On This Page – Quick Medical Summary
If you or someone you love was just diagnosed with pancreatic cancer, you may have seen headlines about a “breakthrough” against a gene called KRAS — and wondered whether it’s real, and whether it could help. Here is the honest answer, and how to use it.
This guide is written for several readers. If you are newly diagnosed or comparing treatments, Sections 4 and 6 explain the new drugs and what their results actually mean. If you are a caregiver, Section 5 lays out the testing and access steps. If your tumor has already been tested and you are waiting on results, Section 3 helps you make sense of them. If you simply saw the headline, Section 2 explains why it matters.
The short version: KRAS drives more than 90% of pancreatic cancers, and for the first time, drugs aimed at it are changing survival in clinical trials. Pancreatic cancer remains one of the deadliest cancers and the third leading cause of cancer death in the US, which is part of why these results matter so much, as reflected in national pancreatic cancer statistics. One drug, daraxonrasib, roughly doubled survival in a major study — but it is not yet FDA-approved, and it is not a cure. What follows is what is true today, and what to ask the team caring for you. For the full picture of the disease, start with our guide to how pancreatic cancer is diagnosed and staged, or review the early warning signs of pancreatic cancer.
ℹ️ Medical Disclaimer: This article is general health information, not medical advice. It describes treatments, clinical-trial results, drug-approval status, and survival statistics that may not apply to your situation — and some drugs discussed, including daraxonrasib, are investigational and not yet FDA-approved for routine use. Drug approvals and trial data change quickly. Consult a board-certified medical oncologist before making any decision about diagnosis, testing, treatment, a procedure, or insurance.
What the KRAS gene does and why it was called “undruggable”
KRAS is a gene that normally works like an on/off switch for the signals that tell a cell to grow and divide. In pancreatic ductal adenocarcinoma — the most common form of pancreatic cancer — a KRAS mutation jams that switch in the “on” position, so the tumor receives a constant grow signal. More than 90% of pancreatic cancers carry such a mutation, which is why KRAS is the disease’s central target.
What KRAS is and what goes wrong in pancreatic cancer
Most KRAS mutations in pancreatic cancer occur at a single spot on the gene called codon 12. A change there alters the KRAS protein so it stays locked in its active, signal-sending form instead of switching off. The constant signal is what drives the uncontrolled growth at the heart of the tumor.
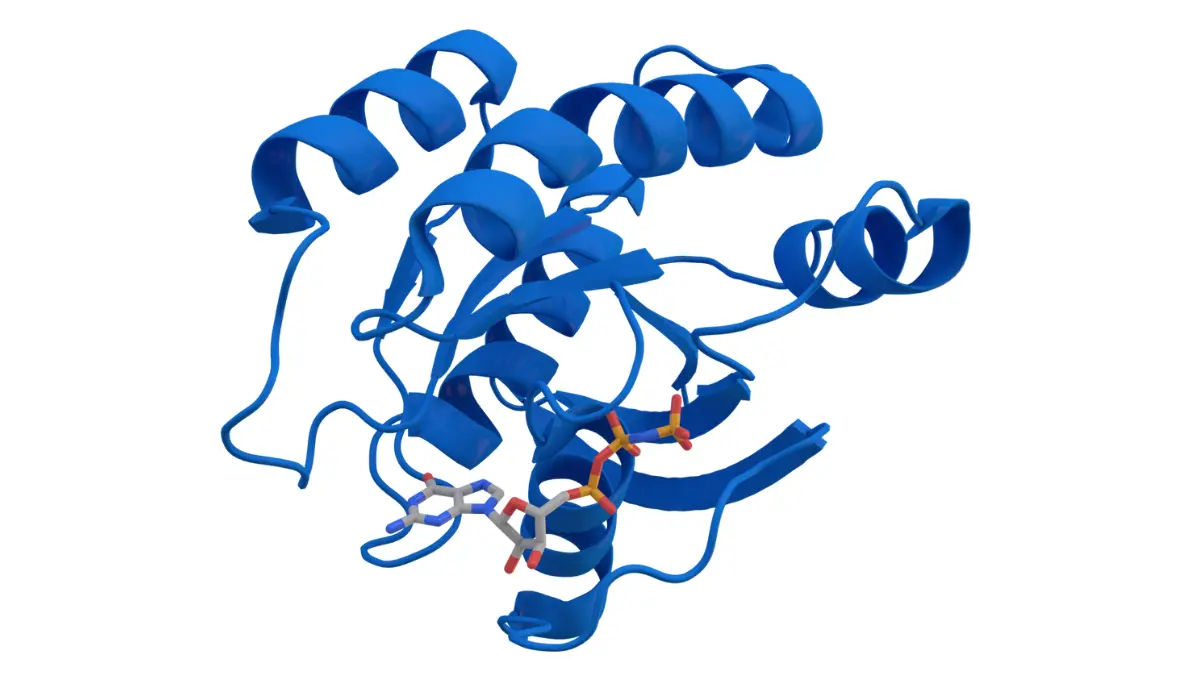
🔬 How It Works: Picture KRAS as a stuck accelerator. A healthy KRAS protein cycles between an active (“on”) state and an inactive (“off”) state. A codon-12 mutation keeps it bound to its active form, so the growth signal never shuts off — even when the cell should be told to rest.
Why decades of attempts failed
For nearly 40 years, KRAS was considered undruggable. The protein’s surface is relatively smooth, without the deep pocket most drugs need to grip, and it holds onto its signaling partner so tightly that blocking it seemed out of reach. Newer drugs finally work around this problem — which is why 2026 marks a genuine turning point in kras pancreatic cancer treatment.
Which KRAS mutation matters: G12D, G12V, G12R, and G12C
Not every KRAS mutation is the same, and the specific type — called a variant — helps determine which treatments may apply. In pancreatic cancer, KRAS G12D is the most common variant, found in roughly 40% of cases, followed by G12V (about 30%) and G12R (about 15–17%).
The most common pancreatic KRAS mutations and how often they occur
| KRAS variant | Approx. frequency in pancreatic cancer | Key clinical detail |
|---|---|---|
| G12D | ~40% | Most common; historically the hardest to target; investigational drugs now emerging |
| G12V | ~30% | Second most common; no approved targeted drug yet |
| G12R | ~15–17% | Occurs almost only in pancreatic cancer; no approved targeted drug |
| Q61 | ~5% | Less common; addressed by some pan-RAS approaches in trials |
| G12C | ~1–2% | Rare here; the only variant with drugs already approved (in other cancers) |
Frequencies per JCO Precision Oncology (2024) and Frontiers in Oncology (2024); verified June 2026.
📊 Clinical Data Point: KRAS G12C — the variant targeted by the first approved KRAS drugs — appears in only about 1–2% of pancreatic cancers — Source: JCO Precision Oncology, 2024.
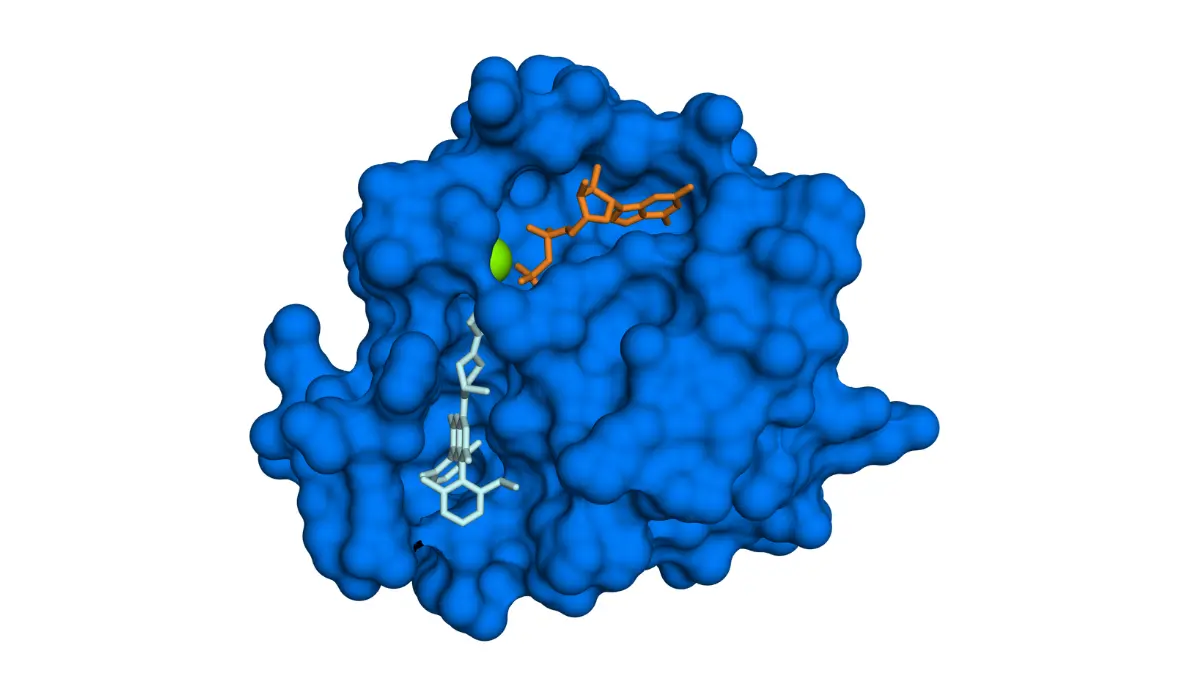
Adapted from Wikimedia Commons KRAS protein G12C mutant with GDP and sotorasib 6OIM, licensed under public domain.
Why your specific variant changes your options
This distribution matters because the first approved KRAS drugs target G12C — the one variant that is rare in pancreatic cancer. Most patients have G12D, G12V, or G12R instead, which is exactly why the newer “pan-RAS” approach covered in the next section is such a shift. Variant type can also carry prognostic information: at a population level, G12D has been linked to worse outcomes, while G12R and KRAS-normal tumors tend to fare somewhat better. Understanding where your tumor falls connects directly to how pancreatic cancer is staged.
✅ Patient Action: Ask your medical oncologist: “Which KRAS variant did my tumor’s testing show, and does it change my treatment options or trial eligibility?”
The new KRAS drugs for pancreatic cancer in 2026
Yes — for the first time, drugs that target KRAS are showing real benefit in pancreatic cancer, though access depends on your situation. The most promising, daraxonrasib, is investigational and works against many KRAS variants at once. Two other drugs are approved for the rare G12C variant, and a newer class is being tested for the common G12D variant. The broader context, including chemotherapy and surgery, is covered in our overview of pancreatic cancer treatment options.
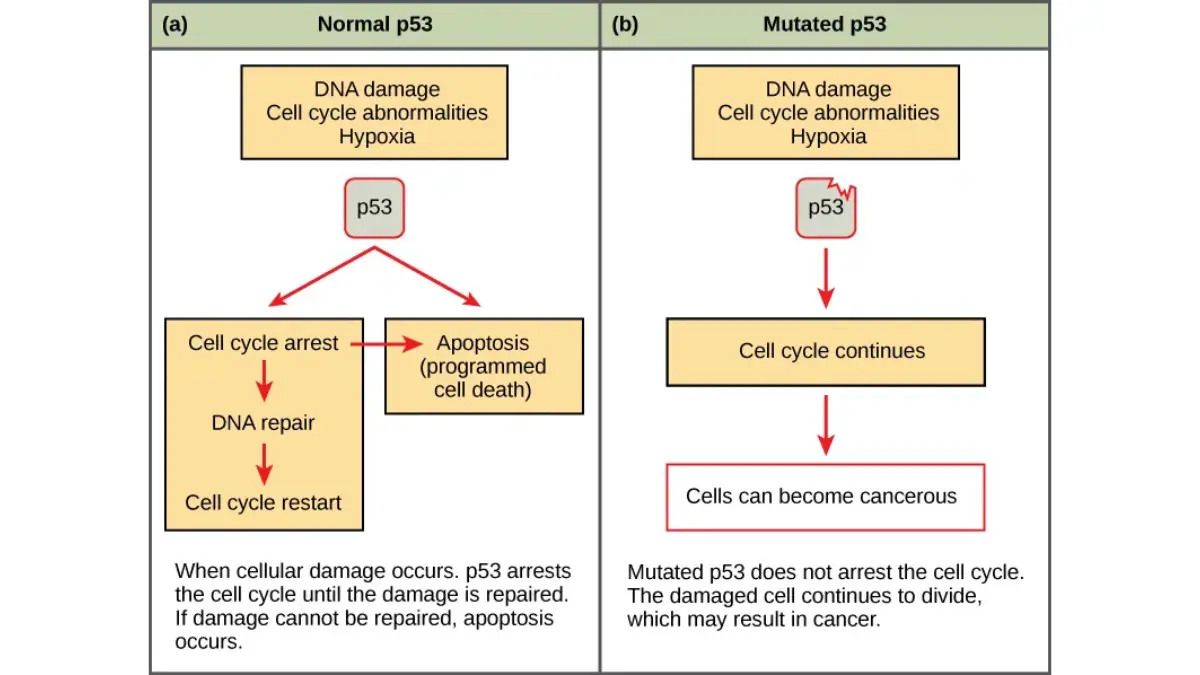
Adapted from OpenStax Figure 6.8, licensed under CC BY 4.0.
Daraxonrasib: the pan-RAS drug that doubled survival in a trial
Daraxonrasib is an oral drug that targets the active form of RAS rather than one specific mutation. In the phase 3 RASolute 302 trial of patients with previously treated metastatic pancreatic cancer, it nearly doubled median overall survival compared with chemotherapy.
📊 Clinical Data Point: In RASolute 302, median overall survival was 13.2 months with daraxonrasib versus 6.7 months with chemotherapy (hazard ratio 0.40) in previously treated metastatic pancreatic cancer — Source: Revolution Medicines / ASCO 2026 (the RASolute 302 trial record).
🔬 How It Works: Rather than gripping KRAS directly, daraxonrasib binds a helper protein called cyclophilin A. That pairing then clamps onto the active RAS protein and switches off its growth signal — an approach that works across many KRAS variants at once.
⚠️ Clinical Warning: Daraxonrasib is not yet FDA-approved and is currently available only through an expanded access program, not as standard care. It also carries real side effects that require active management. Eligibility and access are decisions only your oncologist can make.
Sotorasib and adagrasib: for the rare G12C tumor
Sotorasib and adagrasib are approved KRAS G12C inhibitors — but for lung cancer and, combined with another drug, colorectal cancer, not pancreatic. Because only about 1–2% of pancreatic cancers carry G12C, these apply to very few patients here, and any use is off-label or within a clinical trial.
Setidegrasib and the push to target G12D
Because G12D is pancreatic cancer’s most common variant, targeting it is a major goal. Setidegrasib, an investigational “degrader” that removes the mutant protein rather than blocking it, showed early activity in a phase 1 trial of previously treated patients. It remains experimental and is not approved. How these compare to standard regimens is discussed in our piece on FOLFIRINOX versus gemcitabine chemotherapy.
How to find out if a KRAS-targeted treatment fits your case
Finding out whether a KRAS-targeted treatment could apply to you starts with knowing your tumor’s mutation — and that requires specific testing.
- Ask whether your tumor has had molecular profiling (also called biomarker or genomic testing), which identifies its KRAS variant.
- If it has not, ask whether testing can be run on your existing biopsy sample.
- Ask about clinical trials and expanded access programs, ideally at an NCI-designated cancer center.
Step 1: Confirm your tumor has had molecular profiling
Molecular profiling is recommended in pancreatic cancer and is how your care team identifies the KRAS variant. Tumor markers like CA 19-9 track the cancer’s activity but do not identify mutations — that is a separate test. If you are early in the process, our guide to how pancreatic cancer is diagnosed explains where testing fits.
Step 2: Ask about trials and expanded access at a specialized center
Investigational options like daraxonrasib are reached through clinical trials or expanded access, usually at specialized centers; the NCI maintains an overview of pancreatic cancer treatment and clinical trials. Your oncologist determines whether you are eligible.
🩺 Physician Note: A common point of confusion: the KRAS mutation in a pancreatic tumor is acquired by the tumor itself (called somatic) — it is not an inherited gene passed through families. Separate inherited risk factors, such as BRCA mutations or a strong family history, are a different question. You can check your inherited pancreatic cancer risk factors and raise them with a genetic counselor.
✅ Patient Action: Ask your oncologist or a genetic counselor: “Has my tumor been molecularly profiled for KRAS, and am I a candidate for a KRAS-directed trial or expanded access?”
What the daraxonrasib survival results really mean
A near-doubling of survival is a major result — and it helps to see it against pancreatic cancer’s baseline.
Doubled survival, in context
The overall 5-year relative survival for pancreatic cancer is about 13%, up from roughly 7% a decade ago.
📊 Clinical Data Point: Pancreatic cancer’s overall 5-year relative survival is about 13% — Source: American Cancer Society, Cancer Facts & Figures 2026 (5-year relative survival by stage).
In the trial, daraxonrasib extended median survival from 6.7 to 13.2 months in the second-line, metastatic setting. That is a meaningful gain for patients with few options — but it measures months, not years, and it does not mean a cure. For what these numbers look like in advanced disease, see our guide to life expectancy with stage 4 pancreatic cancer.
Is daraxonrasib approved yet, and what about toxicity?
Not yet. As of mid-2026, daraxonrasib holds FDA Breakthrough Therapy and Orphan Drug designations and is available through an expanded access program, with possible full approval later in 2026. It is not standard care, and whether you can access it depends on your oncologist’s request and your eligibility.
⚠️ Clinical Warning: The survival benefit comes with real toxicity. Reported side effects can be significant and require active monitoring and management by an oncology team — this is not a benign drug. Do not view expanded access as a low-risk or guaranteed option.
Side effects, expectations, and questions for your oncologist
Every KRAS-targeted treatment has side effects, and knowing what to watch for helps you and your team act early.
Side effects to discuss and monitor
Reported effects vary by drug. Daraxonrasib’s benefit comes with toxicity that needs management, and the investigational G12D degrader caused significant side effects in a meaningful share of patients in early testing. Specific symptoms and how to handle them belong with your oncology team, and you can prepare using our guide to managing chemotherapy side effects.
✅ Patient Action: Ask your oncology care team: “Which side effects should prompt me to call you right away, and how would a KRAS option fit with my current chemotherapy plan?”
Don’t pause effective treatment to wait for a headline
Standard chemotherapy combinations remain the backbone of pancreatic cancer care, and an encouraging headline is not a reason to stop a treatment that is working. Investigational drugs are options to discuss with your team, not to chase at the expense of proven care.
⚠️ Clinical Warning: Never stop or change a current cancer treatment to wait for an unapproved drug without your oncologist’s guidance. A gap in effective treatment can allow the cancer to progress.
KRAS and pancreatic cancer treatment: frequently asked questions
1. What is KRAS in pancreatic cancer?
KRAS is a gene that normally switches cell-growth signals on and off. In more than 90% of pancreatic cancers, a KRAS mutation locks that switch “on,” continuously driving tumor growth. That is why KRAS is the central target in pancreatic cancer treatment and the focus of nearly every new drug now in development.
2. Why was KRAS considered “undruggable”?
For nearly four decades, the KRAS protein was considered undruggable because its surface lacks the deep pocket most drugs need to grip, and it binds its signaling partner tightly. Newer drugs finally work around this by targeting the active protein or removing it entirely — which is why effective KRAS pancreatic cancer treatment is now emerging.
3. Which KRAS mutation is most common in pancreatic cancer?
In pancreatic cancer, KRAS G12D is the most common variant, found in roughly 40% of cases, followed by G12V (about 30%) and G12R (about 15–17%). The G12C variant that newer lung-cancer drugs target is rare here, at about 1–2%. Your tumor’s molecular testing identifies which KRAS variant you have.
4. Is there a KRAS drug for pancreatic cancer?
There is real progress in KRAS pancreatic cancer treatment. Daraxonrasib, an oral drug targeting active RAS, nearly doubled survival in a trial but is not yet FDA-approved. Sotorasib and adagrasib are approved for the rare G12C variant in other cancers. Ask your oncologist which, if any, fits your tumor and situation.
5. What is daraxonrasib and how well does it work?
Daraxonrasib is an investigational oral drug that targets the active form of RAS across many KRAS variants. In the RASolute 302 trial of previously treated metastatic pancreatic cancer, median survival was 13.2 versus 6.7 months with chemotherapy. It is promising but not a cure. Discuss whether it suits your case with your oncologist.
6. Is daraxonrasib FDA approved?
Not yet. As of mid-2026, daraxonrasib holds FDA Breakthrough Therapy and Orphan Drug designations and is available through an expanded access program, with possible full approval later in 2026. It is not standard care. Access depends on your oncologist’s request and your eligibility, so ask your treatment team directly.
7. Do sotorasib and adagrasib work for pancreatic cancer?
Sotorasib and adagrasib are approved KRAS G12C inhibitors — but for lung cancer and, with another drug, colorectal cancer, not pancreatic. Because only about 1–2% of pancreatic cancers carry the G12C variant, these drugs apply to very few patients here and are used off-label or in trials. Tumor testing determines relevance; ask your oncologist.
8. What is a KRAS G12D inhibitor or degrader?
G12D is pancreatic cancer’s most common KRAS variant but has been hard to drug. Setidegrasib, an investigational degrader, removes the mutant KRAS protein rather than blocking it, and showed early activity in a phase 1 trial. It remains experimental and unapproved. Ask your oncologist about G12D-directed clinical trials if your tumor carries this variant.
9. How do I find out if I have a KRAS mutation?
Your KRAS status comes from tumor molecular profiling, also called biomarker or genomic testing, which is recommended in pancreatic cancer. Ask your oncologist whether your tumor has been profiled and which variant it showed. Specialized or NCI-designated cancer centers can also discuss clinical trials and expanded access based on those results.
10. Is a KRAS mutation inherited—should my family worry?
The KRAS mutation in a pancreatic tumor is acquired by the tumor itself (somatic) — it is not an inherited gene passed through families. Separate inherited factors, such as BRCA mutations or a strong family history, can affect risk and are worth discussing with a genetic counselor. The two are different questions.
11. What are the side effects of KRAS-targeted treatment?
Side effects of KRAS pancreatic cancer treatment vary by drug and can be significant but are generally manageable — daraxonrasib’s benefit, for example, comes with toxicity that requires monitoring. Specific symptoms and how to handle them should be managed by your oncology team. Call them promptly about severe or worsening symptoms.
The bottom line on KRAS treatment for pancreatic cancer
For the first time in decades, drugs that target KRAS — the gene behind more than 90% of pancreatic cancers — are changing survival in clinical trials. That is real progress. But the leading drug, daraxonrasib, is not yet approved, is not a cure, and reaches patients today only through expanded access or clinical trials.
The most useful next step is a specific conversation with your oncologist: confirm your tumor has been molecularly profiled for its KRAS variant, and ask whether a KRAS-directed trial or expanded access fits your case. Knowing your variant turns a distant headline into a question you can actually act on.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Internal Medicine (2010); Clinical Pharmacology (2013) Experience: 15 years | Location: San Francisco, California Education: BS Molecular Biology, Caltech (2000); MD/PhD, UCSF School of Medicine (2007);…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.