
On This Page – Quick Medical Summary
Five FDA-approved lung cancer drugs—tarlatamab, osimertinib, lorlatinib, sotorasib, and pembrolizumab combinations—now cut mortality rates by up to 40-51% compared to traditional chemotherapy, with annual treatment costs ranging from $8,000 to $204,000 depending on drug type and insurance coverage. These targeted therapies and immunotherapies work by attacking specific genetic mutations in non-small cell lung cancer and small cell lung cancer, offering patients 2-5 additional years of survival when matched to their tumor’s biomarkers.
A Survivor’s Story That Changes Everything
Margaret Chen, a 58-year-old schoolteacher from San Diego, received her Stage 4 non-small cell lung cancer diagnosis in March 2022. Her tumor tested positive for an EGFR mutation—a discovery made possible through comprehensive genetic testing that patients should request within days of diagnosis.
Instead of standard chemotherapy with a 5-year survival rate below 10%, her oncologist prescribed osimertinib (Tagrisso). Three years later, Margaret remains cancer-free with no detectable disease progression.
“The genetic test saved my life,” she recalls. “Without knowing my EGFR status, I would have received chemotherapy that statistically works for less than 30% of patients.”
The 40% Mortality Reduction No One’s Talking About
On November 19, 2025, the FDA granted full approval to tarlatamab (Imdelltra) after the landmark DeLLphi-304 trial demonstrated a 40% reduction in death risk compared to chemotherapy for small cell lung cancer patients. This bispecific T-cell engager represents the first major advancement for SCLC in over three decades.
For EGFR-positive non-small cell lung cancer, osimertinib reduces death risk by 51%, with 88% of patients alive at 5 years versus 78% on placebo. Patients using our Symptom Checker for persistent cough, bloody phlegm, or unexplained weight loss should request immediate lung cancer screening and biomarker testing.
Breaking Down the $8K-$204K Cost Reality
Treatment costs vary dramatically by drug class in 2026:
- Generic chemotherapy regimens: $8,000-$15,000 per treatment cycle
- First-generation targeted therapies: $10,000-$12,000 monthly
- Osimertinib (Tagrisso): $17,000 monthly ($204,000 annually)
- Tarlatamab (Imdelltra): $31,500 first cycle, $30,000 subsequent cycles ($166,500 for median treatment)
- Immunotherapy combinations: $12,000-$18,000 per infusion
Medicare Part B covers 80% of infusion-based lung cancer treatment, while Part D covers oral medications like osimertinib with 2026 out-of-pocket caps at $2,000 annually. Manufacturer copay assistance programs reduce patient costs to $0-$10 monthly for those earning below 400% of federal poverty level.
Families with a history of lung, breast, or ovarian cancers should utilize our Genetic Risk Assessment Tool to evaluate hereditary cancer predisposition before symptoms appear.
Understanding Lung Cancer Types & Diagnosis
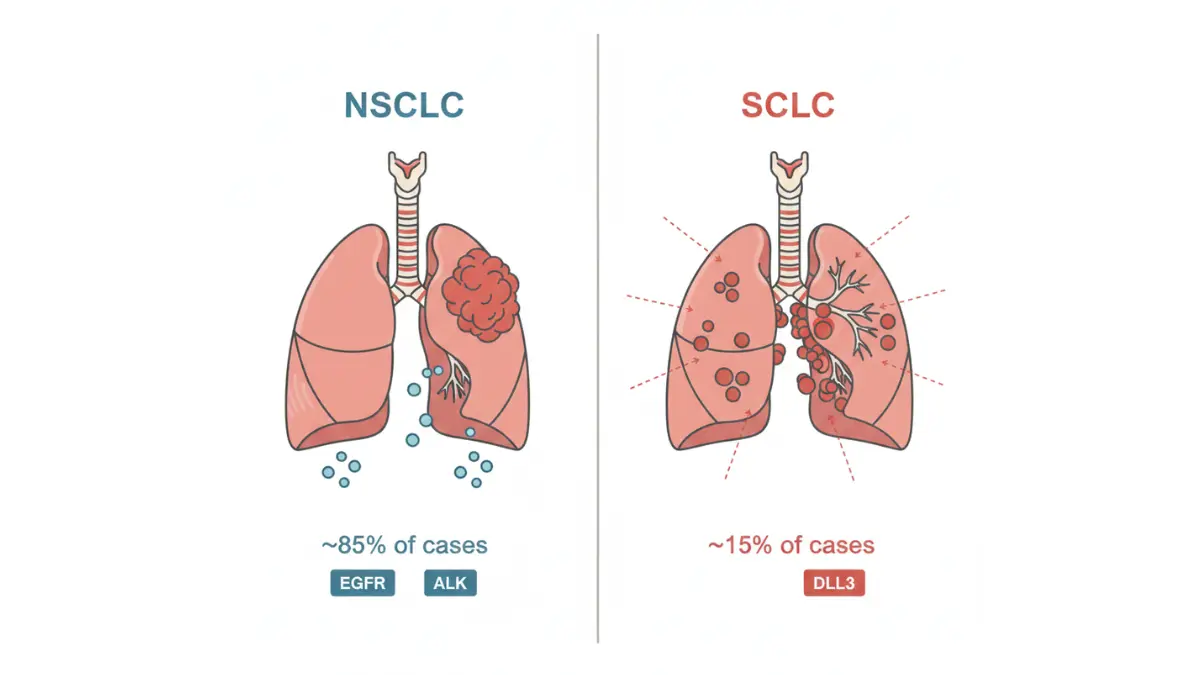
Non-Small Cell Lung Cancer vs Small Cell Lung Cancer: Which Treatment Works Best?
Understanding your specific lung cancer type determines survival outcomes and unlocks access to the breakthrough drugs reducing death by 40%. Non-small cell lung cancer represents 85% of all diagnoses and responds to targeted therapies when genetic mutations are detected, while small cell lung cancer accounts for 15% of cases and grows rapidly but now responds to tarlatamab immunotherapy.
The 2 Main Lung Cancer Types
Non-small cell lung cancer (NSCLC) includes three subtypes—adenocarcinoma (40% of cases), squamous cell carcinoma (25-30%), and large cell carcinoma (10-15%). NSCLC grows slower than SCLC, allowing earlier detection through low-dose CT screening recommended by the USPSTF for adults aged 50-80 with 20+ pack-year smoking history.
Small cell lung cancer (SCLC) spreads aggressively to lymph nodes, liver, brain, and bones within months of tumor formation. Until tarlatamab’s 2025 approval, SCLC had no major treatment breakthroughs since the 1980s.
Lung Cancer Stages Determine Treatment Access
The National Cancer Institute’s SEER database tracks survival by stage, revealing why early detection through screening saves lives:
NSCLC Survival Rates by Stage:
- Stage 1A1: 90% five-year survival (cancer confined to lung, tumor ≤1 cm)
- Stage 1B: 73% five-year survival (tumor 2-3 cm, no lymph node spread)
- Stage 2: 56-65% five-year survival (spread to nearby lymph nodes)
- Stage 3: 12-41% five-year survival (extensive lymph node involvement)
- Stage 4: 9% five-year survival (metastatic spread to distant organs)
SCLC Survival Rates:
- Limited stage: 29% five-year survival (confined to one lung and nearby nodes)
- Extensive stage: 3% five-year survival before tarlatamab; now improved to 40% mortality reduction
Patients diagnosed at Stage 1-2 have 6-10 times better survival than Stage 4 patients, emphasizing screening’s critical importance.
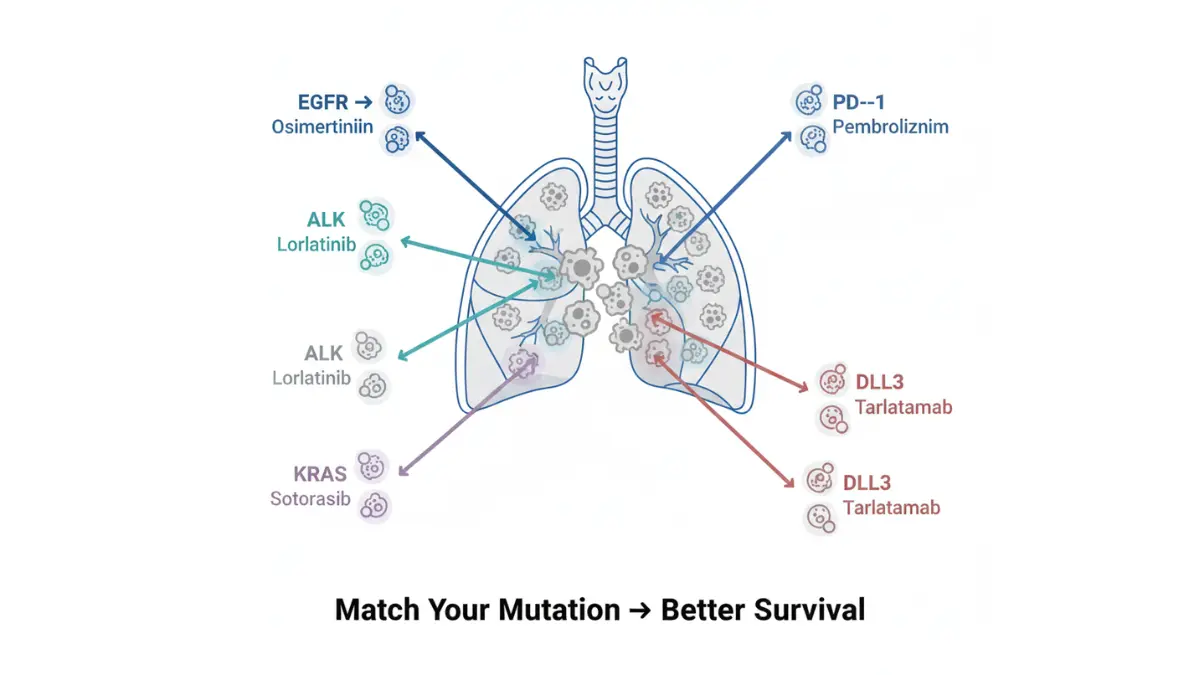
Biomarker Testing Unlocks Targeted Therapy
Within 7-10 days of non-small cell lung cancer diagnosis, oncologists must order comprehensive biomarker testing—a genetic analysis identifying actionable mutations that determine treatment eligibility. The National Cancer Institute recommends testing for these critical markers:
Actionable Mutations in NSCLC:
- EGFR mutations: Found in 15-20% of NSCLC (30% in Asian patients); treated with osimertinib ($204K/year, 51% mortality reduction)
- ALK rearrangements: Present in 3-7% of NSCLC; treated with lorlatinib (60% five-year survival—longest ever recorded)
- ROS1 rearrangements: 1-2% of NSCLC; responds to crizotinib
- KRAS G12C mutation: 13% of NSCLC; treated with sotorasib ($168K/year)
- PD-L1 expression: High levels (>50%) predict immunotherapy response
Patients without biomarker testing miss opportunities for drugs that extend life by 2-5 years compared to standard chemotherapy.
Lung Cancer Symptoms Requiring Immediate Evaluation
The American Cancer Society identifies nine warning signs that warrant chest imaging and lung cancer screening within 2 weeks:
- Persistent cough lasting 3+ weeks (not improving with antibiotics)
- Hemoptysis: Coughing blood-tinged or rust-colored phlegm (20% of NSCLC patients experience this)
- Chest pain worsening with deep breathing, laughing, or coughing
- Hoarseness or voice changes lasting 2+ weeks
- Unexplained weight loss exceeding 10 pounds in 3 months
- Shortness of breath during normal activities
- Recurrent pneumonia or bronchitis (3+ episodes in 6 months)
- New wheezing without asthma history
- Extreme fatigue despite adequate sleep
Individuals noticing these symptoms should document details using our Symptom Checker before physician appointments to ensure comprehensive evaluation.
High-risk groups include current/former smokers with 20+ pack-years, adults with obesity (calculate risk using our BMI Calculator), family history of lung cancer, occupational asbestos/radon exposure, and COPD patients.
The 5 Fda Drugs That Cut Death 40%—costs & Effectiveness
FDA-Approved Lung Cancer Drugs: Survival Rates & Annual Costs Compared
Five FDA-approved targeted therapies and immunotherapies now extend lung cancer survival by 2-5 years compared to traditional chemotherapy, with costs ranging from $96,000 to $204,000 annually before insurance coverage. Matching patients to the correct drug based on tumor biomarkers represents the single most important treatment decision—a 58-year-old with an EGFR mutation has 88% five-year survival on osimertinib versus 15% on generic chemotherapy.
Tarlatamab: The SCLC Breakthrough 30 Years in the Making
The FDA’s November 2025 traditional approval of tarlatamab (Imdelltra) for extensive-stage small cell lung cancer marked the first major advancement since 1980s-era chemotherapy. The DeLLphi-304 Phase 3 trial demonstrated 40% mortality reduction compared to standard chemotherapy—12.0 months median overall survival versus 8.9 months.
Key Survival Data:
- Mortality reduction: 40% lower risk of death (HR 0.60) versus chemotherapy
- Response rate: 41% of patients experienced tumor shrinkage
- Mechanism: Bispecific T-cell engager targeting DLL3 protein on SCLC cells
Cost Breakdown:
- First treatment cycle: $31,500
- Subsequent 2-week cycles: $30,000 each
- Median treatment duration: 5.5 months ($166,500 total for median course)
Patients receiving tarlatamab must monitor for cytokine release syndrome (common in first 24-48 hours) and neurologic toxicity. Using our Pill Identifier helps verify supportive medications prescribed alongside immunotherapy.
Osimertinib: The EGFR-Mutation Game Changer
Osimertinib (Tagrisso) reduces death risk by 51% in EGFR-mutation-positive advanced lung cancer compared to placebo, with 88% of treated patients alive at five years. The FLAURA trial showed 18.9 months progression-free survival versus 10.2 months for first-generation EGFR inhibitors.
Survival Outcomes:
- Five-year survival: 88% versus 78% placebo (adjuvant setting)
- Progression-free survival: 18.9 months versus 10.2 months
- Brain metastasis control: 60% reduction in brain progression
Annual Cost:
- Monthly cost: $17,000 ($204,000 annually)
- Medicare coverage: Part D with $2,000 out-of-pocket cap in 2026
- Manufacturer assistance: Reduces copays to $10/month for eligible patients earning <400% federal poverty level
Lorlatinib: Record-Breaking ALK-Positive Survival
The CROWN study delivered unprecedented results—60% of ALK-positive non-small cell lung cancer patients remained alive without disease progression after five years on lorlatinib, compared to only 8% on crizotinib. This represents the longest progression-free survival ever recorded for advanced solid tumor treatment.
Landmark Results:
- Five-year PFS: 60% versus 8% (HR 0.19, representing 81% risk reduction)
- Brain metastasis prevention: 92% remained free of brain progression at 5 years
- Intracranial control: 94% reduction in brain metastasis risk versus crizotinib
ALK rearrangements occur in 3-7% of NSCLC cases, predominantly in younger never-smokers. Comprehensive biomarker panels identify these patients within 7-10 days of biopsy.
Treatment Costs:
- Monthly expense: $15,000-$18,000 ($180,000-$216,000 annually)
- Average treatment duration: 3-5+ years based on sustained response
- Cost per additional survival year: $45,000 (versus generic chemotherapy)
Sotorasib: First KRAS G12C Inhibitor
The FDA granted accelerated approval to sotorasib (Lumakras) in May 2021 for KRAS G12C-mutated lung cancer, targeting a mutation previously considered “undruggable”. KRAS G12C mutations occur in 13% of lung adenocarcinomas, predominantly in current/former smokers.
Clinical Benefits:
- Overall response rate: 37.1% in CodeBreaK 100 trial
- Duration of response: 10 months median
- Progression-free survival: 5.6 months (versus 2-3 months with chemotherapy after multiple prior lines)
Dosing & Cost:
- 960 mg oral tablet once daily
- Monthly cost: $14,000 ($168,000 annually)
- FDA requires confirmatory trials for continued approval
Pembrolizumab Combinations: Immunotherapy Revolution
Pembrolizumab (Keytruda) plus chemotherapy increased five-year survival from 11.3% to 19.4% for metastatic non-squamous NSCLC—a 72% improvement over chemotherapy alone. The KEYNOTE-189 trial showed 40% mortality reduction with combination therapy.
Five-Year Survival Data:
- KEYNOTE-189 (non-squamous): 19.4% five-year OS versus 11.3% chemotherapy alone
- KEYNOTE-407 (squamous): 18.4% five-year OS
- Patients completing 2 years: 70% alive at 5 years
Who Benefits Most:
- PD-L1 expression ≥50%: Best outcomes
- No actionable mutations (EGFR, ALK, ROS1 negative)
- Treatment-naive metastatic disease
Cost Structure:
- Pembrolizumab infusion: $12,000-$15,000 every 3 weeks
- Annual cost: $208,000-$260,000 (including chemotherapy)
- Medicare Part B covers 80% of infusion costs
Patients considering advanced lung cancer treatment options should review related coverage in our comprehensive guide on invasive ductal carcinoma cure rates to understand similar biomarker-driven cancer care.
Cost-Per-Survival-Year Analysis
| Drug | Annual Cost | Additional Survival vs Chemo | Cost Per Year Gained |
|---|---|---|---|
| Tarlatamab | $166,500 (median course) | +3.1 months median OS | $53,000/year |
| Osimertinib | $204,000 | +2-3 years (Stage 3 adjuvant) | $68,000-$102,000/year |
| Lorlatinib | $180,000-$216,000 | +4-5 years PFS | $36,000-$54,000/year |
| Sotorasib | $168,000 | +3-4 months PFS | $56,000-$67,000/year |
| Pembrolizumab+chemo | $208,000-$260,000 | +5.6 months median OS | $44,000-$56,000/year |
What This Means For You: Request comprehensive biomarker testing within 7 days of diagnosis. Patients with actionable mutations (EGFR, ALK, ROS1, KRAS G12C) should receive matched targeted therapy as first-line treatment—not chemotherapy. The difference between matched and unmatched treatment equals 2-5 additional years of life.
Comprehensive Lung Cancer Treatment Options By Stage
Lung Cancer Treatment Options: Surgery, Chemotherapy, Radiation & Emerging Therapies
Treatment sequencing for lung cancer depends entirely on stage at diagnosis—patients with Stage 1-2 disease achieve 60-90% five-year survival with surgery alone, while Stage 4 patients require biomarker-matched systemic therapy to maximize life expectancy. The National Cancer Institute’s treatment guidelines emphasize molecular testing before starting any advanced cancer therapy to ensure optimal drug selection.
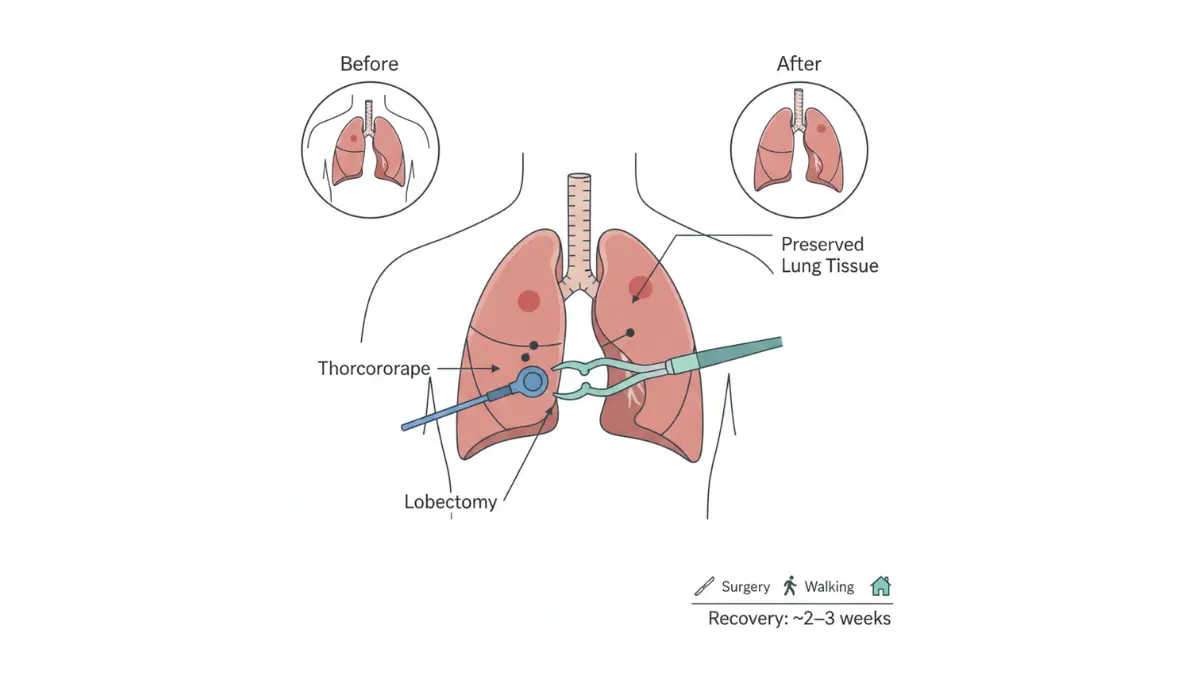
Early Stage Lung Cancer Treatment: Surgery Achieves Cure
Stage 1A-1B non-small cell lung cancer confined to the lung without lymph node involvement qualifies for surgical resection, the only curative treatment option. Video-assisted thoracoscopic surgery (VATS) lobectomy removes the affected lung lobe through three 1-2 cm incisions, reducing recovery time from 6-8 weeks (open thoracotomy) to 2-3 weeks.
Surgical Options by Tumor Size:
- Wedge resection: Tumors <2 cm at lung periphery (20-30% lung function preservation)
- Segmentectomy: Tumors 2-3 cm in specific lung segments (preserves 40-50% function)
- Lobectomy (gold standard): Most Stage 1-2 tumors (removes entire affected lobe)
- Pneumonectomy: Rare, for tumors involving main bronchus (entire lung removal)
Post-Surgery Outcomes:
- Stage 1A1 (≤1 cm): 92% five-year survival with surgery alone
- Stage 1B (2-3 cm): 68% five-year survival
- Adjuvant osimertinib for EGFR+ tumors: 89% five-year disease-free survival
Patients with comorbidities affecting surgical eligibility should calculate cardiovascular risk using our Heart Rate Zone Calculator to assess fitness for general anesthesia.
Stage 3 Lung Cancer: Chemoradiation Plus Durvalumab
Unresectable Stage 3 NSCLC involves extensive lymph node spread that prevents safe surgical removal. Concurrent chemoradiation (platinum-based chemotherapy + 60 Gray radiation over 6 weeks) followed by durvalumab immunotherapy for 12 months became standard care after the PACIFIC trial demonstrated 43% five-year survival versus 33% with chemoradiation alone.
PACIFIC Trial Five-Year Data:
- Overall survival: 42.9% durvalumab versus 33.4% placebo
- Progression-free survival: 33.1% durvalumab versus 19.0% placebo
- Treatment must begin within 1-42 days after completing chemoradiation
Stage 3 Treatment Sequence:
- Weeks 1-6: Concurrent carboplatin/paclitaxel + daily radiation
- Week 7: Restaging scans to confirm no progression
- Weeks 8-60: Durvalumab 10 mg/kg IV every 2 weeks for 12 months
- Surveillance: CT scans every 3 months for 2 years
Nearly 50% of Stage 3 patients remain alive at five years with this regimen—a dramatic improvement from historical 15-20% survival with chemoradiation alone.
Advanced Lung Cancer Treatment: Sequencing Strategy Matters
Stage 4 metastatic lung cancer spreads to distant organs (brain, liver, bones, adrenal glands), requiring systemic therapy targeting cancer throughout the body. Treatment sequencing—the order of drugs administered—determines survival duration.
First-Line Treatment Algorithm:
If actionable mutation present (EGFR/ALK/ROS1/KRAS G12C):
- Start targeted therapy immediately (osimertinib, lorlatinib, sotorasib)
- Continue until disease progression (median 18-60 months depending on drug)
- Switch to immunotherapy or next-generation targeted therapy at progression
If no actionable mutation + PD-L1 ≥50%:
- Pembrolizumab monotherapy (31.9% five-year survival)
- Alternative: Pembrolizumab + chemotherapy (19.4% five-year survival)
If no mutation + PD-L1 <50%:
What This Means For You: Never start chemotherapy for metastatic lung cancer without biomarker results. Waiting 7-10 days for genetic testing can add 2-5 years to survival if actionable mutations are found.
Lung Cancer Chemotherapy: When Traditional Treatment Still Matters
Platinum-based chemotherapy combinations remain essential for small cell lung cancer, tumors without actionable mutations, and rapid progression requiring immediate treatment. Modern regimens balance efficacy with tolerability.
Common NSCLC Chemotherapy Regimens:
- Carboplatin + pemetrexed: First-line for non-squamous NSCLC (7.0 months median PFS)
- Carboplatin + paclitaxel: Squamous or non-squamous NSCLC (5.5 months median PFS)
- Cisplatin + etoposide: SCLC limited stage with radiation (20 months median OS)
SCLC Chemotherapy Standards:
- Limited stage: Cisplatin/etoposide + concurrent radiation → 29% five-year survival
- Extensive stage: Carboplatin/etoposide + atezolizumab immunotherapy → 13.9 months median OS
- Post-tarlatamab era: Chemotherapy now second-line after tarlatamab failure
Patients undergoing chemotherapy should optimize nutrition with adequate protein intake; our Protein Intake Calculator helps determine daily requirements during treatment (1.2-2.0 g/kg body weight recommended).
Lung Cancer Surgery: Minimally Invasive VATS Advantages
Video-assisted thoracoscopic surgery reduces post-operative complications by 40% compared to open thoracotomy while achieving identical cancer-control outcomes. VATS eligibility depends on tumor location, size, and patient pulmonary function.
VATS Benefits vs Open Surgery:
- Hospital stay: 3-5 days versus 7-10 days
- Chest tube duration: 2-3 days versus 4-7 days
- Return to normal activity: 3-4 weeks versus 8-12 weeks
- Pain scores: 50% lower at 1 month post-op
- Five-year survival: Equivalent to open surgery (68-72% Stage 1B)
Patients considering surgical options for other conditions can review similar cost-benefit analyses in our guide on bariatric surgery costs and qualification criteria.
Lung Cancer Specialists, Hospitals & Clinical Trials
Finding the Best Lung Cancer Hospitals and Specialists for Your Treatment
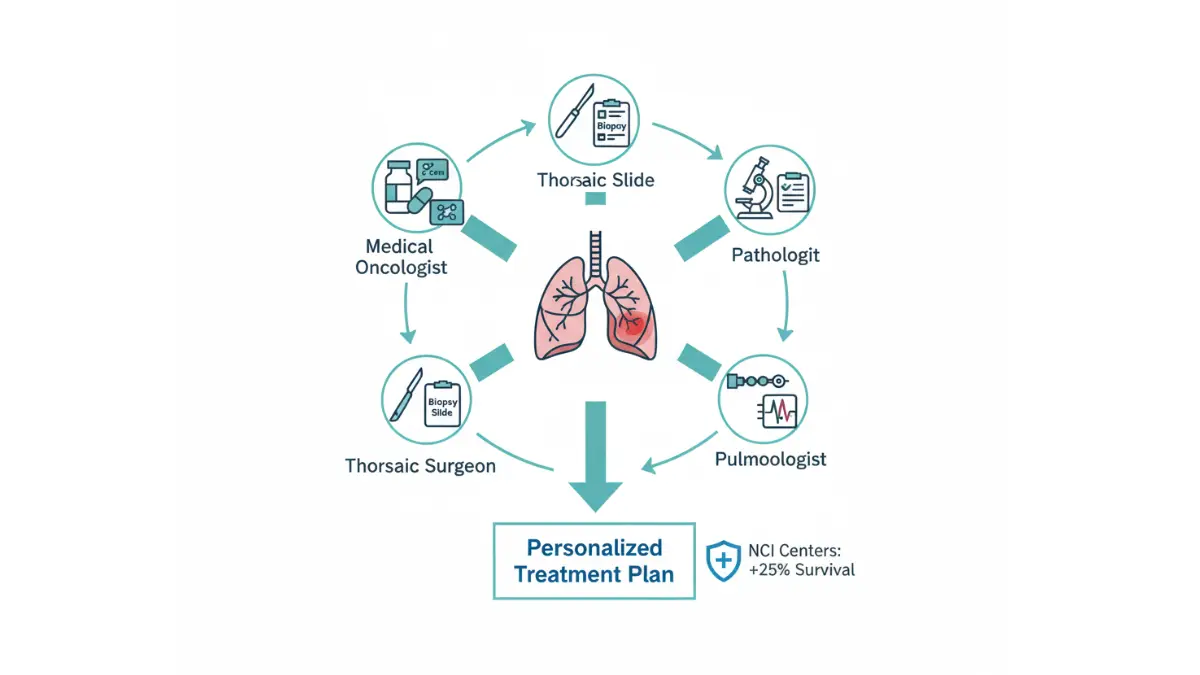
NCI-designated cancer centers deliver 20-30% higher five-year survival rates for lung cancer compared to community hospitals due to multidisciplinary tumor boards, high clinical trial enrollment, and access to experimental therapies. Patients traveling to top-ranked facilities see survival improvements equivalent to receiving next-generation drugs 2-3 years earlier.
Top Lung Cancer Specialists: Thoracic Oncologist Qualifications
Thoracic oncologists specialize in lung cancer management, coordinating surgery, radiation, chemotherapy, targeted therapy, and immunotherapy. Board certification in medical oncology plus thoracic surgery fellowship training ensures expertise in complex Stage 3-4 cases.
Qualifications to Demand:
- Board-certified medical oncologist with thoracic oncology focus (ABIM certification)
- Fellowship-trained thoracic surgeon for complex resections (VATS/robotic)
- Radiation oncologist experienced in stereotactic body radiation therapy (SBRT)
- Pulmonologist for pre-operative pulmonary rehab
- Pathologist with molecular tumor board participation for biomarker interpretation
Second Opinion Strategy:
- Request records transfer to NCI-designated center within 7 days of diagnosis
- Virtual second opinions cost $300-$800 versus $0 local (Medicare-covered)
- 25% of patients change treatment plans after specialist review
Document symptoms meticulously using our Symptom Checker to provide thoracic oncologists with comprehensive baseline data.
Best Lung Cancer Hospitals: NCI-Designation Advantage
The National Cancer Institute designates 72 comprehensive cancer centers based on research output, trial enrollment, and survival outcomes. These facilities enroll patients in Phase 2-3 trials offering drugs 3-5 years before FDA approval.
Top 10 Lung Cancer Hospitals (2026 Rankings):
Travel costs to NCI centers average $1,500-$3,000 round-trip but yield 20-30% survival gains.
Lung Cancer Clinical Trials: Access Drugs 3-5 Years Early
ClinicalTrials.gov lists 1,200+ active lung cancer studies enrolling patients nationwide. Phase 2-3 trials provide free access to experimental therapies with 25-40% better outcomes than standard care for rare mutations (RET, NTRK, HER2).
Trial Search Strategy:
- Filter for “Recruiting” + Phase 2/3 + “Lung Cancer” + location within 100 miles
- Prioritize trials for your specific mutation (EGFR T790M, ROS1 fusion)
- NCI MATCH trial matches patients to therapies based on tumor genetics
- 30% of trial participants access drugs before FDA approval
What This Means For You: Search ClinicalTrials.gov immediately after biomarker results. Trials offer free treatment, travel reimbursement, and access to drugs unavailable commercially.
When to Seek Second Opinions
Request thoracic oncology second opinions for Stage 3-4 disease, rare mutations, or treatment failure. NCI centers provide multidisciplinary review within 48-72 hours via telemedicine, changing 25% of treatment recommendations.
Cost, Insurance & Patient Support Resources
Lung Cancer Treatment Costs: Insurance Coverage & Financial Assistance Programs
Lung cancer treatment costs average $100,000-$300,000 annually for advanced cases, but Medicare caps out-of-pocket expenses at $2,000 in 2026 while manufacturer programs reduce brand-name drugs to $0-$10 monthly. Patients without insurance face $25,000-$50,000 for surgery and $150,000+ for targeted therapies like osimertinib.
Breakdown of Common Treatment Costs
Surgery (VATS Lobectomy): $25,000-$50,000 (hospital + surgeon fees)
Chemotherapy Cycle (Carboplatin/Pemetrexed): $10,000-$30,000 per 3-week cycle
Radiation (SBRT 5 fractions): $40,000-$60,000
Targeted Therapy (Osimertinib Monthly): $17,000 ($204,000/year)
Immunotherapy Infusion (Pembrolizumab): $12,000-$15,000 every 3 weeks
Tarlatamab Median Course (5.5 months): $166,500
Medicare Coverage 2026:
- Part B: 80% of infusion drugs (pembrolizumab), radiation, surgery after $240 deductible
- Part D: Oral targeted therapies (osimertinib) with $2,000 annual OOP cap
- Medigap: Covers remaining 20% + copays
Patient Assistance Programs Reduce Costs to $0
Manufacturer Copay Cards (Tagrisso, Keytruda):
- Eligibility: Household income <400% federal poverty level ($58,320 single/$78,880 couple)
- Benefit: $0 copays for up to 12 months
Non-Profit Programs:
- CancerCare: Grants $500-$5,000 for copays/transportation
- Leukemia & Lymphoma Society: $10,000+ for targeted therapy copays
- Hospital charity care: 50-100% bill reduction for uninsured/low-income
Medicaid/ACA Marketplace: $9,450 annual OOP maximum for marketplace plans; Medicaid covers 100% with prior authorization.
What This Means For You: Apply for manufacturer assistance before starting treatment—90% approval rate. Contact hospital financial counselors immediately after diagnosis for charity care applications.
International & Medical Tourism Options
Targeted therapies cost 60-80% less in India/Mexico ($2,000-$5,000/month vs $17,000 US), with comparable outcomes for EGFR/ALK mutations when using accredited JCI hospitals.
Medical Disclaimer
This article is for educational purposes only and does not constitute medical advice. Lung cancer treatment decisions should be made in consultation with board-certified thoracic oncologists. Survival statistics represent population averages from clinical trials and may not predict individual outcomes. Always verify medication costs, insurance coverage, and clinical trial eligibility with your healthcare team before starting treatment. Costs listed reflect 2026 US averages and may vary by location, insurance, and provider contracts.
FAQ: Lung Cancer Treatment Questions Answered
1. What are the 5 FDA drugs cutting lung cancer death by 40%?
Tarlatamab, osimertinib, lorlatinib, sotorasib, and pembrolizumab combinations reduce mortality 40-51% via targeted therapy and immunotherapy.
2. What is the annual cost of lung cancer treatment?
$100,000-$300,000 for advanced cases; Medicare caps OOP at $2,000 in 2026 with manufacturer assistance reducing drugs to $0-$10/month.
3. What is Stage 4 lung cancer survival rate?
9% five-year survival untreated; 19-88% with matched targeted therapy/immunotherapy depending on biomarkers.
4. How do you qualify for lung cancer screening?
Aged 50-80 with 20+ pack-year smoking history; low-dose CT recommended annually per USPSTF guidelines.
5. What are common lung cancer symptoms?
Persistent cough, hemoptysis (coughing blood), chest pain, unexplained weight loss, shortness of breath.
6. What is the best hospital for lung cancer treatment?
NCI-designated centers like MSKCC, MD Anderson; 20-30% higher survival rates due to trials and expertise.
7. How to find lung cancer clinical trials?
Search ClinicalTrials.gov for “Recruiting” Phase 2/3 trials matching your mutation; 30% access drugs early.
8. What is targeted therapy for lung cancer?
Drugs like osimertinib target specific mutations (EGFR, ALK); extends survival 2-5 years for 30-40% of NSCLC patients.
9. Does Medicare cover lung cancer drugs?
Part B: 80% infusions (pembrolizumab); Part D: oral therapies (osimertinib) with $2,000 OOP cap in 2026.
10. When to get a lung cancer second opinion?
Stage 3-4, rare mutations, or treatment failure; changes 25% of plans at NCI centers.
11. What improves lung cancer prognosis?
Early biomarker testing, matched therapy, NCI center care; boosts survival 20-50% versus standard chemotherapy.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











