On This Page – Quick Medical Summary
If someone close to you was just diagnosed, or you have a habit or condition you’ve been worried about, you’re probably asking a hard question: did something cause this, and could it happen to me? Here’s the honest starting point — pancreatic cancer rarely has a single, identifiable cause, and having a risk factor is not the same as having the disease.
This guide is built to be read three ways. If you’re weighing your own risk, the two sections on changeable and fixed risk factors are written for you. If you’re worried because pancreatic cancer runs in your family, skip ahead to the section on inherited risk. And if you’ve noticed something that concerns you, the warning-signs section explains when it’s worth raising with a doctor.
Most people with one or more risk factors never develop pancreatic cancer. Understanding which factors you can influence — and which you can’t — is what turns worry into something you can actually act on. For how the disease is found and treated, our overview of pancreatic cancer symptoms and stages walks through the full picture.
ℹ️ Medical Disclaimer: This article is general health information, not medical advice. It does not diagnose disease, recommend treatment, or replace genetic testing or screening decisions made with a professional. Risk factors describe statistical patterns across large populations, not predictions about any one person. For a personal risk assessment, genetic testing, or screening, consult a board-certified physician, a gastroenterologist, or a certified genetic counselor.
Do we actually know what causes pancreatic cancer?
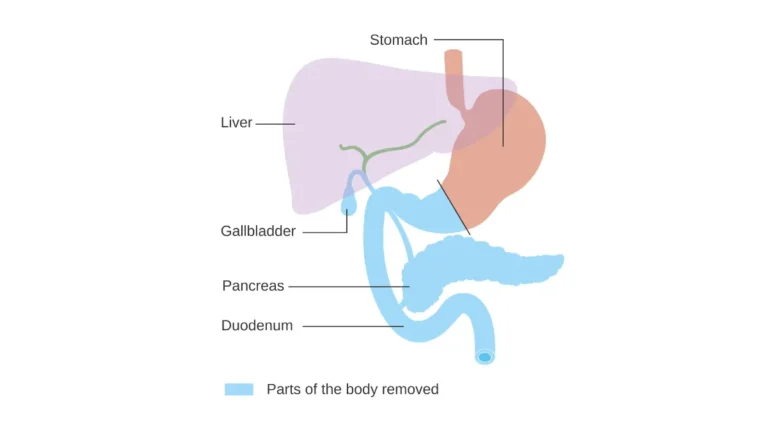
Pancreatic cancer begins when the DNA inside pancreatic cells changes and tells those cells to grow and divide when they shouldn’t. Researchers can describe how this process unfolds much better than they can pin down what set it off in any single person.
That gap is the key to this whole topic. A risk factor is anything that raises the statistical odds of a disease across a population; a true cause directly produces it. For most people with pancreatic cancer, no one can point to a single cause.
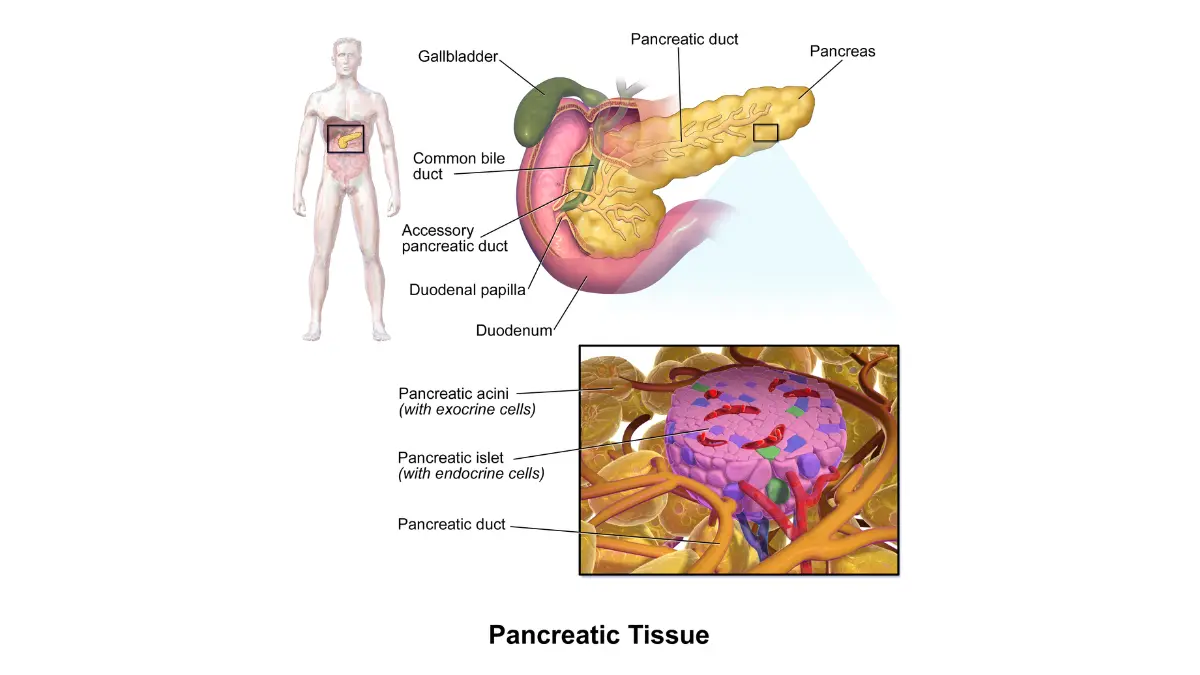
🔬 How It Works: Healthy cells follow DNA instructions that control when they grow and when they die. In pancreatic cancer, mutations switch those controls off, so cells keep multiplying and form a tumor. Most of these mutations are acquired during life — from aging, smoking, or chance errors when cells copy themselves — rather than inherited from a parent.
What’s the difference between a cause and a risk factor?
Think of risk factors as things that stack the odds, not things that seal a verdict. A lifelong smoker may never develop pancreatic cancer, while someone with no obvious risk factors might. The factors below shift probability; they don’t determine outcomes.
Why most cases aren’t inherited
Most pancreatic cancers are described as sporadic, meaning they come from acquired mutations and are not passed down through a family. Inherited gene changes explain only a minority of cases — a point we return to in the section on family history below.
Risk factors you can change
Some of the strongest known risk factors for pancreatic cancer are things you have at least some control over. The changeable ones include:
- Smoking — the single most important avoidable risk factor
- Excess body weight, especially around the waist
- Long-standing type 2 diabetes
- Chronic pancreatitis and heavy alcohol use
- Heavy workplace exposure to certain industrial chemicals
Smoking — the biggest changeable risk
Smoking is the clearest avoidable driver of pancreatic cancer, and the link strengthens with how much and how long a person smokes. Cigars and smokeless tobacco raise risk too. The encouraging part: risk starts to fall after a person quits.
📊 Clinical Data Point: People who smoke are about twice as likely to develop pancreatic cancer as people who never smoked, and roughly 25% of cases are thought to be caused by smoking. — Source: American Cancer Society
Excess weight and body fat
Carrying excess weight is an established risk factor, and where the weight sits seems to matter. Extra fat around the waistline may raise risk even in someone who isn’t obese overall.
📊 Clinical Data Point: People with obesity — a BMI of 30 or higher — are about 20% more likely to develop pancreatic cancer than people at a healthy weight. — Source: American Cancer Society
If you’re not sure where you fall, you can check your BMI as a starting point, keeping in mind it’s a rough screen, not a diagnosis.
Long-standing type 2 diabetes
Pancreatic cancer is more common in people with type 2 diabetes, though researchers don’t fully understand why the two are linked. Part of the overlap may trace back to excess weight, which raises the risk of both. There’s an important wrinkle here: sudden, new-onset diabetes in an older adult can sometimes be an early effect of a pancreatic tumor rather than a cause — which is why new-onset diabetes and pancreatic cancer is worth understanding on its own.
Chronic pancreatitis and heavy alcohol use
Chronic pancreatitis — long-term inflammation of the pancreas — is linked to a substantially higher risk of pancreatic cancer. It often appears alongside heavy alcohol use and smoking, which makes those exposures hard to untangle. Because the two conditions can look similar early on, it helps to understand the difference between pancreatitis and pancreatic cancer.
Heavy workplace chemical exposure
Heavy, sustained exposure to certain chemicals used in dry cleaning and metalworking may modestly raise risk. This is far less significant for most people than smoking or weight, but it matters for workers with years of occupational contact. You can read more in the American Cancer Society’s risk-factor overview.
Risk factors you can’t change
Other risk factors are simply part of who you are, and no lifestyle change will alter them. Knowing them helps you understand your baseline — without reading them as a sentence.
Age — mostly a disease of older adults
Pancreatic cancer is overwhelmingly a disease of later life, and risk climbs steadily with age. Cases before 45 are uncommon. If you’re younger and otherwise healthy, this is genuinely reassuring context.
📊 Clinical Data Point: The median age at diagnosis is 71, and about two-thirds of people diagnosed are 65 or older. — Source: NCI SEER, Cancer Stat Facts
Sex and race or ethnicity
The disease is slightly more common in men than in women. It’s also diagnosed more often in Black Americans than in other US groups, and researchers don’t yet fully understand why — some of the difference may be tied to higher rates of related risk factors, but that doesn’t explain all of it.
Family history
Having a first-degree relative — a parent, sibling, or child — with pancreatic cancer raises your risk, and the increase depends on how many relatives are affected. That doesn’t mean the disease is common; it remains relatively rare overall, even as it causes a large share of cancer deaths.
📊 Clinical Data Point: An estimated 67,530 Americans will be diagnosed with pancreatic cancer in 2026. It makes up only about 3% of new cancers but is the third-leading cause of US cancer death. — Source: American Cancer Society, Cancer Statistics 2026
You can explore current numbers in more detail through the latest SEER incidence and survival data. What family history actually means for you is the question the next section answers.
Is pancreatic cancer hereditary?
Most pancreatic cancers are not inherited. The large majority of people diagnosed have no known family link, a smaller group has a familial pattern, and only a small fraction is tied to a specific inherited genetic syndrome.
📊 Clinical Data Point: About 85–90% of people with pancreatic cancer have no known familial risk; an estimated 5–10% have familial risk, and roughly 3–5% are linked to an inherited genetic syndrome such as Peutz-Jeghers syndrome. — Source: U.S. Preventive Services Task Force
How often is it actually inherited?
If one relative had pancreatic cancer, that usually does not place you in a high-risk category. Doctors generally reserve the term “familial pancreatic cancer” for families with two or more affected first-degree relatives. So a single case in your wider family is worth mentioning to your doctor, but it rarely means intensive action.
Gene changes and syndromes linked to higher risk
A minority of pancreatic cancers trace to inherited mutations that run in families, often as part of a recognized syndrome. According to the National Cancer Institute, the inherited gene changes and syndromes most associated with higher risk include:
- BRCA1 and BRCA2 — best known for hereditary breast and ovarian cancer
- PALB2 and ATM — other genes seen in familial pancreatic cancer
- CDKN2A — linked to familial atypical multiple mole melanoma (FAMMM)
- STK11 — the gene behind Peutz-Jeghers syndrome
- Mismatch-repair genes (MLH1, MSH2, MSH6, PMS2) — the basis of Lynch syndrome
- PRSS1 — associated with hereditary pancreatitis
When to consider a genetic counselor
Genetic testing is a decision you make with a professional, not from a web page — results carry real implications for you and your relatives, and they need expert interpretation. A genetic risk assessment can help you organize your family history before that conversation, and understanding how pancreatic cancer is diagnosed can prepare you for what comes after.
✅ Patient Action: If two or more close blood relatives have had pancreatic cancer, or a relative carries a known mutation such as BRCA2, ask your doctor for a referral to a certified genetic counselor and ask directly: “Does my family history meet the criteria for genetic testing?”
Can you lower your risk — and should you be screened?
You can’t erase your risk of pancreatic cancer, but the changeable factors give you real levers to pull:
- Don’t smoke — or get support to quit
- Reach and keep a healthy weight
- Limit alcohol
- Manage type 2 diabetes with your care team
Steps that genuinely lower risk
The most effective steps mirror the modifiable risk factors: not smoking does the most, followed by maintaining a healthy weight and limiting alcohol. These won’t guarantee anything, but across a population they measurably reduce risk, and they protect against far more than this one disease.
Why there’s no routine screening for most people
This is where honest expectation-setting matters. There is no mammogram-equivalent for the pancreas, and screening healthy people can do more harm than good.
📊 Clinical Data Point: The U.S. Preventive Services Task Force recommends against screening for pancreatic cancer in average-risk adults who have no symptoms, because no test has been shown to find it early enough to save lives without causing significant harm. — Source: U.S. Preventive Services Task Force
Who may qualify for high-risk surveillance
That recommendation does not apply to people at high risk — those with certain inherited syndromes or a strong family history. For them, specialists sometimes offer surveillance using endoscopic ultrasound or MRI, but whether and when to do it is a clinical decision made case by case, not something to start on your own.
✅ Patient Action: If you have an inherited syndrome or a strong family history, ask a gastroenterologist or your genetic counselor: “Do I qualify for a high-risk pancreatic surveillance program, and what would it involve?”
When higher risk should prompt a conversation with your doctor
Risk awareness is only useful if you know when to act on it. A few specific situations are worth raising promptly rather than waiting.
⚠️ Clinical Warning: In an adult over 50, suddenly developing type 2 diabetes — especially alongside weight loss you can’t explain — can occasionally be an early sign of pancreatic cancer rather than ordinary diabetes. It usually isn’t cancer, but it’s worth prompt evaluation.
New diabetes after 50 with unexplained weight loss
New diabetes on its own is common and usually unrelated to cancer. The combination that deserves attention is new diabetes plus losing weight without trying, which is one reason unexplained weight loss is taken seriously. It’s also worth knowing the early signs of pancreatic cancer so you can describe anything unusual clearly.
A strong family pattern
If several close relatives have had pancreatic cancer — or a related cancer such as breast, ovarian, or melanoma in a pattern — that’s a reason to start a genetic-counseling conversation rather than to panic.
✅ Patient Action: If you’ve recently developed diabetes and have lost weight without trying, ask your primary care doctor: “Given these changes, is any further evaluation of my pancreas warranted?”
Frequently asked questions about pancreatic cancer risk
1. What is the main cause of pancreatic cancer?
There is no single cause of pancreatic cancer. It begins when DNA changes make pancreatic cells grow uncontrollably, and the strongest known risk factor is smoking, linked to about a quarter of cases. In most people, doctors can’t trace the disease to one specific cause, which is why they talk about risk factors rather than causes.
2. Does smoking cause pancreatic cancer?
Smoking is the single biggest avoidable risk factor for pancreatic cancer. People who smoke are about twice as likely to develop it as those who never smoked, and roughly 25% of cases are thought to be smoking-related. Cigars and smokeless tobacco also raise risk, and quitting lowers it over time.
3. Can diabetes cause pancreatic cancer?
Pancreatic cancer is more common in people with type 2 diabetes, though the reason isn’t fully understood. Importantly, sudden new diabetes in an older adult can sometimes be an early sign of a pancreatic tumor rather than a cause. If you develop diabetes alongside unexplained weight loss, discuss it promptly with your doctor.
4. Does being overweight raise the risk of pancreatic cancer?
Yes. People with obesity — a BMI of 30 or higher — are about 20% more likely to develop pancreatic cancer than people at a healthy weight. Carrying excess fat around the waistline may raise risk even in someone who isn’t obese overall, so where weight sits matters, not just the number on the scale.
5. Is pancreatic cancer hereditary?
Most pancreatic cancer is not inherited. About 85–90% of people diagnosed have no known family link; roughly 5–10% have a familial pattern, and about 3–5% are tied to an inherited syndrome such as a BRCA2 mutation. A certified genetic counselor can assess whether testing makes sense for you.
6. Should I get genetic testing if a relative had pancreatic cancer?
Not automatically. A single affected relative usually doesn’t place you in a high-risk group. Genetic testing is a decision made with a genetic counselor based on your full family history, including related cancers like breast or ovarian. Ask your doctor for a referral if the pattern in your family concerns you.
7. At what age does pancreatic cancer usually develop?
Pancreatic cancer is largely a disease of older adults. The median age at diagnosis is 71, and about two-thirds of people diagnosed are 65 or older. Cases before age 45 are uncommon, which means younger, otherwise-healthy adults face a genuinely low baseline risk.
8. Does alcohol cause pancreatic cancer?
Heavy alcohol use is linked to chronic pancreatitis — long-term inflammation of the pancreas — which itself raises pancreatic cancer risk. Heavy drinking and smoking often occur together, which makes their effects hard to separate. Limiting alcohol is one of the changeable steps that lowers your overall risk.
9. Who is most at risk of pancreatic cancer?
Risk is highest in older adults, people who smoke, and those with obesity or long-standing type 2 diabetes. Chronic pancreatitis, heavy alcohol use, being a Black American, and having a strong family history or inherited syndrome also raise risk. Most people with these factors still never develop the disease.
10. Can you lower your risk of pancreatic cancer?
You can’t eliminate it, but you can lower it. Not smoking, keeping a healthy weight, limiting alcohol, and managing type 2 diabetes with your care team all reduce risk across a population. There is no proven screening test for people at average risk, so prevention focuses on these everyday factors.
11. Can pancreatic cancer be detected early in high-risk people?
For most people, no screening test is recommended. People with certain inherited syndromes or a strong family history may be offered surveillance with MRI or endoscopic ultrasound under specialist care. Whether you qualify is a decision your doctor or genetic counselor makes based on your individual risk.
The bottom line on pancreatic cancer risk
The honest takeaway is steadying: risk factors stack the odds, but they don’t decide your future, and most people who have them never develop pancreatic cancer. The changeable factors — smoking, weight, alcohol, and diabetes management — are worth acting on precisely because they’re within reach and protect your health broadly.
If pancreatic cancer runs in your family, the right next step isn’t worry — it’s a conversation with your doctor or a certified genetic counselor about whether your history warrants testing or surveillance. For the wider picture of how this disease develops, is diagnosed, and is treated, our guide to pancreatic cancer symptoms and stages is the place to continue.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.