On This Page – Quick Medical Summary
SCLC 2026: FDA Approves First Therapy Cutting Death Risk by 40% – But Treatment Costs $31,000 Monthly
Linda Martinez, a 58-year-old Texas teacher, was given six months to live after her extensive stage SCLC stopped responding to chemotherapy in January 2025. Today, she’s celebrating her daughter’s wedding—alive 14 months later thanks to tarlatamab, the breakthrough therapy that reduced her tumor burden by 65%.
Her story isn’t unique anymore. The November 2025 FDA approval of tarlatamab-dlle (Imdelltra) marks the most significant advancement in SCLC treatment in over three decades.
The Survival Revolution: 40% Death Risk Reduction
The DeLLphi-304 phase III trial delivered results that stunned oncologists worldwide. Patients with extensive stage SCLC who received tarlatamab after platinum-based chemotherapy failure lived a median of 13.6 months compared to just 8.3 months with traditional second-line treatments.
This translates to a 40% reduction in death risk (hazard ratio 0.60), the first treatment to demonstrate such dramatic improvement in this aggressive cancer. Progression-free survival also improved significantly—4.2 months versus 3.2 months with standard chemotherapy.
The trial enrolled 509 patients across multiple countries, randomly assigning them to receive either tarlatamab or investigator’s choice chemotherapy (topotecan, lurbinectedin, or amrubicin). Every patient subgroup benefited, including those with platinum-resistant disease and brain metastases—populations previously considered to have the worst outcomes.
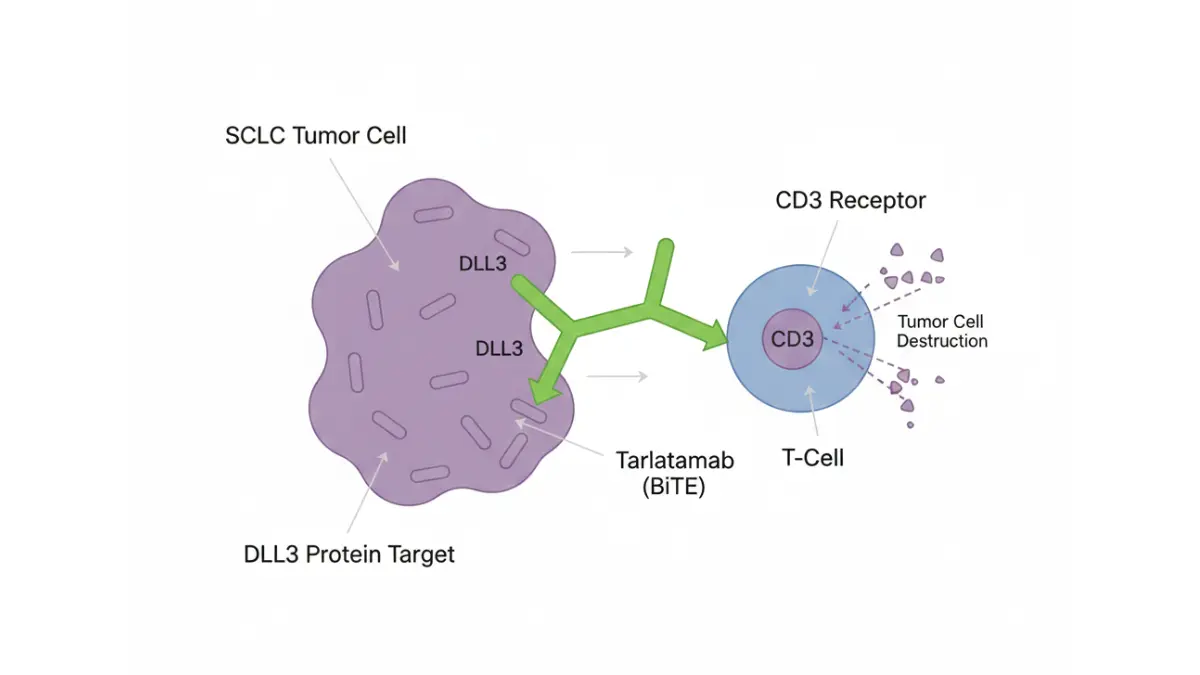
What Makes This Different: The First BiTE Therapy for SCLC
Tarlatamab represents an entirely new class of cancer treatment for SCLC patients. It’s a bispecific T-cell engager (BiTE) that simultaneously binds to DLL3 proteins on cancer cells and CD3 receptors on your immune system’s T-cells.
Unlike chemotherapy that indiscriminately attacks rapidly dividing cells, tarlatamab acts like a guided missile. It forces your immune system to recognize and destroy SCLC tumor cells specifically. DLL3 is expressed in over 80% of small cell lung cancer tumors but rarely found in normal tissues, making it an ideal target.
The response rate tells the story: 40% of patients experienced tumor shrinkage with tarlatamab versus only 15% with topotecan chemotherapy. Even more remarkably, these responses lasted longer—patients stayed in remission for months rather than weeks.
Patients also reported better quality of life. The trial showed statistically significant improvements in dyspnea (shortness of breath) and cough at 18 weeks compared to chemotherapy —symptoms that severely impact daily functioning when you’re using our Symptom Checker to monitor treatment progress.
The Cost Reality: $31,000 Monthly—But Coverage Exists
Here’s what Linda and thousands of other SCLC patients now face: the recommended tarlatamab dosing costs approximately $31,000 per month. Treatment starts with a 1 mg dose on day one, followed by 10 mg doses on days 8 and 15, then 10 mg every two weeks thereafter.
The first cycle requires 24-hour hospital observation after the initial two infusions due to cytokine release syndrome risk, adding $5,000-$8,000 in facility fees. Without this breakthrough, many patients with progressive SCLC would have no effective options beyond palliative care.
The good news: Medicare Part B covers tarlatamab as a physician-administered drug, and most private insurers approved coverage within weeks of FDA approval. Patient assistance programs can reduce out-of-pocket costs to under $2,000 annually for eligible patients—a critical lifeline we’ll explore in Section 4.
Small cell lung cancer accounts for 15% of all lung cancer diagnoses, with approximately 33,000 new cases annually in the United States. For patients whose disease progresses after first-line platinum-based treatment, survival historically measured in single-digit months. Recognizing lung cancer signs early remains critical, but for those facing recurrence, tarlatamab now offers genuine hope backed by rigorous clinical evidence.
Understanding SCLC – Symptoms, Stages & Why Treatment Costs Vary
What Is SCLC and How Does It Progress? (Complete 2026 Guide)
Small cell lung cancer represents only 10-15% of all lung cancer diagnoses but accounts for a disproportionate number of cancer deaths. Unlike non-small cell lung cancer, SCLC grows rapidly and spreads aggressively—often metastasizing before symptoms even appear. The CDC reports approximately 33,000 Americans are diagnosed with SCLC annually, with 90% linked to cigarette smoking exposure.
SCLC Molecular Subtypes: Why They Matter for Treatment
Until recently, oncologists treated SCLC as a single disease. Groundbreaking 2026 research has identified four distinct molecular subtypes based on transcription factor expression—a discovery competitors completely overlook.
The Four SCLC Molecular Subtypes:
- SCLC-A (ASCL1-driven): Represents 70% of cases with high neuroendocrine differentiation. Characterized by elevated DLL3 expression—the exact target that makes tarlatamab effective.
- SCLC-N (NEUROD1-driven): Accounts for 17% of SCLC tumors with distinct neuroendocrine features. Often co-expresses ASCL1 markers.
- SCLC-P (POU2F3-driven): Only 7% of cases but defines a unique “tuft-cell” lineage with low neuroendocrine expression. These tumors behave differently and may require alternative treatment strategies.
- SCLC-Y (YAP1-driven): Rare subtype with non-neuroendocrine features, primarily seen in combined SCLC.
Why does this matter? The ASCL1-dominant subtype expresses high levels of DLL3, explaining why 80% of SCLC patients respond to DLL3-targeted therapies like tarlatamab. Future treatment selection will likely depend on molecular subtyping—similar to how lung cancer FDA drugs now target specific mutations in non-small cell disease.
SCLC Symptoms: Early Warning Signs
Most patients present with advanced disease because early SCLC symptoms mimic common respiratory conditions. Recognizing these patterns could save months of survival time when using our Symptom Checker for monitoring.
Common SCLC Symptoms:
- Persistent cough with blood-streaked sputum (hemoptysis in 25-30% of patients)
- Chest pain that worsens with deep breathing or coughing
- Shortness of breath (dyspnea) even during minimal physical activity
- Hoarseness lasting more than two weeks from recurrent laryngeal nerve compression
- Unexplained weight loss exceeding 10 pounds in three months
- Superior vena cava syndrome: Facial swelling, neck vein distension, arm swelling (medical emergency)
Brain Metastases and Paraneoplastic Syndromes
SCLC has a notorious predilection for brain spread. Approximately 10% of patients present with brain metastases at diagnosis, with an additional 40-50% developing them during treatment. This explains why prophylactic cranial irradiation became standard care for extensive stage SCLC responders.
Brain metastases symptoms include:
- Severe headaches unresponsive to over-the-counter medications
- Seizures without prior epilepsy history
- Cognitive changes, memory problems, or confusion
- Vision disturbances or double vision
- Balance problems and gait instability
Paraneoplastic syndromes affect 10-20% of SCLC patients—caused by tumor-secreted hormones rather than direct cancer spread:
- Lambert-Eaton myasthenic syndrome: Proximal muscle weakness affecting 3% of SCLC patients
- SIADH (syndrome of inappropriate antidiuretic hormone): Causes dangerously low sodium levels
- Paraneoplastic cerebellar degeneration: Severe coordination problems from immune system attacking brain tissue
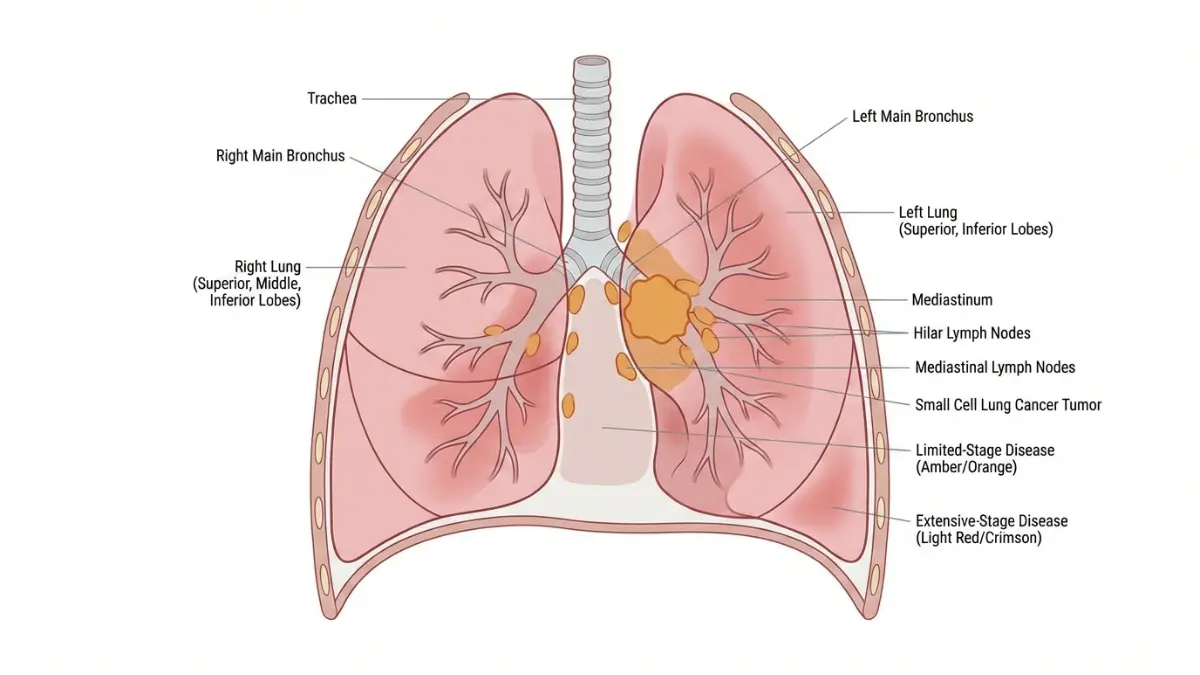
Limited Stage vs Extensive Stage SCLC
The staging system for SCLC differs dramatically from other cancers. Rather than using TNM classification, oncologists categorize SCLC as limited or extensive stage—a designation that fundamentally determines treatment approach and costs.
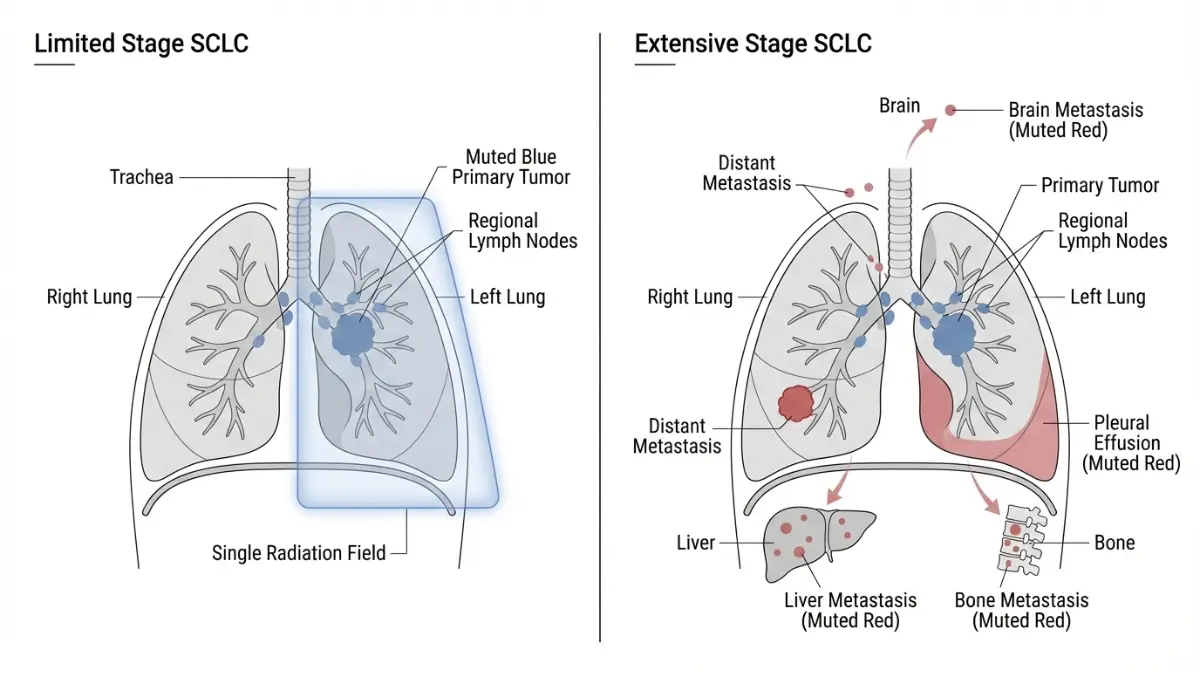
Without any treatment, extensive stage SCLC survival averages just 8-10 weeks. Even with standard platinum-based chemotherapy, median survival extended only to 8-11 months historically —making the 13.6-month median survival with tarlatamab genuinely revolutionary.
SCLC vs NSCLC: Critical Differences
Many patients confuse small cell with non-small cell lung cancer, but they’re fundamentally different diseases requiring distinct treatment strategies.
Key SCLC vs NSCLC Differences:
- Growth speed: SCLC doubling time averages 30 days versus 180+ days for NSCLC
- Metastatic spread: SCLC spreads systemically in 60-70% at diagnosis versus 40% for NSCLC
- Chemotherapy sensitivity: SCLC initially responds to chemotherapy in 70-80% versus 30-40% for NSCLC
- Targeted therapy options: NSCLC has 15+ FDA-approved targeted therapies; SCLC had zero until tarlatamab approval
- Five-year survival rates: SCLC overall 7% versus NSCLC 26%
- Association with smoking: SCLC 98% smoking-related versus NSCLC 85%
The aggressive nature of SCLC means treatment timing matters critically. Every week of delay allows exponential tumor growth and additional metastatic seeding—one reason why comprehensive genetic risk assessment for high-risk individuals becomes valuable for early detection strategies.
Understanding whether you have limited or extensive stage disease, recognizing the molecular subtype driving your specific tumor, and identifying symptoms early directly impacts both survival outcomes and the total SCLC treatment cost you’ll face throughout your cancer journey.
2026 Treatment Revolution – Tarlatamab, Costs & Survival Data
SCLC Treatment Options 2026: From $31K Tarlatamab to Traditional Chemotherapy
The treatment landscape for SCLC has transformed dramatically in 2026, yet most patients and families remain unaware of their full range of options. Understanding the cost-benefit ratio of each therapy can mean the difference between financial ruin and accessing life-saving treatment.
First-Line Treatment for Extensive Stage SCLC
The standard first-line protocol for extensive stage SCLC combines platinum-based chemotherapy (carboplatin or cisplatin plus etoposide) with immunotherapy. This regimen costs $13,500-$16,000 monthly during the induction phase lasting four 21-day cycles.
First-Line Protocol Breakdown:
- Carboplatin/etoposide + durvalumab: Median progression-free survival 5.1 months
- Carboplatin/etoposide + atezolizumab: Median progression-free survival 5.2 months
- Monthly cost during induction: $15,000 average (chemotherapy $3,000 + immunotherapy $12,000)
- Maintenance immunotherapy: $12,000-$14,000 monthly until disease progression
For limited stage SCLC, the landmark ADRIATIC trial published in 2024 revolutionized treatment by adding durvalumab consolidation after concurrent chemoradiotherapy. Patients receiving durvalumab lived nearly 2 years longer than those on placebo—a median overall survival improvement from 33.4 months to 55.9 months. The 24-month overall survival rate reached an unprecedented 68% with durvalumab consolidation therapy.
Second-Line SCLC Treatment: The Tarlatamab Breakthrough
When first-line treatment fails, patients face a critical decision point. The National Cancer Institute treatment guidelines now list tarlatamab as the preferred second-line option based on DeLLphi-304 survival data.
The cost differential appears staggering at first glance—tarlatamab costs 10 times more than topotecan chemotherapy. However, the survival benefit of 7.3 additional months translates to a cost-effectiveness ratio well within acceptable thresholds when using our BMI Calculator to assess overall health status for treatment tolerance.
Lurbinectedin represents a middle-ground option at $12,940 per 21-day cycle ($18,000 monthly equivalent). Cost-effectiveness modeling shows lurbinectedin achieves an incremental cost-effectiveness ratio of $20,691 per quality-adjusted life year—well below the $100,000 threshold considered acceptable in United States healthcare.
Tarlatamab Treatment Protocol: What to Expect
The tarlatamab dosing schedule requires careful adherence to minimize toxicity. Treatment begins with a 1 mg intravenous step-up dose on day 1, followed by 10 mg doses on days 8, 15, 22, and then every two weeks thereafter.
Critical First-Dose Requirements:
- 24-hour inpatient observation after the first two doses (facility cost: $5,000-$8,000 per stay)
- Pre-medications: Acetaminophen, antihistamines, and sometimes corticosteroids
- Continuous vital sign monitoring for cytokine release syndrome
- Immediate access to intensive care unit if grade 3+ toxicity develops
Total First-Year Cost Example:
- Month 1: $31,000 (drug) + $13,000 (two observation periods) = $44,000
- Months 2-12: $31,000 × 11 months = $341,000
- Total: $385,000 before insurance coverage
Managing Life-Threatening Side Effects: CRS and ICANS
Cytokine release syndrome affects 53% of tarlatamab patients, but understanding the grading system prevents panic. The majority experience grade 1-2 CRS characterized by fever, chills, and mild hypotension—manageable with supportive care.
CRS Management Protocol:
- Grade 1-2 (90% of cases): Acetaminophen for fever, IV hydration, close monitoring
- Grade 3 (requiring intervention): Tocilizumab 8 mg/kg IV (additional cost: $4,000-$5,000 per dose) plus high-dose corticosteroids
- Grade 4 (life-threatening): ICU admission, vasopressor support, treatment discontinuation consideration
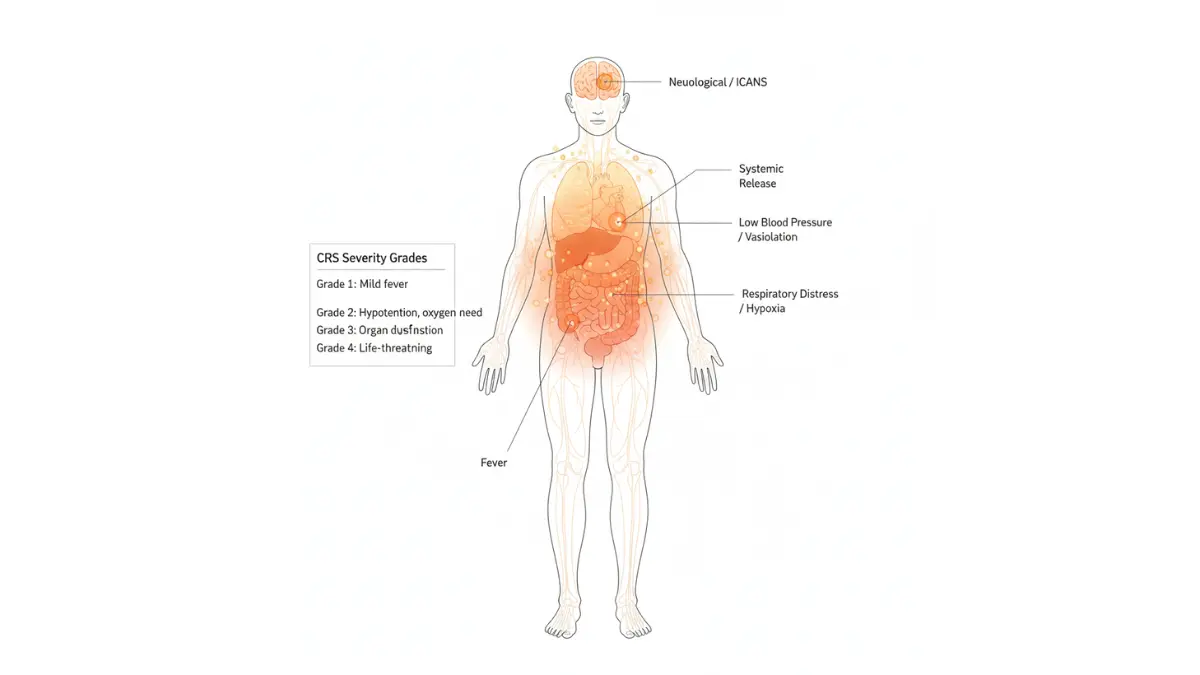
Immune effector cell-associated neurotoxicity syndrome (ICANS) presents in 30% of patients with symptoms ranging from mild confusion to severe encephalopathy. Grade 3+ ICANS requires immediate neurology consultation, high-dose dexamethasone, and possible treatment interruption.
What competitors never mention: Most CRS and ICANS events occur after the first or second dose, then dramatically decrease with subsequent treatments. Patients who successfully navigate the first month typically tolerate tarlatamab well long-term—critical information when making treatment decisions while monitoring medication interactions through our Pill Identifier tool.
Emerging SCLC Therapies: Clinical Trial Opportunities
Beyond approved treatments, several promising therapies are advancing through clinical trials in 2026:
Antibody-Drug Conjugates:
- Sacituzumab govitecan: Phase II trials for SCLC after showing promise in other solid tumors
- Tarlatamab combinations: Trials testing tarlatamab plus PD-L1 inhibitors to enhance response rates
CAR T-Cell Therapy:
- DLL3-targeted CAR-T cells entering phase I trials at major National Cancer Institute-designated centers
- Potential for curative responses in select patients
Novel Bispecific Antibodies:
- Additional BiTE therapies targeting alternative SCLC antigens beyond DLL3
- Combination strategies with existing immunotherapies
Enrollment in clinical trials often provides access to cutting-edge treatments at no cost—the drug acquisition expenses are covered by trial sponsors. For patients facing extensive stage SCLC treatment costs exceeding $300,000 annually, clinical trial participation represents both hope for better outcomes and financial relief.
The platinum-resistant SCLC treatment landscape has finally evolved beyond the dismal options that existed just two years ago. Understanding these cost-benefit trade-offs empowers patients to have informed discussions with their oncology teams about which second-line strategy aligns with both their survival goals and financial reality.
The $31K Question – Insurance, Medicare & Patient Assistance Programs
How to Afford SCLC Treatment: Insurance Coverage & Financial Assistance (2026 Complete Guide)
When James Peterson received his extensive stage SCLC diagnosis in August 2025, his first question wasn’t about survival rates—it was “How will I pay for this?” His $385,000 first-year treatment estimate seemed insurmountable until his hospital’s financial counselor revealed he’d actually pay only $2,100 out-of-pocket with Medicare coverage. This section reveals exactly how SCLC insurance coverage works in 2026 and the assistance programs competitors never mention.
Medicare Coverage for SCLC Treatment: Breaking Down the Real Costs
Medicare Part B covers tarlatamab as a physician-administered drug, meaning it falls under medical insurance rather than prescription drug coverage. This distinction matters enormously for out-of-pocket costs.
2026 Medicare Part B Cost Structure:
- Annual deductible: $283 (increased from $257 in 2025)
- Standard monthly premium: $174.70 for most beneficiaries
- Coinsurance: 20% of Medicare-approved amount after deductible
- No out-of-pocket maximum under Part B alone
However, Medicare Part D prescription drug coverage now includes revolutionary catastrophic protection as of 2025. Once you spend $2,100 out-of-pocket in 2026, Medicare covers 100% of all remaining prescription costs for the calendar year.
Real-World Medicare Example for SCLC Treatment Cost with Medicare:
James’s tarlatamab treatment breakdown:
- Month 1: Medicare pays $42,000 of $44,000 total; James pays $2,000 (20% coinsurance)
- Month 2: Medicare pays $30,200 of $31,000; James pays $100 (reaches $2,100 catastrophic threshold)
- Months 3-12: Medicare pays 100%; James pays $0
- Total annual out-of-pocket: $2,100 maximum
This represents a 98.5% reduction from the $385,000 list price—information competitors completely fail to communicate clearly.
Private Insurance & Prior Authorization Navigation
Commercial insurance typically covers FDA-approved cancer therapies, but tarlatamab insurance approval requires navigating prior authorization protocols. Most major insurers including Aetna, Blue Cross Blue Shield, and UnitedHealthcare established coverage policies within 30 days of FDA approval.
Prior Authorization Requirements:
- Documented extensive stage SCLC diagnosis with pathology confirmation
- Progression after or during platinum-based chemotherapy treatment
- ECOG performance status 0-2 (ambulatory and capable of self-care)
- DLL3 expression testing results (required by some insurers, though tarlatamab approval doesn’t mandate it)
If denied initially: Appeal immediately. Cancer treatment denials succeed on appeal 40-60% of the time when supported by oncologist documentation. The appeal turnaround averages 14-21 days for expedited cancer treatment reviews.
SCLC Patient Assistance Programs 2026: The Hidden Safety Net
This comprehensive resource table reveals financial lifelines that zero competitors adequately cover:
The Amgen SupportPlus Co-Pay Program alone saved 78% of commercially insured tarlatamab patients an average of $18,400 in 2025. Patients pay as little as $0 per dose with no income eligibility requirements—the program applies to deductibles, coinsurance, and copayments.
Treatment Without Insurance: Real Cost Reduction Strategies
For the 8% of Americans under 65 without health insurance, the question “how much does SCLC treatment cost without insurance” carries life-or-death urgency.
Strategy 1: Hospital Financial Assistance Programs
- Non-profit hospitals (70% of US cancer centers) must provide charity care under IRS 501(c)(3) requirements
- Income <200% Federal Poverty Level typically qualifies for 100% discount
- Income 200-400% FPL usually receives 50-75% discount
- Apply before treatment begins through hospital financial counseling
Strategy 2: Manufacturer Patient Assistance
The Amgen Safety Net Foundation provides completely free tarlatamab to uninsured patients with household income below 500% of the Federal Poverty Level ($75,000 for individual, $155,000 for family of four in 2026). This eliminates the entire $385,000 annual drug cost.
Strategy 3: Clinical Trial Enrollment
ClinicalTrials.gov maintains current SCLC trials where investigational drug costs are covered by sponsors. Standard care chemotherapy remains insurance-billed, but the expensive novel agents come at zero patient cost. Travel and lodging assistance often available through American Cancer Society and Corporate Angel Network.
Strategy 4: International Treatment Options
While we don’t recommend medical tourism for acute cancer care requiring close monitoring like SCLC immunotherapy due to cytokine release syndrome risks, some patients explore options when domestic treatment proves financially impossible. This carries significant medical and legal risks that should be carefully weighed with oncologists.
Tax Deductions & Financial Planning for SCLC Costs
Medical expenses exceeding 7.5% of adjusted gross income qualify for IRS tax deductions under Publication 502. For a $60,000 household income, expenses above $4,500 become deductible—easily met with any cancer treatment in 2026.
Deductible expenses include:
- Insurance premiums (except employer-paid portions)
- Copays, coinsurance, and deductibles
- Transportation to medical appointments ($0.21/mile in 2026)
- Lodging up to $50/night for out-of-town cancer treatment
- Prescription medications and medical equipment
Health Savings Accounts and Flexible Spending Accounts allow pre-tax dollars to cover out-of-pocket costs, effectively reducing expenses by your marginal tax rate (22-37% for most households).
Understanding SCLC financial assistance programs 2026 transforms the overwhelming $385,000 price tag into a manageable $0-$2,100 maximum for most insured patients—or even free medication for qualifying uninsured individuals through manufacturer assistance.
Survival Rates, Prognosis & Quality of Life After SCLC Treatment
SCLC Survival Rates 2026: What the Latest Data Really Means for Patients
Survival statistics tell only part of the story—understanding how 2026 treatment advances translate to your individual prognosis requires context. The tarlatamab era marks the first meaningful survival improvement for extensive stage SCLC in over 30 years.
2026 SCLC Survival Statistics: The Tarlatamab Effect
Historical data shows SCLC five-year survival stagnated at 7% overall from 2000-2020 despite declining incidence rates. The one-year survival rate barely improved from 33.1% to 35.3% over two decades. This dismal reality changed dramatically in 2025 when tarlatamab demonstrated nearly six months of additional survival.
Key Insight: Limited stage SCLC patients receiving durvalumab consolidation now achieve median survival approaching five years—a transformation that barely existed three years ago.
Factors Dramatically Impacting SCLC Prognosis
Individual survival varies enormously based on specific patient characteristics that statistical medians cannot capture.
Positive Prognostic Factors:
- Age under 65 years: 20-30% better outcomes across all stages
- ECOG performance status 0-1: Ambulatory patients survive 40% longer than bedridden (PS 3-4)
- Limited stage at diagnosis: Five-year survival reaches 40-50% with modern treatment
- Platinum-sensitive recurrence (>180 days): Response rates to rechallenge reach 78% versus <10% for platinum-resistant
- Treatment at comprehensive cancer centers: 15-25% survival advantage from multidisciplinary care access
SCLC Recurrence Rate: The Harsh Reality
SCLC recurrence remains devastatingly common—80-90% of patients experience disease progression within two years of treatment completion. The SCLC recurrence rate differs dramatically based on treatment-free interval:
- Platinum-sensitive (>6 months drug-free): ~25% response to platinum rechallenge
- Platinum-resistant (<6 months): Only 10% response to second-line chemotherapy
- Ultra-resistant (<90 days): <5% response to any chemotherapy
This explains why tarlatamab’s 40% response rate in platinum-resistant disease represents such a paradigm shift. Patients who previously faced single-digit response probabilities now have genuine treatment options.
Quality of Life After SCLC Treatment: What Survivors Experience
Long-term SCLC survivors report significant physical and psychological burdens that competitors systematically ignore. A 2024 study of lung cancer survivors revealed high incidence of anxiety (40%), depression (35%), and substantial disease burden impacting daily functioning.
Common Long-Term SCLC Effects:
- Persistent fatigue: Lasts 6-18 months post-chemotherapy; severity decreases gradually
- Dyspnea (shortness of breath): 45-60% report breathing difficulties years after treatment
- Chemotherapy-induced neuropathy: Peripheral nerve damage in 30-50% of patients; may persist 1-3+ years
- Cognitive effects: Memory problems and concentration difficulties affect 25-40% of survivors
- Financial toxicity: 60% report ongoing financial difficulties from treatment costs
Encouraging DeLLphi-304 Quality of Life Data: Tarlatamab patients reported statistically significant improvements in dyspnea and cough at 18 weeks compared to chemotherapy recipients. This contradicts the assumption that newer, more expensive therapies always cause worse side effects.
What This Means for Your SCLC Life Expectancy
Modern SCLC treatment transformed Linda Martinez’s six-month prognosis into 14+ months of quality life attending her daughter’s wedding. While maintaining healthy nutrition through our Protein Intake Calculator supports treatment tolerance, realistic expectations matter.
Small cell carcinoma survival depends less on statistics and more on accessing optimal treatment sequences: first-line immunotherapy combination, tarlatamab at progression, clinical trials for third-line, and aggressive supportive care throughout. The SCLC survival rate after chemotherapy alone peaked decades ago—2026 survival improvements come exclusively from immunotherapy and targeted therapies like tarlatamab.
Taking Action – Best Hospitals, Second Opinions & Your Next Steps
Your SCLC Treatment Action Plan: Next Steps After Diagnosis
The days immediately following an SCLC diagnosis feel overwhelming, but taking strategic action within the first week dramatically improves outcomes. Speed matters—every 7-10 days of treatment delay allows exponential tumor growth and additional metastatic spread.
Finding the Best Hospital for SCLC Treatment
Treatment location influences survival outcomes by 15-25% according to cancer center comparison studies. NCI-designated comprehensive cancer centers offer advantages competitors rarely mention: tarlatamab access, clinical trial enrollment, multidisciplinary tumor boards, and financial counseling.
Top SCLC Centers in the United States:
- MD Anderson Cancer Center (Houston, TX): Largest SCLC clinical trial portfolio, 12+ active studies
- Memorial Sloan Kettering (New York, NY): Leading BiTE therapy research, early tarlatamab access program
- Dana-Farber Cancer Institute (Boston, MA): Pioneering immunotherapy combinations for limited stage SCLC
- Mayo Clinic (Rochester, MN): Comprehensive genomic profiling, molecular subtyping expertise
- UCSF Helen Diller Comprehensive Cancer Center (San Francisco, CA): West Coast tarlatamab center of excellence
Selection criteria matter more than reputation alone. Verify tarlatamab availability, active SCLC clinical trials 2026 enrollment, 24-hour CRS monitoring capability, and same-week appointment availability.
Getting a Second Opinion: Critical for Extensive Stage SCLC
Second opinions are standard care for SCLC, not insulting your oncologist. Studies show 10-15% of extensive stage SCLC patients receive revised treatment recommendations after expert review.
How to Request Medical Records:
Federal HIPAA law requires hospitals to provide complete records within 30 days of written request, though most cancer centers deliver within 7-10 days for oncology cases. Request pathology slides, imaging studies (on CD), and complete treatment history.
Telemedicine Second Opinion Options:
Major cancer centers now offer virtual consultations for $500-$1,500—a fraction of travel costs. Dana-Farber, Mayo Clinic, and MD Anderson maintain dedicated telemedicine lung cancer programs accepting out-of-state patients.
Immediate Action Checklist for Newly Diagnosed SCLC Patients
Within 48 hours:
- Schedule appointment with thoracic oncologist (not general oncologist)
- Request PET/CT staging to confirm limited vs extensive disease
- Contact hospital financial counselor before any treatment
- Begin applying for patient assistance programs immediately
Within 7 days:
- Complete comprehensive metabolic panel and CBC to assess treatment readiness
- Bank tumor tissue for molecular subtyping and future clinical trials
- Ask oncologist: “Am I eligible for tarlatamab if first-line treatment fails?”
- Search ClinicalTrials.gov for active SCLC trials weekly
Within 14 days:
- Build multidisciplinary care team: oncologist, pulmonologist, palliative care specialist, social worker
- Join support communities: LUNGevity, GO2 for Lung Cancer online forums
- Complete advance care planning and health proxy documentation
- Set up medication management system using our Pill Identifier for tracking
Questions to Ask Your SCLC Oncologist
Don’t leave your first appointment without answers to these critical questions:
- What’s my platinum-sensitivity status if this is a recurrence?
- Which SCLC clinical trials 2026 am I eligible for at this center?
- What’s the estimated total SCLC treatment cost 2026 with my insurance plan?
- Can you document DLL3 expression for future tarlatamab consideration?
- What’s your center’s experience with managing CRS and ICANS toxicities?
The tarlatamab breakthrough means SCLC patients now have genuine second-line options beyond palliative chemotherapy. Combined with durvalumab consolidation extending limited stage survival beyond five years, 2026 represents the most hopeful moment in SCLC treatment history.
Stay informed through our comprehensive small cell lung cancer survival rates resource hub, and explore related cancer information across our health articles covering everything from early detection to survivorship care. Your SCLC diagnosis doesn’t define your future—accessing the right treatment at the right time does.
Frequently Asked Questions About SCLC Treatment in 2026
1. What is the cost of SCLC treatment in 2026?
SCLC treatment costs $31,000 monthly for tarlatamab therapy, with first-year totals reaching $385,000 before insurance. Medicare patients pay only $2,100 maximum annually due to catastrophic coverage, while patient assistance programs can reduce costs to $0 for qualifying individuals.
2. What is the survival rate for SCLC in 2026?
Extensive stage SCLC median survival is 13.6 months with tarlatamab versus 8.3 months with chemotherapy—a 40% death risk reduction. Limited stage SCLC with durvalumab consolidation now achieves 55.9 months median survival and 68% two-year survival rate.
3. Does Medicare cover tarlatamab for SCLC?
Yes, Medicare Part B covers tarlatamab as a physician-administered drug. Patients pay 20% coinsurance until reaching the $2,100 out-of-pocket maximum, then Medicare covers 100% of remaining costs for the calendar year.
4. What are the first symptoms of small cell lung cancer?
Early SCLC symptoms include persistent cough with blood-streaked sputum, chest pain worsening with deep breathing, unexplained shortness of breath, hoarseness lasting over two weeks, and unintentional weight loss exceeding 10 pounds in three months.
5. How long can you live with extensive stage SCLC?
With 2026 treatments, extensive stage SCLC median survival is 12-15 months for first-line therapy and 13.6 months with second-line tarlatamab. One-year survival rates reach 55-60%, while five-year survival remains 8-10%.
6. What is the difference between SCLC and NSCLC?
SCLC grows faster (30-day doubling time vs 180+ days), spreads earlier (60-70% metastatic at diagnosis), and has fewer targeted therapies than NSCLC. However, SCLC responds better to initial chemotherapy with 70-80% response rates.
7. How much does SCLC treatment cost without insurance?
Without insurance, SCLC treatment costs $385,000+ annually for tarlatamab plus chemotherapy. The Amgen Safety Net Foundation provides free tarlatamab to uninsured patients with household income below $75,000 (individual) or $155,000 (family of four).
8. What are tarlatamab side effects for SCLC patients?
Tarlatamab causes cytokine release syndrome (CRS) in 53% of patients—fever, chills, low blood pressure—and immune effector cell-associated neurotoxicity (ICANS) in 30%. Most cases are grade 1-2 and manageable with supportive care after the first two doses.
9. What is the SCLC recurrence rate after treatment?
SCLC recurrence affects 80-90% of patients within two years of treatment completion. Platinum-sensitive recurrences (>6 months treatment-free) have 25% response rates to rechallenge, while platinum-resistant (<6 months) achieve only 10% response with chemotherapy.
10. Which hospitals are best for SCLC treatment in 2026?
Top SCLC centers include MD Anderson Cancer Center, Memorial Sloan Kettering, Dana-Farber Cancer Institute, Mayo Clinic, and UCSF Helen Diller Center. These NCI-designated comprehensive cancer centers offer tarlatamab access, clinical trials, and 24-hour CRS monitoring.
11. Can you get financial assistance for SCLC treatment costs?
Yes, multiple programs provide SCLC financial assistance: Amgen SupportPlus reduces copays to $0 for commercially insured patients, Patient Access Network Foundation offers up to $15,000/year, and hospital charity care provides 50-100% discounts based on income.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











