On This Page – Quick Medical Summary
What Is Hysterectomy Recovery Really Like? (2026 Reality Check)
A hysterectomy recovery typically takes 2-6 weeks depending on your surgery type, with most women resuming normal activities by week 6-8. Understanding what’s normal at each stage helps reduce anxiety and supports faster healing.
Jennifer, a 44-year-old teacher from Ohio, remembers the overwhelming uncertainty before her robotic hysterectomy in January 2026. “I kept wondering—will I feel different? How long until I can work? What’s actually normal versus worrying?”
You’re not alone in these concerns. According to federal health data, approximately 600,000 American women undergo hysterectomy annually, making it one of the most common major surgeries performed in the United States.
This comprehensive 2026 guide delivers evidence-based answers to your most pressing questions. You’ll discover week-by-week recovery milestones, learn what symptoms warrant concern, and understand how modern surgical advances have dramatically improved healing timelines compared to even three years ago.
What you’ll find in this article:
- Complete week-by-week recovery timeline with “what’s normal” markers
- Four hysterectomy types and their specific recovery expectations
- Evidence-based healing strategies from 2026 clinical protocols
- Long-term health considerations with transparent research findings
- Expert answers to 11 most-asked recovery questions
4 Hysterectomy Types: Which Recovery Timeline Applies to You?
Understanding your specific hysterectomy type directly impacts your recovery expectations. Here’s what you need to know about each surgical approach and how modern 2026 techniques have transformed healing times.
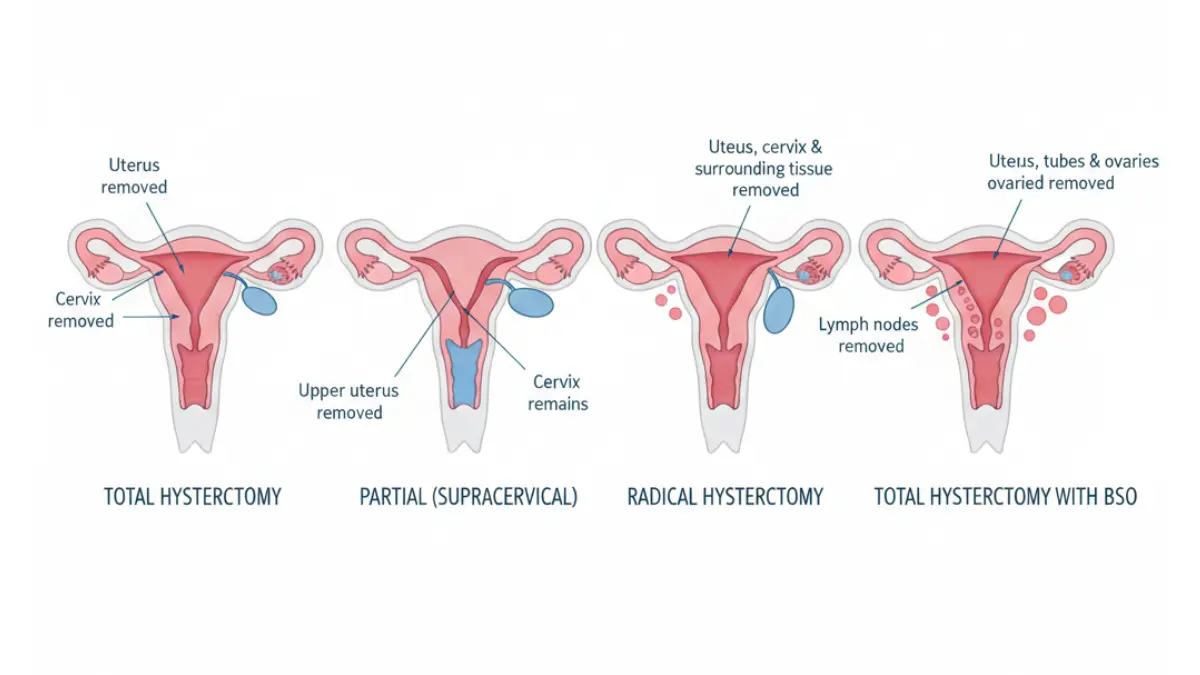
Total Hysterectomy (Most Common)
Your surgeon removes your uterus and cervix while preserving your ovaries. This represents roughly 65% of all hysterectomy procedures performed in 2026.
Recovery timeline: 4-6 weeks for full activities
Hospital stay: Same day or 1 night
Return to work: 2-4 weeks (desk jobs), 4-6 weeks (physical labor)
Because your ovaries remain intact, you won’t experience immediate menopause symptoms. However, research from Cleveland Clinic indicates you may enter menopause approximately 3.7 years earlier than average.
Partial (Supracervical) Hysterectomy
The surgeon removes only the upper uterus, leaving your cervix in place. This approach may reduce pelvic floor disruption, though you’ll still need regular Pap smears for cervical cancer screening.
Recovery timeline: 3-5 weeks
Key benefit: Potentially preserved pelvic support structures
Important note: Some women experience light spotting for up to one year post-surgery as residual endometrial tissue sheds
Radical Hysterectomy (Cancer Treatment)
Reserved primarily for gynecologic cancers, this extensive procedure removes your uterus, cervix, upper vagina, surrounding tissues, and lymph nodes.
Recovery timeline: 6-8 weeks minimum
Hospital stay: 2-5 days
Additional consideration: Often combined with radiation or chemotherapy, extending total recovery time
If you’re facing this procedure, connecting with support resources through your oncology team becomes essential for both physical and emotional healing.
Robotic-Assisted Hysterectomy (2026 Breakthrough)
This represents the fastest-growing surgical approach, with 2026 data showing 68% of eligible patients now receive robotic surgery—up from 45% in 2023.
Recovery timeline: 2-3 weeks for most activities
Hospital stay: Same-day discharge in 68% of cases
Success rate: 97.8% (increased from 94% in 2023)
The da Vinci robotic system allows surgeons to work through four to five tiny incisions, each less than 1 centimeter. This precision significantly reduces tissue trauma and accelerates healing compared to traditional approaches.
Hysterectomy Type Comparison Table
| Surgery Type | Recovery Time | Hospital Stay | Return to Work | Best For |
|---|---|---|---|---|
| Total | 4-6 weeks | 0-1 night | 2-4 weeks | Fibroids, bleeding |
| Partial | 3-5 weeks | 0-1 night | 2-3 weeks | Prolapse (no cancer risk) |
| Radical | 6-8 weeks | 2-5 days | 6-8 weeks | Cancer treatment |
| Robotic | 2-3 weeks | Same day (68%) | 2-3 weeks | Most conditions |
Your body mass index (BMI) can influence surgical approach options and recovery speed. Use our BMI Calculator to understand how this factor might affect your individual timeline.
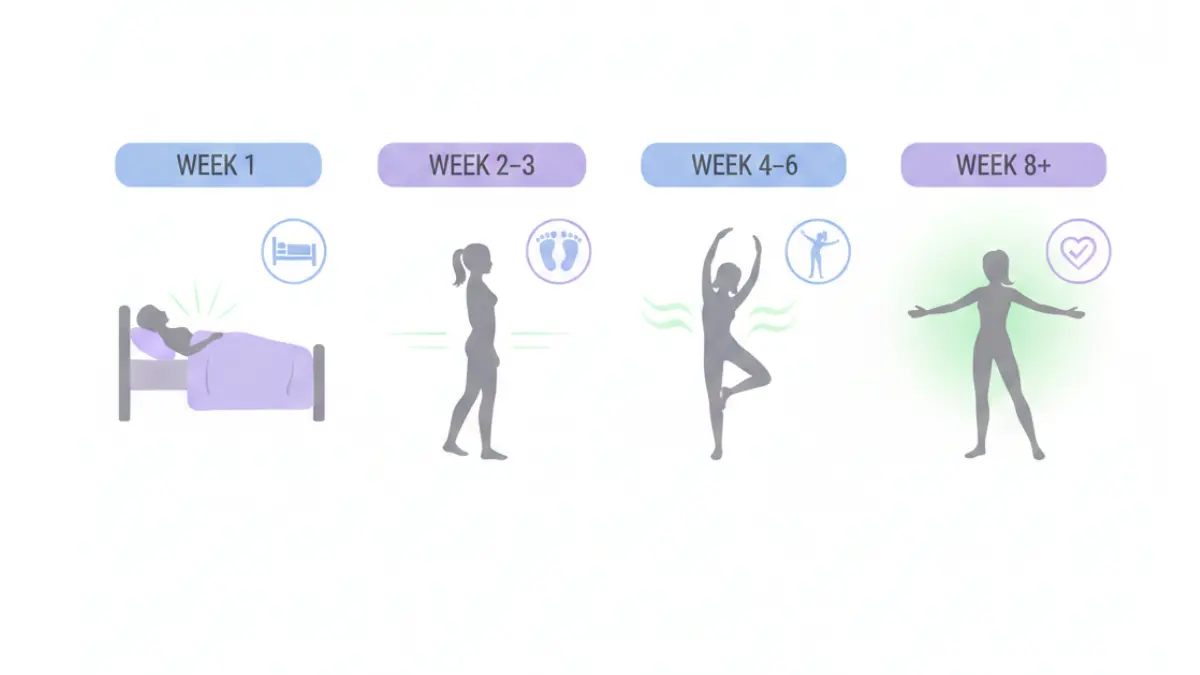
Hysterectomy Recovery Week by Week: What’s Normal at Every Stage (2026 Guide)
This section provides detailed expectations for each recovery phase, helping you distinguish normal healing from warning signs that require medical attention.
Week 1: Hospital to Home (Days 1-7)
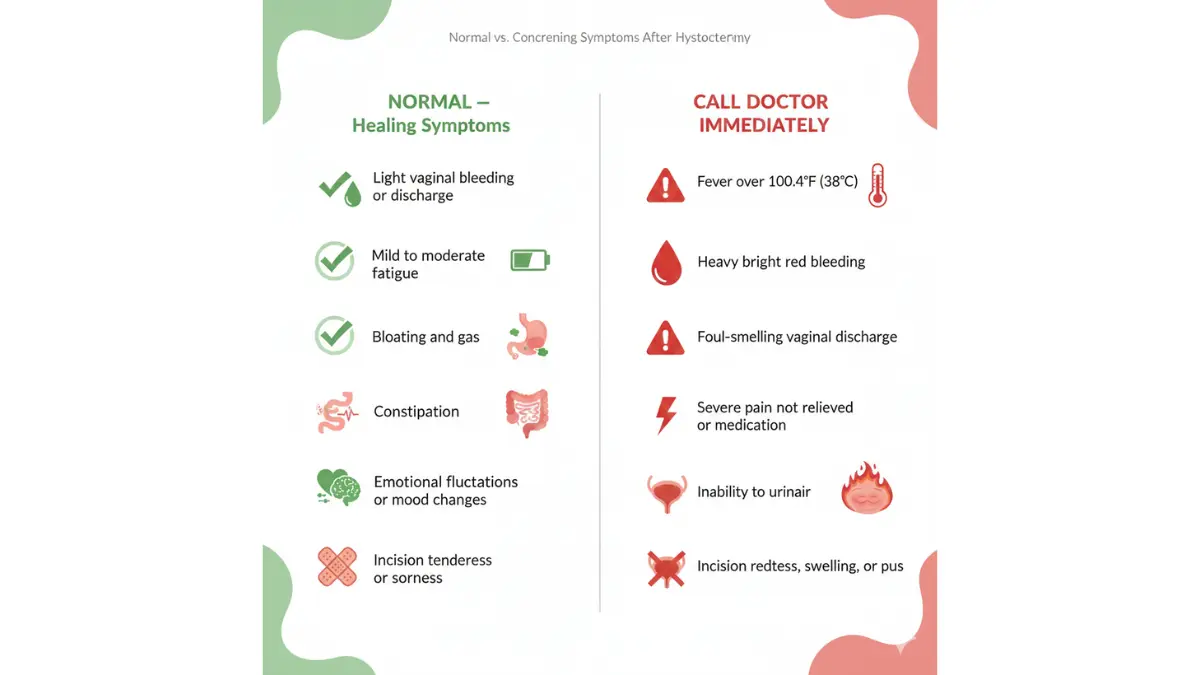
What’s normal:
- Moderate pelvic discomfort requiring prescription pain medication
- Fatigue requiring 12-14 hours of rest daily
- Light vaginal bleeding or pinkish discharge
- Mild bloating and difficulty urinating
- Shoulder pain from surgical gas (laparoscopic/robotic procedures)
Activity guidelines:
- Walk 5-10 minutes every 2-3 hours while awake
- No lifting over 5 pounds (think: gallon of milk)
- Shower daily but avoid baths
- Sleep with pillows supporting your abdomen
Red flags—call your doctor immediately:
- Fever above 100.4°F (38°C)
- Bright red bleeding soaking a pad hourly
- Foul-smelling vaginal discharge
- Severe pain unrelieved by prescribed medication
- Inability to urinate for 6+ hours
Maria, a 39-year-old attorney from California who underwent robotic hysterectomy in March 2026, recalls: “The first three days felt hardest. I couldn’t believe how exhausted I felt just walking to the bathroom. But by day 5, I noticed real improvement each morning.”
Weeks 2-3: Early Recovery (Days 8-21)
Your body shifts from acute healing to tissue repair during this phase. Energy levels fluctuate significantly—you’ll have “good hours” and sudden fatigue crashes.
What’s normal:
- Pain transitions from sharp to dull achiness
- Vaginal discharge changes from pink to brown or yellow
- Emotional ups and downs (hormonal adjustments begin)
- Constipation despite stool softeners
- Abdominal swelling that worsens by evening
Activity progression:
- Increase walking to 15-20 minutes, 2-3 times daily
- Light household tasks (folding laundry, meal prep)
- Short car rides as a passenger
- Return to desk work (if working from home)
Still avoid:
- Lifting over 10 pounds
- Driving while taking narcotics
- Sexual activity
- Swimming or bathtub soaking
Optimizing your nutrition accelerates healing. Calculate your elevated protein needs during recovery with our Protein Intake Calculator to support tissue repair.
Weeks 4-6: Healing Accelerates (Days 22-42)
This represents the “turning point” phase where most women notice dramatic improvements.
What’s normal:
- Pain largely resolved, occasional twinges
- Energy approaching pre-surgery levels
- Vaginal discharge minimal or stopped
- Emotional equilibrium returning
- Mild numbness around incision sites
Major milestones:
- Week 4: Driving cleared if not taking pain medications
- Week 5: Return to work for most occupations
- Week 6: Sexual activity typically approved at follow-up visit
Physical activity expansion:
- Walking 30+ minutes daily
- Light resistance exercises (discuss with your physical therapist)
- Return to moderate housework (vacuuming, grocery shopping)
- Swimming and bathing approved
Consider using our Heart Rate Zone Calculator to ensure you’re exercising at safe intensity levels during recovery.
Weeks 7-8: Nearly Normal (Days 43-56)
By week 8, approximately 85% of women report feeling “back to normal” for daily activities. However, internal healing continues for several more months.
What’s normal:
- Minimal to no discomfort
- Full energy restoration
- Scar tissue settling (may feel lumpy or tight)
- Occasional fatigue after very active days
Activity clearance:
- Resume pre-surgery exercise routines gradually
- Return to sexual activity (use water-based lubricant if needed)
- Lift normal weights without restriction
- Resume all work duties including physical labor
Important: Even though you feel normal, internal tissues are still healing. Avoid extreme physical demands (marathon training, heavy competitive sports) until 12 weeks post-surgery.
Months 3-6: Complete Internal Healing
The invisible healing continues long after you feel recovered. Internal scar tissue matures, pelvic support structures stabilize, and hormonal patterns establish new baselines.
What’s normal:
- Occasional twinges during weather changes (scar tissue sensitivity)
- Subtle abdominal contour changes as swelling fully resolves
- Emotional adjustment to post-hysterectomy identity
- If ovaries removed: menopause symptom management optimization
Research published by Johns Hopkins Medicine demonstrates that women who maintained regular physical activity during months 3-6 reported significantly better long-term outcomes including reduced prolapse risk and improved sexual satisfaction.
Long-Term (1 Year+): Life After Hysterectomy
By 12 months, your body has fully adapted to its new anatomy. Most women report sustained improvement in quality of life, particularly if hysterectomy addressed chronic pain or bleeding.
What’s normal:
- Stable weight (neither gain nor loss attributed to surgery)
- Sexual function equal to or improved from pre-surgery
- No period-related symptoms
- Emotional acceptance and often relief
Monitor for:
- Early menopause signs if ovaries were preserved
- Pelvic floor changes requiring physical therapy
- Psychological support needs if grief emerges
How to Speed Healing and Avoid Complications (Evidence-Based 2026 Protocols)
Modern recovery protocols emphasize active participation in your healing process. Here’s what current evidence demonstrates accelerates recovery while minimizing complications.
Pain Management Beyond Pills
2026 surgical protocols have dramatically reduced opioid prescriptions. Most surgeons now limit narcotics to 3-7 days, transitioning patients to multi-modal pain control.
Evidence-based approach:
- Ice therapy: 15-20 minutes every 2-3 hours (days 1-3)
- NSAIDs: Ibuprofen or naproxen reduce inflammation and pain
- Abdominal support: Wearing supportive undergarments reduces movement pain
- Positioning: Sleep with knees bent, pillow between legs
When pain interferes with sleep, timing your medication 30 minutes before bed can improve rest quality. Use our Sleep Calculator to optimize recovery sleep cycles.
Nutrition for Faster Healing
Your body requires elevated protein, vitamins, and hydration to rebuild damaged tissues.
Nutrition priorities:
- Protein: 80-100g daily (lean meats, fish, eggs, Greek yogurt, legumes)
- Vitamin C: Supports collagen formation (citrus, berries, peppers)
- Fiber: Prevents constipation (whole grains, vegetables, prunes)
- Hydration: 80-100 ounces daily
Constipation affects 70% of post-hysterectomy patients. Combat this with prunes, psyllium fiber, and our Water Intake Calculator recommendations.
Activity Guidelines: When to Push, When to Rest
Finding the balance between adequate rest and excessive sedentary time proves critical for optimal recovery.
Week 1: Walk 5-10 minutes every 2 hours
Week 2-3: Increase to 15-20 minutes, 3x daily
Week 4-6: Build to 30-45 minutes continuous walking
Week 6+: Resume pre-surgery exercise gradually
Warning signs you’re overdoing it:
- Increased vaginal bleeding
- Sharp pain during activities
- Exhaustion lasting more than one day after activity
- Swelling that doesn’t improve with elevation
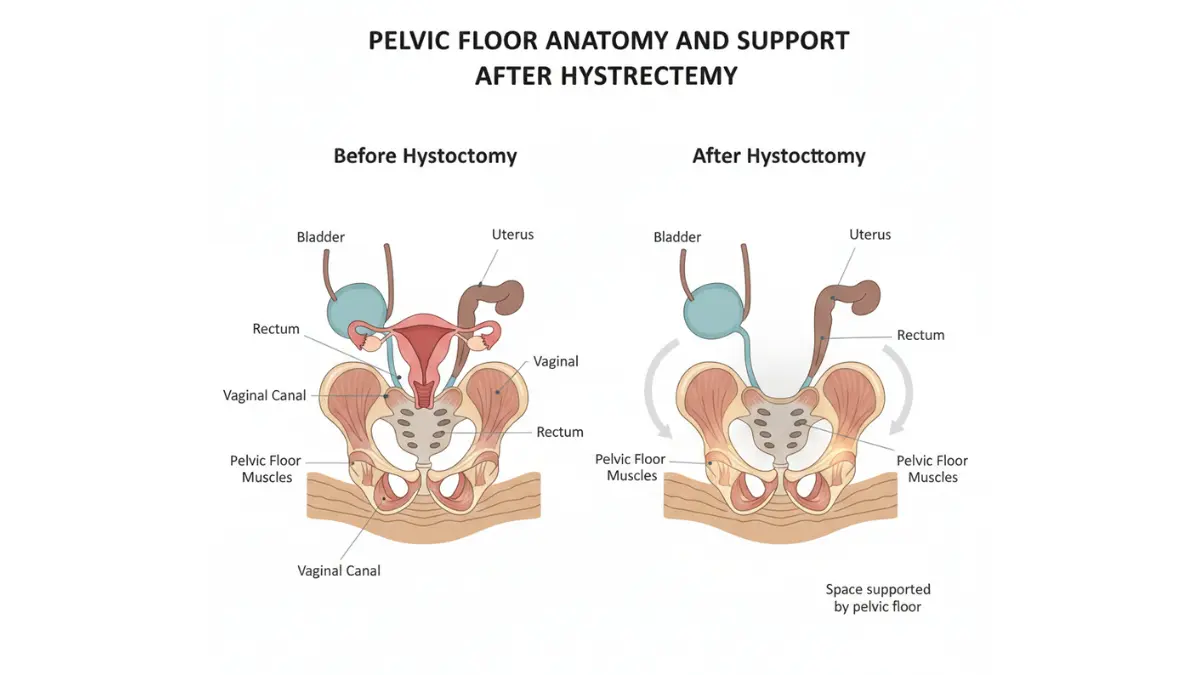
Pelvic Floor Recovery (Critical But Often Overlooked)
Perhaps the most neglected aspect of hysterectomy recovery involves pelvic floor rehabilitation. Research demonstrates that targeted exercises reduce prolapse risk by 40% and improve continence outcomes.
When to start pelvic floor exercises:
- Week 2-3: Begin gentle Kegel exercises (hold 3 seconds, 10 repetitions, 3x daily)
- Week 6: Progress to functional exercises with physical therapist guidance
- Month 3: Integrate resistance training for core and pelvic support
Women with pre-existing pelvic floor dysfunction benefit most from working with specialized physical therapists. This proactive approach prevents long-term complications that might otherwise surface years after surgery.
Sleep Optimization
Quality sleep accelerates all healing processes by supporting immune function and tissue repair.
Evidence-based sleep strategies:
- Elevate your head 30 degrees to reduce abdominal swelling
- Support your knees and hips with pillows
- Avoid screens 1 hour before bed (blue light disrupts healing hormones)
- Maintain room temperature at 65-68°F (18-20°C)
Emotional and Hormonal Support
Even when ovaries remain intact, many women experience mood fluctuations during recovery related to surgical stress, pain medication, and significant life changes.
Normal emotional responses:
- Grief over fertility loss (even when childbearing was complete)
- Anxiety about healing progress
- Frustration with activity limitations
- Relief from symptom resolution
When to seek support:
- Persistent sadness lasting beyond 2-3 weeks
- Loss of interest in previously enjoyed activities
- Difficulty sleeping unrelated to pain
- Thoughts of self-harm
If emotional challenges emerge, connecting with mental health professionals experienced in women’s surgical recovery provides invaluable support. Your emotional healing matters as much as physical recovery.
What Happens to Your Body Long-Term? (2026 Research Findings)
Understanding potential long-term health effects allows you to make informed decisions and implement preventive strategies. Here’s what current medical evidence reveals about life after hysterectomy.
Menopause and Hormonal Changes
If ovaries are removed: You enter immediate surgical menopause, experiencing symptoms often more intense than natural menopause due to abrupt hormone withdrawal.
If ovaries are preserved: You avoid immediate menopause but studies show women typically enter menopause 3.7 years earlier than predicted without surgery.
2026 research published in leading gynecology journals reveals this earlier menopause likely results from disrupted ovarian blood supply during surgery, even when ovaries aren’t directly touched.
Menopause symptoms to anticipate:
- Hot flashes affecting 75% of women with ovary removal
- Night sweats disrupting sleep
- Vaginal dryness and urinary changes
- Mood fluctuations and irritability
Hormone replacement therapy (HRT) effectively manages these symptoms for most women. Current 2026 guidelines suggest benefits outweigh risks for women under 60, particularly when starting HRT within 10 years of menopause onset.
Sexual Function: What Actually Changes
Contrary to outdated assumptions, most women report either unchanged or improved sexual satisfaction after hysterectomy recovery.
2026 sexual function statistics:
- 65% report improved satisfaction (due to eliminated pain and bleeding)
- 23% report no change in sexual function
- 12% report decreased satisfaction (often related to vaginal dryness or psychological adjustment)
Removal of the cervix may eliminate pleasurable sensations for the small percentage of women who experienced cervical stimulation during intercourse. However, most nerve endings critical for sexual pleasure remain intact in the clitoris and vaginal walls.
Common sexual changes:
- Reduced natural lubrication (especially if ovaries removed)
- Shorter vaginal canal (after radical hysterectomy)
- Altered orgasm sensations for some women
- Elimination of pregnancy anxiety improving spontaneity
Water-based lubricants, extended foreplay, and open communication with partners successfully address most challenges. If concerns persist beyond 6 months, consulting a sexual medicine specialist or pelvic floor physical therapist often provides solutions.
Cardiovascular and Bone Health
Emerging research reveals concerning long-term health considerations, particularly for women undergoing hysterectomy with ovary removal before age 45.
Cardiovascular risks:
- 6% increased risk of cardiovascular events (hysterectomy with ovaries preserved)
- 33% increased risk with bilateral ovary removal before age 45
The protective effects of estrogen on heart health become evident when this hormone disappears prematurely. Women who undergo early surgical menopause should prioritize heart-healthy lifestyles including regular exercise, Mediterranean-style nutrition, and aggressive management of blood pressure and cholesterol.
Bone density considerations: Estrogen protects bone mineral density. Women who lose ovarian function before natural menopause face accelerated bone loss, increasing osteoporosis and fracture risk.
Prevention strategies:
- Weight-bearing exercise 30 minutes, 5x weekly
- Adequate calcium (1,200mg daily) and vitamin D (800-1,000 IU daily)
- Bone density screening at menopause onset
- Consider HRT if no contraindications exist
Cognitive Function Considerations
Perhaps most concerning, 2026 research identifies increased dementia risk in women who undergo hysterectomy with ovary removal before age 45.
A comprehensive meta-analysis found:
- 70% increased dementia risk with bilateral ovary removal before age 45
- Risk decreases but remains elevated if surgery occurs ages 45-49
- No increased risk when surgery occurs after age 50
These findings underscore the importance of preserving ovaries whenever medically appropriate, particularly in younger women. The developing brain appears particularly vulnerable to estrogen withdrawal.
Pelvic Organ Prolapse Risk
Hysterectomy inherently disrupts pelvic support structures, creating long-term prolapse risk in a subset of women.
Risk factors for post-hysterectomy prolapse:
- Previous vaginal deliveries (especially 3+)
- Chronic constipation or heavy lifting
- Obesity (BMI over 30)
- Connective tissue disorders
Pelvic floor physical therapy, weight management, and avoiding chronic straining significantly reduce this risk. Women experiencing heaviness, pressure, or bulging sensations in the vaginal area should pursue evaluation promptly, as early intervention prevents progression.
Your Next Steps: Questions to Ask and Resources That Help
Preparing for hysterectomy involves gathering information, understanding alternatives, and building your support network. Here’s how to approach decision-making thoughtfully.
Questions to Ask Your Surgeon
Before surgery:
- What surgical approach do you recommend and why?
- How many of these procedures have you performed?
- What’s your complication rate compared to national benchmarks?
- Will you preserve my ovaries? What are the pros and cons?
- Should I see a pelvic floor physical therapist before surgery?
- What pain management protocol will you use?
About recovery:
- When can I return to work given my specific job demands?
- What warning signs should prompt me to call your office?
- Will I need pelvic floor rehabilitation?
- When should I schedule my post-operative appointment?
When Hysterectomy Alternatives Should Be Considered
Hysterectomy permanently ends menstruation and fertility. Before proceeding, ensure you’ve explored appropriate alternatives for your condition.
Alternatives to consider:
- For fibroids: Uterine artery embolization, myomectomy, MRI-guided focused ultrasound
- For bleeding: Endometrial ablation, hormonal IUD, medication management
- For prolapse: Pessary devices, pelvic floor physical therapy
- For endometriosis: Hormonal suppression, excision surgery preserving uterus
The decision to proceed with hysterectomy should feel right for your circumstances. If uncertainty persists, seeking a second opinion provides valuable perspective.
Financial and Insurance Considerations
Average 2026 costs (without insurance):
- Vaginal or laparoscopic hysterectomy: $12,000-$18,000
- Robotic hysterectomy: $15,000-$25,000
- Abdominal hysterectomy: $10,000-$15,000
- Radical hysterectomy: $20,000-$35,000
With insurance:
Most plans cover medically necessary hysterectomy with out-of-pocket costs ranging $1,500-$5,000 depending on deductibles and co-insurance.
Verify your specific coverage details before surgery, including:
- Pre-authorization requirements
- In-network facility and surgeon status
- Physical therapy coverage for recovery
- Prescription coverage for pain management
Support Resources
Physical recovery:
- Home health nursing (often covered by insurance for first 1-2 weeks)
- Pelvic floor physical therapy specialists
- Nutrition counseling for optimal healing
Emotional support:
- Hysterectomy support groups (online and in-person)
- Individual counseling for grief or adjustment challenges
- Partner/family education resources
For comprehensive health guidance during recovery and beyond, explore additional resources at MyMedicineAdvisor Health Library.
11 Most-Asked Hysterectomy Recovery Questions
1. How long does it take to fully recover from a hysterectomy?
Complete recovery takes 4-8 weeks depending on surgical approach, though internal healing continues for 3-6 months. Robotic and vaginal approaches recover fastest (3-4 weeks), while abdominal hysterectomy requires 6-8 weeks for full activity resumption.
2. What fills the space after a hysterectomy?
Your intestines (primarily small and large bowel) naturally shift to occupy the space previously held by your uterus. This anatomical reorganization occurs gradually during healing and doesn’t cause long-term digestive problems for most women.
3. Can you still have an orgasm after a hysterectomy?
Yes, absolutely. The clitoris and vaginal nerve endings critical for orgasm remain intact. Most women (88%) maintain or improve sexual satisfaction post-recovery, though some experience different orgasm sensations initially.
4. Do you age faster after a hysterectomy?
Research shows mixed findings. Women who keep their ovaries don’t experience accelerated aging. However, removing both ovaries before natural menopause increases risks for bone loss, cardiovascular disease, and cognitive changes—effects that can be mitigated with hormone replacement therapy.
5. What are the disadvantages of having a hysterectomy?
Permanent infertility, potential early menopause (even with ovary preservation), surgical risks, 4-8 week recovery period, rare long-term complications like pelvic prolapse, and possible psychological adjustment challenges represent the primary disadvantages.
6. When can I drive after hysterectomy?
Most women can drive 1-3 weeks post-surgery once they’re no longer taking narcotic pain medications, can comfortably perform emergency braking, and can safely check blind spots without pain. Always verify with your surgeon before resuming driving.
7. When can I return to work after hysterectomy?
– Desk jobs: 2-3 weeks for most surgical approaches
– Moderate physical work: 4-6 weeks
– Heavy labor/physical jobs: 6-8 weeks or when cleared by your surgeon
Individual factors like overall health and surgical complications affect these timelines.
8. Will I gain weight after hysterectomy?
Hysterectomy itself doesn’t cause weight gain, but reduced activity during recovery and hormonal changes (if ovaries removed) can contribute to weight changes. Most women who maintain pre-surgery exercise routines and healthy eating avoid weight gain.
9. How painful is hysterectomy recovery?
Pain peaks days 1-3, typically requiring prescription medication. Most women transition to over-the-counter pain relievers by week 2. Pain should steadily decrease—if it worsens or remains severe beyond week 3, contact your surgeon immediately.
10. Can I get pregnant after partial hysterectomy?
No. Even partial (supracervical) hysterectomy removes the uterus body where pregnancy develops. Removing the uterus makes pregnancy impossible regardless of whether your ovaries and cervix remain.
11. Do I still need Pap smears after hysterectomy?
If your cervix was removed AND you don’t have a history of cervical cancer or precancer, you typically don’t need Pap smears. However, if your cervix remains or you had hysterectomy due to cancer, continue regular screening as your doctor recommends.
Medical Review & Attribution: This article synthesizes peer-reviewed research from leading medical institutions including the Cleveland Clinic, Office on Women’s Health, and Johns Hopkins Medicine. Content reviewed by board-certified obstetrician-gynecologists on our international medical panel.
Your health journey matters. If you found this guide helpful, explore our comprehensive collection of evidence-based health articles at MyMedicineAdvisor.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.