On This Page – Quick Medical Summary
A pancreatic cancer diagnosis raises one urgent question: what can be done? The honest answer is that pancreatic cancer treatment is not one path — it is chosen by the stage of the cancer and, above all, by whether the tumor can be removed with surgery.
This guide compares the standard options side by side. If you are newly diagnosed, start with how options are decided, then the stage-by-stage map below. If you are weighing chemotherapy, the regimen comparison covers FOLFIRINOX, gemcitabine combinations, and the newer NALIRIFOX. If surgery may be possible, that section explains who qualifies and why the hospital matters. If you are a caregiver, the closing sections cover supportive care, trials, and the questions to ask. For the wider picture, this sits alongside the pillar guide to understanding pancreatic cancer from first signs to treatment. Throughout, figures come from named authorities, and the limits of each treatment are stated as plainly as the benefits.
ℹ️ Medical Disclaimer: This article is general education, not medical advice, and does not replace diagnosis, treatment, or guidance from your care team. Decisions about surgery, chemotherapy, radiation, medications, and coverage must be made with your physicians based on your diagnosis, stage, health, and molecular testing. Consult a board-certified medical or surgical oncologist before acting, and call your local emergency number for any emergency.
What determines your pancreatic cancer treatment options
The first thing an oncology team establishes is whether the tumor is resectable — able to be removed by surgery. That distinction shapes everything that follows.
Doctors sort pancreatic cancer into four groups: resectable (removable now); borderline resectable (possibly removable, often after treatment to shrink it); locally advanced (grown into nearby blood vessels, not safely removable); and metastatic (spread to distant organs such as the liver).
Only a minority of tumors are removable at diagnosis, which is why the sections below matter for most readers. See the guides on resectable versus unresectable disease and how pancreatic cancer is staged.
Why molecular and germline testing matters
Modern treatment increasingly depends on testing the tumor and, separately, your inherited genes. Results can reveal targeted or immunotherapy options for a subset of patients.
🩺 Physician Note: Current guidance emphasizes offering people with pancreatic cancer both germline genetic testing and tumor molecular profiling. These tests identify the small groups who may benefit from a PARP inhibitor or immunotherapy — options that are invisible without testing.
✅ Patient Action: Ask your medical oncologist: “Has my tumor had molecular profiling, and should I have germline genetic testing for BRCA and related mutations?”
For the authoritative menu of options, see the National Cancer Institute’s treatment overview.
Surgery for pancreatic cancer: who qualifies and what it involves
Surgery offers the best chance of long-term control for the minority whose cancer can be fully removed.
What percentage of patients can have surgery?
Removable disease is the exception, because symptoms often appear only after the cancer has spread.
📊 Clinical Data Point: About 15–20% of pancreatic cancers can be removed with surgery at diagnosis; up to roughly 80% are found at a later stage. — Source: Johns Hopkins Medicine, 2026.
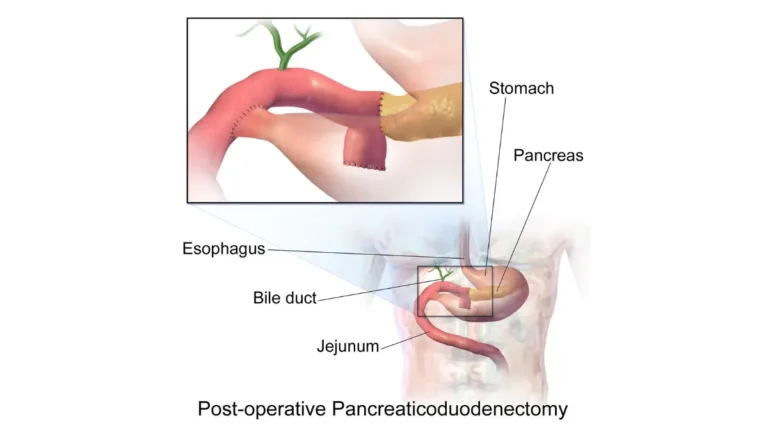
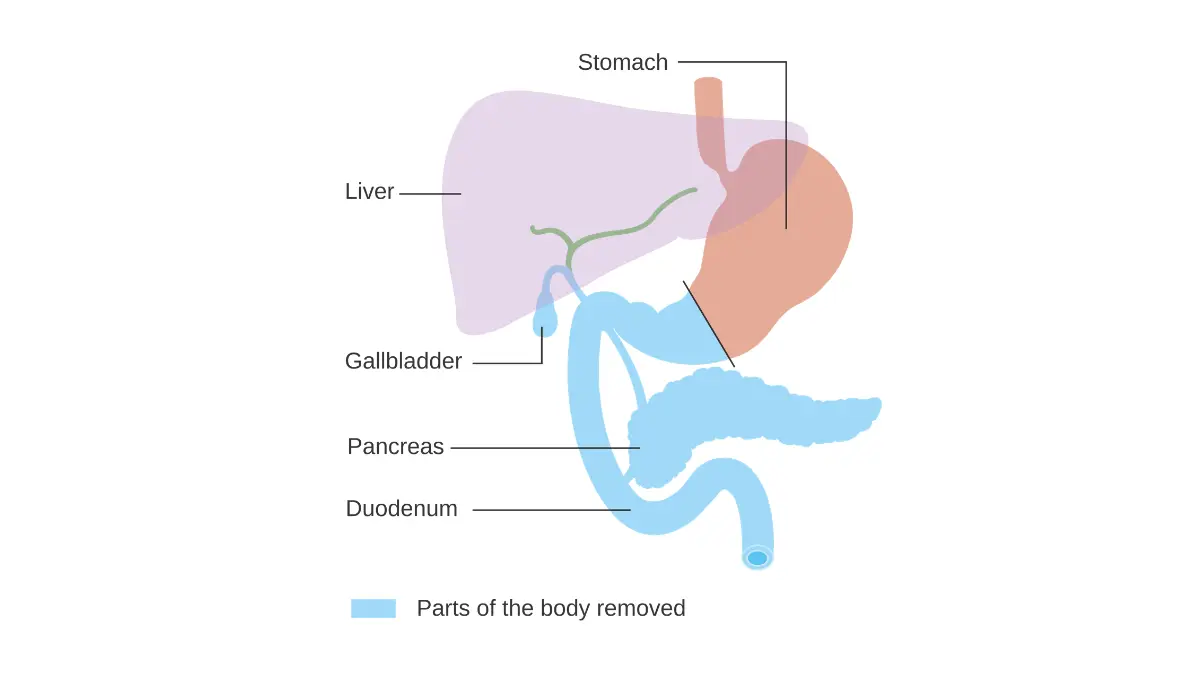
The Whipple procedure and other operations
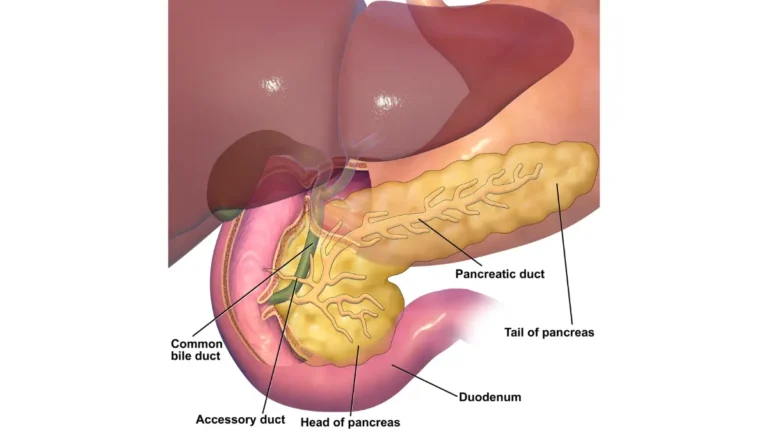
The most common operation is the Whipple procedure (pancreaticoduodenectomy). It removes the head of the pancreas, the duodenum, the gallbladder, part of the bile duct, and sometimes part of the stomach, then reconnects the remaining organs. Tumors in the body or tail are usually removed by distal pancreatectomy. Whether you are a candidate depends on imaging and a full workup, explained in how pancreatic cancer is diagnosed.
Why a high-volume surgical center matters
Where surgery happens changes outcomes. The American Cancer Society suggests having pancreatic surgery at a hospital that performs at least 15 to 20 of these operations per year, because higher-volume centers have lower complication and mortality rates.
✅ Patient Action: Ask a surgical oncologist: “How many pancreatic resections does this center perform each year, and am I a candidate for surgery now or for treatment first?”
Chemotherapy options compared: FOLFIRINOX, gemcitabine combinations, and NALIRIFOX
Chemotherapy is used before surgery, after surgery, or as the main treatment when surgery is not possible — and the choice depends heavily on how fit a person is.
| Regimen | What it combines | Best for (patient profile) | Median overall survival (trial) | Main tradeoff |
|---|---|---|---|---|
| FOLFIRINOX | 5-FU, leucovorin, irinotecan, oxaliplatin | Fitter patients with good performance status | 11.1 months vs 6.8 for gemcitabine alone (PRODIGE/ACCORD 11) | Strongest, but the most side effects |
| Gemcitabine + nab-paclitaxel | Gemcitabine and nab-paclitaxel | Patients who need a gentler regimen | 8.5 months vs gemcitabine alone (MPACT) | Better tolerated, somewhat less effective |
| NALIRIFOX | Liposomal irinotecan, oxaliplatin, 5-FU, leucovorin | First-line metastatic disease | 11.1 months vs 9.2 for gemcitabine + nab-paclitaxel (NAPOLI 3) | Benefit modest vs the doublet; high cost |
Figures are median overall survival in each trial population (PRODIGE/ACCORD 11, MPACT, and NAPOLI 3, as reported by the FDA and peer-reviewed literature), not a prediction for any individual.
NALIRIFOX: a newer first-line option
The NALIRIFOX regimen was FDA-approved in February 2024 for first-line metastatic disease, per the FDA’s approval of this regimen. Honesty matters here: its survival edge over gemcitabine plus nab-paclitaxel was modest, about two months, and it has never been compared head-to-head with FOLFIRINOX, which appears similarly effective and costs far less.
🔬 How It Works: These regimens combine drugs that damage cancer-cell DNA and block the enzymes cells use to copy it. In NALIRIFOX, the irinotecan is wrapped in a tiny fatty shell (a liposome) so it circulates longer and reaches the tumor in higher amounts.
Adjuvant chemotherapy after surgery
After a successful operation, chemotherapy lowers the chance the cancer returns. A modified FOLFIRINOX or a gemcitabine-based regimen is standard, again guided by overall health.
⚠️ Clinical Warning: These regimens commonly cause severe diarrhea and a drop in white blood cells, raising infection risk. Suitability depends on performance status — how well a person can carry out daily activities — which is why the same regimen is not right for everyone.
Radiation, targeted therapy, and immunotherapy
Beyond surgery and chemotherapy, a few options apply to specific situations or tumor biology — helping a minority, not most.
Radiation therapy and SBRT
Radiation, including focused stereotactic body radiation therapy (SBRT), has a selective and still-debated role. It is used mainly for borderline resectable or locally advanced disease, or to relieve symptoms.
Targeted therapy: olaparib for BRCA mutations
For people with an inherited BRCA1 or BRCA2 mutation, the PARP inhibitor olaparib is FDA-approved as maintenance therapy when metastatic disease has not progressed after at least 16 weeks of first-line platinum-based chemotherapy. In the POLO trial it lengthened the time before the cancer worsened (median 7.4 versus 3.8 months), though it did not significantly improve overall survival, and only a small share of patients carry this inherited mutation. See the FDA’s approval of olaparib.
🔬 How It Works: Cells with a BRCA mutation have already lost one major way to repair DNA. A PARP inhibitor blocks a second repair pathway, so cancer cells accumulate too much damage to survive while healthy cells are largely spared.
If hereditary risk runs in your family, you can assess your hereditary cancer risk with our tool, though it is general education, not a diagnostic test.
Immunotherapy and emerging KRAS-targeted treatments
Immunotherapy helps a very small group. The checkpoint inhibitor pembrolizumab is approved across tumor types for cancers that are MSI-high or mismatch-repair deficient (dMMR) — only about 1% of pancreatic cancers — where it can produce durable responses. For the rest, it is not standard. The large majority of pancreatic cancers carry a KRAS mutation, and KRAS-targeted drugs are in clinical trials rather than approved first-line care.
✅ Patient Action: Ask your oncologist or genetic counselor: “Has my tumor been tested for BRCA, MSI/dMMR, and KRAS, and do any targeted or immunotherapy options — or a trial — apply to me?”
Matching treatment to stage: how decisions are made
Putting it together, treatment is matched to where the cancer stands at diagnosis.
- Resectable: surgery, followed by chemotherapy.
- Borderline resectable: chemotherapy (sometimes with radiation) first, then surgery if the tumor shrinks enough.
- Locally advanced: chemotherapy, sometimes with radiation, since surgery is not possible.
- Metastatic: systemic chemotherapy, with maintenance or targeted options for biomarker-selected patients. See what to expect with stage 4 disease.
Stage at diagnosis also shapes the statistics, which must be read with care.
📊 Clinical Data Point: Five-year relative survival is 44% for localized, 17% for regional, and 3% for distant pancreatic cancer, and 13% across all stages combined (diagnosed 2015–2021). — Source: American Cancer Society, Cancer Facts & Figures 2026.
These figures, from the American Cancer Society’s survival data, reflect people diagnosed and treated years ago. Outcomes have been improving, and no statistic predicts what will happen for one person.
✅ Patient Action: Ask your oncology team: “Based on my exact stage and health, what is my treatment plan, and its goal — potential cure, long-term control, or comfort?”
Supportive care, second opinions, and questions to ask
Treatment is only part of good care, and the steps here carry real weight.
Supportive (palliative) care runs alongside treatment, not instead of it: pain control, nutrition support with pancreatic enzyme replacement to aid digestion, and relieving a blocked bile duct with a small stent. Starting it early improves quality of life. Tracking response sometimes uses the CA 19-9 tumor marker, and advanced and end-of-life care is covered separately.
A second opinion at a high-volume center is reasonable and can change whether surgery is offered. Clinical trials are a legitimate option at any stage, not a last resort; you can search open pancreatic cancer clinical trials by location and stage. Because the disease is so often found late — the reason its early warning signs get so much attention — acting quickly on your plan matters.
✅ Patient Action: Bring these questions to your appointment: What is my exact stage? Can my tumor be removed, now or after treatment? Has it been molecularly tested? Which regimen fits me and why? Is a trial an option?
Frequently asked questions
1. What are the main treatment options for pancreatic cancer?
The main pancreatic cancer treatment options are surgery, chemotherapy, radiation, targeted therapy, and immunotherapy, used alone or in combination. Which apply depends first on the stage and on whether the tumor can be removed with surgery, the single most important factor. Your oncology team tailors the plan to your stage, overall health, and goals.
2. Can pancreatic cancer be cured?
Long-term control or cure is mainly possible for the roughly 15–20% with removable (resectable) disease, treated with surgery followed by chemotherapy. Advanced disease is usually treatable but not curable, and five-year survival varies sharply by stage — from 44% for localized to 3% for distant disease. Discuss your individual outlook with your oncologist.
3. What percentage of pancreatic cancers can be operated on?
About 15–20% of pancreatic cancers can be removed with surgery at the time of diagnosis, according to Johns Hopkins Medicine. The rest are usually found at a later stage, when the tumor has grown into nearby blood vessels or spread. A high-volume surgeon should confirm whether surgery is possible for you.
4. What is the Whipple procedure?
The Whipple procedure, or pancreaticoduodenectomy, is the most common pancreatic cancer surgery. It removes the head of the pancreas, the duodenum, the gallbladder, part of the bile duct, and sometimes part of the stomach, then reconnects the remaining organs. It treats removable tumors in the head of the pancreas and is best done at a high-volume center.
5. Is FOLFIRINOX or gemcitabine plus nab-paclitaxel better?
FOLFIRINOX is generally stronger, with a longer median survival in trials (11.1 versus 6.8 months for gemcitabine alone), but it causes more side effects and suits fitter patients. Gemcitabine plus nab-paclitaxel (median 8.5 months) is often better tolerated. The right choice depends on performance status and goals, which your oncologist weighs with you.
6. What is NALIRIFOX?
NALIRIFOX combines liposomal irinotecan with oxaliplatin, fluorouracil, and leucovorin. The FDA approved it for first-line metastatic pancreatic cancer in February 2024; in the NAPOLI 3 trial its median survival was 11.1 months versus 9.2 for gemcitabine plus nab-paclitaxel. The benefit is modest and the cost higher, so discuss suitability with your oncologist.
7. Is there targeted therapy for pancreatic cancer?
Yes, for a minority. Olaparib, a PARP inhibitor, is FDA-approved as maintenance therapy for people with an inherited BRCA1 or BRCA2 mutation whose metastatic cancer has not progressed on at least 16 weeks of platinum-based chemotherapy. It improved progression-free survival but not overall survival. Molecular and genetic testing identifies who qualifies, so ask your oncologist.
8. Does immunotherapy work for pancreatic cancer?
Immunotherapy helps only the roughly 1% of pancreatic cancers that are MSI-high or mismatch-repair deficient (dMMR), where the checkpoint inhibitor pembrolizumab can produce durable responses. For the other patients, immunotherapy is not standard treatment. Tumor testing determines whether it applies, which is a question to raise with your oncology team.
9. What treatment is used for metastatic pancreatic cancer?
Metastatic pancreatic cancer is treated mainly with systemic chemotherapy — FOLFIRINOX, gemcitabine plus nab-paclitaxel, or NALIRIFOX — with maintenance or targeted options such as olaparib for biomarker-selected patients. The goal is usually long-term control and quality of life rather than cure. Your oncologist matches the regimen to your overall health and goals.
10. Should I get a second opinion?
Yes, a second opinion is reasonable, especially at a high-volume pancreatic center, where complication and mortality rates are lower. A second review can change whether surgery is offered, often the most consequential decision in pancreatic cancer. Seeking one rarely delays care in most cases, but confirm the timing with your treating oncologist.
11. Are clinical trials worth considering?
Yes. Clinical trials are a standard option to consider at any stage of pancreatic cancer, not only after other treatments have been tried, and they may offer access to newer approaches. You can search trials by location and stage on ClinicalTrials.gov. Ask your oncologist whether a specific trial is a good fit for you.
Taking the next step
Pancreatic cancer treatment is decided by stage, shaped by molecular testing, and best managed by a team — and a few patient-controlled choices matter. Confirm your exact stage, ask whether your tumor and genes have been tested, consider a high-volume center, and ask about clinical trials. None of this replaces your oncology team, and the figures here are population data, not a forecast. For the wider context, return to the guide on understanding pancreatic cancer from first signs to treatment.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Internal Medicine (2010); Clinical Pharmacology (2013) Experience: 15 years | Location: San Francisco, California Education: BS Molecular Biology, Caltech (2000); MD/PhD, UCSF School of Medicine (2007);…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.