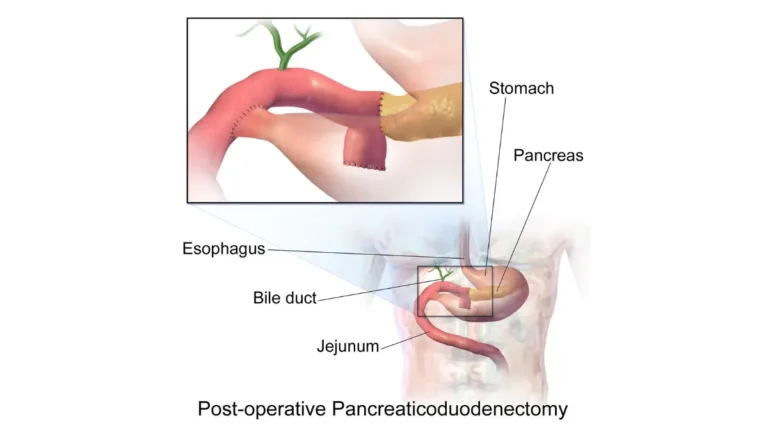
Stage vs. resectability: what actually decides treatment
Here is the part many staging guides skip. Your stage number describes how far the cancer has spread, but your oncologist plans treatment around a different question — whether the tumor can be surgically removed. The two are related, not identical.
Resectable, borderline resectable, and unresectable
Pancreatic tumors are sorted into three surgical categories:
- Resectable: the tumor can be removed completely with surgery.
- Borderline resectable: the tumor touches nearby vessels enough that immediate surgery is risky; chemotherapy, sometimes with radiation, often comes first to shrink it.
- Unresectable: the tumor cannot be safely removed — either locally advanced (wrapped around major arteries) or metastatic.
🩺 Physician Note: A common point of confusion is assuming an early stage automatically means surgery. It doesn’t. Whether an operation is offered depends on the tumor’s exact relationship to nearby arteries and veins, which is why a specialized surgical evaluation matters as much as the stage number.
Why an early stage doesn’t automatically mean surgery
A tumor can be small yet sit against a critical artery, making it borderline resectable. The point of starting with chemotherapy is sometimes to move a borderline tumor into the resectable category. According to the National Cancer Institute’s treatment guidance, surgery offers the best chance at long-term control — but only a minority of tumors are removable at diagnosis. Even when a tumor is removed, surgery is paired with chemotherapy, and doctors speak of long-term control rather than a guaranteed cure.
✅ Patient Action: Ask a surgical oncologist or hepatobiliary surgeon at a high-volume pancreatic center: “Is my tumor resectable, borderline resectable, or unresectable — and what would change that classification?”
Survival rates by stage, and what the numbers really mean
Survival statistics are often the first thing people search for and the hardest to read calmly. The figures below come from the National Cancer Institute’s SEER database, which groups cases by how far the cancer has spread rather than by AJCC stage number.
5-year survival by stage
SEER reports relative survival in three groups: localized (no spread beyond the pancreas), regional (nearby structures or lymph nodes), and distant (distant organs).
| SEER stage | What it means | Share of cases | 5-year relative survival |
|---|---|---|---|
| Localized | Confined to the pancreas | 15% | 43.6% |
| Regional | Nearby nodes or structures | 28% | 17.0% |
| Distant | Distant organs | 51% | 3.4% |
| All stages combined | — | — | 13.7% |
Source: NCI SEER Cancer Stat Facts, cases diagnosed 2016–2022. Relative survival reflects survival from the cancer itself, excluding other causes of death.
📊 Clinical Data Point: Just over half of pancreatic cancers — 51% — are found only after spreading to distant organs, while about 15% are caught while still localized. — Source: NCI SEER Cancer Stat Facts (2016–2022).
Why these numbers can’t predict your outcome
A relative survival rate is a population average, not a personal forecast. It reflects people diagnosed years ago, before the newest treatments, and it doesn’t account for your age, overall health, tumor biology, or how you respond to therapy.
⚠️ Clinical Warning: One survival percentage can mislead badly if matched to the wrong stage system. The SEER groups (localized/regional/distant) are not the same as AJCC stage numbers (I–IV), so don’t assume “stage I” maps onto the “localized” figure. Ask your oncologist how your specific situation compares.
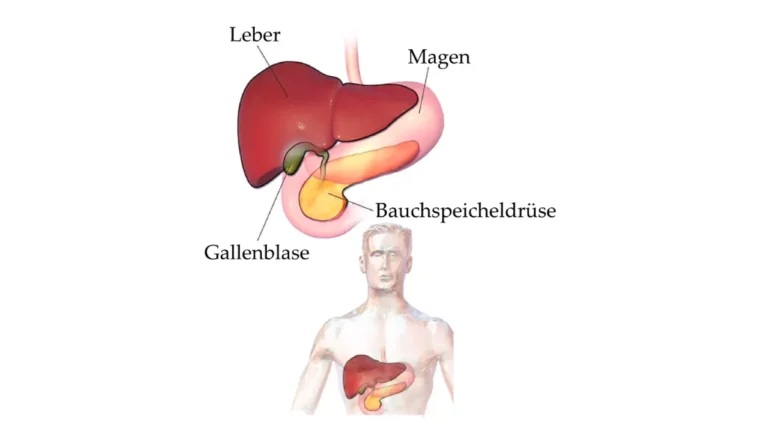
Why pancreatic cancer is often found late
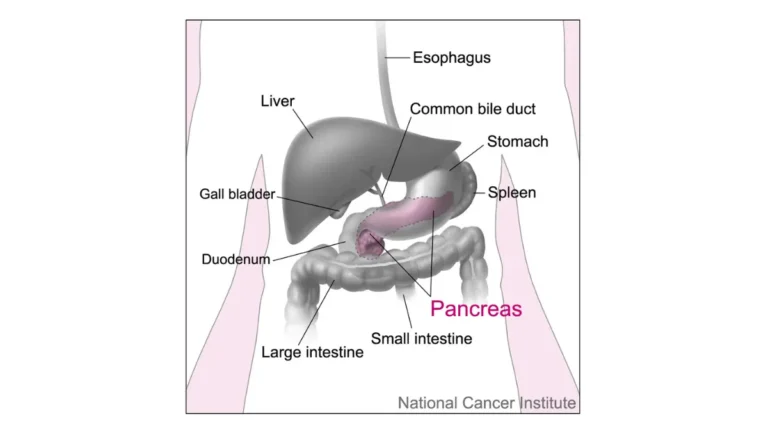
The pancreas sits deep in the abdomen, and early disease rarely causes obvious symptoms. That is why recognizing the early signs of pancreatic cancer and clues like new-onset diabetes matters — they are sometimes the only hints before the cancer advances.
How doctors determine your stage
Your stage is pieced together from several tests, which is why it can be refined over time — and sometimes changes after surgery.
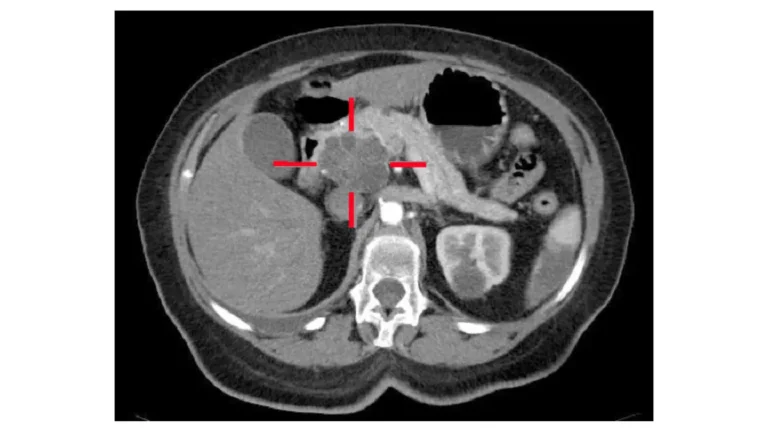
Imaging, biopsy, and blood tests
Staging usually starts with a specialized CT scan (a “pancreatic protocol” CT), sometimes with MRI, to map the tumor against nearby vessels. An endoscopic ultrasound (EUS) takes a closer look and can guide a biopsy to confirm the diagnosis. A blood test for the marker CA 19-9 is often used alongside imaging to support diagnosis and track the cancer, though it is not a standalone test. Some patients have a staging laparoscopy — a small camera procedure — to find spread too subtle for scans. Our guides explain the tests used to diagnose pancreatic cancer and what the CA 19-9 marker can and can’t tell you.
Why your stage can change after surgery
🔬 How It Works: Before surgery, doctors assign a clinical stage from imaging and biopsy. If you have an operation, a pathologist examines the removed tissue and lymph nodes and assigns a pathologic stage. The pathologic stage is often more advanced than the clinical one — frequently because lymph node involvement doesn’t show on scans — so a shift in your stage number after surgery is common and expected.
What to do after you learn your stage
Understanding your stage helps most when it turns into specific next steps with your team.
Questions worth asking your oncologist
Walk in with concrete questions rather than general worry:
- What is my exact stage, and is it clinical or pathologic?
- Is my tumor resectable, borderline resectable, or unresectable?
- What is the goal of my treatment — to remove the cancer, control it, or relieve symptoms?
- Am I a candidate for any clinical trials?
Why a second opinion and a high-volume center matter
Pancreatic cancer is complex, and outcomes are measurably better at centers that treat many of these cases. A second opinion — especially for borderline or unresectable tumors — is standard, not an insult to your doctor. If you have a family history, relatives may want to assess their hereditary risk factors, since inherited syndromes account for a meaningful share of cases.
When clinical trials are worth asking about
For advanced or unresectable disease, trials can offer access to newer treatments. The list of open pancreatic cancer clinical trials is searchable by location and stage.
✅ Patient Action: Before treatment planning, ask your medical oncologist: “Given my stage and resectability, what is my full treatment plan, and am I eligible for any clinical trials I should consider now?”
Frequently asked questions about pancreatic cancer stages
1. What are the stages of pancreatic cancer?
Pancreatic cancer stages run from 0 to IV. Stage 0 is carcinoma in situ, confined to the duct lining. Stages I and II are limited to or near the pancreas. Stage III is locally advanced, involving major arteries or several lymph nodes. Stage IV means the cancer has spread to distant organs.
2. How is the stage of pancreatic cancer determined?
Staging combines a pancreatic-protocol CT scan, often endoscopic ultrasound with biopsy, the CA 19-9 blood marker, and sometimes a staging laparoscopy. Doctors assign T, N, and M categories and combine them into one stage. Ask your team which tests set your stage and whether it is clinical or pathologic.
3. What does stage 4 (metastatic) pancreatic cancer mean?
Stage 4 pancreatic cancer means the cancer has spread beyond the pancreas to distant organs, most often the liver, peritoneum, or lungs. It is the most advanced stage, and treatment shifts toward controlling the cancer and easing symptoms rather than removing it. The stage describes where the cancer is, not a fixed timeline.
4. What is the difference between stage and resectability?
Stage describes how far pancreatic cancer has spread; resectability describes whether the tumor can be removed. Treatment is planned around resectability — resectable, borderline resectable, or unresectable — not the stage number alone. A small, early-stage tumor can still be borderline resectable if it sits against a major artery. Your surgical oncologist determines this.
5. What is the 5-year survival rate by stage?
Using SEER data, 5-year relative survival is about 43.6% for localized pancreatic cancer, 17.0% for regional, and 3.4% for distant, with an overall rate of 13.7%. These are population averages from cases diagnosed years ago and cannot predict one person’s outcome. Ask your oncologist how your situation compares.
6. Can early-stage pancreatic cancer be cured?
Early-stage, resectable pancreatic cancer offers the best chance at long-term control, and surgery is paired with chemotherapy. Even then, doctors generally speak of long-term control rather than a guaranteed cure, because the disease can recur. The earlier it is found and removed, the better the odds. Your oncology team can explain your specific outlook.
7. What is borderline resectable pancreatic cancer?
Borderline resectable means the tumor touches nearby blood vessels enough that immediate surgery is risky, though removal may become possible. Treatment often starts with chemotherapy, sometimes radiation, to shrink the tumor and improve the chance of a complete operation. A specialized surgical evaluation decides whether and when surgery is feasible.
8. Why is pancreatic cancer usually found at a late stage?
The pancreas sits deep in the abdomen, and early pancreatic cancer rarely causes clear symptoms. As a result, just over half of cases are diagnosed only after spreading to distant organs. Subtle clues like new-onset diabetes, unexplained weight loss, or jaundice can appear, which is why they are worth taking seriously.
9. Does a higher stage always mean a worse outcome?
A higher stage generally means more advanced disease and, on average, lower survival. But stage is one factor among many — tumor biology, overall health, resectability, and treatment response all matter, so two people at the same stage can have different outcomes. Your care team can interpret what your stage means for you.
10. What tests are used to stage pancreatic cancer?
The main staging tests are a pancreatic-protocol CT scan, sometimes MRI, endoscopic ultrasound with biopsy, the CA 19-9 blood marker, and occasionally a staging laparoscopy. Together they map the tumor, check lymph nodes, and look for distant spread. Ask your doctor which tests you have had and what they showed.
11. What questions should I ask my oncologist about my stage?
Ask for your exact stage and whether it is clinical or pathologic, whether your tumor is resectable, the goal of your treatment, and whether you qualify for clinical trials. For complex or borderline cases, ask about a second opinion at a high-volume pancreatic center. Clear questions help you make informed decisions with your team.
Putting your stage in context
A pancreatic cancer stage is a description, not a destiny. Your stage number tells you how far the cancer has spread; resectability tells you what treatment is possible; and survival statistics describe populations, not your individual path. The most useful next step is a focused conversation with a medical or surgical oncologist — ideally at a high-volume center — about your exact stage, whether surgery is on the table, and which trials might fit. With the right team and clear questions, the number on your report becomes a starting point for decisions rather than the last word.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Internal Medicine (2010); Clinical Pharmacology (2013) Experience: 15 years | Location: San Francisco, California Education: BS Molecular Biology, Caltech (2000); MD/PhD, UCSF School of Medicine (2007);…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.