CMV Test Pregnancy: What Your Results Really Mean (2025)
A CMV test pregnancy measures cytomegalovirus antibodies (IgG and IgM) in your blood to determine if you have a current, past, or no infection. Understanding your CMV test results is critical because primary CMV infection during pregnancy carries a 30-40% transmission risk to your baby, while past infection reduces this to just 1-3%.
When Sarah’s Routine Test Changed Everything
Sarah, a 29-year-old first-time mom in her second trimester, never expected her routine prenatal screening to reveal CMV positive pregnancy results. Like 60-80% of infected pregnant women, she had no CMV pregnancy symptoms—no fever, no fatigue, nothing. But her blood work showed both IgG and IgM antibodies, launching her into a whirlwind of specialist appointments, ultrasounds, and anxiety about what this meant for her baby.
Her story mirrors thousands of expecting mothers who discover cytomegalovirus pregnancy diagnoses each year. With proper testing interpretation and expert guidance using tools like the Pregnancy Due Date Calculator to track gestational timing, Sarah learned to navigate her diagnosis with confidence.
What You’ll Learn in This Complete Guide
- How to interpret your CMV IgG positive pregnancy and CMV IgM positive pregnancy results with specific antibody ranges
- What CMV avidity test scores mean—including exact percentage breakdowns that determine infection timing
- Critical differences between primary CMV infection pregnancy versus reactivation or reinfection
- Trimester-specific risks: Why CMV pregnancy first trimester exposure matters most for congenital CMV outcomes
- Actionable prevention strategies backed by 2025 research from CDC and international health authorities
- When CMV screening pregnancy is recommended and what CMV blood test pregnancy options exist
Understanding CMV in Pregnancy: The Clinical Context
Cytomegalovirus belongs to the herpesvirus family and remains one of the most common congenital infections worldwide. In the United States, approximately 1 in 200 babies is born with congenital CMV, making it the leading infectious cause of birth defects and non-genetic hearing loss.
The Centers for Disease Control and Prevention confirms that CMV transmission to baby occurs most frequently during first-trimester primary infections, when the developing fetal organs are most vulnerable. However, most pregnant women considering CMV screening pregnancy don’t realize that 60-90% of congenitally infected infants show no symptoms at birth.
Current CMV antibody test pregnancy protocols use blood serology to detect IgG (indicating past exposure) and IgM (suggesting recent or current infection) antibodies. When results show both antibodies present, a CMV avidity test becomes essential to determine whether infection occurred before conception or during pregnancy—a distinction that fundamentally changes risk assessment and clinical management.
Tracking your pregnancy milestones with tools like the Pregnancy Weight Gain Calculator helps contextualize when testing should occur and how gestational age affects result interpretation.
⚠️ Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult your healthcare provider or maternal-fetal medicine specialist for personalized guidance regarding CMV test pregnancy results and management decisions.
Understanding Your CMV Blood Test Pregnancy Results
When you receive CMV test pregnancy results, you’re looking at blood serology that detects specific antibodies your immune system produces in response to cytomegalovirus exposure. These CMV antibody test pregnancy results provide crucial timing information—but only when interpreted correctly with clinical context and gestational age from tools like your Pregnancy Due Date Calculator.
Types of CMV Antibody Test Pregnancy
Modern CMV blood test pregnancy protocols utilize three distinct antibody assessments, each revealing different aspects of infection timing and immunity status:
CMV IgG Antibody Test: Detects immunoglobulin G antibodies that develop 2-3 weeks after initial infection and persist lifelong. According to University of Iowa Health Care laboratory standards, results below 0.8 AI (antibody index) indicate no previous CMV positive pregnancy exposure, while values above 1.0 AI confirm past infection. The CDC emphasizes that a positive CMV IgG positive pregnancy result alone cannot distinguish between recent and remote infection.

CMV IgM Antibody Test: Measures immunoglobulin M antibodies that appear during acute infection phases. However, CMV IgM positive pregnancy results carry significant interpretation challenges—up to 90% are false positives due to cross-reactivity with other antibodies, reactivation events, or autoimmune conditions. This exceptionally high false-positive rate makes IgM alone inadequate for diagnosing primary CMV infection pregnancy.
CMV Avidity Test: Determines IgG antibody maturity by measuring binding strength. This critical test distinguishes recent infections (occurring within 3-4 months) from older exposures, making it essential when both IgG and IgM are positive during CMV screening pregnancy.
CMV Test Results Explained: Complete Breakdown
Your CMV test results explained depend on antibody combinations and timing. Here’s the comprehensive interpretation framework used by maternal-fetal medicine specialists:
| Test Result Combination | What It Means | Infection Timing | Transmission Risk to Baby | Next Steps |
|---|---|---|---|---|
| IgG Negative, IgM Negative | No CMV exposure detected | Never infected | 0% current risk | Practice strict prevention; consider repeat testing if high-risk exposure |
| IgG Positive, IgM Negative | Past CMV positive pregnancy (immunity present) | Infection occurred >6 months ago | 1-3% (reactivation/reinfection) | Routine prenatal monitoring; assess via Pregnancy Weight Gain Calculator |
| IgG Negative, IgM Positive | Probable primary CMV infection pregnancy | Within last 6 weeks | 30-40% (highest risk) | URGENT: Maternal-fetal medicine referral; repeat testing in 2-3 weeks; avidity testing |
| IgG Positive, IgM Positive | Requires further testing | Uncertain—needs avidity | Variable (5-40%) | CMV avidity test mandatory to determine timing |
| IgG Equivocal (0.9-1.0 AI) | Borderline result | Early seroconversion possible | Unknown until clarified | Repeat in 10-14 days per University of Washington Medical Center protocols |
Critical Note: Research published in the American Journal of Obstetrics and Gynecology confirms that 10-28% of pregnant women with primary CMV infection pregnancy may not show detectable IgM antibodies, creating false reassurance. This underscores why CMV pregnancy symptoms evaluation and exposure history matter as much as laboratory values.
What Does CMV Positive Mean? Breaking Down the Numbers
When reviewing your CMV test results, specific numerical thresholds determine positive versus negative status. Understanding these ranges helps you contextualize what does CMV positive mean for your pregnancy:
CMV IgG Positive Pregnancy Ranges:
- <0.8 AI: Negative—no detectable antibodies
- 0.9-1.0 AI: Equivocal—possible early seroconversion requiring repeat testing
- >1.0 AI: Positive—confirms past or current infection
The CDC Laboratory Testing Guidelines recommend paired samples taken 1-3 months apart to diagnose primary CMV infection pregnancy through seroconversion (first sample negative, second positive).
CMV IgM Positive Pregnancy Interpretation:
- <0.8 AI: Negative—no acute infection markers
- >1.0 AI: Positive—suggests recent infection, reactivation, or false positive
False Positive Considerations: Women with autoimmune conditions (lupus, antiphospholipid syndrome) show false-positive CMV IgM rates of 16.5% compared to just 0.9% in healthy pregnancies. These false positives paradoxically correlate with worse pregnancy outcomes—including earlier delivery and intrauterine growth restriction—making comprehensive evaluation through Genetic Risk Assessment Tool screening valuable.
Cross-reactivity creates additional false positives in women with Epstein-Barr virus, parvovirus B19, or during CMV pregnancy first trimester hormonal changes when immune system modulation peaks.
What This Means For You
If your results show IgG+/IgM-: You have immunity from past infection, likely acquired before conception. Your CMV negative pregnancy risk for primary infection is essentially eliminated, though 1-3% reactivation risk remains manageable through routine prenatal care.
If your results show IgG-/IgM+: This represents potential primary CMV infection pregnancy—the highest-risk scenario. Contact your maternal-fetal medicine specialist within 48 hours for avidity testing and serial ultrasound planning.
If your results show IgG+/IgM+: Don’t panic—remember 90% of IgM positives are false. Avidity testing (covered in Section 3) definitively determines whether infection occurred before or during pregnancy, fundamentally changing your congenital CMV risk assessment.
The CMV Avidity Test – Your Critical Timeline Indicator
CMV IgG Avidity: The Test That Determines Your Infection Timeline
When your CMV blood test pregnancy shows both IgG and IgM antibodies positive, the CMV avidity test becomes your most powerful diagnostic tool for determining infection timing. This single test can differentiate between a primary CMV infection pregnancy requiring intensive monitoring and a pre-conception infection with minimal fetal risk—potentially eliminating 90% of your anxiety in one result.

How the CMV Avidity Test Works
CMV IgG avidity measures antibody maturity by testing binding strength between IgG antibodies and viral antigens. During acute cytomegalovirus pregnancy infections, your immune system produces low-avidity (weak-binding) IgG antibodies that gradually mature into high-avidity (strong-binding) antibodies over 3-6 months.
The test uses a chemical wash step—low-avidity antibodies detach easily while mature antibodies resist removal. Results appear as an avidity index percentage that directly correlates with infection age. According to National Institutes of Health research, avidity testing demonstrates 95-100% negative predictive value for ruling out recent infections when high avidity is detected in the first trimester.
Maternal-fetal medicine specialists order CMV avidity test protocols when CMV IgM positive pregnancy results create diagnostic uncertainty. The CDC recommends avidity testing as a critical component of comprehensive CMV screening pregnancy in high-risk populations.
CMV Avidity Test Results Interpretation
Understanding your CMV IgG avidity percentage determines whether you need high-risk pregnancy management or routine prenatal care. Here’s how specialists interpret these critical numbers:
| Avidity Result | Percentage Range | Infection Timeline | Risk Level | Clinical Meaning |
|---|---|---|---|---|
| Low Avidity | <30-40% | Within last 12-16 weeks | HIGH RISK | Confirms primary CMV infection pregnancy; 30-40% transmission probability |
| Intermediate Avidity | 40-60% | 3-5 months ago | Moderate-Uncertain | Borderline window; may need repeat testing in 2-3 weeks with clinical correlation |
| High Avidity | >60-70% | >4-6 months before conception | LOW RISK | Rules out recent infection; reduces to 1-3% reactivation risk |
| Very High Avidity | >80% | >12 months ago | Minimal Risk | Strong immunity; standard prenatal care sufficient |
Real Patient Case: Maria, 32, discovered CMV positive pregnancy at 14 weeks with both IgG and IgM detected. Her initial panic transformed to relief when avidity testing revealed 78% high avidity—definitively proving infection occurred at least 6 months before conception. Her baby was born healthy without congenital CMV, demonstrating how avidity testing prevents unnecessary interventions while identifying truly high-risk pregnancies.
The University of Iowa Hospitals emphasizes that avidity interpretation must account for laboratory-specific cutoffs, which vary between testing platforms from 30-50% for low avidity thresholds.
Timing Matters: CMV Avidity by Trimester
CMV avidity test interpretation changes based on when testing occurs during pregnancy. Understanding these trimester-specific implications helps contextualize your results alongside tracking tools like the Fetal Growth Percentile Calculator:
First Trimester Avidity Testing (Weeks 1-13):
- High avidity: Definitively rules out recent infection; provides maximum reassurance
- Low avidity: Confirms CMV pregnancy first trimester primary infection—highest risk period for congenital CMV symptoms
- Optimal timing: Testing before 12 weeks offers clearest diagnostic certainty
- Action: High avidity eliminates need for serial ultrasounds beyond routine anatomy scans
Second Trimester Avidity Testing (Weeks 14-27):
- High avidity: Still helpful but less definitive—could represent infection occurring 4-6 months prior (late first trimester)
- Intermediate avidity: More common; requires clinical judgment combining exposure history and CMV pregnancy symptoms
- Limitation: Six-month window means high avidity doesn’t completely exclude early pregnancy infection
- Strategy: Combine with detailed ultrasound examination for CMV ultrasound findings markers
Third Trimester Avidity Testing (Weeks 28-40):
- Limited clinical utility: High avidity expected even with second-trimester infections
- Primary use: Retrospective diagnosis if CMV baby symptoms appear at birth
- Focus shifts: From avidity to ultrasound monitoring and amniocentesis consideration
- Planning: Coordinate neonatal testing regardless of maternal avidity results
What This Means For You
If you have high avidity (>60%) in first trimester: Breathe easier. Your infection occurred before pregnancy, dramatically reducing CMV transmission to baby risk to baseline 1-3%. Continue routine prenatal care with your Pregnancy Weight Gain Calculator tracking and standard anatomy ultrasound at 20 weeks.
If you have low avidity (<40%) at any trimester: This confirms primary CMV infection pregnancy requiring immediate maternal-fetal medicine consultation. Serial ultrasounds every 2-4 weeks will monitor for growth restriction, brain calcifications, and other CMV ultrasound findings. Amniocentesis discussion becomes relevant after 20-21 weeks gestation to directly test fetal infection status.
If you have intermediate avidity (40-60%): Request repeat testing in 2-3 weeks. Rising avidity suggests older infection, while persistent intermediate values may indicate infection during the ambiguous 3-5 month window requiring individualized counseling and enhanced monitoring.
CMV Infection Pregnancy Risks & Congenital Cmv
Primary CMV Infection Pregnancy vs. Reactivation: Understanding the Risks
The distinction between primary CMV infection pregnancy (first-time infection) and reactivation (reawakening of dormant virus) fundamentally determines your baby’s risk profile. Understanding these differences helps you interpret your CMV positive pregnancy results and guides appropriate monitoring strategies.
CMV Transmission to Baby: The Real Numbers
Primary CMV infection pregnancy transmission rates dramatically exceed reactivation scenarios. When mothers acquire their first cytomegalovirus pregnancy infection during gestation, vertical transmission occurs in 30-40% of cases according to CDC epidemiological data. This high rate reflects the absence of maternal antibodies to protect the developing fetus during critical organ formation periods.
In contrast, mothers with pre-existing immunity face just 1-3% transmission risk from viral reactivation. Their established antibody repertoire provides partial fetal protection even when dormant virus reactivates due to pregnancy-related immune suppression. However, reinfection with different CMV strains—occurring in 2-5% of seropositive mothers—creates intermediate risk between primary infection and simple reactivation.
Trimester timing profoundly impacts CMV transmission to baby outcomes. First-trimester primary CMV infection pregnancy carries the highest symptomatic disease risk (25-30%), while third-trimester transmission, though more frequent (40-50%), usually produces milder or asymptomatic congenital CMV. Tracking gestational timing through tools like your Pregnancy Due Date Calculator helps contextualize these risk calculations.
International data from European, Asian, and Latin American cohorts confirm these transmission patterns across diverse populations, with primary infection consistently demonstrating 10-15 times higher transmission than reactivation regardless of geographic region.
Congenital CMV: What Happens When Baby Gets Infected
Congenital CMV represents the most common non-genetic cause of childhood hearing loss and the leading infectious cause of birth defects in developed nations. Among infected newborns, 85-90% appear completely healthy at birth—but 10-15% develop delayed symptoms, particularly progressive CMV hearing loss baby complications that emerge by age 4-6 years.
The spectrum of CMV baby symptoms ranges from subtle developmental delays to severe multi-organ involvement. Symptomatic newborns face 40-58% risk of long-term neurodevelopmental disabilities including intellectual impairment, cerebral palsy, and vision loss. Even asymptomatic infants carry 10-15% risk of developing sensorineural CMV hearing loss baby complications, often not detected until school age when speech and language delays become apparent.
Congenital CMV symptoms severity correlates with infection timing—earlier gestational age at maternal infection predicts worse outcomes. Brain development during the first 20 weeks makes neural structures particularly vulnerable to viral damage, resulting in structural abnormalities visible on ultrasound and MRI.
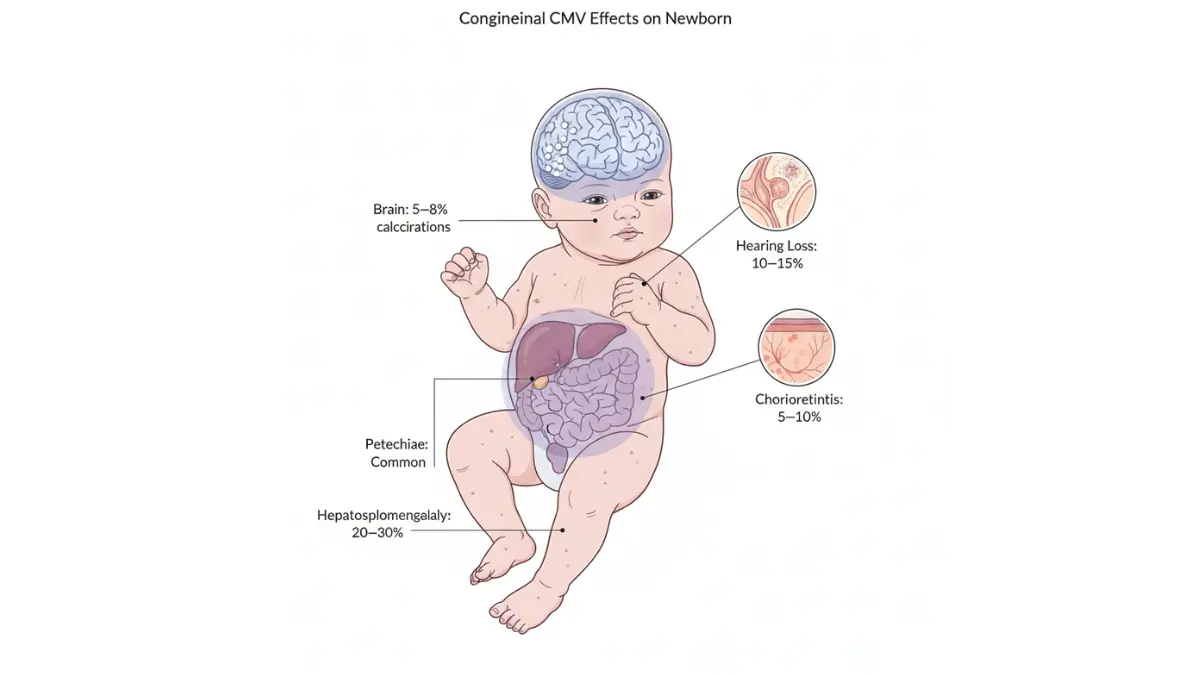
Congenital CMV Symptoms & Frequency
| Symptom | Percentage Affected | Severity | Long-term Impact |
|---|---|---|---|
| CMV hearing loss baby | 10-15% of all infected; 50% of symptomatic | Progressive in 50% of cases | Leading non-genetic cause; may worsen over childhood |
| Microcephaly (small head) | 5-8% | Severe | High developmental disability risk; correlates with intellectual impairment |
| Intrauterine growth restriction | 30-40% | Mild to severe | Monitor with Fetal Growth Percentile Calculator; may normalize postnatally |
| Petechiae (skin rash) | 60-80% at birth | Mild; resolves spontaneously | Cosmetic only; typically disappears within weeks |
| Hepatosplenomegaly (enlarged liver/spleen) | 40-60% | Moderate | Usually resolves; may indicate more severe systemic involvement |
| Jaundice | 40-60% | Mild to moderate | Typically resolves with phototherapy; rarely indicates liver damage |
| Intracranial calcifications | 15-20% | Severe marker | Strong predictor of neurodevelopmental impairment and seizures |
| Chorioretinitis (eye inflammation) | 10-15% | Moderate to severe | Vision impairment; may progress to blindness if untreated |
CMV Ultrasound Findings: What Doctors Look For
Serial ultrasound monitoring becomes essential when primary CMV infection pregnancy is confirmed. Maternal-fetal medicine specialists trained in high-resolution ultrasound protocols examine specific markers indicating fetal infection.
Key CMV ultrasound findings include:
- Intracranial calcifications: Bright spots in brain tissue, particularly around ventricles (periventricular distribution)
- Ventriculomegaly: Enlarged fluid-filled brain spaces suggesting developmental disruption
- Echogenic bowel: Abnormally bright intestinal appearance on ultrasound
- Fetal growth restriction: Serial measurements falling below 10th percentile tracked via Fetal Growth Percentile Calculator
- Hydrops fetalis: Severe fluid accumulation indicating advanced disease
- Hepatosplenomegaly: Enlarged fetal liver and spleen visible by second trimester
Absence of CMV ultrasound findings provides partial reassurance but doesn’t exclude infection—30-40% of infected fetuses show completely normal ultrasounds throughout pregnancy. This limitation explains why some specialists recommend amniocentesis after 21 weeks gestation to directly test amniotic fluid for viral DNA, providing definitive fetal infection diagnosis.
CMV Pregnancy Symptoms: Maternal Signs
Most pregnant women with CMV infection pregnancy risks remain completely asymptomatic—making screening and incidental detection crucial for diagnosis. When CMV pregnancy symptoms occur, they typically include:
- Mononucleosis-like illness: Prolonged fatigue lasting 2-4 weeks, often dismissed as normal pregnancy tiredness
- Low-grade fever: Temperature 99-101°F (37.2-38.3°C) without obvious cause
- Sore throat and swollen lymph nodes: Mimicking streptococcal pharyngitis or viral upper respiratory infections
- Muscle aches and malaise: Generalized body discomfort indistinguishable from pregnancy-related changes
- Rarely: Hepatitis with elevated liver enzymes or pneumonia in immunocompromised women
The 60-80% asymptomatic rate means most primary CMV infection pregnancy cases are detected only through routine serological screening or when ultrasound abnormalities prompt retroactive testing. This underscores the value of awareness among high-risk populations including daycare workers, teachers, and mothers of toddlers who should consider proactive CMV screening pregnancy protocols available through their Genetic Risk Assessment Tool evaluation.
CMV Pregnancy Treatment & Prevention Strategies
CMV Pregnancy Treatment Options & Evidence-Based Prevention (2025 Update)
Managing CMV positive pregnancy requires balancing limited treatment options with aggressive prevention strategies. While no cure exists for congenital CMV, emerging therapies show promise in reducing CMV transmission to baby severity and improving outcomes when maternal infection occurs.
Current CMV Test When Pregnant: Treatment Landscape
Maternal Antiviral Treatment: Valacyclovir (Valtrex) represents the most studied maternal therapy for primary CMV infection pregnancy. A 2024 multicenter randomized controlled trial published by researchers at major academic medical centers demonstrated that high-dose valacyclovir (8 grams daily) initiated before 20 weeks gestation reduced CMV transmission to baby rates from 40% to 27%—a significant 33% relative risk reduction. However, this therapy remains investigational, requiring comprehensive counseling through maternal-fetal medicine specialists familiar with current protocols detailed in CDC treatment guidelines.
Hyperimmune Globulin (CMV-IVIG): This concentrated antibody preparation showed initial promise but recent Phase III trials revealed no significant benefit in preventing congenital CMV when administered to mothers with confirmed primary CMV infection pregnancy. The American College of Obstetricians and Gynecologists now categorizes CMV-IVIG as experimental pending additional research, though some European protocols continue investigating modified dosing regimens.
Neonatal Treatment: Valganciclovir therapy initiated within the first month of life for symptomatic congenital CMV prevents progressive CMV hearing loss baby complications in 70-85% of treated infants according to long-term follow-up studies. Six-month treatment courses demonstrate superior outcomes compared to shorter protocols, making early diagnosis through newborn screening critically important.
2025 Research Updates: International expert panels from North America, Europe, and Asia convened through the International Congenital Cytomegalovirus Recommendations Group now recommend serial ultrasound monitoring every 2-4 weeks for confirmed maternal infections rather than immediate treatment initiation, allowing identification of the 60% of fetuses who never develop infection or remain asymptomatic.
How to Prevent CMV Pregnancy: Actionable Hygiene Strategies
Prevention remains the most effective intervention against CMV infection pregnancy risks. Rigorous hygiene protocols reduce transmission by up to 90% in high-risk populations including daycare workers and mothers with young children.
First Trimester CMV Prevention (Weeks 1-13):
- Hand hygiene: Wash hands with soap and water for 20+ seconds after every diaper change, nose wiping, or handling children’s toys
- Avoid saliva sharing: No sharing cups, utensils, or food with children under age 3 (peak viral shedding period)
- Kissing protocols: Kiss children on head/shoulder rather than lips to avoid saliva contact
- Environmental cleaning: Disinfect surfaces contacted by children’s saliva or urine (changing tables, toys, countertops) using EPA-registered disinfectants
- Pregnancy planning: Track conception timing with Ovulation Calculator to implement prevention strategies immediately upon attempting pregnancy

Second & Third Trimester Continued Vigilance:
Prevention remains equally important throughout pregnancy despite the CMV pregnancy first trimester carrying highest symptomatic congenital CMV risk. Viral shedding from young children peaks at ages 1-3 years, with 70% of daycare-attending toddlers actively shedding virus in saliva and urine for months to years after initial infection.
High-Risk Occupation Considerations:
Daycare workers and early childhood educators face 5-8% annual primary CMV infection pregnancy acquisition rates—10 times higher than the general pregnant population. These professionals should discuss CMV screening pregnancy protocols with employers and consider temporary reassignment during pregnancy if feasible. Teachers working with children under age 3 benefit from identical prevention strategies integrated into daily routines.
Sexual Transmission Prevention:
Though less common than child-to-mother transmission, sexual activity transmits cytomegalovirus pregnancy infections in 1-2% of cases when partners have discordant serostatus. Condom use throughout pregnancy reduces this risk, particularly when male partners work in high-exposure occupations or have recent mononucleosis-like illnesses.
Who Should Get CMV Screening Pregnancy?
Universal prenatal CMV screening pregnancy remains controversial. Current CDC recommendations do not mandate routine screening, but specific high-risk populations benefit from proactive CMV antibody test pregnancy protocols:
- Daycare workers and early childhood educators (5-8% annual infection risk)
- Mothers with children under age 6 in daycare settings (3-4% annual risk)
- Healthcare workers in pediatric or neonatal intensive care units
- Women with immunocompromising conditions (HIV, transplant recipients)
- Previous pregnancy loss or structural abnormalities on current pregnancy ultrasound
- Regional variations: Some European countries (Italy, Belgium) mandate first-trimester screening; implementation varies globally
Discuss individual risk assessment through comprehensive evaluation tools like the Genetic Risk Assessment Tool that factors occupational exposures, household composition, and pregnancy history into personalized screening recommendations.
Key Prevention Takeaway: Consistent hand hygiene after contact with young children’s bodily fluids prevents 84-90% of CMV transmission to baby cases—making simple behavioral changes your most powerful tool against congenital CMV.
Living With CMV Test Results – Your Action Plan
Your CMV Test Pregnancy Action Plan: Next Steps Based on Your Results
Receiving CMV test pregnancy results transforms abstract medical information into personal decisions requiring clear, actionable guidance. Your specific antibody combination determines monitoring intensity, specialist involvement, and prevention strategies for the remainder of your pregnancy.
If You Test CMV Negative During Pregnancy
A CMV negative pregnancy result means you’ve never been exposed to cytomegalovirus—approximately 40-60% of pregnant women in the United States fall into this category according to CDC surveillance data. Your action plan focuses on aggressive prevention:
- Implement strict hand hygiene protocols after contact with young children’s saliva, urine, or nasal secretions—washing for 20+ seconds with soap eliminates 84-90% transmission risk
- Avoid sharing food, drinks, or utensils with children under age 6, particularly those attending daycare
- Consider repeat testing if high-risk exposure occurs (new daycare enrollment, mononucleosis-like illness in household members)
- Monitor symptoms through tools like the Symptom Checker if unexplained fever or prolonged fatigue develops
- Discuss screening intervals with your provider—some recommend second-trimester repeat testing for daycare workers
Your susceptibility requires vigilance, but consistent prevention strategies provide excellent protection against primary CMV infection pregnancy acquisition throughout gestation.
If You Test CMV Positive (Past Infection)
CMV IgG positive pregnancy with negative IgM indicates immunity from pre-conception infection—the most reassuring scenario affecting 50-70% of women depending on geographic region and socioeconomic factors. Your dramatically reduced 1-3% reactivation risk requires minimal modifications:
- Continue routine prenatal care without additional CMV-specific monitoring beyond standard anatomy ultrasound at 20 weeks
- Track normal pregnancy milestones using your Pregnancy Due Date Calculator and standard growth assessments
- No special precautions needed regarding childcare, work exposure, or daily activities
- Reassure yourself that established immunity protects your baby throughout pregnancy
- Inform pediatrician at delivery for appropriate newborn evaluation protocols
Women with pre-existing immunity can confidently focus on comprehensive prenatal wellness explored through Health Tips resources rather than CMV-specific interventions.
If You Have Primary CMV Infection in Pregnancy
Confirmed or suspected primary CMV infection pregnancy demands immediate specialized care coordination. Your high-risk status (30-40% CMV transmission to baby probability) requires comprehensive monitoring:
Immediate Actions (Within 48-72 Hours):
- Maternal-fetal medicine referral for subspecialty consultation and counseling
- Baseline detailed ultrasound examining brain structures, growth parameters, and organ development
- Avidity testing confirmation if not already performed to verify infection timing
Ongoing Management:
- Serial ultrasounds every 2-4 weeks monitoring for CMV ultrasound findings including intracranial calcifications, ventriculomegaly, and growth restriction
- Amniocentesis discussion after 21 weeks gestation to determine fetal infection status definitively
- Valacyclovir therapy consideration if infection confirmed before 20 weeks—discuss risks/benefits with maternal-fetal medicine team familiar with latest protocols
- Coordinate pediatric infectious disease consultation for delivery planning and immediate neonatal testing
Emotional Support Resources:
Primary infection diagnosis creates profound anxiety. Connect with National CMV Foundation support groups, seek counseling through your healthcare system, and remember that 60% of exposed fetuses never develop infection and 85-90% of infected babies appear healthy at birth.
Global Expert Perspectives on CMV Management
Dr. Suresh Boppana (University of Alabama): “Early identification through targeted CMV screening pregnancy protocols, combined with rigorous prevention education, represents our best strategy until effective vaccines become available. Women should understand that negative results require continued vigilance while positive immunity provides reassurance.”
Professor Yves Ville (Paris Necker Hospital, France): “European experience with universal first-trimester screening demonstrates feasibility, though optimal implementation requires comprehensive counseling infrastructure to manage the psychological impact of positive results and prevent unnecessary anxiety.”
Dr. Rangasami Ramalingam (AIIMS New Delhi, India): “In resource-limited settings, targeted screening of high-risk populations—daycare workers, mothers with multiple young children—maximizes cost-effectiveness while addressing populations with 5-10 times baseline risk of primary CMV infection pregnancy acquisition.”
Your CMV test results don’t define your pregnancy outcome—they guide personalized care strategies. Whether you’re maintaining prevention as a CMV negative pregnancy, reassured by pre-existing immunity in CMV positive pregnancy scenarios, or navigating specialized monitoring for primary infection, remember that comprehensive prenatal care, expert guidance, and informed decision-making give you and your baby the best possible outcomes. Early detection through CMV antibody test pregnancy screening, combined with evidence-based management, transforms uncertainty into actionable plans that protect maternal and fetal health throughout your pregnancy journey.
11 Frequently Asked Questions About CMV Test Pregnancy
1. What does a positive CMV test mean during pregnancy?
A CMV positive pregnancy result indicates antibodies are present, meaning you’ve been exposed to cytomegalovirus either before or during pregnancy. If only IgG is positive, you have past immunity with 1-3% transmission risk. If both IgG and IgM are positive, avidity testing determines whether infection is recent (high-risk) or old (low-risk).
2. Should I get tested for CMV during pregnancy?
CMV screening pregnancy isn’t universally recommended but is beneficial if you work in daycare, have young children at home, or have unexplained pregnancy complications. High-risk women (daycare workers, teachers of young children) should discuss testing with their provider around 8-12 weeks gestation.
3. Can CMV cause miscarriage?
Primary CMV infection pregnancy rarely causes miscarriage directly but increases risk of intrauterine growth restriction and fetal complications. Most CMV-related pregnancy losses occur in severe symptomatic cases with hydrops fetalis or multiple organ involvement detected on ultrasound.
4. What’s the difference between CMV IgG and IgM?
CMV IgG positive pregnancy indicates past infection and immunity lasting lifelong. CMV IgM positive pregnancy suggests recent infection but has a 90% false-positive rate, requiring avidity testing for accurate interpretation.
5. How accurate is the CMV avidity test?
The CMV avidity test demonstrates 95-100% accuracy for ruling out recent infection when high avidity (>60%) is detected in the first trimester. Low avidity (<40%) confirms infection within the past 3-4 months with high reliability.
6. Can I prevent CMV if I’m pregnant and work in daycare?
Yes—rigorous hand hygiene after every diaper change, avoiding saliva sharing (no kissing on lips, sharing utensils), and environmental disinfection reduce CMV transmission by 84-90%. These strategies are highly effective even in high-exposure settings.
7. What are the chances my baby will be affected?
Primary CMV infection pregnancy transmits to 30-40% of babies, but only 10-15% of infected newborns show symptoms at birth. Pre-existing immunity (past infection) reduces transmission risk to just 1-3%.
8. When is CMV most dangerous during pregnancy?
CMV pregnancy first trimester infections carry highest risk for severe congenital CMV symptoms including microcephaly and brain calcifications. However, third-trimester infections transmit more frequently but typically cause milder or asymptomatic disease.
9. Is there treatment for CMV in pregnancy?
Valacyclovir (Valtrex) is investigational for CMV pregnancy treatment, reducing transmission by 33% when started before 20 weeks. Hyperimmune globulin remains experimental with limited proven benefit in recent trials.
10. Will my baby need testing if I had CMV?
If you have CMV IgG positive pregnancy only (past immunity), standard newborn care suffices. If primary CMV infection pregnancy occurred or fetus showed CMV ultrasound findings, your baby needs immediate saliva/urine testing within 21 days of birth plus auditory screening.
11. Can I breastfeed with CMV?
Women with CMV positive pregnancy (past immunity) can safely breastfeed full-term healthy infants—transmitted virus through breast milk rarely causes disease in term babies. Premature infants (<32 weeks) may need counseling about freezing/pasteurizing breast milk to reduce reactivated virus transmission.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.