On This Page – Quick Medical Summary
Hearing the word unresectable about your own tumor — or a parent’s — can land like a verdict. It usually isn’t one.
Whether a pancreatic cancer can be removed by surgery depends mostly on one thing: whether the tumor is touching or wrapped around the large blood vessels behind the pancreas. It is not simply a measure of whether cancer has “spread.”
Where you are right now decides what to read next. If you’ve been told your tumor is resectable, the surgery section explains what’s ahead. If it’s borderline resectable or locally advanced, the treatment and next-step sections matter most — because chemotherapy can sometimes change the answer. If it’s metastatic, our guide to what to expect with stage 4 pancreatic cancer speaks to that situation directly.
This article explains what each term means, how doctors decide, and what genuinely comes next — clearly, and without false comfort.
ℹ️ Medical Disclaimer: This article is educational. It does not diagnose pancreatic cancer, stage a tumor, or recommend specific surgery, chemotherapy, radiation, or medication. Whether any individual tumor can be removed is a judgment only a qualified pancreatic (hepatobiliary) surgical team can make after reviewing that person’s own imaging. Before acting on any treatment decision, consult a board-certified surgical and medical oncologist.
What “resectable” actually means
Resectable means a surgeon can remove the entire visible tumor along with a rim of healthy tissue around it — a clear, or negative, margin that doctors call an R0 resection. Unresectable means complete removal isn’t safely possible, almost always because of where the tumor sits rather than how big it is.
Why blood vessels decide the answer
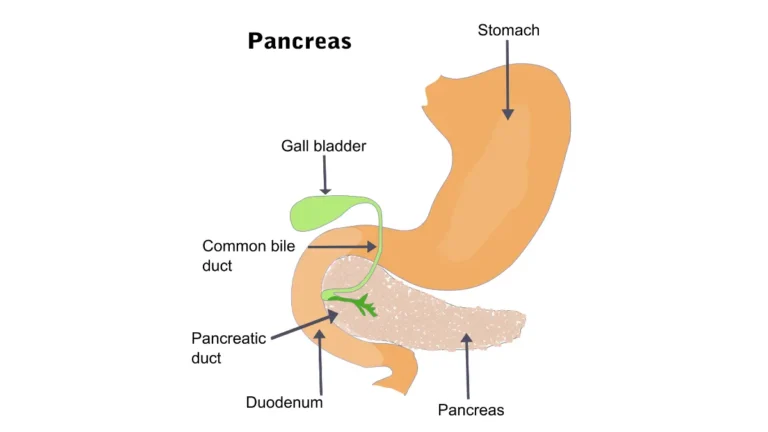
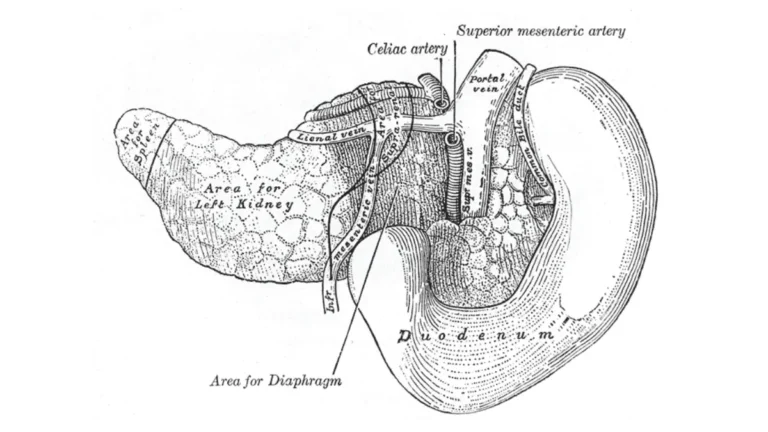
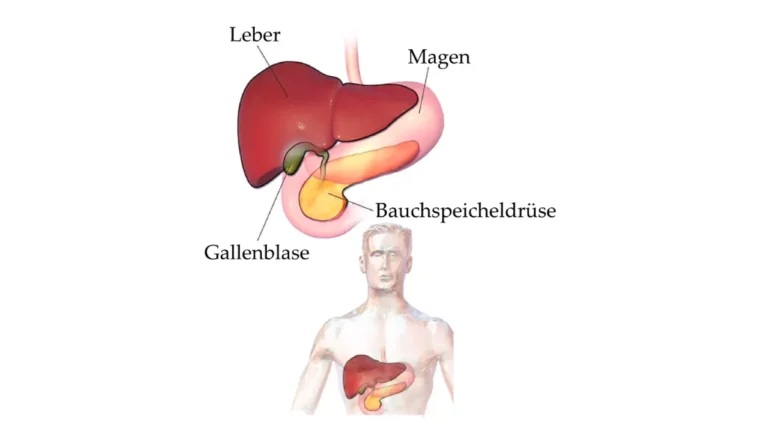
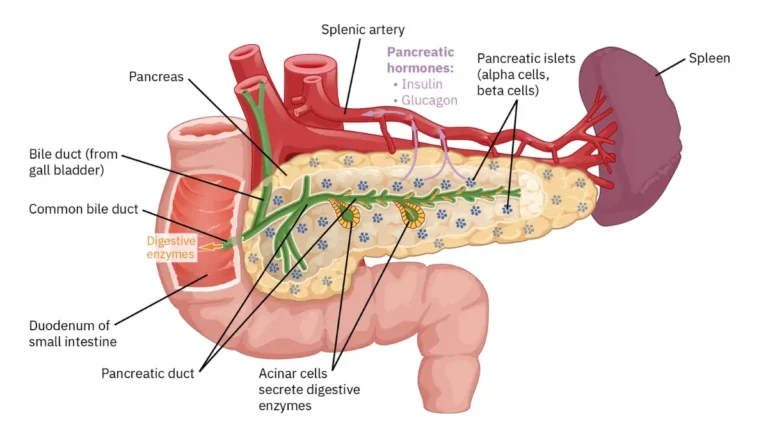
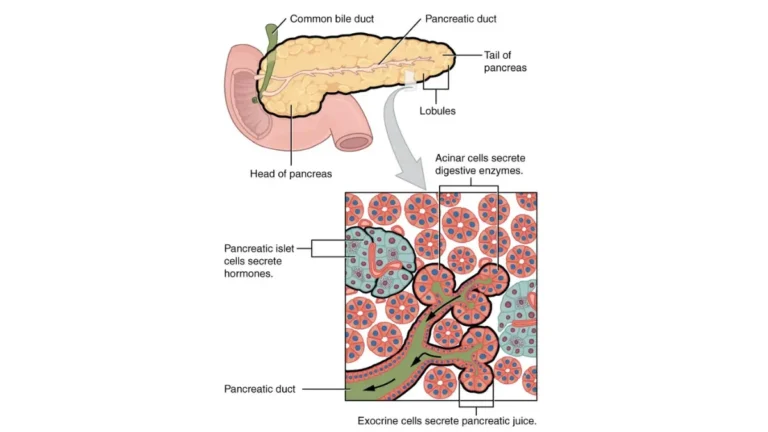
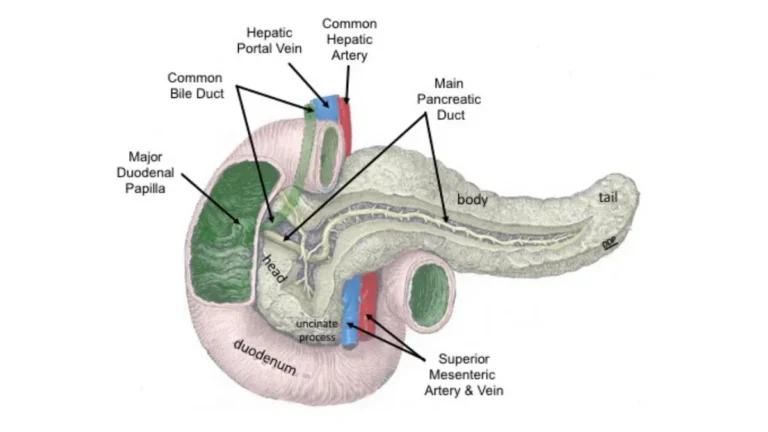
The pancreas rests against several critical vessels: the superior mesenteric artery, the celiac axis, the common hepatic artery, the superior mesenteric vein, and the portal vein. How much the tumor touches these vessels is what sorts it into a category.
🔬 How It Works: A surgeon can often remove and rebuild a vein that a tumor touches. The major arteries, though, feed the intestines, liver, and spleen — so a tumor wrapped around an artery usually can’t be taken out without unacceptable risk. That is why two tumors of identical size can fall into different categories.
The four categories at a glance
Doctors group pancreatic tumors into four buckets — resectable, borderline resectable, locally advanced (unresectable), and metastatic — based on vessel involvement and whether the cancer has reached distant sites. The next section defines each one.
The four categories: resectable, borderline, locally advanced, and metastatic
These four categories, drawn from NCCN-derived resectability criteria, are the map your whole treatment plan is built on. The simplified table below shows what separates them.
| Category | What it means (simplified) | Key clinical detail |
|---|---|---|
| Resectable | No tumor contact with arteries; little or no vein contact | Surgery is possible up front (often with chemo around it) |
| Borderline resectable | Limited artery contact, or vein contact a surgeon could rebuild | Chemotherapy usually comes first to shrink it back from the vessel |
| Locally advanced (unresectable) | A major artery is encased, or a vein is blocked beyond repair — but no distant spread | Treated to control it; can sometimes convert to operable |
| Metastatic | Cancer has reached the liver, lung, abdominal lining, or distant lymph nodes | Whole-body (systemic) therapy, not surgery, is the focus |
Source: NCCN-derived resectability criteria, summarized via the National Cancer Institute and StatPearls (NCBI).
The distinction that readers most often miss sits in the bottom two rows. Locally advanced disease is its own category — the cancer has grown into nearby vessels but has not spread to distant organs. That is different from metastatic disease.
🩺 Physician Note: Current NCCN guidance frames resectability as a vascular-anatomy decision and recommends it be made by a multidisciplinary team at a high-volume center, rather than from a single scan read in isolation. The same tumor can be judged differently depending on who reviews the images and how vessel contact is measured.
✅ Patient Action: Ask your oncologist which of the four categories your imaging places you in — and specifically whether any artery is involved. That one detail drives whether surgery is on the table. For broader context on how tumors are classified, see the National Cancer Institute’s pancreatic cancer treatment overview.
How doctors decide if a tumor can be removed
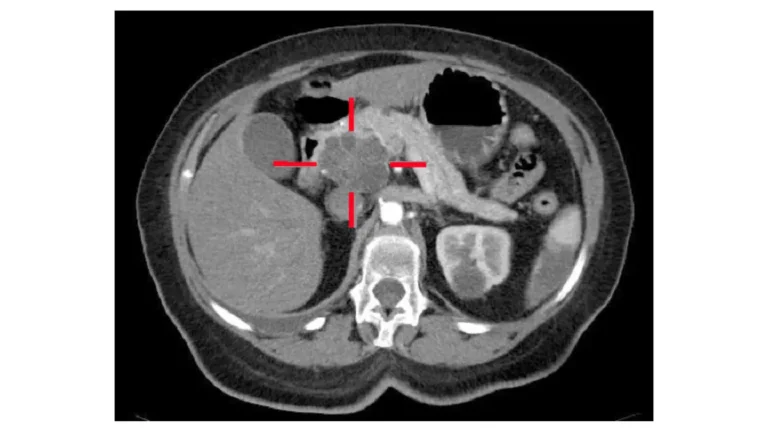
The judgment of resectability rests mostly on a specialized CT scan — a “pancreatic-protocol” CT that captures the tumor and the surrounding vessels in fine detail.
The pancreatic-protocol CT scan
This scan is timed so that arteries and veins light up separately, letting a radiologist measure how much of each vessel the tumor contacts. An endoscopic ultrasound, an MRI, the CA 19-9 blood test, and a biopsy often round out the picture. Our explainers on how pancreatic cancer is diagnosed and on the CA 19-9 tumor marker blood test walk through each step.
🔬 How It Works: Because contrast dye reaches arteries and veins at slightly different moments, a timed CT can show the exact degree — measured in degrees of the vessel’s circumference — that a tumor wraps around each one. That measurement is what assigns the tumor to its category.
Why a team reviews your case
Guidelines call for a multidisciplinary tumor board at a high-volume center to review the imaging together. Germline genetic testing is also now recommended for everyone diagnosed with pancreatic cancer; if a strong family history is your worry, you can assess inherited pancreatic cancer risk as a starting point for that conversation.
When surgery itself is the final test
Sometimes a tumor that looked removable on imaging turns out, once surgery begins, to have spread further than expected — and the operation is adjusted or stopped to avoid doing more harm than good.
What treatment looks like for each category
Treatment follows the category — and for some people, the category itself can move.
If it’s resectable
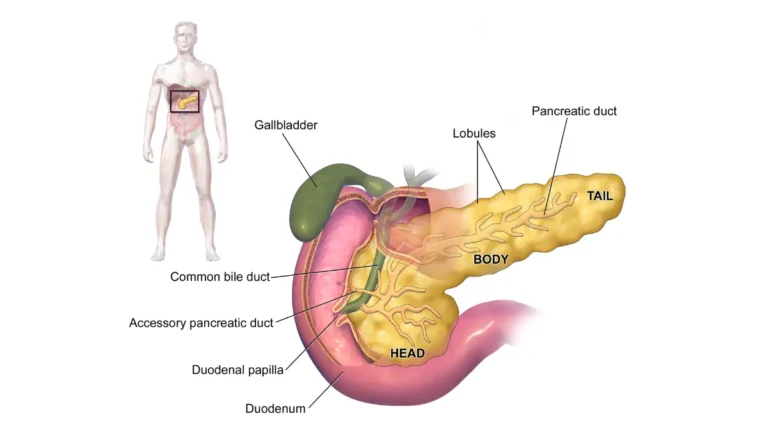
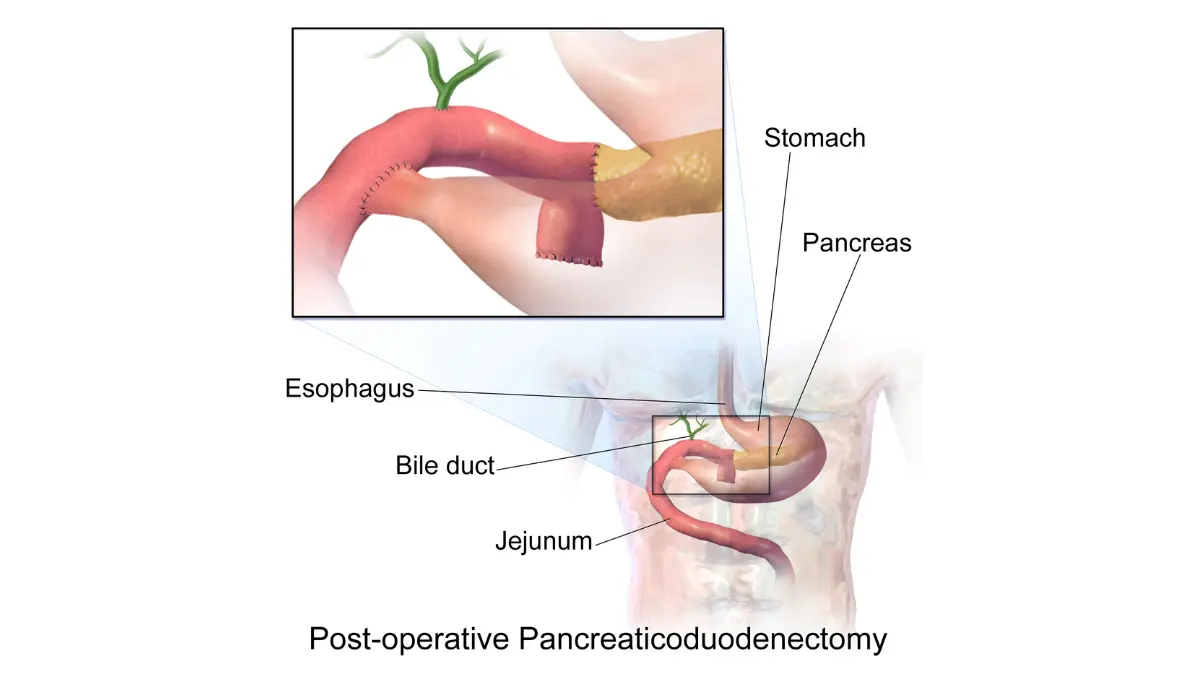
Surgery is the only treatment that offers a realistic chance of cure. The operation depends on where the tumor sits: a Whipple procedure (pancreaticoduodenectomy) for tumors in the head of the pancreas, a distal pancreatectomy for the body or tail, or a total pancreatectomy for whole-gland disease. Chemotherapy usually follows, and sometimes comes first.
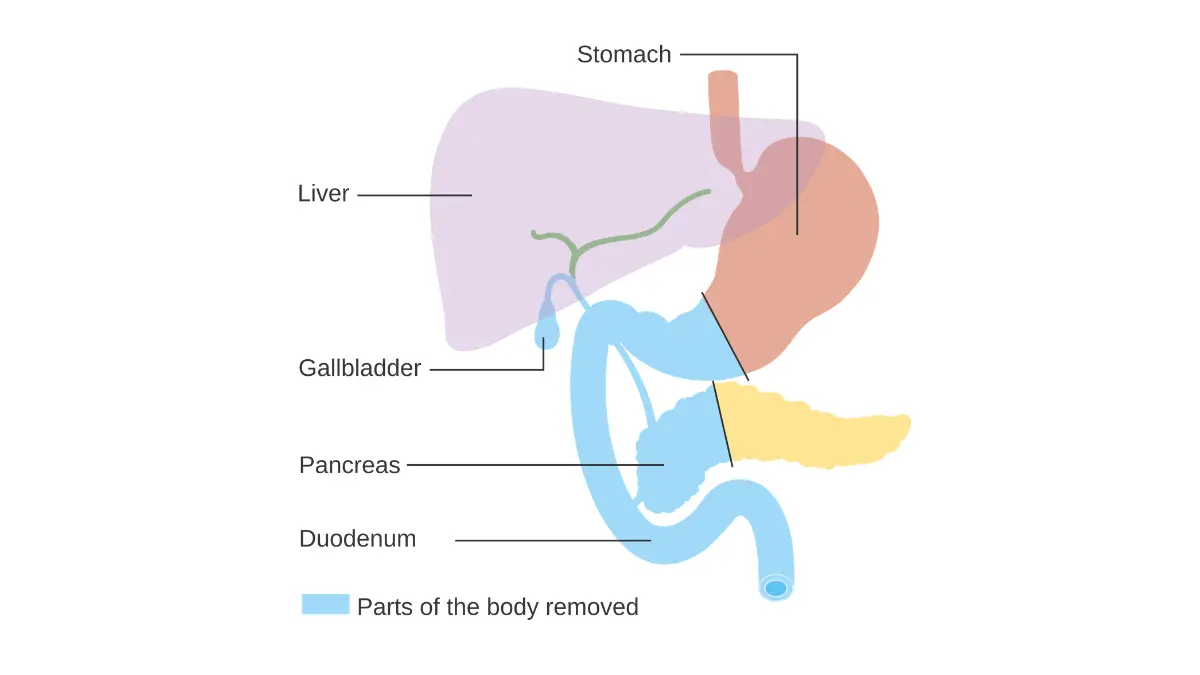
Adapted from Wikimedia Commons Diagram showing the parts removed with a Whipple’s operation CRUK 337.svg, licensed under CC BY-SA 4.0.
✅ Patient Action: Outcomes are better at experienced centers, so ask whether your surgery would be done at a hospital that performs at least 15–20 of these operations a year — the American Cancer Society’s stated benchmark. Their guide to pancreatic cancer surgery explains each operation.
If it’s borderline resectable
Here the usual path is neoadjuvant chemotherapy — chemotherapy given before surgery to shrink the tumor away from the vessels and improve the odds of a clean margin. Regimen names you may hear include FOLFIRINOX and gemcitabine plus nab-paclitaxel; your oncology team selects and doses any regimen.
If it’s locally advanced or unresectable
Can unresectable pancreatic cancer become resectable? Sometimes. Borderline tumors and some locally advanced tumors can become operable after months of chemotherapy, occasionally with radiation — a process called downstaging or conversion. For others, treatment focuses on controlling the cancer for as long as possible. Not everyone converts, and that possibility is something only your team can weigh.
🩺 Physician Note: Guidelines describe pre-surgery chemotherapy as the standard approach for borderline-resectable disease precisely because shrinking the tumor first improves the chance of removing it completely. This is the clearest reason that “unresectable today” is not always permanent.
If it’s metastatic
When cancer has reached distant organs, surgery is not the goal; systemic therapy is used to slow the disease and ease symptoms. Our guide to stage 4 pancreatic cancer covers that path in depth.
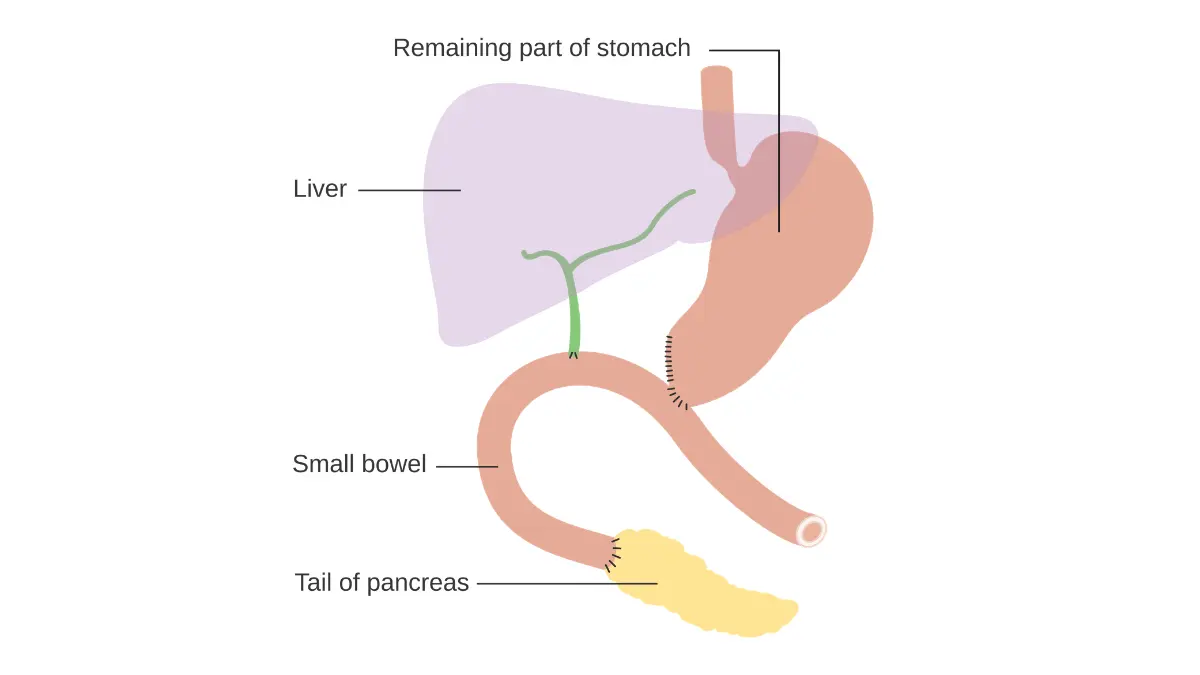
Adapted from Wikimedia Commons Diagram showing how the pancreas and bowel is joined back together after a Whipple’s operation CRUK 140.svg, licensed under CC BY-SA 4.0.
Survival by category — and why “stage” and “operability” aren’t the same
Only about 15–20% of pancreatic cancers can be surgically removed at the time they’re found; most are diagnosed after the cancer has already grown into nearby vessels or spread to distant sites.
What share of tumors is removable at diagnosis
📊 Clinical Data Point: Among U.S. pancreatic cancer cases, an estimated 15% are localized at diagnosis, 28% have reached regional lymph nodes, and 51% are already distant (metastatic). — Source: NCI SEER Cancer Stat Facts, 2016–2022 data.
Survival after surgery vs. unresectable disease
Survival figures describe large groups, not any individual. By SEER’s measure, overall 5-year relative survival for pancreatic cancer is 13.7%; for cancer still localized to the pancreas it is 43.6%, for regional spread 17.0%, and for distant disease 3.4% (NCI SEER, 2016–2022). In studies, people who have a complete (R0) resection followed by chemotherapy do meaningfully better than the all-stages average — with median survival roughly 20–24 months, versus about 9–13 months for locally advanced unresectable disease (per analyses in Annals of Oncology). These averages span all ages and health states and predate the newest treatments, so they describe a population, not a person’s prognosis.
Why “localized” doesn’t always mean “operable”
This is the point most sources blur. SEER’s “localized, regional, distant” labels describe how far a cancer has spread — not whether it can be removed. A tumor can be “localized” (confined to the pancreas) yet unresectable because it encases an artery, and the 15–20% that are resectable don’t line up exactly with any single SEER stage. Our explainer on how pancreatic cancer is staged and the NCI’s survival statistics show how these systems differ.
If you’ve been told it’s unresectable: what to do next
An “unresectable” label is a clinical judgment — and judgments can differ between centers, especially for tumors sitting near the borderline.
Get a second opinion at a high-volume center
A review by a surgeon who performs many pancreatic operations can sometimes reclassify a tumor, or surface options a general center didn’t raise.
✅ Patient Action: Request a second opinion at a high-volume pancreatic surgery center, and ask two specific questions: “Could neoadjuvant therapy make my tumor operable?” and “Am I a candidate for a clinical trial?”
Ask about downstaging and clinical trials
For borderline and locally advanced disease, trials testing newer chemotherapy and radiation combinations may offer a route toward surgery. The National Cancer Institute’s clinical trials information is a place to start looking.
⚠️ Clinical Warning: Move promptly, but not blindly. Pancreatic tumors can progress quickly, and the window where surgery or downstaging is possible can narrow — yet rushing to act on a single opinion without a high-volume review can also close doors. Balance speed with getting the right team in front of your imaging.
Frequently asked questions about resectable and unresectable pancreatic cancer
1. What is the difference between resectable and unresectable pancreatic cancer?
Resectable pancreatic cancer can be completely removed by surgery; unresectable cancer cannot be removed safely, usually because the tumor encases a major artery, blocks a vein beyond repair, or has spread to distant organs. The distinction turns on the tumor’s relationship to nearby blood vessels, not its size alone.
2. What makes a pancreatic tumor unresectable?
A tumor is generally unresectable when it wraps more than halfway around a major artery (the superior mesenteric artery or celiac axis), blocks a key vein in a way that can’t be reconstructed, or has spread to distant sites such as the liver. A specialist confirms this from detailed imaging.
3. What percentage of pancreatic cancer is resectable?
Only about 15–20% of pancreatic cancers can be surgically removed when they are diagnosed. Most are found later, after the tumor has grown into nearby vessels or spread, which is why early evaluation by a specialist matters so much.
4. Can unresectable pancreatic cancer become resectable?
Sometimes. Borderline tumors and some locally advanced tumors can become operable after months of chemotherapy, occasionally with radiation — a process called downstaging or conversion. Not everyone converts. Whether this is realistic in your case is a judgment for your oncology and surgical team.
5. Is borderline resectable pancreatic cancer curable?
Borderline resectable cancer can sometimes be removed completely after chemotherapy shrinks it back from the blood vessels, and complete removal offers the only realistic chance of cure. Outcomes vary widely by how the tumor responds to treatment, so discuss your specific situation with a surgical oncologist.
6. What is the survival rate for resectable vs. unresectable pancreatic cancer?
Survival differs sharply. In studies, median survival after a complete surgical removal plus chemotherapy is roughly 20–24 months, versus about 9–13 months for locally advanced unresectable disease. These are population averages that predate the newest treatments and cannot predict an individual outcome.
7. What surgery is used for resectable pancreatic cancer?
Three operations are used, depending on tumor location: a Whipple procedure for tumors in the head of the pancreas, a distal pancreatectomy for the body or tail, and a total pancreatectomy for whole-gland disease. Your surgical team determines which is appropriate.
8. How long can you live with unresectable (locally advanced) pancreatic cancer?
In published studies, median survival for locally advanced unresectable disease is roughly 9–13 months, though this varies with treatment response, overall health, and whether the tumor can later be downstaged toward surgery. Averages describe groups, not individuals — your oncologist can speak to your specific picture.
9. What is neoadjuvant therapy for pancreatic cancer?
Neoadjuvant therapy is chemotherapy — sometimes with radiation — given before surgery, mainly for borderline resectable tumors. The goal is to shrink the tumor away from nearby blood vessels and improve the chance of removing all of it with a clear margin. Your oncology team selects any regimen.
10. Why is pancreatic cancer often found when it’s already unresectable?
Pancreatic cancer frequently causes few clear symptoms until it has grown into nearby vessels or spread, which is why about half of cases are distant at diagnosis. Recognizing early signs of pancreatic cancer and acting on persistent symptoms can occasionally allow earlier evaluation.
11. Should I get a second opinion if I’m told my cancer is unresectable?
Yes — resectability is a judgment that can differ between centers, and a high-volume pancreatic surgery center may reclassify a tumor or raise options such as neoadjuvant therapy or a trial. Ask directly whether downstaging could make surgery possible. A prompt second opinion is worth pursuing.
Where this leaves you
The line between resectable and unresectable pancreatic cancer is drawn by anatomy — how the tumor sits against the major blood vessels — not by the word “cancer” alone. That line can move: borderline and some locally advanced tumors become operable after chemotherapy, and a second opinion at a high-volume center sometimes changes the plan. None of that lessens how serious this diagnosis is, but it does mean “unresectable” is rarely the end of the conversation. Bring your questions to your team, ask which category you’re in and why, and read our complete guide to pancreatic cancer symptoms and stages for the fuller picture.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Internal Medicine (2010); Clinical Pharmacology (2013) Experience: 15 years | Location: San Francisco, California Education: BS Molecular Biology, Caltech (2000); MD/PhD, UCSF School of Medicine (2007);…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.