On This Page – Quick Medical Summary
What Your Colonoscopy Results Really Mean
Sarah, a 52-year-old teacher from Ohio, sat in her car staring at the patient portal notification: “Your colonoscopy results are ready.” Her hands trembled as she clicked. The report showed “tubular adenoma with low-grade dysplasia”—words that meant nothing to her but triggered immediate panic. Three days later, after understanding what her colonoscopy result actually indicated, Sarah felt relief wash over her. The polyp had been removed successfully during the procedure, and she simply needed a follow-up screening in five years instead of the standard ten.
Your colonoscopy result tells you what your doctor found inside your colon during the procedure—ranging from completely normal findings to polyps, inflammation, or signs requiring further attention. Most people (50-70%) receive normal results, while 25-30% have benign polyps removed during the procedure. Only 3-5% of colonoscopy findings reveal advanced polyps or cancer requiring immediate intervention.
This comprehensive 2026 guide decodes every possible colonoscopy finding using real pathology report examples, updated screening guidelines, and evidence-based follow-up protocols. You’ll learn exactly what each result means, when you’ll receive different types of findings, and what actions to take in the next 24-48 hours. Whether your report mentions adenomas, sessile serrated lesions, or shows completely clear results, you’ll understand the medical terminology and know your precise next steps.
Why read this today? New 2026 guidelines from the American Gastroenterological Association have modified surveillance intervals for certain polyp types, affecting millions of Americans’ follow-up schedules. Understanding your colonoscopy result accurately can prevent unnecessary anxiety and ensure you follow the correct monitoring timeline for your specific situation.
Understanding Your Results Timeline & Delivery Process
When and How You’ll Receive Your Colonoscopy Results
The timing and method of receiving your colonoscopy result depends entirely on what your gastroenterologist found during the visual examination and whether tissue samples required laboratory analysis.
Immediate Results (Day 0)
Your doctor typically discusses preliminary colonoscopy findings while you’re still in the recovery area, usually 30-60 minutes after your procedure ends. Because sedation medications like midazolam affect short-term memory, many patients don’t fully recall this conversation—which is completely normal.
What you’ll learn immediately:
- Whether the examination was complete (cecum reached)
- If polyps were visualized and removed
- Visual appearance of your colon lining
- Recommended follow-up timeline (preliminary)
The quality of your bowel preparation significantly impacts result accuracy. According to the American College of Gastroenterology, inadequate preparation requires repeat colonoscopy within 1 year because up to 27% of polyps can be missed with poor visibility.
Key distinction: Visual findings (what your doctor sees) differ from pathology findings (what laboratory analysis reveals). Your doctor can identify and remove a polyp immediately, but determining whether that polyp contains precancerous cells requires microscopic examination by a pathologist.
| Result Type | Timing | Delivery Method | Completeness |
|---|---|---|---|
| Visual findings | Day 0 (immediate) | Verbal + procedure notes | Preliminary assessment |
| Normal (no biopsies) | Day 0 (immediate) | Verbal confirmation | Complete and final |
| Pathology results | 5-10 business days | Portal, phone, or mail | Complete and final |
| Cancer findings | 2-3 days (expedited) | Phone call from doctor | Requires staging workup |
The 5-10 Business Day Pathology Window
When your gastroenterologist removes polyps or takes tissue biopsies, those specimens travel to a pathology laboratory where specialists examine them under microscopes using various staining techniques. This process cannot be rushed without compromising accuracy.
What pathologists evaluate:
- Cell type and architecture (histology)
- Presence and grade of dysplasia
- Depth of tissue involvement
- Margins of resection (complete vs incomplete removal)
Michael Chen, a 58-year-old engineer from California, received his pathology report 7 business days after his colonoscopy. The report confirmed three small tubular adenomas with low-grade dysplasia—all completely removed. His doctor called to discuss the findings and scheduled his next colonoscopy for 5 years later, rather than the 10-year interval for normal results. The National Cancer Institute emphasizes that polyp removal during colonoscopy reduces colorectal cancer incidence by up to 76-90% when appropriate surveillance follows.
Expedited protocols for cancer: If your gastroenterologist suspects malignancy based on visual appearance, most pathology departments prioritize these specimens. You’ll typically receive a phone call within 48-72 hours, followed by rapid referral to oncology and surgical consultations.
Understanding Different Communication Methods
The delivery method for your colonoscopy result often signals the urgency and complexity of findings, though practices vary by healthcare system.
Phone calls typically indicate:
- Abnormal findings requiring discussion
- Follow-up colonoscopy needed sooner than 10 years
- Additional testing or specialist referral recommended
- Questions about your symptoms or family history
Patient portal messages commonly deliver:
- Normal results with no polyps found
- Routine pathology reports for small benign polyps
- Confirmation of follow-up intervals
- Copies of procedure reports and images
Standard mail usually contains:
- Official procedure documentation
- Detailed pathology reports
- Insurance coding and billing information
- Follow-up appointment reminders
If you experience any concerning symptoms after your colonoscopy—including severe abdominal pain, fever over 100.4°F, or heavy rectal bleeding—use our symptom checker and contact your doctor immediately, regardless of when results are scheduled.
Pro tip: Request access to your colonoscopy images through your patient portal. Most modern colonoscopy equipment captures high-resolution photos of your cecum (proving complete examination) and any abnormalities found. These images help you understand your results and provide valuable documentation if you need a second opinion.
Decoding Normal Colonoscopy Results
What “Normal” or “Negative” Results Actually Mean
A normal colonoscopy result means your gastroenterologist completed a thorough examination of your entire colon and found no polyps, masses, inflammation, or other abnormalities requiring intervention. This outcome occurs in approximately 50-70% of screening colonoscopies for average-risk adults.
Components of a Clean Colonoscopy Report
Your procedure report should document three critical quality indicators that validate the thoroughness and reliability of your examination. These metrics directly impact how confident you and your doctor can feel about your normal results.
“Adequate bowel preparation” indicates your colon was clean enough for accurate visualization. The Boston Bowel Preparation Scale rates each colon segment from 0-3, with scores of 2 or 3 considered adequate. Research from the American Gastroenterological Association shows that poor preparation leads to polyp miss rates as high as 27% for small polyps and 12% for larger adenomas.
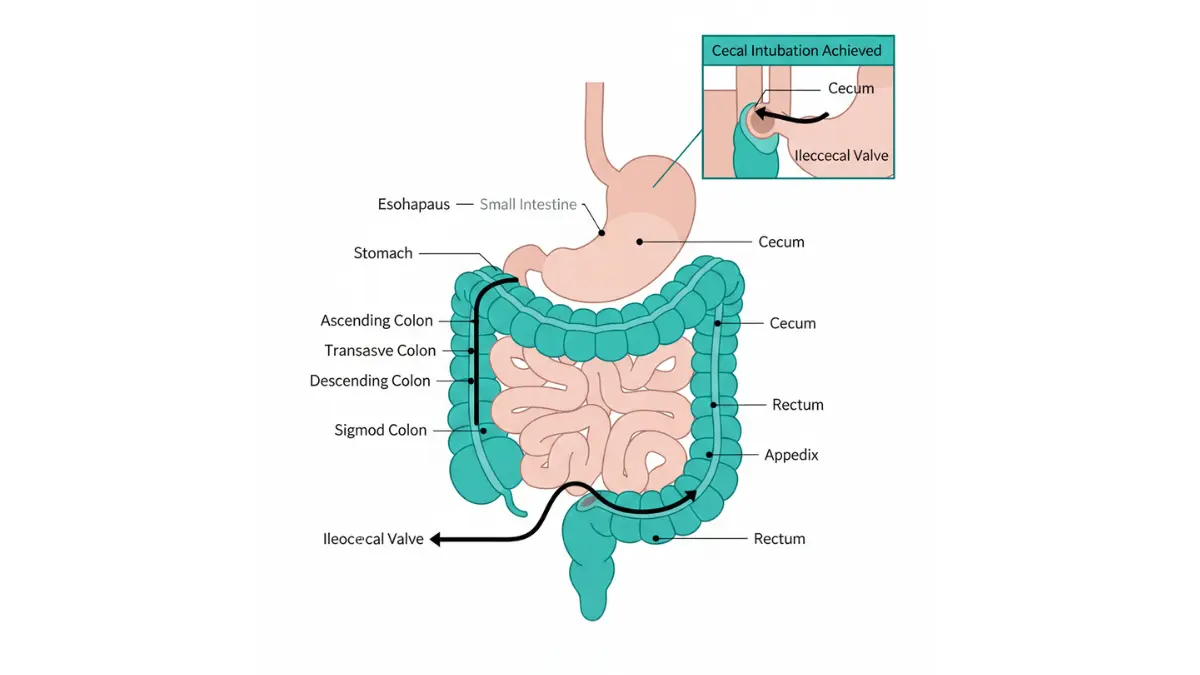
“Cecal intubation achieved” confirms your doctor reached the beginning of your colon (where it connects to your small intestine). Complete examination requires visualizing the cecum and typically photographing the ileocecal valve and appendiceal orifice as landmarks. Incomplete colonoscopies miss up to 20% of polyps located in the right colon—the same area where aggressive cancers often develop.
Withdrawal time measures how long your gastroenterologist spent carefully examining your colon lining while removing the colonoscope. Studies published by the National Institutes of Health demonstrate that withdrawal times under 6 minutes correlate with significantly lower polyp detection rates. High-quality exams typically involve 7-10 minutes of withdrawal time for normal colons.
Your Follow-Up Schedule After Normal Results
With a high-quality normal colonoscopy result, average-risk adults typically wait 10 years before their next screening. However, several factors modify this timeline based on your individual risk profile.
Standard 10-year interval applies when:
- No polyps or masses detected
- Adequate bowel preparation achieved
- Complete cecal examination documented
- No personal history of inflammatory bowel disease
- No first-degree relatives with colorectal cancer before age 60
Shortened intervals may be recommended for:
- Strong family history (parent or sibling diagnosed before age 60): 5-year intervals
- Personal history of inflammatory bowel disease: 1-3 year intervals depending on disease extent
- Previous adenomas removed in prior colonoscopy: 3-5 year intervals based on polyp characteristics
- Hereditary cancer syndromes like Lynch syndrome: annual screening often required
Jennifer Rodriguez, a 49-year-old accountant from Texas, received normal colonoscopy results but learned her follow-up should occur in 5 years instead of 10. Her father was diagnosed with colon cancer at age 58, placing her at increased risk despite her clean results. Since obesity increases colorectal cancer risk by 30-50% according to Centers for Disease Control data, she also used our BMI calculator to track weight management as an additional prevention strategy.
| Risk Category | Next Colonoscopy | Key Factors |
|---|---|---|
| Average risk, normal results | 10 years | No polyps, no family history, age 45-75 |
| One first-degree relative with CRC age 60+ | 10 years | Same as average risk per 2026 guidelines |
| One first-degree relative with CRC before age 60 | 5 years | Start at age 40 or 10 years before relative’s diagnosis |
| Multiple first-degree relatives with CRC | 3-5 years | Consider genetic counseling |
| Personal history IBD (extensive colitis) | 1-3 years | Depends on disease duration and extent |
| Lynch syndrome confirmed | 1-2 years | Begin age 20-25 or 2-5 years before earliest family diagnosis |
What Normal Results DON’T Rule Out
While a normal colonoscopy result provides excellent reassurance about colorectal health, certain conditions require different diagnostic approaches and won’t be detected during standard colonoscopy.
Microscopic colitis causes chronic watery diarrhea but shows normal-appearing colon lining. Diagnosis requires random biopsies during colonoscopy, which aren’t routinely performed unless you have diarrhea symptoms. If you experience ongoing digestive symptoms despite normal colonoscopy findings, discuss additional testing with your gastroenterologist.
Functional disorders like irritable bowel syndrome (IBS) don’t show structural abnormalities on colonoscopy. Your normal result helps exclude inflammatory bowel disease and cancer but doesn’t explain IBS symptoms, which require clinical diagnosis based on symptom patterns.
Small intestinal diseases including celiac disease and Crohn’s disease affecting only the small bowel won’t be visible during colonoscopy, which examines only the large intestine and last few inches of the ileum. Separate testing may be needed for upper GI symptoms.
If you develop new symptoms after receiving normal colonoscopy results—such as blood in stool, unexplained weight loss, persistent abdominal pain, or change in bowel habits—contact your doctor promptly. While your colonoscopy reduces cancer risk, it doesn’t eliminate it completely, and new symptoms warrant evaluation regardless of recent normal findings.
Understanding Polyps & Abnormal Findings
Complete Guide to Colonoscopy Polyp Results
Polyps appear in approximately 25-30% of screening colonoscopies, with prevalence increasing significantly with age. Finding polyps during your colonoscopy result doesn’t mean you have cancer—in fact, the opposite is true. Polyp removal during colonoscopy prevents up to 90% of potential colorectal cancers by eliminating precancerous growths before they transform into malignancy.
Polyp Classification System Explained
Your pathology report classifies each polyp by size, shape, and location—factors that directly influence your cancer risk and follow-up colonoscopy timing.

Size categories and implications:
- 1-5mm (diminutive polyps): Typically low risk, often hyperplastic in the rectosigmoid region
- 6-9mm (small polyps): Moderate surveillance requirements, especially if adenomatous
- ≥10mm (large polyps): Higher malignancy risk (10-15% contain high-grade dysplasia or cancer)
- ≥20mm (giant polyps): May require specialized removal techniques or surgical referral
Shape classifications matter:
- Pedunculated polyps grow on stalks, allowing easier complete removal with snare polypectomy
- Sessile polyps lack stalks and sit flat against the colon wall, requiring careful removal to prevent incomplete resection
- Flat or depressed lesions pose the highest risk for containing advanced pathology and can be challenging to detect
A comprehensive study published by Duke University School of Medicine found that colonoscopists with adenoma detection rates below 20% missed significantly more advanced neoplasia compared to physicians detecting adenomas in 30% or more of screening exams. This quality metric directly impacts patient outcomes.
Types of Polyps and Cancer Risk
Your pathology report reveals the most critical information: polyp histology (cell type). This classification determines both your cancer risk and surveillance colonoscopy schedule.
Hyperplastic Polyps (25-40% of all polyps)
These small, sawtooth-patterned polyps typically occur in the rectum and sigmoid colon. They carry essentially zero malignancy risk when small and located in the left colon.
- Appearance: Usually <5mm, pale or same color as surrounding tissue
- Cancer risk: Near zero for typical rectosigmoid hyperplastic polyps
- Follow-up: Return to 10-year interval if only small hyperplastic polyps found
Important exception: Large (≥10mm) hyperplastic polyps in the right colon require the same surveillance as sessile serrated lesions.
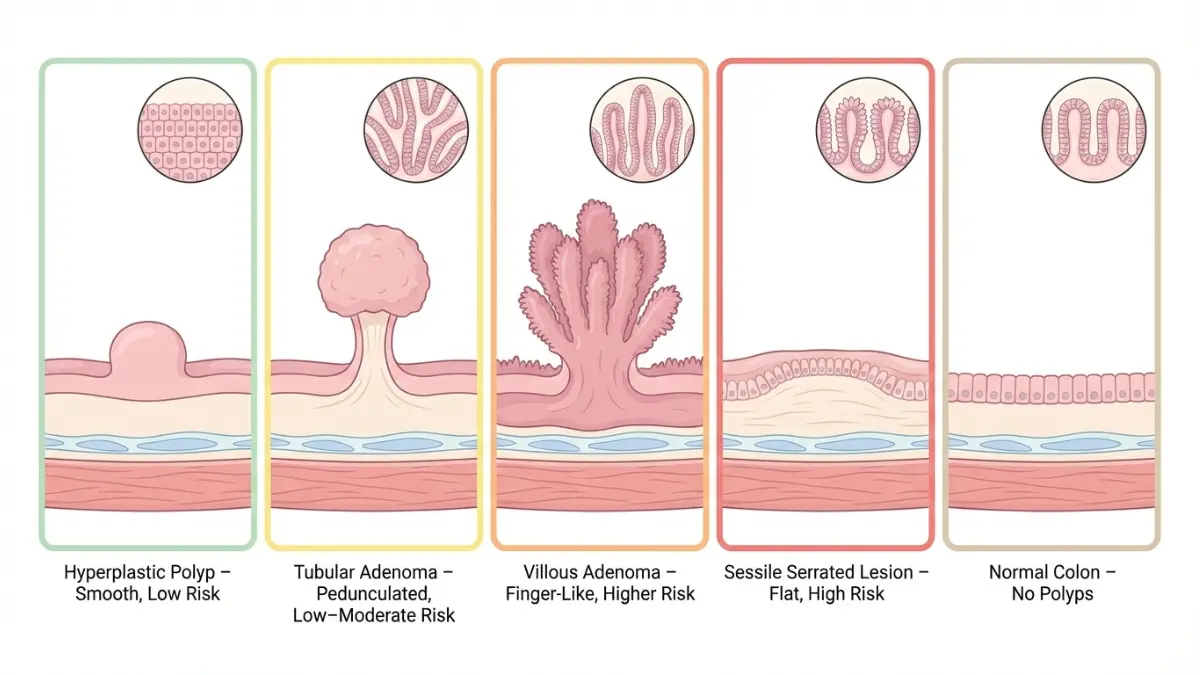
Adenomatous Polyps (60-70% of all polyps)
Adenomas are precancerous polyps that, if left in place for years, can progress to colorectal cancer. The transformation typically takes 10-15 years, which is why colonoscopy screening is so effective at prevention.
Tubular adenomas (80-85% of adenomas):
- Most common adenoma type
- Lowest malignancy risk among adenomas (5-10% if >1cm)
- Well-circumscribed with visible blood vessels
- Complete removal during colonoscopy is usually straightforward
David Morrison, a 62-year-old from Michigan, learned his colonoscopy result showed two small tubular adenomas (6mm and 8mm), both completely removed with low-grade dysplasia. His gastroenterologist explained that his 5-year surveillance interval would prevent any progression to cancer. Since maintaining a healthy weight reduces adenoma recurrence risk by approximately 20%, David also used our weight loss calculator to set realistic goals for the next five years.
Tubulovillous adenomas (10-15% of adenomas):
- Mixed architectural features combining tubular and villous patterns
- Intermediate malignancy risk (15-20% if >1cm)
- More likely to recur after removal compared to purely tubular types
- May require more frequent surveillance (3-5 years)
Villous adenomas (5-10% of adenomas):
- Finger-like projections giving velvety appearance
- Highest malignancy risk among adenoma subtypes (40% if >2cm)
- More difficult to achieve complete removal
- Often require 3-year surveillance intervals even when completely excised
Sessile Serrated Lesions (10-15% of all polyps)
Previously called “sessile serrated adenomas” or “sessile serrated polyps,” these flat lesions predominantly occur in the right colon and can be challenging to detect even for experienced colonoscopists.
- Location: Typically right colon (cecum, ascending colon, transverse colon)
- Appearance: Flat or slightly raised, pale, covered with mucus, hard to visualize
- Cancer risk: Can develop into cancer through alternate pathway (BRAF mutation)
- Growth rate: May progress to cancer faster than traditional adenomas (3-5 years vs 10-15 years)
The National Cancer Institute notes that up to 30% of colorectal cancers arise through the serrated pathway, making detection and removal of these lesions particularly important for cancer prevention.
Surveillance requirements for SSLs:
- Small (<10mm) SSL without dysplasia: 5-10 year interval
- Large (≥10mm) SSL or any SSL with dysplasia: 3-year interval
- Multiple SSLs: Consider genetic evaluation for serrated polyposis syndrome
Traditional Serrated Adenomas (Rare: <1% of polyps)
These uncommon polyps combine serrated architecture with dysplasia, creating a lesion with malignant potential similar to conventional adenomas.
- Appearance: Often pedunculated (on a stalk) in the left colon
- Cancer risk: High malignancy potential, especially when >1cm
- Follow-up: Treat as advanced adenoma with 3-year surveillance
Pathology Report Decoder: Real Examples
Understanding the exact language in your pathology report transforms confusing medical terminology into actionable information about your health.
Example 1: Low-Risk Finding
PATHOLOGY REPORT:
Specimen A (ascending colon, 7mm):
Histology: Tubular adenoma with low-grade dysplasia
Margins: Negative for dysplasia
Translation: Your doctor found and completely removed a small precancerous polyp from the right side of your colon. The cells showed early changes (low-grade dysplasia) but nothing concerning, and the edges of the removed tissue were clear, confirming complete excision. Similar to our guide on endoscopy results, understanding your specific findings helps you know exactly what actions follow.
Your risk: Very low. The polyp was caught early and fully removed.
Next steps: Return for colonoscopy in 5-7 years depending on whether this was your only polyp.
Example 2: Moderate-Risk Finding
PATHOLOGY REPORT:
Specimen B (transverse colon, 12mm):
Histology: Tubulovillous adenoma with high-grade dysplasia
Margins: Cannot be assessed (piecemeal resection)
Translation: Your doctor found a larger polyp (>1cm) with more advanced precancerous changes (high-grade dysplasia) that had to be removed in pieces rather than all at once. The villous component and high-grade dysplasia increase concern, and piecemeal removal means there’s a small chance some polyp tissue remains.
Your risk: Moderate. While not cancer, this represents more advanced precancerous change.
Next steps:
- Short-interval colonoscopy in 6-12 months to check for residual polyp tissue
- If clear at follow-up, then 3-year surveillance intervals
- Consider genetic risk assessment using our genetic risk assessment tool if you have family history of colorectal cancer
Example 3: Requires Immediate Action
PATHOLOGY REPORT:
Specimen C (sigmoid colon, 22mm):
Histology: Adenocarcinoma arising in tubulovillous adenoma, moderately differentiated
Invasion: Limited to submucosa (pT1)
Margins: Positive at deep margin
Translation: Your polyp contained early-stage cancer that has grown into the second layer of the colon wall. Because the bottom margin of the removed tissue showed cancer cells, complete removal wasn’t achieved through colonoscopy alone.
Your risk: You have early colorectal cancer requiring additional treatment.
Next steps:
- Surgical consultation within 2 weeks for partial colon resection
- CT scans to evaluate for metastasis (cancer spread)
- Oncology referral for staging and treatment planning
- Expected 5-year survival rate exceeds 90% for pT1 lesions with appropriate treatment
| Polyp Type | Cancer Risk Over 10 Years | Surveillance Interval | Key Features |
|---|---|---|---|
| Small hyperplastic (<10mm, rectosigmoid) | <1% | 10 years | Benign, no concern |
| Tubular adenoma <10mm (1-2 polyps) | 3-5% | 5-7 years | Low-grade dysplasia |
| Tubular adenoma ≥10mm OR 3-10 adenomas | 8-12% | 3 years | Increased number or size |
| Villous adenoma or HGD | 15-30% | 3 years (check in 6-12 months first) | Advanced features |
| Sessile serrated lesion ≥10mm | 10-15% | 3 years | Right colon, flat |
| ≥10 adenomas | 25-40% | 1 year + genetic testing | Possible polyposis syndrome |
What Happens During Polyp Removal
Understanding the technical aspects of polypectomy helps you interpret terms like “piecemeal resection” and “thermal injury” that may appear in your colonoscopy result.
Snare polypectomy involves looping a wire around the polyp base, applying electrical current to cut and cauterize simultaneously. This technique works well for pedunculated (stalked) polyps and smaller sessile polyps.
Endoscopic mucosal resection (EMR) lifts larger flat polyps by injecting saline beneath them, then removes them with a snare. Polyps >2cm often require piecemeal (multiple pieces) removal, which carries 10-20% recurrence risk requiring surveillance colonoscopy at 6-12 months.
Cold snare technique removes small polyps without electrical current, reducing perforation and bleeding risks. The American College of Gastroenterology now recommends cold snare for polyps ≤10mm when feasible.
Tattooing involves injecting sterile India ink near large polyp sites, creating a permanent blue-black mark visible during future colonoscopies or surgery. If your report mentions “site tattooed,” this guides surgeons to the exact location if cancer is found or helps locate the area during surveillance exams.
Beyond Polyps: Other Abnormal Findings
Your colonoscopy result may reveal conditions besides polyps that explain symptoms or require monitoring.
Diverticulosis (Present in 50-70% of adults over age 60)
Small pouches bulging through weak spots in the colon wall appear as grape-like outpouchings during colonoscopy. Most people with diverticulosis have zero symptoms and require no treatment.
- Location: Usually sigmoid colon (lower left abdomen)
- Significance: Benign unless they bleed or become infected (diverticulitis)
- Follow-up: No change to surveillance intervals unless complications occur
- Lifestyle: Adequate fiber intake (25-30g daily) may reduce diverticulitis risk
Inflammatory Bowel Disease Markers
Colonoscopy findings suggesting Crohn’s disease or ulcerative colitis include continuous inflammation, loss of normal vascular pattern, friability (bleeds easily when touched), and ulceration.
- Ulcerative colitis: Continuous inflammation starting at rectum, extending proximally
- Crohn’s disease: Patchy (“skip”) lesions anywhere in GI tract, cobblestone appearance
- Diagnostic approach: Multiple biopsies from affected and normal areas
- Next steps: Gastroenterology follow-up, possible additional imaging, medication initiation
Vascular Lesions and Bleeding Sources
Arteriovenous malformations (AVMs or angioectasias) appear as small red spots on the colon lining and can cause chronic blood loss leading to anemia.
- Appearance: Cherry-red, spider-like vessels in the right colon
- Treatment: Often cauterized during colonoscopy
- Follow-up: Monitor for recurrence if causing significant anemia
- Association: More common in patients with chronic kidney disease or aortic stenosis
Strictures and Narrowing
Tight segments preventing colonoscope passage may result from previous surgery, chronic inflammation, radiation therapy, or tumor growth.
- Diagnostic challenge: Cannot examine beyond stricture
- Next steps: CT colonography or barium enema to evaluate proximal colon
- Treatment: Endoscopic dilation for benign strictures, surgery for malignant causes
- Red flag: New stricture without known cause requires exclusion of cancer
Research published by Johns Hopkins Medicine demonstrates that early detection through colonoscopy reduces colorectal cancer mortality by 68%, with most of this benefit coming from polyp removal during the procedure.
Follow-Up Protocols & Next Steps
What to Do After Receiving Your Colonoscopy Results
The actions you take in the 48 hours after receiving your colonoscopy result significantly impact long-term outcomes, especially when abnormalities require additional evaluation or treatment.
Surveillance Colonoscopy Decision Tree
Your next colonoscopy timing depends on specific findings documented in your pathology report. The 2026 American Gastroenterological Association guidelines provide evidence-based intervals that balance cancer prevention with minimizing unnecessary procedures.
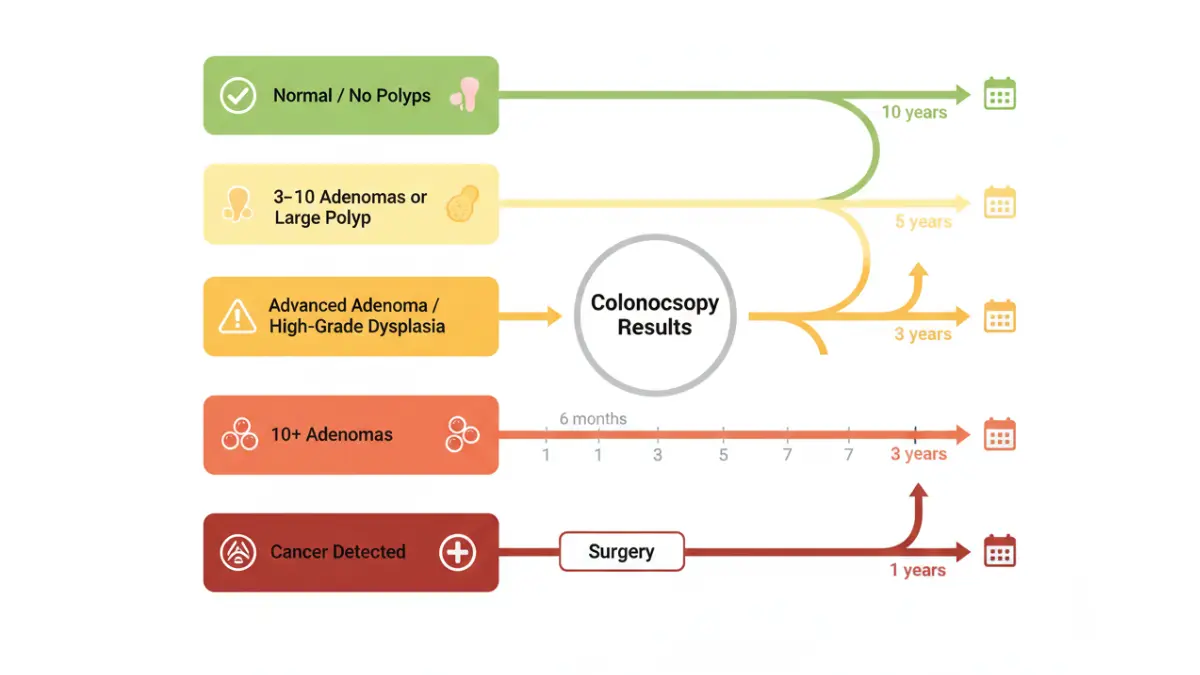
IF YOU HAD ZERO POLYPS: → Average risk: Return in 10 years → Family history (parent/sibling with CRC before age 60): Return in 5 years → Poor bowel prep: Return in 1 year → Incomplete exam: Return in 1 year
IF YOU HAD 1-2 SMALL (<10mm) TUBULAR ADENOMAS: → Low-grade dysplasia: Return in 5-7 years → High-grade dysplasia in small polyp (rare): Return in 3 years → Positive family history: May shorten to 3 years
IF YOU HAD 3-10 ADENOMAS, ANY ≥10mm, OR VILLOUS FEATURES: → Standard recommendation: Return in 3 years → If ≥10 total adenomas: Return in 1 year + genetic counseling → Piecemeal removal of large polyp: Return in 6 months to check site, then 3 years
IF YOU HAD SESSILE SERRATED LESION: → Small (<10mm) without dysplasia: Return in 5-10 years → Large (≥10mm) or with dysplasia: Return in 3 years → Multiple SSLs: Consider serrated polyposis syndrome evaluation
IF CANCER WAS DETECTED: → Surgical consultation within 1-2 weeks → Staging CT scans ordered → Post-surgical surveillance colonoscopy at 1 year
Lisa Patterson, a 67-year-old from Florida, received a colonoscopy result showing 4 small tubular adenomas, all completely removed with low-grade dysplasia. Her gastroenterologist scheduled her next colonoscopy in 3 years. Understanding that maintaining healthy BMI reduces adenoma recurrence by up to 25% according to Harvard T.H. Chan School of Public Health research, Lisa committed to lifestyle changes during her 3-year surveillance window.
| Colonoscopy Finding | Next Colonoscopy Timing | Additional Actions |
|---|---|---|
| Normal exam, adequate prep | 10 years | Maintain healthy lifestyle, monitor symptoms |
| 1-2 small tubular adenomas | 5-7 years | Consider aspirin if cardiovascular indications |
| 3-10 adenomas or any ≥10mm | 3 years | Evaluate family history, lifestyle counseling |
| >10 adenomas | 1 year | Genetic testing for polyposis syndromes |
| Sessile serrated lesion ≥10mm | 3 years | Consider testing for BRAF mutations |
| Piecemeal removal of large polyp | 6 months, then 3 years | Verify complete resection before standard surveillance |
| High-grade dysplasia in polyp | 3 years (some recommend 6-month check first) | Ensure complete removal documented |
| Cancer detected | Post-surgery surveillance at 1 year | Surgical resection, staging, oncology follow-up |
When Genetic Testing Is Recommended
Certain colonoscopy result patterns trigger evaluation for hereditary colorectal cancer syndromes, which require specialized surveillance and management.
Lynch syndrome (hereditary nonpolyposis colorectal cancer) indicators:
- Colorectal cancer diagnosed before age 50
- Multiple family members with Lynch-associated cancers (colorectal, endometrial, ovarian, gastric)
- Tumor testing showing microsatellite instability (MSI-high) or mismatch repair deficiency
Familial adenomatous polyposis (FAP) indicators:
- ≥10 cumulative adenomas (or >100 for classic FAP)
- Family history of FAP or attenuated FAP
- Onset of multiple adenomas in teens or twenties
Serrated polyposis syndrome criteria:
- ≥5 serrated lesions proximal to sigmoid, with ≥2 being ≥10mm
- 20 serrated lesions throughout colon
- First-degree relative with serrated polyposis syndrome
The National Comprehensive Cancer Network recommends genetic counseling and testing for anyone meeting these criteria. Identifying hereditary syndromes allows for:
- Intensified colonoscopy surveillance (often annual)
- Screening of at-risk family members
- Consideration of risk-reducing medications or surgery
- Screening for extracolonic cancers in certain syndromes
Our genetic risk assessment tool helps you evaluate whether your personal and family history warrants discussion with a genetics specialist.
Insurance coverage: The Affordable Care Act requires most insurance plans to cover genetic counseling and testing for individuals meeting medical criteria without cost-sharing. Medicare also covers these services when medically indicated.
Lifestyle Modifications That Matter
Evidence-based lifestyle changes reduce both adenoma recurrence and colorectal cancer incidence, making the years between surveillance colonoscopies valuable for prevention.
Dietary modifications with strongest evidence:
- Increase fiber intake to 25-30g daily: Associated with 10-20% reduction in adenoma recurrence
- Limit red meat to <500g per week: Processed meat shows strongest cancer association
- Increase calcium intake to 1,200mg daily: Calcium supplementation reduced adenoma recurrence by 15% in randomized trials
- Maintain vitamin D levels >30 ng/mL: Low vitamin D correlates with increased colorectal cancer risk
Physical activity recommendations:
- ≥150 minutes moderate-intensity exercise weekly: Associated with 20-25% lower colorectal cancer risk
- Avoid prolonged sedentary time: Even with exercise, sitting >6 hours daily increases risk
- Maintain healthy body weight: Each 5-point BMI increase above 25 raises colorectal cancer risk 5-10%
Studies from the American Institute for Cancer Research demonstrate that individuals following comprehensive lifestyle recommendations experience up to 45% lower colorectal cancer incidence compared to those with multiple risk factors.
Robert Kim, a 55-year-old executive from Illinois with a colonoscopy result showing multiple adenomas, implemented systematic changes using our calorie deficit calculator to lose 30 pounds over 6 months. He also utilized our protein intake calculator to ensure adequate nutrition during weight loss, an approach supported by research showing improved adenoma outcomes with sustained weight management.
Aspirin and NSAIDs (2026 update): Research consistently shows regular aspirin use (81-325mg daily) reduces adenoma recurrence by 15-20% and colorectal cancer incidence by approximately 30%. However, the U.S. Preventive Services Task Force recommends aspirin primarily for cardiovascular disease prevention, with colorectal cancer risk reduction as a beneficial side effect.
Who should consider aspirin:
- Age 50-59 with ≥10% 10-year cardiovascular disease risk
- Previous adenomas, especially if multiple or advanced
- No increased bleeding risk
- Willing to take daily aspirin for ≥10 years
Tobacco and alcohol:
- Smoking cessation: Reduces colorectal cancer risk 20-40% within 10 years of quitting
- Alcohol limitation: ≤1 drink daily for women, ≤2 for men; heavy drinking (≥3 drinks daily) increases risk 50%
What This Means For You:
- Schedule your follow-up colonoscopy before leaving your gastroenterologist’s office
- If multiple adenomas were found, request referral to registered dietitian for personalized nutrition counseling
- Document your results and pathology reports in a personal health file for future reference
- Discuss aspirin therapy with your primary care physician if you have cardiovascular risk factors
- Share your colonoscopy result with first-degree relatives, especially if advanced adenomas or multiple polyps were found
Cost, Insurance & Practical Considerations
Financial and Logistical Aspects of Colonoscopy Results
Understanding the financial implications of your colonoscopy result helps you anticipate costs and navigate insurance coverage, particularly when findings trigger additional procedures or surveillance.
Insurance Coverage for Pathology Testing
The distinction between “screening” and “diagnostic” colonoscopy profoundly affects your out-of-pocket costs, often creating confusion when polyps are discovered during what began as a screening procedure.
Screening colonoscopy coverage (no polyps found):
- Preventive service: $0 copay, $0 coinsurance, $0 deductible under ACA
- Medicare: Fully covered every 10 years for average risk
- Private insurance: Mandated coverage without cost-sharing
- Includes: Procedure, anesthesia, facility fees, pathologist professional fees (if biopsies taken)
What changes when polyps are removed:
The moment your gastroenterologist removes a polyp, some insurers reclassify the procedure from “screening” to “diagnostic,” potentially triggering:
- Deductibles (typically $500-$5,000 depending on plan)
- Coinsurance (usually 10-30% of allowed amounts)
- Copayments ($50-$500 for specialist procedures)
However, 2021 federal regulations and many state laws now require insurers to maintain screening status even when polyps are removed during the same procedure. Unfortunately, enforcement and compliance vary significantly by insurer and state.
Typical pathology costs when cost-sharing applies:
- Single polyp pathology: $150-$400 (laboratory facility fee + pathologist interpretation)
- Multiple polyp specimens: $300-$800 (each polyp examined separately)
- Immunohistochemistry studies: $200-$600 additional (special stains for certain diagnoses)
- Molecular testing (MSI, BRAF): $800-$2,500 (for cancer or serrated polyps requiring genetic evaluation)
According to Medicare.gov, Medicare beneficiaries face no cost-sharing for screening colonoscopy even when polyps are removed, setting the standard many commercial insurers now follow.
Appeal strategies if incorrectly billed:
- Request documentation showing procedure began as screening with appropriate diagnosis codes (Z12.11)
- Cite federal and state laws requiring full coverage of screening colonoscopy including polypectomy
- Obtain letter from gastroenterologist confirming screening indication
- File formal appeal citing ACA Section 2713 preventive services requirements
- Contact state insurance commissioner if insurer denies legitimate screening claim
James Wilson, a 51-year-old from North Carolina, received a $1,200 bill after his screening colonoscopy revealed and removed two small adenomas. After his gastroenterologist provided documentation that the procedure was scheduled and performed as preventive screening, his insurer reversed the charges and covered the full amount, including pathology fees, without cost-sharing.
Second Opinions and Report Accuracy
Pathology interpretation involves subjective assessment, particularly for distinguishing polyp types and dysplasia grades. Inter-observer variability (disagreement between pathologists) occurs in 10-20% of cases, especially for:
- Distinguishing hyperplastic polyps from sessile serrated lesions
- Grading dysplasia (low-grade vs high-grade)
- Determining presence of invasive cancer in large polyps
When to consider pathology second opinion:
- High-grade dysplasia diagnosis (affects surveillance interval significantly)
- Cancer detected in polyp specimen
- Discrepancy between visual appearance and pathology diagnosis
- Unusual or rare polyp type diagnosed
- Treatment decisions hinge on pathology interpretation
How to obtain slide review:
- Request copies of pathology slides from original laboratory (nominal fee usually $25-$100)
- Send slides to academic medical center pathology department for expert review
- Expect 1-2 weeks for comprehensive re-evaluation
- Cost typically $300-$800 for expert consultation
Top pathology centers for GI second opinions:
- Johns Hopkins Hospital (Baltimore, MD)
- Cleveland Clinic (Cleveland, OH)
- Mayo Clinic (Rochester, MN; Scottsdale, AZ; Jacksonville, FL)
Most pathology second opinions confirm the original diagnosis, providing reassurance. In the 15-20% of cases with diagnostic changes, these revisions can meaningfully alter surveillance intervals or treatment recommendations, making second opinions valuable for significant findings.
What to Do in the Next 24-48 Hours
Taking organized action immediately after receiving your colonoscopy result ensures you understand findings, follow appropriate next steps, and maintain documentation for future reference.
Immediate action checklist:
Within 24 hours:
- Review your complete pathology report, not just the summary
- Write down questions while information is fresh
- Call your doctor’s office if anything is unclear or concerning
- Take photos of your report for easy mobile access
- Share results with your primary care physician
Within 48 hours:
- Schedule your next colonoscopy if interval is ≤5 years
- If cancer was detected, expect call from surgeon or oncologist within 2-3 business days
- Review colonoscopy images if available through patient portal
- Document in personal health record with date and findings
- Inform first-degree relatives if you had multiple or advanced adenomas
Questions to ask your gastroenterologist:
For polyp findings:
- “Were all polyps completely removed (R0 resection)?”
- “What’s the exact size and location of each polyp?”
- “Do my results suggest I should see a genetic counselor?”
- “Should I modify my diet or lifestyle based on these findings?”
- “Do I need any additional testing or imaging?”
For cancer diagnosis:
- “What stage is the cancer based on initial pathology?”
- “Which surgeon or oncologist do you recommend?”
- “What’s the expected timeline from diagnosis to treatment?”
- “What are my treatment options and expected outcomes?”
- “Can you explain what happens next in simple terms?”
Document organization tips:
- Create digital folder with all colonoscopy reports, pathology results, and images
- Note medication adjustments (especially if you stopped blood thinners for procedure)
- Track any post-procedure symptoms or concerns
- Maintain list of questions that arise between appointments
- Set calendar reminders for surveillance colonoscopy 6-12 months before due date
For ongoing health management and monitoring between colonoscopies, explore our comprehensive health tips section, which includes evidence-based guidance on digestive health, cancer prevention, and wellness strategies that complement your surveillance plan. Similar resources about understanding other diagnostic results, like our guide on CT scan abnormalities, can help you navigate additional testing if recommended.
What This Means For You: Your colonoscopy result provides a detailed roadmap for colorectal cancer prevention. Normal results offer reassurance for the next decade, while polyp findings enable removal of precancerous growths before they transform into cancer. By understanding your specific pathology, following evidence-based surveillance intervals, and implementing lifestyle modifications, you dramatically reduce your risk of developing colorectal cancer—one of the most preventable malignancies through screening.
Frequently Asked Questions about Colonoscopy
1. How long after a colonoscopy do you get biopsy results?
Most pathology results return within 5-10 business days after your colonoscopy. The timing depends on your laboratory’s workload and whether special stains or molecular testing is needed. If your gastroenterologist suspects cancer based on visual appearance, pathology departments typically expedite processing, with results available in 2-3 days. You’ll receive normal or routine findings through your patient portal or mail, while abnormal results usually trigger a phone call from your doctor’s office.
2. What percentage of colonoscopy polyps are cancerous?
Approximately 3-5% of polyps removed during colonoscopy contain cancer or high-grade dysplasia (advanced precancerous cells). The vast majority of polyps are benign adenomas or hyperplastic polyps. Even advanced adenomas with high-grade dysplasia aren’t technically cancer but represent the last step before malignant transformation. Your specific cancer risk depends on polyp size (larger polyps carry higher risk), histology (villous features increase concern), and degree of dysplasia present.
3. Can colonoscopy results be wrong?
While colonoscopy is highly accurate, errors can occur. The polyp miss rate ranges from 6-27% depending on colonoscopist skill, bowel preparation quality, and polyp characteristics. Flat sessile serrated lesions in the right colon are most commonly missed. Pathology interpretation also has 10-20% inter-observer variability, particularly for distinguishing polyp subtypes and dysplasia grades. This is why colonoscopy quality metrics (adenoma detection rate, withdrawal time, cecal intubation rate) matter and why second opinions have value for significant findings.
4. What does high-grade dysplasia mean in colonoscopy results?
High-grade dysplasia indicates that cells within your polyp show advanced precancerous changes, appearing significantly abnormal under the microscope but haven’t yet invaded through the basement membrane (which would make them cancer). Think of it as the final step before cancer develops. Polyps with high-grade dysplasia require complete removal and typically trigger 3-year surveillance intervals rather than the 5-10 year intervals for low-grade dysplasia. If high-grade dysplasia wasn’t completely removed, you may need repeat colonoscopy in 6-12 months to verify no residual abnormal tissue remains.
5. Should I be worried if polyps were found during colonoscopy?
Finding polyps during colonoscopy is actually good news—your screening caught precancerous growths before they became cancer. Approximately 25-30% of colonoscopies detect polyps, and the vast majority are benign or early precancerous stages. Most importantly, polyp removal during colonoscopy reduces your colorectal cancer risk by 76-90% compared to never having screening. Your specific follow-up interval depends on polyp number, size, and type, but finding and removing polyps represents screening working exactly as intended for cancer prevention.
6. How often should I have a colonoscopy if adenomas were found?
Surveillance intervals depend on adenoma characteristics. For 1-2 small (<10mm) tubular adenomas with low-grade dysplasia, return in 5-7 years. If you had 3-10 adenomas, any adenoma ≥10mm, or adenomas with villous features or high-grade dysplasia, return in 3 years. Ten or more adenomas requires 1-year follow-up plus genetic testing for polyposis syndromes. Your gastroenterologist considers your family history, overall health, and life expectancy when personalizing these recommendations based on 2026 guidelines from the American Gastroenterological Association.
7. What’s the difference between a screening and diagnostic colonoscopy for billing?
A screening colonoscopy is performed on asymptomatic individuals at appropriate intervals for cancer prevention and must be covered without cost-sharing under the Affordable Care Act. A diagnostic colonoscopy investigates specific symptoms (bleeding, pain, diarrhea) or follows up known abnormalities, and may involve deductibles and coinsurance. Confusion arises when polyps are removed during screening procedures—federal regulations require insurers to maintain screening status and full coverage even when polypectomy occurs, but enforcement varies by insurer. Always verify your plan’s specific policy and appeal if incorrectly billed.
8. Can I eat normally after receiving colonoscopy results?
Once you’ve recovered from your procedure (usually 24 hours), you can resume your normal diet regardless of findings. If polyps were removed, some gastroenterologists recommend avoiding NSAIDs like ibuprofen for 1-2 weeks to reduce bleeding risk at polypectomy sites, though this varies by practice. If you had large polyps removed or multiple polypectomies, your doctor may advise avoiding nuts, seeds, popcorn, or rough fiber for several days. Long-term dietary modifications—increasing fiber, reducing red and processed meat—help prevent future polyps but don’t require immediate implementation.
9. Do I need genetic testing if multiple polyps were found?
Genetic testing becomes important when you have ≥10 cumulative adenomas, multiple sessile serrated lesions meeting serrated polyposis syndrome criteria, or colorectal cancer diagnosed before age 50. These patterns suggest possible hereditary syndromes like Lynch syndrome, familial adenomatous polyposis, or serrated polyposis syndrome. Identifying these conditions changes management significantly—often requiring annual colonoscopy, screening for extracolonic cancers, and testing of at-risk family members. Discuss genetic counseling with your gastroenterologist if you have multiple polyps, especially if your family history includes early-onset colorectal cancer.
10. What happens if cancer is found during colonoscopy?
If your pathology report confirms cancer, expect a phone call from your gastroenterologist within 2-3 days to discuss findings and next steps. You’ll receive referrals to colorectal surgeon and medical oncologist, usually with appointments scheduled within 1-2 weeks. Staging workup includes CT scans of chest, abdomen, and pelvis to evaluate cancer spread, plus blood tests including CEA tumor marker. Treatment typically involves surgical resection (partial colon removal), followed by chemotherapy if cancer has spread to lymph nodes or beyond. Early-stage colorectal cancer (confined to colon wall) has excellent prognosis with 5-year survival rates exceeding 90%.
11. How accurate are colonoscopy findings?
Colonoscopy accuracy depends on multiple quality factors. High-quality colonoscopies with excellent bowel preparation, complete cecal intubation, and adequate withdrawal time (≥6-7 minutes) detect approximately 95% of polyps ≥10mm and 75-90% of smaller polyps. However, colonoscopy quality varies significantly between providers—gastroenterologists with high adenoma detection rates (≥30% for men, ≥20% for women) find substantially more polyps than lower-performing colleagues. This variability is why professional societies track quality metrics. To maximize accuracy, ensure your colonoscopy is performed by board-certified gastroenterologist at accredited facility with adequate bowel preparation.
12. Can stress affect colonoscopy results?
Stress and anxiety don’t directly change what your gastroenterologist finds during colonoscopy—polyps, cancer, and structural abnormalities exist independently of your emotional state. However, severe anxiety can indirectly affect results through two mechanisms. First, stress may cause poor bowel preparation compliance (not drinking all the prep solution), leading to inadequate visualization and higher polyp miss rates. Second, stress and anxiety commonly cause functional GI symptoms like abdominal pain and altered bowel habits, which is why colonoscopy is often performed—but the exam typically finds no structural explanation for these functional disorders.
13. What if I disagree with my colonoscopy results?
If your colonoscopy result doesn’t align with your symptoms or expectations, several options exist. First, request thorough discussion with your gastroenterologist about findings and their implications—sometimes confusion stems from miscommunication rather than incorrect results. For pathology concerns, obtain second opinion from expert GI pathologist at academic medical center, which changes diagnosis in 15-20% of complex cases. If symptoms persist despite normal colonoscopy, consider additional testing like CT enterography (evaluates small bowel), capsule endoscopy, or referral to specialized motility center for functional disorders. Document your concerns and symptoms carefully to guide further evaluation.
14. Are colonoscopy findings the same everywhere in the world?
Colorectal polyp and cancer prevalence varies significantly by geography. Highest rates occur in North America, Western Europe, Australia, and New Zealand, while rates remain lower (though rising) in Asia, Africa, and South America. These differences reflect dietary patterns, genetic factors, and screening availability. However, pathology classifications and surveillance guidelines are largely standardized internationally—adenomas and sessile serrated lesions are diagnosed using similar criteria worldwide. The major difference lies in healthcare system structure and screening recommendations, with some countries beginning average-risk screening at age 50 rather than 45.
15. How do I prepare for my follow-up colonoscopy appointment?
When scheduling your surveillance colonoscopy, verify your previous pathology reports are available to your gastroenterologist—this determines appropriate timing. Update your current medication list, especially blood thinners, which may require temporary discontinuation. Document any new GI symptoms or family history changes since your last procedure. Schedule the colonoscopy before your recommended interval expires, as delays beyond surveillance intervals reduce cancer prevention effectiveness. Most importantly, plan logistics ahead—arrange ride home, clear schedule for prep day and procedure day, and obtain prep supplies early to avoid last-minute stress that can interfere with adequate bowel cleansing.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Colonoscopy results should always be interpreted by your healthcare provider in the context of your individual medical history, symptoms, family history, and overall health status. If you have concerns about your colonoscopy findings or require guidance on surveillance intervals, consult your gastroenterologist or primary care physician. The information presented reflects current evidence and 2026 guidelines but cannot replace personalized medical evaluation and treatment planning.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.