On This Page – Quick Medical Summary
A bowel obstruction means the digestive tract is partly or fully blocked, so food, fluid, and gas can’t move through the way they should. With pancreatic cancer, this can happen — and while it’s frightening, a blockage can usually be relieved or managed once it’s recognized.
Use this guide based on where you are right now. If you or someone you care for has severe stomach pain, keeps vomiting, and can’t pass gas or stool, skip to the emergency signs below and get care without delay. If you were recently diagnosed and want to understand why this happens and what to watch for, the next sections walk through it plainly. If you’re wondering what doctors can actually do about a blockage, the treatment section covers the options.
This article explains the two ways pancreatic cancer blocks the gut, the signs to watch for, which symptoms are an emergency, and how a blockage is diagnosed and treated.
ℹ️ Medical Disclaimer: This article is general health information and does not diagnose, treat, or replace care from a qualified clinician. It does not provide medication doses, self-treatment steps, or individual recommendations for surgery, procedures, or insurance. A bowel obstruction can be a medical emergency — if you have severe abdominal pain, persistent vomiting, a swollen belly with no passage of gas or stool, or fever, seek emergency care immediately. Discuss your symptoms and options with a board-certified oncologist and your palliative care team.
Why pancreatic cancer can block the digestive tract
Pancreatic cancer can block the digestive tract in two different places, and knowing which one you may be facing helps the symptoms make sense.
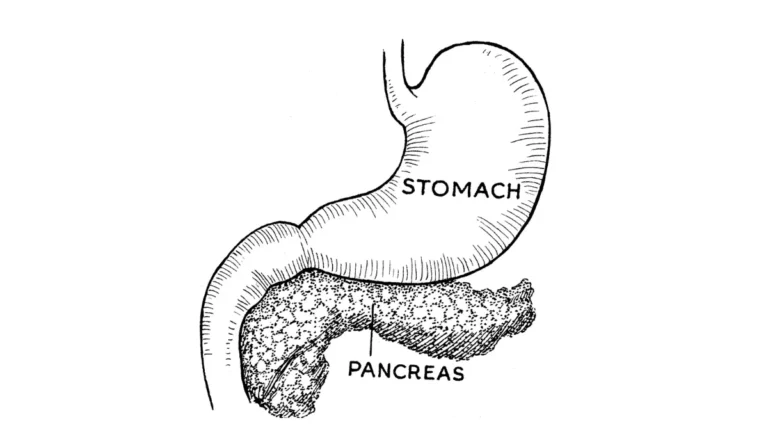
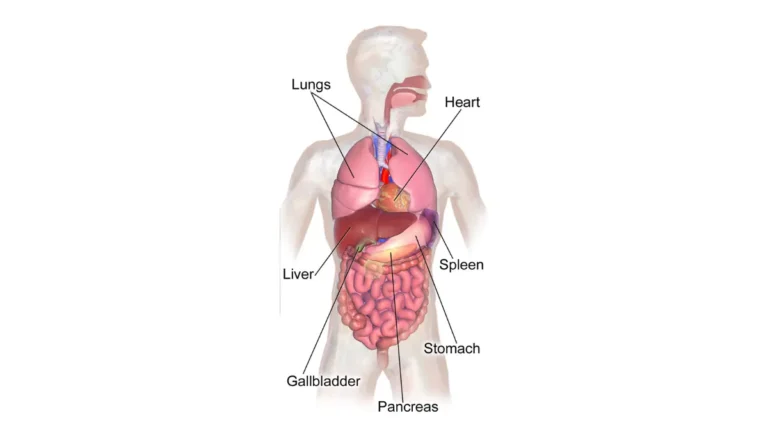
🔬 How It Works: The head of the pancreas sits directly against the duodenum — the first stretch of small intestine, just past the stomach. A tumor there can press on or grow into that narrow passage, slowing or stopping the stomach from emptying.
When the tumor presses on the stomach’s outlet
Most pancreatic tumors begin in the head of the pancreas, right next to where the stomach empties. When a tumor narrows this outlet, the stomach can’t drain properly — a problem called gastric outlet obstruction.
📊 Clinical Data Point: Roughly 10–25% of people with pancreatic cancer develop gastric outlet obstruction at some point (estimates vary across studies) — Source: published clinical reviews, 2024–2025.
This is one of the more common ways the cancer interferes with eating. It can also occur alongside a blocked bile duct, which causes jaundice in pancreatic cancer.
When cancer spreads to the abdomen
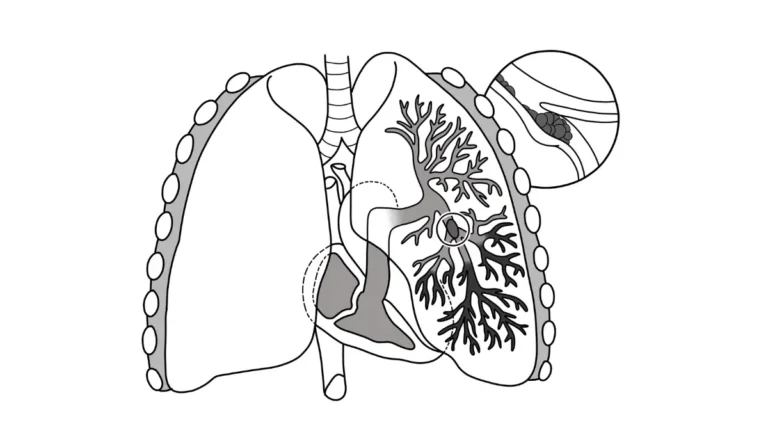
Pancreatic cancer can also block the small or large intestine lower down, usually in more advanced disease. This tends to happen when cancer spreads to the lining of the abdomen (the peritoneum) or the tissue that anchors the bowel (the mesentery), kinking or compressing it.
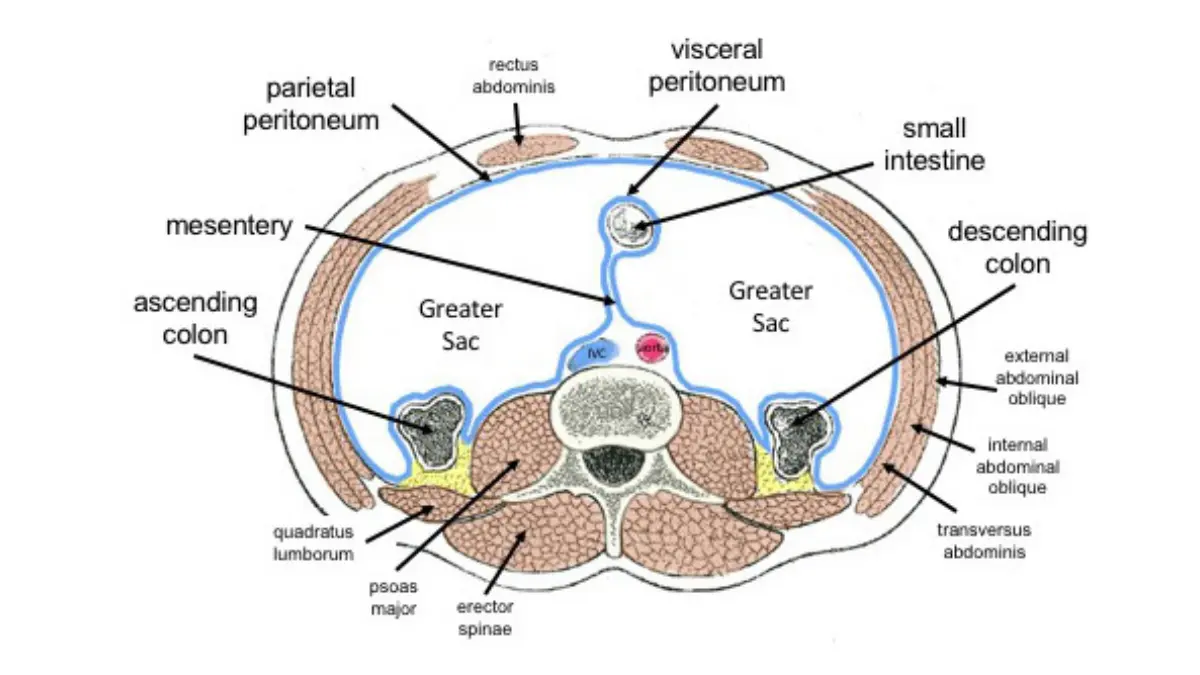
Adapted from Wikimedia Commons General Distribution of the Peritoneum, licensed under CC BY-SA 4.0.
According to the National Cancer Institute, this kind of malignant bowel obstruction is a recognized complication of advanced cancers inside the abdomen. To see where this fits in the larger picture, our guide to how pancreatic cancer develops and spreads walks through the stages.
Signs of a bowel obstruction in pancreatic cancer
The signs of a blockage depend on where it is and how complete it is, but several symptoms show up again and again.
Common signs of a bowel obstruction in pancreatic cancer include:
- Nausea and vomiting — sometimes large amounts, or food eaten hours earlier
- Bloating and a swollen, distended belly
- Cramping, colicky belly pain that comes in waves
- Feeling full after only a few bites (early satiety)
- Constipation, or being unable to pass gas or stool at all
- Loss of appetite and, over time, weight loss
The National Cancer Institute lists abdominal pain, cramps, distension, nausea, vomiting, and the absence of gas and stool as signs of a malignant bowel obstruction. You can read more in the National Cancer Institute’s guide to gastrointestinal complications.
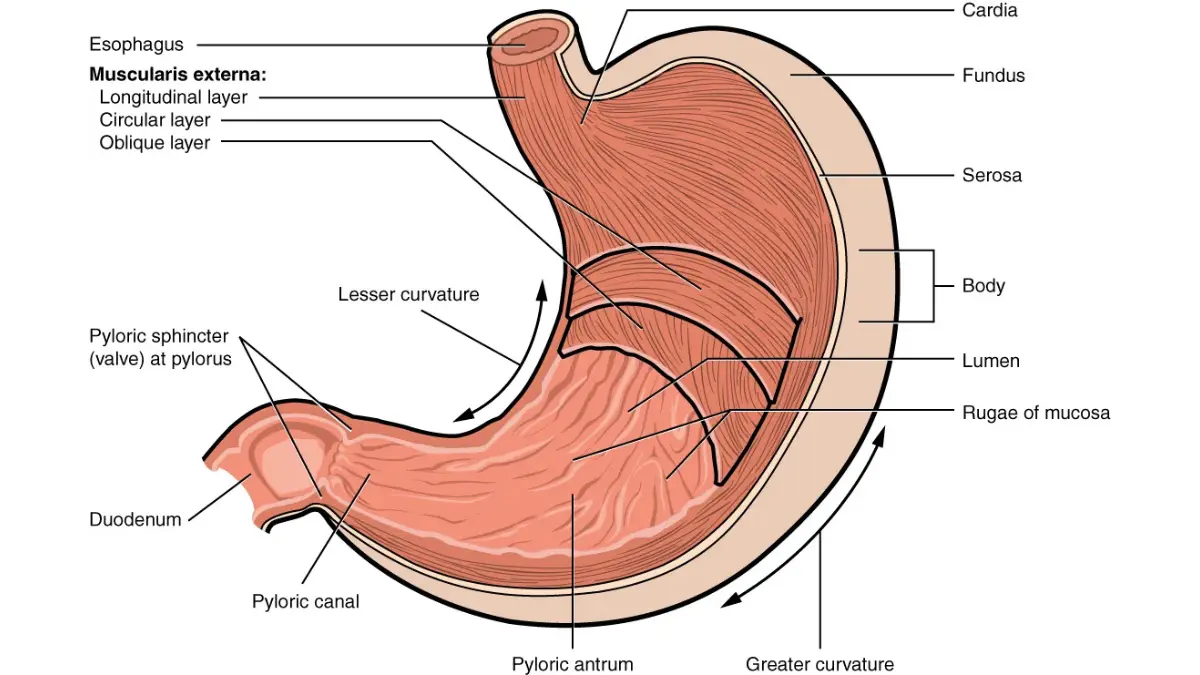
Adapted from OpenStax The Stomach Figure 23.15, licensed under CC BY 4.0.
Early and upper-blockage signs
When the blockage is high up, at the stomach’s outlet, vomiting tends to come early and the belly may not swell much at first. Feeling full quickly, bloating after meals, and bringing food back up are common. Because these overlap with other pancreatic cancer symptoms, it helps to compare them against the broader early signs of pancreatic cancer.
Lower and complete-blockage signs
A blockage lower in the intestine usually builds more gradually. The belly swells, cramping spreads, and bowel movements slow or stop. With a complete blockage, you typically can’t pass gas or stool at all, while a partial one may still let some through.
How the location changes what you feel
Small-intestine blockages often cause sharp, wave-like cramps around the navel that return every few minutes. Large-intestine blockages tend to cause steadier, more spread-out discomfort with increasing constipation. The pain pattern can resemble other problems, so it’s worth knowing where pancreatic cancer pain is usually felt — and a clinician is needed to confirm what’s causing it.
When obstruction symptoms are an emergency
A bowel obstruction can become a medical emergency, so it helps to know exactly which signs mean “get care now.”
⚠️ Clinical Warning: A complete blockage can cut off the blood supply to part of the bowel (strangulation) or cause it to tear (perforation), which can lead to a dangerous abdominal infection. These complications can develop within hours and are life-threatening without prompt treatment.
Go to the emergency room now if you have these signs
- Severe or constant abdominal pain
- Vomiting that won’t stop, or vomiting that smells like stool
- A swollen, hard belly with no passing of gas or stool
- Fever, chills, or a racing heartbeat
- Signs of dehydration — very little urine, dark urine, or dizziness
Tell the team you have pancreatic cancer and a possible bowel obstruction.
What complete blockage, strangulation, and perforation mean
A complete obstruction stops everything from moving through and usually needs urgent treatment. Strangulation means a section of bowel loses its blood supply; perforation means it tears and leaks, which can cause peritonitis — a serious infection of the abdomen. Waiting these out is risky, because they can worsen quickly.
✅ Patient Action: At the emergency department, ask the team to evaluate for a bowel obstruction with a CT scan, and tell them about your pancreatic cancer diagnosis and any recent change in vomiting or bowel movements.
How doctors confirm a bowel obstruction
Because a blockage is urgent, testing usually happens quickly, and treatment may begin alongside it.
Exam and blood tests
A clinician checks the belly for swelling, tenderness, and bowel sounds, and asks about your last bowel movement and any vomiting. Blood tests — a complete blood count, an electrolyte panel, and a urinalysis — help show dehydration and how your body is handling the blockage. The National Cancer Institute describes this same basic workup for a suspected obstruction.
Imaging — CT and X-ray
A CT scan is the main test; it shows where the blockage is and whether the bowel’s blood supply is affected. A plain abdominal X-ray can also reveal dilated loops of bowel and trapped air and fluid. For a plain-language overview, see MedlinePlus on intestinal obstruction.
How bowel obstruction is treated in pancreatic cancer
A blockage can often be relieved or managed, even when removing the cancer with surgery isn’t possible.
First steps — resting the gut, fluids, and decompression
Initial care usually means nothing to eat or drink for a while, fluids through a vein to correct dehydration, and sometimes a thin nasogastric tube through the nose to drain the stomach and ease pressure. These steps relieve symptoms while the team decides what comes next.
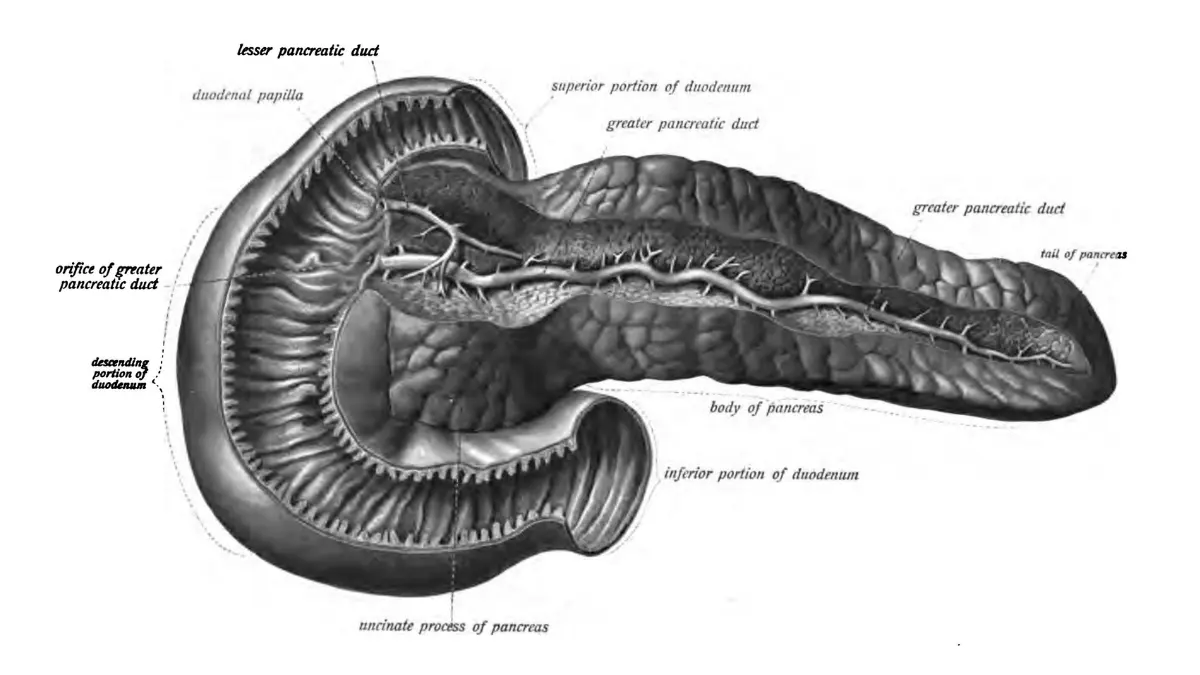
Adapted from AnatomyTool Servier Drawing Stomach and Duodenum, licensed under CC BY 3.0.
Procedures — a stent, surgical bypass, or a venting tube
For a blocked stomach outlet, a doctor may place a stent (a small expandable tube) during an endoscopy to reopen the passage, or perform surgery to route food around the blockage (a bypass). When the bowel is blocked and surgery isn’t an option, a venting gastrostomy — a tube placed through the abdominal wall — can drain fluid and ease nausea and vomiting.
| Approach | What it does | Best for |
|---|---|---|
| Endoscopic stent | Reopens a blocked stomach outlet without surgery; quicker recovery | Fast relief, or when someone isn’t well enough for surgery |
| Surgical bypass | Routes food around the blockage; can last longer | People healthy enough for surgery |
| Venting gastrostomy | Drains fluid to ease nausea and vomiting | Comfort-focused care when the bowel can’t be reopened |
General clinical education based on published reviews; your care team chooses the option that fits you.
Whether surgery is realistic depends on the cancer and your overall health — our guide on whether the cancer can be removed with surgery explains that, and you can see the full range of treatment options for pancreatic cancer too.
Medicines to ease symptoms
Doctors may use medicines to calm the gut and reduce nausea, including a medicine called octreotide that lowers digestive secretions, a steroid to reduce swelling around the blockage, and anti-nausea medicines.
🔬 How It Works: Octreotide is a lab-made version of a natural hormone (somatostatin). It slows the secretions that build up behind a blockage, reducing the volume of fluid and easing nausea and vomiting.
Palliative care focuses on comfort and symptom relief and can work alongside cancer treatment — not only at the end of life.
✅ Patient Action: Ask your oncology and palliative care team which option fits your goals — for example, “Given my overall health, is a stent, a bypass, or a venting tube the best way to relieve this blockage?”
What caregivers should watch for and do
Caregivers are often the first to notice a blockage starting, which makes a few simple daily checks valuable.
Daily signs worth tracking
Keep a quick note of whether food and fluids stay down, how the belly looks and feels, when the last bowel movement or passing of gas happened, and the level of pain. A clear pattern — vomiting, a swelling belly, and no bowel movements — is worth reporting promptly.
When to call the team versus go to the ER
Call the oncology team the same day for new or worsening vomiting, bloating, or constipation that’s out of the ordinary. Go to the emergency room for severe constant pain, vomiting that won’t stop, no passing of gas or stool, or fever — the red flags above. Noticing changes early gives the team more options.
Frequently asked questions about bowel obstruction in pancreatic cancer
1. Can pancreatic cancer cause a bowel obstruction?
Yes. Pancreatic cancer can cause a bowel obstruction in two ways: a tumor in the head of the pancreas can block the stomach’s outlet, and advanced cancer can spread to the abdomen and block the intestine lower down. Both interfere with how food, fluid, and gas move through the digestive tract.
2. What are the first signs of a bowel blockage with pancreatic cancer?
Early signs of a bowel obstruction often include nausea, vomiting, bloating, feeling full after a few bites, and cramping belly pain that comes in waves. When the blockage is higher up, vomiting tends to start early. Report new or worsening symptoms to your oncology team promptly.
3. Is a bowel obstruction in pancreatic cancer an emergency?
It can be. Seek emergency care for severe or constant abdominal pain, vomiting that won’t stop, a swollen belly with no passing of gas or stool, or fever. These can signal a complete bowel obstruction or a cut-off blood supply, which need urgent treatment. When in doubt, get evaluated.
4. What’s the difference between gastric outlet obstruction and bowel obstruction?
Gastric outlet obstruction is a blockage at the stomach’s exit, usually from a tumor in the head of the pancreas, so the stomach can’t empty. A lower bowel obstruction blocks the small or large intestine, often from cancer spreading to the abdomen. The symptoms and timing differ.
5. Can you still pass stool with a partial bowel obstruction?
Sometimes, yes. With a partial bowel obstruction, some stool or gas may still get through, though bowel movements often slow down. With a complete obstruction, passing gas or stool usually becomes impossible. A change like this with pancreatic cancer is worth reporting to your care team quickly.
6. How do doctors test for a bowel obstruction?
Doctors examine the belly, ask about vomiting and bowel movements, and run blood tests for dehydration. A CT scan is the main imaging test and shows where the bowel obstruction is; a plain X-ray can also help. Discuss any test results and next steps with your medical team.
7. Can a bowel obstruction from pancreatic cancer be treated without surgery?
Often, yes. A blocked stomach outlet can sometimes be reopened with an endoscopic stent, and a venting tube can ease nausea and vomiting when the bowel can’t be reopened. Medicines can reduce digestive secretions and nausea. Your oncology and palliative care team will recommend the best approach.
8. What is a venting gastrostomy?
A venting gastrostomy is a tube placed through the abdominal wall into the stomach to drain built-up fluid. For a bowel obstruction that can’t be reopened, it can relieve nausea, vomiting, and pressure, improving comfort. It’s a symptom-focused option your care team may suggest when surgery isn’t possible.
9. Does a bowel obstruction mean my pancreatic cancer is getting worse?
A bowel obstruction often occurs in more advanced pancreatic cancer, but it’s a complication to manage rather than a verdict on its own. Many blockages can be relieved or eased. What it means depends on factors like the cancer’s stage and your overall health, so discuss it directly with your oncology team.
10. What should caregivers watch for?
Caregivers can track whether food and fluids stay down, how the belly looks and feels, when the last bowel movement or passing of gas happened, and pain levels. A pattern of vomiting, a swelling belly, and no bowel movements should be reported to the oncology team promptly.
11. What does octreotide do for a bowel obstruction?
Octreotide is a medicine that lowers the digestive secretions that build up behind a blockage. By reducing that fluid, it can ease nausea and vomiting and improve comfort in a bowel obstruction, especially when surgery isn’t an option. Your medical team decides whether and how to use it.
The bottom line and your next step
Recognizing the signs of a bowel obstruction — vomiting, bloating, cramping, and no passing of gas or stool — lets you act quickly, which matters most when the emergency red flags appear. Even in advanced pancreatic cancer, the blockage can often be relieved or managed with a stent, surgery, a venting tube, or symptom medicines.
Keep your oncology and palliative care team in the loop about any change in symptoms or comfort. They can match the right approach to your situation and goals, and act sooner when you flag changes early.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.