On This Page – Quick Medical Summary
When Marcus Thompson stepped on the scale at 347 pounds in March 2025, his doctor delivered a stark warning: bariatric surgery or face diabetes complications within two years. Eighteen months after his gastric sleeve procedure, Marcus has lost 187 pounds and reversed his pre-diabetes completely.
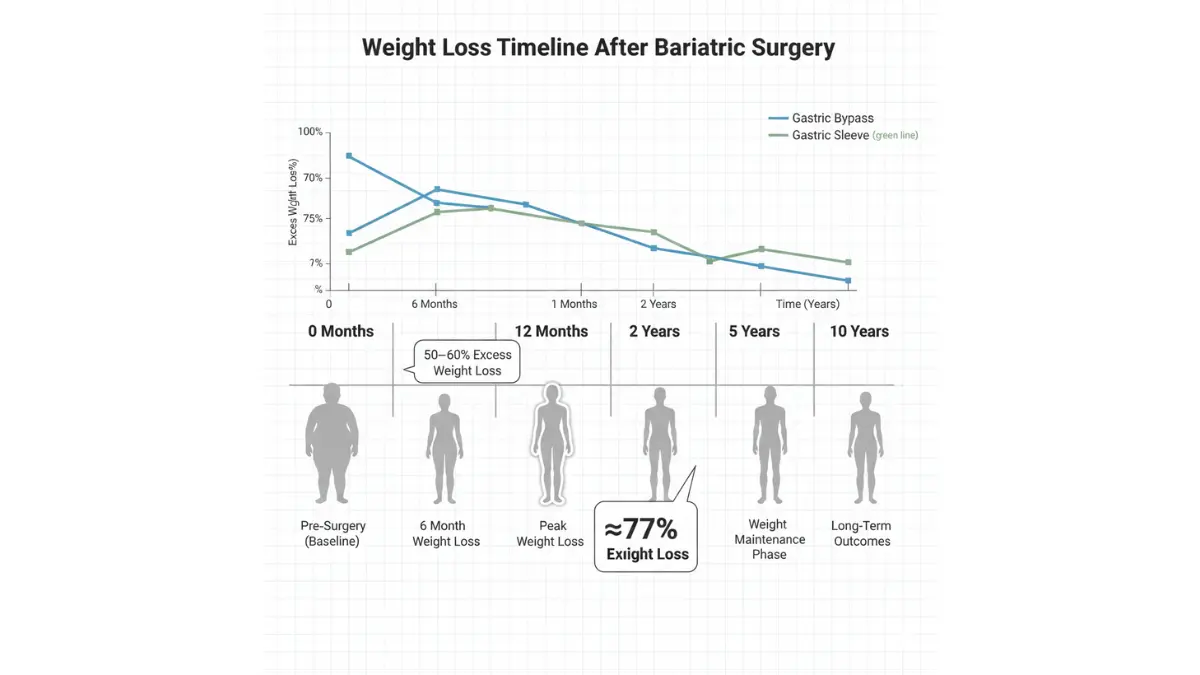
Bariatric surgery is the most effective long-term obesity treatment, with patients achieving 77% excess weight loss within 12 months according to 2025 ASMBS clinical data. This metabolic surgery permanently alters your digestive system to restrict food intake and reduce nutrient absorption, delivering sustained weight reduction that diet and exercise alone cannot match.
The three primary weight loss surgery procedures in 2026 are:
- Gastric sleeve (sleeve gastrectomy): Removes 80% of stomach
- Gastric bypass (Roux-en-Y): Creates small stomach pouch, reroutes intestines
- Gastric band: Places adjustable band around upper stomach
Average costs range from $15,000 to $35,000 depending on procedure type, geographic location, and insurance coverage. Modern robotic-assisted techniques using systems like da Vinci and Stanford’s new MARS robot have reduced complication rates to just 4%, with mortality risk at 0.1%—safer than appendectomy or knee replacement.
Calculating your current BMI is the critical first step in determining surgical eligibility. Bariatric surgery requirements typically include BMI ≥40, or BMI ≥35 with obesity-related conditions like type 2 diabetes or hypertension.
This guide covers 2026’s latest bariatric surgery cost breakdowns, success rate data, procedure comparisons, insurance navigation, and the emerging GLP-1 medication alternative (Ozempic, Wegovy) that’s changing the decision-making landscape.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Consult a board-certified bariatric surgeon for personalized treatment recommendations.
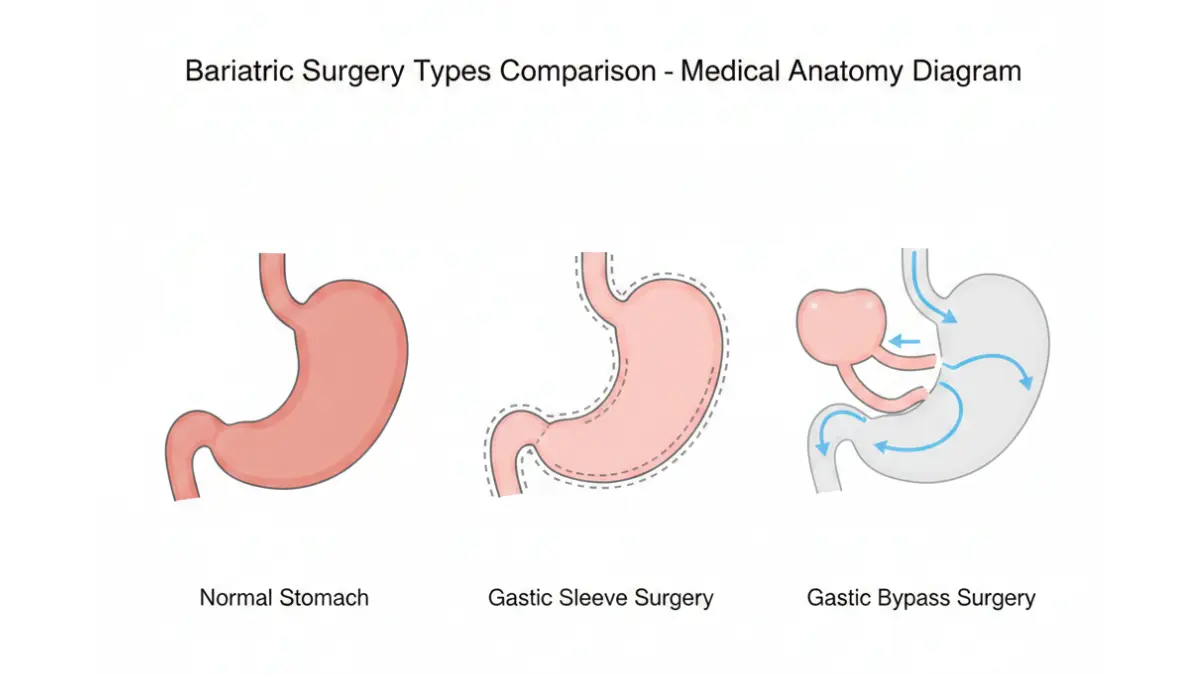
Types & Comparison
2026 Bariatric Surgery Types: Which Delivers Best Results?
Laparoscopic surgery techniques have revolutionized bariatric procedures, replacing open surgery with minimally invasive approaches that accelerate recovery and minimize scarring. Understanding each metabolic surgery option helps you make informed decisions with your surgeon.
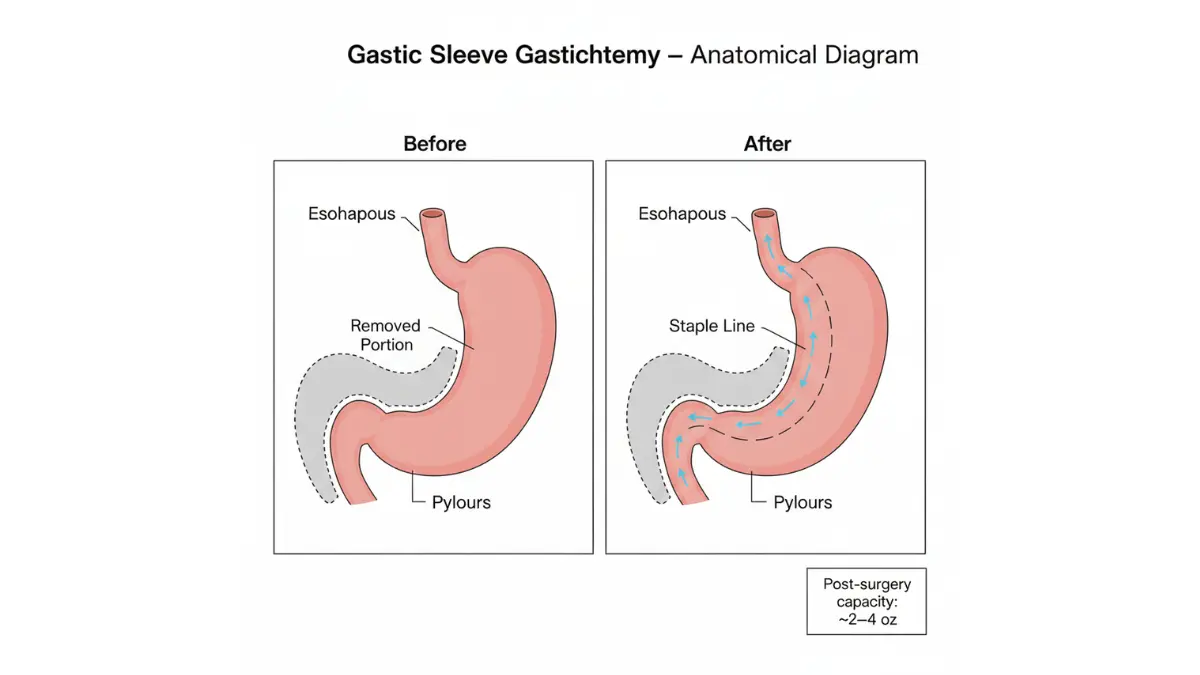
Gastric Sleeve Surgery (Most Popular 2026)
Sleeve gastrectomy dominates the field, accounting for 63% of all bariatric procedures nationwide. Surgeons remove approximately 80% of your stomach, creating a banana-shaped tube that holds just 2-4 ounces.
Key advantages:
- No intestinal rerouting (preserves normal digestion)
- 60-70% excess weight loss at 12 months
- Shorter operating time (60-90 minutes)
- Lower vitamin deficiency risk vs bypass
- Irreversible but highly effective
The laparoscopic approach requires just 4-5 small incisions. Patients typically discharge within 48 hours and return to desk work in 2-3 weeks.
Gastric Bypass (Roux-en-Y): Gold Standard
Gastric bypass remains the “gold standard” for maximum excess weight loss, delivering 70-80% reduction within 18 months. The procedure creates an egg-sized stomach pouch, then connects it directly to the middle small intestine, bypassing the remaining stomach and upper intestine.
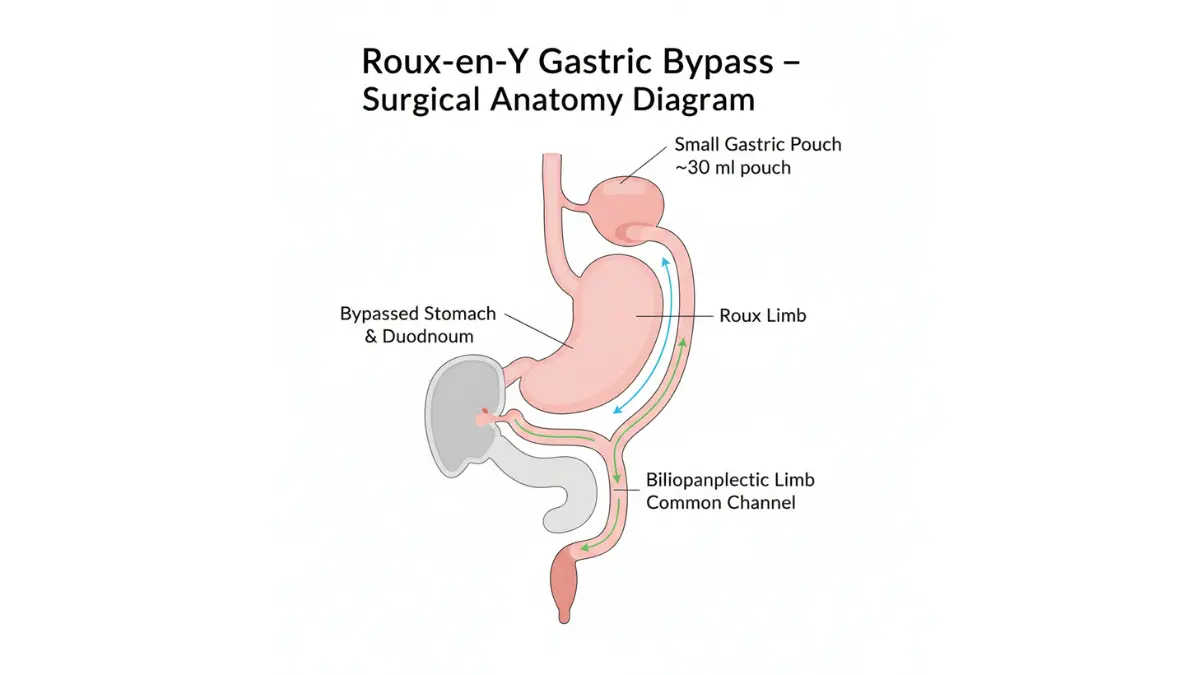
Why surgeons recommend bypass:
- Highest diabetes remission rate (80% at 2 years)
- Superior long-term weight maintenance
- Effective for severe obesity (BMI >50)
- Reduces acid reflux significantly
Trade-offs include:
- Lifelong vitamin supplementation required
- Higher surgical complexity
- Dumping syndrome risk (10-15% of patients)
- Longer recovery vs sleeve
This Roux-en-Y procedure works through both restriction and malabsorption, making it particularly effective for metabolic syndrome reversal.
Gastric Band: Declining Use
Adjustable gastric banding places a silicone ring around the upper stomach, creating a small pouch. While reversible and low-risk, bariatric surgery specialists now rarely recommend banding due to:
- Lower weight loss (40-50% excess weight)
- High revision surgery rates (40% within 10 years)
- Frequent band slippage or erosion
- Slower results vs modern alternatives
NEW: Robotic-Assisted & Magnetic Procedures
2026 brings surgical innovations that further reduce complications:
Da Vinci Robotic System: Enhanced 3D visualization and precision have cut leak rates by 35% compared to traditional laparoscopy.
Stanford MARS Robot: Uses magnetic surgical instruments, reducing incisions from 5 to just 2-3 entry points while improving cosmetic outcomes.
These advanced technologies are now available at ASMBS-accredited centers nationwide, though they may increase surgical costs by $3,000-$5,000.
| Procedure | Weight Loss (12mo) | Operating Time | Hospital Stay | Cost Range |
|---|---|---|---|---|
| Gastric Sleeve | 60-70% | 60-90 min | 1-2 days | $15K-$23K |
| Gastric Bypass | 70-80% | 120-180 min | 2-3 days | $20K-$35K |
| Gastric Band | 40-50% | 30-60 min | Same day | $14K-$18K |
Costs & Insurance
Bariatric Surgery Costs 2026: What You’ll Actually Pay
Bariatric surgery cost varies dramatically based on procedure type, geographic location, hospital facility fees, and whether you have insurance coverage. Here’s the financial reality patients face in 2026.
Average Costs by Procedure Type
According to National Institute of Diabetes and Digestive and Kidney Diseases data:
- Gastric sleeve: $15,000-$23,000
- Gastric bypass: $20,000-$35,000
- Gastric band: $14,000-$18,000
- Revision surgeries: $18,000-$30,000
These totals include surgeon fees ($3,000-$8,000), anesthesia ($1,500-$3,000), hospital facility charges ($8,000-$15,000), and pre-operative testing ($1,000-$2,000).
Geographic variations create significant price differences:
- Northeast/West Coast: 25-40% higher than national average
- Midwest/South: 15-30% below average
- Rural areas: Limited surgeon availability but competitive pricing
Insurance Coverage Requirements & Pre-Authorization
Most commercial insurance and Medicare cover bariatric surgery requirements when you meet these criteria:
Coverage checklist:
- ✅ BMI ≥40 (any circumstances)
- ✅ BMI ≥35 with comorbidities (diabetes, hypertension, sleep apnea)
- ✅ Documented 6-12 month weight loss attempt history
- ✅ Psychological evaluation clearance
- ✅ Nutritional counseling completion
- ✅ No active substance abuse
Pre-authorization timelines average 6-12 weeks. Understanding your current health metrics through tools like the Body Fat Calculator and BMR Calculator strengthens insurance applications.
Important: 78% of commercial plans cover bariatric procedures, but 15% impose mandatory 6-month supervised diet programs that delay surgery approval.
Real Patient Cost Examples
Case 1 – Jennifer (Portland, OR):
- Procedure: Gastric sleeve
- Insurance: Blue Cross (80/20 coverage)
- Total billed: $22,400
- Patient paid: $4,480 (deductible + coinsurance)
Case 2 – Robert (Dallas, TX):
- Procedure: Gastric bypass
- Insurance: Self-pay (no coverage)
- Negotiated cash price: $16,500
- Patient paid: $16,500 (payment plan: $458/month × 36 months)
Case 3 – Angela (Medicare, Miami, FL):
- Procedure: Gastric sleeve
- Insurance: Medicare Part A + B
- Total billed: $19,800
- Patient paid: $226 (Part B deductible only)
The Weight Loss Calculator helps project your expected results against surgical investment costs.
Tax deduction note: Bariatric surgery qualifies as deductible medical expense under IRS rules when medically necessary, potentially reducing after-tax costs by 22-37% depending on your bracket.
Success Rates & Outcomes
Bariatric Surgery Success Rates: 2026 Data & Long-Term Results
Bariatric surgery success rate data from multi-year clinical studies reveals outcomes far superior to non-surgical obesity treatment. Understanding realistic expectations helps patients prepare mentally and physically for transformation.
Weight Loss Timeline: What to Expect
According to ASMBS 2025 outcomes research:
Month 1-6: Rapid weight loss phase
- Average loss: 50-60% of excess body weight
- Gastric bypass leads: 3-5 lbs/week initially
- Gastric sleeve follows: 2-4 lbs/week
- Strict liquid then pureed diet phase
Month 6-12: Continued steady loss
- 77% excess weight loss achievement (ASMBS data)
- Weight loss stabilizes to 1-2 lbs/week
- Regular food reintroduction complete
- Most visible physical transformation occurs
Year 2-5: Maintenance phase
- 50-60% maintain excess weight loss long-term
- 20-30% regain 10-20% of lost weight
- Lifestyle habits determine sustainability
- Annual follow-up visits critical
Year 5-10: Long-term outcomes
- 50% excess weight loss maintained on average
- Better outcomes with continued nutritional support
- Regain more common without behavioral changes
Patricia Chen’s journey exemplifies typical results: at 5’4″ and 285 pounds (BMI 48.9), she underwent gastric sleeve in January 2024. By January 2026, she maintains 168 pounds—a 117-pound loss representing 71% excess weight reduction.
Diabetes & Comorbidity Resolution Rates
Metabolic surgery delivers dramatic health improvements beyond weight loss:
Type 2 Diabetes:
- 80% remission rate within 2 years post-surgery
- 30-50% sustained remission at 10 years
- Medication reduction in 95% of patients
- A1C improvements averaging 2.5-3.5 points
Hypertension:
- 60-70% complete resolution
- Blood pressure medication reduction in 80%
- Average systolic reduction: 25-35 mmHg
Sleep Apnea:
- 75-85% improvement or resolution
- CPAP elimination in 60% of patients
High Cholesterol:
- 70% normalization within 18 months
- LDL reductions of 25-40%
Long-Term Success: 5 & 10-Year Data
Long-term research published in JAMA Surgery demonstrates:
- 30-50% reduction in premature death risk
- Sustained weight maintenance in 50-70% of patients
- 9.3-year life expectancy increase for diabetic patients
- Cost-effectiveness within 2-4 years through reduced medication and complication costs
James Mitchell’s decade-long success story: gastric bypass at age 45 (starting weight 378 lbs) led to 210-pound weight maintenance for 10 years, complete diabetes remission, and elimination of 7 daily medications. His experience aligns with the Calorie Deficit Calculator projections for sustained metabolic changes.
Eligibility, Risks & Recovery
Am I a Candidate? Requirements, Risks & Recovery Guide
Bariatric surgery requirements have expanded in 2026, allowing more patients access to this life-saving treatment based on updated ASMBS/IFSO guidelines.
2026 Eligibility Requirements
Primary criteria:
- BMI ≥40: Recommended regardless of other conditions
- BMI ≥35: With one or more obesity-related comorbidity (diabetes, heart disease, sleep apnea, hypertension)
- BMI 30-34.9: Considered for patients with type 2 diabetes or metabolic syndrome who’ve failed medical management
Asian-population adjustments:
- BMI ≥27.5 qualifies for surgery consideration
- Lower thresholds reflect different obesity-related disease risk profiles
Additional requirements:
- Age 18-65 (exceptions for adolescents and older adults)
- Failed supervised weight loss attempts (6-12 months documented)
- Psychological clearance (no active eating disorders, untreated depression)
- Commitment to lifelong dietary changes and follow-up
- No active substance abuse or untreated medical conditions
Check your eligibility using the BMI Calculator and Ideal Weight Calculator.
Risks & Complication Rates (2026 Safety Data)
Modern laparoscopic surgery techniques have made bariatric procedures among the safest major operations:
Overall safety profile:
- Mortality risk: 0.1% (1 in 1,000 procedures)
- Major complications: 4% (infection, bleeding, leaks)
- Minor complications: 15% (nausea, vitamin deficiency, dumping syndrome)
Procedure-specific risks:
| Risk Factor | Gastric Sleeve | Gastric Bypass | Gastric Band |
|---|---|---|---|
| Leak rate | 1-2% | 1-3% | <1% |
| Bleeding | 1-2% | 2-4% | <1% |
| Long-term vitamin deficiency | Low | High | Minimal |
| Dumping syndrome | Rare | 10-15% | None |
| Revision surgery need (10yr) | 5-10% | 10-15% | 35-40% |
Serious complications like pulmonary embolism occur in <1% of cases with modern prophylaxis protocols.

Recovery Timeline: Hospital to Full Activity
Hospital phase (Days 1-3):
- Gastric sleeve: 1-2 day stay
- Gastric bypass: 2-3 day stay
- Pain managed with IV then oral medications
- Clear liquid diet begins 4-6 hours post-surgery
- Walking encouraged within 4 hours of procedure
Home recovery (Weeks 1-4):
- Week 1-2: Liquid diet only, minimal activity
- Week 3-4: Pureed foods, return to desk work
- Pain resolves within 7-10 days for most patients
- Fatigue normal due to caloric restriction
Returning to normal (Weeks 4-12):
- Soft foods introduced week 4-6
- Regular foods by week 8-10
- Exercise progression: walking → light cardio → strength training
- Full recovery and unrestricted activity by 12 weeks
Lifelong requirements:
- Daily multivitamin with iron
- Calcium and vitamin D supplementation
- B12 injections or sublingual (bypass patients)
- Protein intake 60-80g daily
- Annual bloodwork monitoring
Understanding post-operative nutritional needs is essential for long-term success.
Decision-Making & Alternatives
Bariatric Surgery vs GLP-1 Medications: 2026 Comparison
The emergence of GLP-1 medications (Ozempic, Wegovy, Mounjaro) has transformed obesity treatment decision-making in 2025-2026. Understanding how these drugs compare to bariatric surgery helps patients choose the most appropriate intervention.
Surgery vs GLP-1 Drugs: The Data
Recent ASMBS research comparing bariatric surgery to GLP-1 medications reveals significant differences:
| Factor | Bariatric Surgery | GLP-1 Medications |
|---|---|---|
| Weight loss (2 years) | 60-80% excess weight | 15-20% total body weight |
| Diabetes remission | 70-80% | 40-50% |
| Treatment duration | One-time intervention | Indefinite injections |
| Annual cost | $0 after surgery | $12,000-$16,000/year |
| Weight regain after stopping | 20-30% over 10 years | 60-70% within 1 year |
| Cardiovascular benefit | 30-50% mortality reduction | 20% reduction |
Nicole Rodriguez tried Wegovy for 18 months, losing 42 pounds (starting weight 267). Within 6 months of stopping due to cost, she regained 38 pounds. She subsequently underwent gastric sleeve and has maintained 95-pound loss for 2 years—her insurance now covers the one-time surgery but not ongoing medications.
When GLP-1 medications work best:
- BMI 30-35 without major comorbidities
- Needle-comfort and weekly injection compliance
- Insurance coverage or financial resources ($1,000-$1,400/month)
- Preference for non-surgical intervention
When surgery is superior:
- BMI ≥40 or ≥35 with diabetes
- Failed medication attempts
- Seeking one-time definitive treatment
- Long-term cost-effectiveness priority
Some patients benefit from combination therapy—using GLP-1 drugs pre-surgery to reduce surgical risk, then relying on the permanent anatomical change post-operatively.
Choosing a Bariatric Surgeon: Accreditation Checklist
Essential qualifications:
- ✅ Board certification in general surgery
- ✅ Fellowship training in bariatric surgery
- ✅ Hospital ASMBS/MBSAQIP accreditation
- ✅ Minimum 125 procedures annually (surgeon volume)
- ✅ Complication rate <5% (program tracking)
Questions to ask your surgeon:
- How many of my specific procedure have you performed?
- What’s your leak/complication rate?
- What happens if I need revision surgery?
- How does your program support long-term follow-up?
- Can I speak with 2-3 past patients?
Find qualified surgeons at ASMBS provider directory.
What to Expect at Your First Consultation
Your initial bariatric surgeon consultation typically includes:
- Complete medical history review
- Physical examination and vital signs
- BMI calculation and weight history discussion
- Comorbidity assessment (diabetes, hypertension screening)
- Procedure option review based on your profile
- Insurance pre-authorization timeline explanation
- Required pre-operative testing outline
Many programs offer multidisciplinary team evaluations including nutritionists, psychologists, and exercise physiologists on the same day.
Related surgical procedures like gastric sleeve cost analysis and appendectomy recovery comparisons provide additional context for understanding surgical commitments.
11 Most-Asked Bariatric Surgery Questions (2026)
1. How much weight will I lose?
Most patients lose 60-80% of excess weight within 12-18 months, averaging 100-150 pounds depending on starting weight.
2. Does insurance cover bariatric surgery?
Yes—78% of commercial plans and Medicare cover surgery for patients meeting BMI ≥35-40 with documented medical necessity.
3. What’s the safest bariatric procedure?
Gastric sleeve offers the best safety-to-effectiveness ratio with 0.1% mortality risk and 60-70% weight loss.
4. How long is recovery?
Return to desk work in 2-3 weeks; full recovery and unrestricted activity by 12 weeks post-surgery.
5. Will I need plastic surgery after?
30-40% of patients elect panniculectomy or body contouring to address excess skin after major weight loss.
6. Can surgery cure diabetes?
Yes—70-80% achieve complete type 2 diabetes remission within 2 years; 30-50% maintain remission at 10 years.
7. What’s the mortality risk?
Modern bariatric surgery has 0.1% mortality rate—safer than knee replacement or gallbladder removal.
8. How much does it cost without insurance?
Self-pay prices range $14,000-$35,000 depending on procedure; many programs offer payment plans averaging $400-$600 monthly.
9. Can I have surgery with BMI 35?
Yes, if you have obesity-related comorbidities like diabetes, hypertension, or sleep apnea requiring medical treatment.
10. What’s better: sleeve or bypass?
Gastric sleeve offers easier recovery and fewer nutritional deficiencies; bypass delivers slightly higher weight loss and diabetes remission rates.
11. Do I need lifelong vitamins?
Yes—all bariatric surgery patients require daily multivitamin, calcium, vitamin D, and potentially B12 supplementation permanently.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.