On This Page – Quick Medical Summary
If you’re Black and you’ve seen a headline tying your community to pancreatic cancer, the worry makes sense — and the underlying facts are real. Black Americans carry the highest pancreatic cancer incidence of any racial or ethnic group in the United States. The size of that gap is only half the story, though, because most of what drives it can be acted on.
This guide is built around why you’re here, and it sits alongside our full picture of pancreatic cancer symptoms and stages. If you want the actual numbers, start with how much higher the risk really is. If a relative was just diagnosed, the sections on outcomes and on care gaps will matter most. If pancreatic cancer runs in your family, the part on biology speaks to you, and if you’re noticing symptoms now, go straight to the warning signs.
The thread through all of it: this disparity is shaped mainly by risk factors and access to care — not by anything inherent to race.
ℹ️ Medical Disclaimer: This article is general health education, not medical advice. It does not diagnose pancreatic cancer, recommend treatment or medication, or replace personalized screening or risk counseling, and the statistics here describe populations rather than your individual outcome. For decisions about your own risk, symptoms, family history, or testing, consult a board-certified gastroenterologist, oncologist, or your primary care physician.
How much higher is pancreatic cancer risk for Black Americans?
Black Americans are diagnosed with pancreatic cancer at a rate roughly 30% to 70% higher than other racial groups — the highest incidence of any group tracked by the National Cancer Institute. That gap has persisted for decades, and it appears in deaths as well as diagnoses.
📊 Clinical Data Point: Overall 5-year relative survival for pancreatic cancer is about 13%, and roughly 11% for Black patients. — Source: American Cancer Society, Cancer Statistics 2025.
These figures describe large populations, not any single person. A relative survival rate compares people with this cancer to people without it, and it reflects those diagnosed at least five years ago — before several recent treatment advances. Your own outlook depends on stage at diagnosis, tumor biology, overall health, and treatment, which is why the American Cancer Society’s survival-rate explainer stresses asking your care team how the numbers apply to you.
Black Americans also have somewhat higher age-adjusted mortality than White Americans, according to the NCI’s surveillance data. The reasons sit in the next three sections — and most of them are changeable.
Why the gap exists: the risk factors doing most of the work
Most of the excess risk traces back to a handful of risk factors that are simply more common in Black communities. The leading ones are cigarette smoking, long-standing type 2 diabetes, obesity, and heavy alcohol use.
🔬 How It Works: Chronic inflammation and metabolic stress — from smoking’s carcinogens, years of high blood sugar, or excess body fat — repeatedly damage pancreatic cells. Over time, that damage raises the chance a cell turns cancerous.
These exposures are shaped by social and economic conditions, not personal failing, and the research shows the pattern differs by sex. In men, established factors — smoking, long-term diabetes, and family history — explain almost the entire Black–White gap; in women, alcohol and higher body weight contribute more. Notably, a peer-reviewed review of these disparities finds that known risk factors still don’t fully account for the gap — which is why access and biology also matter.
If weight is one of your factors, you can check where your BMI falls, and our guide to what causes pancreatic cancer covers which exposures are within reach.
The part that isn’t about you: access and care gaps
A meaningful share of the disparity comes from the care system, not the patient. Studies of treatment patterns show Black and White patients are recommended surgery at similar rates, yet Black patients are less likely to actually undergo the operation that offers the best chance of long-term survival.
Two other gaps compound this. Black patients remain under-represented in pancreatic cancer clinical trials, which shapes how well new therapies get studied across populations. And unlike breast, colon, lung, or prostate cancer, pancreatic cancer has no standard screening test for average-risk people, so most cases are found late.
✅ Patient Action: If you or a relative is facing pancreatic cancer, ask directly: “Can I be referred to a high-volume pancreatic center, and am I a candidate for surgery or a clinical trial?”
You can read how pancreatic cancer clinical trials work and who can join, or search open studies at the federal clinical trials registry

Adapted from Wikimedia Commons NIAID Clinical Trial Stream, licensed under CC BY 2.0.
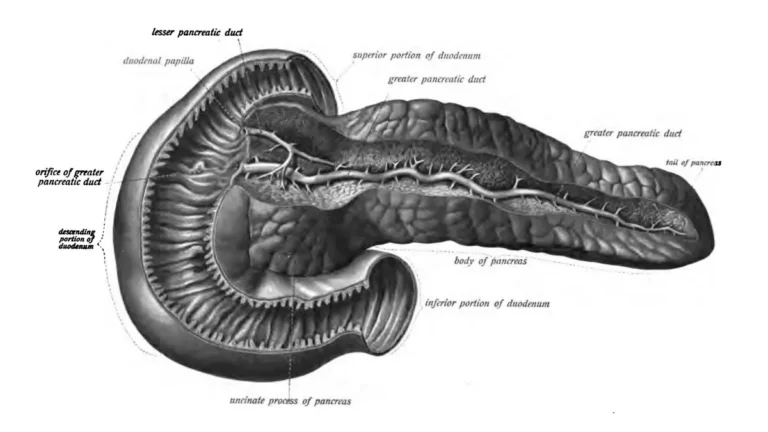
Is pancreatic cancer genetic? What the biology actually says
The fear that this risk is locked in by ancestry is the one worth meeting head-on, and the current evidence does not support it.
🩺 Physician Note: Researchers emphasize that the inherited risk of pancreatic cancer is thought to be broadly similar across racial groups. The biological differences under study are in tumor characteristics and in risk-factor exposure — not in race itself.
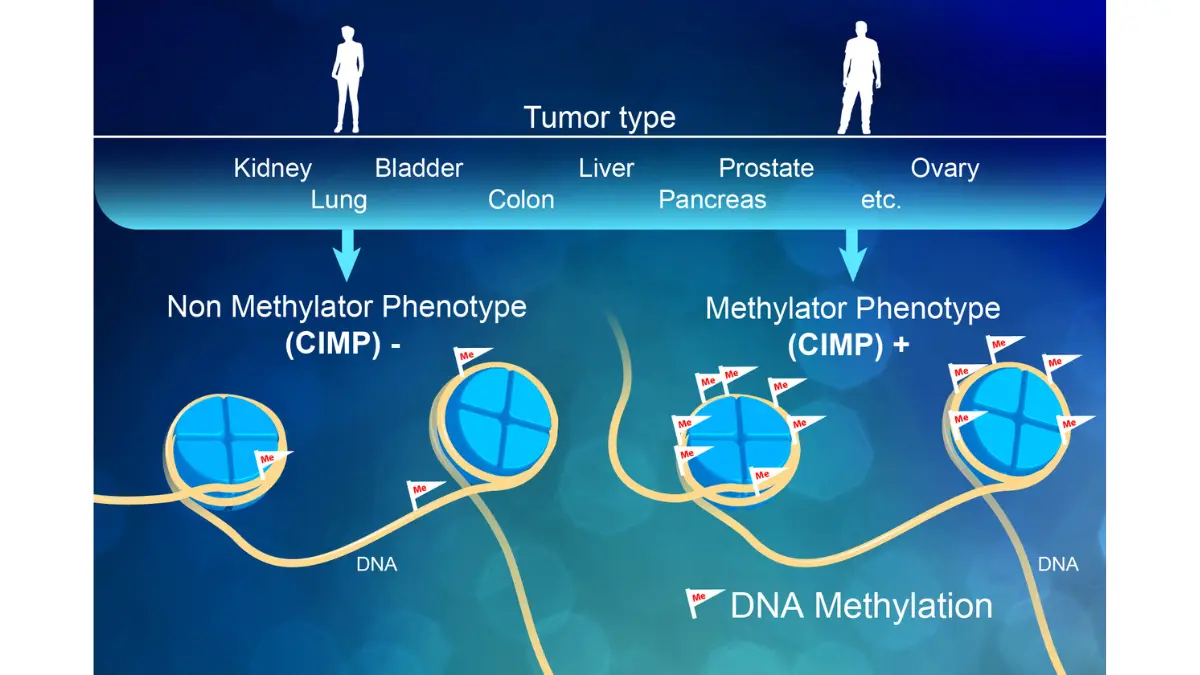
What differs is more specific. DNA methylation — chemical tags that switch genes on or off without altering the DNA code itself — has been observed to vary between Black and White individuals, and certain tumor mutations (including KRAS) and immune markers appear more often in Black patients.
🔬 How It Works: Think of methylation as a dimmer switch sitting on top of a gene: it can turn the gene’s activity up or down without rewriting the gene. These patterns are an active research frontier, not a verdict on any individual.
Adapted from Wikimedia Commons Darryl Leja NHGRI, licensed under CC BY 2.0.
Family history is the genetic factor that clearly matters for you — a close relative with pancreatic cancer raises your risk. Our explainer on whether pancreatic cancer is hereditary covers what counts as a meaningful family pattern.
What you can actually do to lower your risk
Because so much of the gap runs through modifiable factors, several evidence-backed steps genuinely lower risk:
- Stop smoking — the single most important change, with benefit that grows the longer you stay quit.
- Manage blood sugar if you have type 2 diabetes, and ask about it if you don’t.
- Reach and hold a healthier weight, since obesity is a consistent contributor.
- Limit alcohol, which weighs more heavily in the data for women.
- Bring your family history to a doctor so it can be factored into your care.
✅ Patient Action: At your next visit, ask your primary care physician: “Given my family history and risk factors, do I need genetic counseling or any monitoring?” If two or more close relatives had pancreatic cancer, a genetic counselor referral is reasonable to raise.
None of this guarantees prevention — it shifts the odds. To weigh inherited risk, you can gauge your genetic risk and read about genetic testing for pancreatic cancer before that conversation.
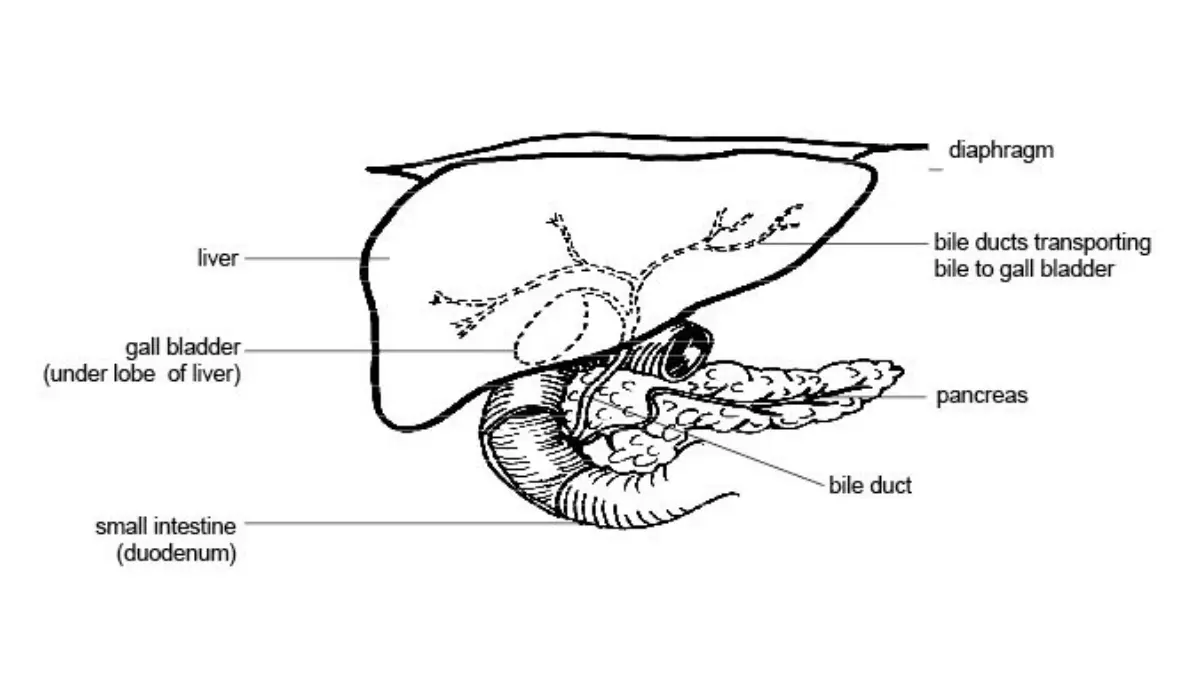
Warning signs — and pushing to be taken seriously
Pancreatic cancer is hard to catch early because its symptoms are easy to mistake for ordinary problems. The ones worth a prompt medical visit include:
- Yellowing of the skin or eyes (jaundice)
- Unexplained weight loss
- Pain in the upper abdomen that may radiate to the back
- New-onset diabetes without an obvious cause
- Pale, greasy stools or dark urine

Adapted from Wikimedia Commons CDC Public Health Image Library, licensed under Public Domain.
Most of these have benign explanations, and only a clinician can sort that out — so the goal is evaluation, not self-diagnosis. If your concerns are brushed aside, it is reasonable to ask why a test is or isn’t being ordered, and to seek a second opinion.
✅ Patient Action: Tell your primary care physician (or ask for a gastroenterology referral): “Could these symptoms warrant imaging or further work-up — and if not, what is the reason?”
You can run your symptoms through our symptom checker as a starting point, read the early signs of pancreatic cancer in more depth, or see the National Library of Medicine’s plain-language overview.
Pancreatic cancer in Black Americans: common questions
1. What is the survival rate for Black pancreatic cancer patients?
The 5-year relative survival is about 11% for Black patients, compared with roughly 13% overall (American Cancer Society, 2025). These are population figures, not an individual prognosis, and outcomes depend heavily on stage at diagnosis. Ask your oncologist how they apply to your specific situation.
2. Why do Black Americans have higher pancreatic cancer rates?
The higher rate of pancreatic cancer in Black Americans is driven mainly by more prevalent modifiable risk factors — smoking, long-term diabetes, and obesity — shaped by social conditions, plus gaps in access to care. It is not caused by inherent racial biology.
3. Is pancreatic cancer genetic in African Americans?
Inherited risk is thought to be broadly similar across racial groups. Family history clearly raises risk, and some tumor biology differs and is being studied, but pancreatic cancer in African Americans is not written into race. Discuss a strong family history with your doctor.
4. What are the main risk factors for Black Americans?
The leading risk factors are cigarette smoking, long-standing type 2 diabetes, obesity, heavy alcohol use, and a family history of pancreatic cancer. Most are modifiable, which is why awareness and early lifestyle changes can meaningfully shift personal risk over time.
5. Does diabetes increase pancreatic cancer risk?
Yes — long-standing type 2 diabetes is an established risk factor and is more common among Black Americans. New-onset diabetes without a clear cause can occasionally be an early warning sign of pancreatic cancer. Raise unexplained new diabetes with your physician.
6. Can Black Americans lower their pancreatic cancer risk?
Yes. Quitting smoking, managing blood sugar and weight, and limiting alcohol all reduce risk, and discussing family history allows appropriate monitoring. None of these guarantees prevention, but together they improve the odds. Your doctor can tailor specific steps to your situation.
7. Do Black patients get worse pancreatic cancer treatment?
Research shows similar surgery recommendations but lower rates of actually receiving surgery, plus under-representation in clinical trials. These are care-access gaps you can push against by seeking a high-volume center and a second opinion. Ask your team directly about surgery and trial eligibility.
8. What are early warning signs of pancreatic cancer?
Jaundice, unexplained weight loss, upper-abdominal or back pain, new-onset diabetes, and pale stools or dark urine are recognized signs. Most have harmless causes, so they call for medical evaluation rather than alarm. See a clinician promptly if several appear together or persist.
9. Is pancreatic cancer more deadly for Black Americans?
Black Americans have higher mortality and lower 5-year survival than White Americans. This is driven largely by risk-factor prevalence, later-stage diagnosis, and access gaps — not by an unchangeable racial trait. Earlier evaluation and more equitable care narrow the difference.
10. Should Black Americans get screened for pancreatic cancer?
There is no standard screening test for average-risk adults. People with a strong family history or known genetic risk should ask a doctor about genetic counseling and whether high-risk monitoring applies. Routine population screening is not currently available for this cancer.
11. Does family history change my risk?
Yes — a first-degree relative with pancreatic cancer raises your risk and may justify genetic counseling. Ask your clinician whether your family pattern meets the threshold for testing or monitoring. This is one of the clearest, most actionable pieces of your personal risk picture.
The bottom line — and your next step
The disparity is real: Black Americans face the highest pancreatic cancer incidence in the country and worse survival. But the largest forces behind it — smoking, diabetes, obesity, and unequal access to surgery and trials — are the kind that respond to action, both personal and systemic.
The single most useful thing you can do is turn this from a statistic into a conversation. Bring your risk factors and family history to your next appointment, and ask what they mean for you specifically. That one step does more than any number on this page.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.