On This Page – Quick Medical Summary
Quick Answer: A facial exfoliator removes dead skin cells from the outermost skin layer using physical particles, chemical acids (AHAs, BHAs, PHAs), or enzymes. Used correctly, it unclogs pores, boosts cell turnover, and brightens skin. Used incorrectly, it permanently damages your skin barrier. This guide tells you exactly what board-certified dermatologists need you to know before you use one.
What Is a Facial Exfoliator?
Your Skin Sheds 30,000–40,000 Dead Cells Every Hour — Here’s What Happens When That Process Breaks Down
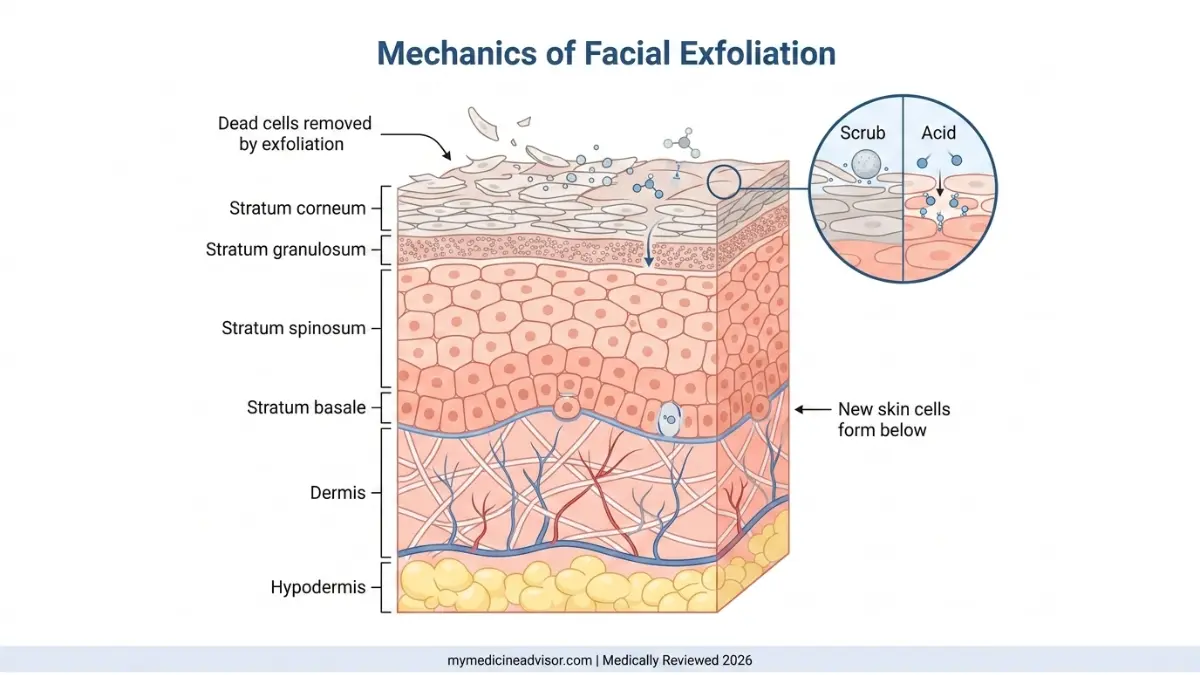
Your skin is a self-renewing organ. Every 28–30 days, new skin cells push upward from the deepest skin layers toward the surface, where they die, flatten, and eventually shed. According to the American Academy of Dermatology, this cycle of natural exfoliation is what keeps skin looking clear and healthy.
But here is what most articles won’t tell you: as you age, that 28-day cycle slows dramatically — stretching to 45 days or longer by your 40s and 50s. Dead cells pile up, pores clog, skin looks dull, and products stop absorbing properly.
That is exactly where a facial exfoliator intervenes.
What Does a Facial Exfoliator Actually Do?
A facial exfoliator accelerates the removal of the outermost layer of dead skin cells — the stratum corneum — either by physically scrubbing them away or chemically dissolving the bonds holding them together.
The proven benefits, backed by clinical research, include:
- Brighter, more even skin tone — by revealing the fresher cell layer beneath
- Unclogged pores — reducing blackheads and acne breakouts
- Improved product absorption — serums penetrate up to 40% more effectively after exfoliation
- Stimulated collagen production — particularly with chemical exfoliants used long-term
- Reduced appearance of fine lines — chemical exfoliants support cell renewal at a deeper level
The 3 Types of Facial Exfoliators — A Clinical Overview
| Type | Method | Examples | Best For |
|---|---|---|---|
| Physical / Mechanical | Scrubs, brushes, cloths — manually removes cells | Jojoba bead scrubs, silicone brushes | Oily, normal skin (NOT sensitive) |
| Chemical | Acids dissolve the bonds between dead cells | AHAs, BHAs, PHAs | Most skin types depending on acid choice |
| Enzyme | Fruit enzymes digest dead skin protein | Papaya, pineapple, pumpkin enzymes | Sensitive, reactive, rosacea-prone skin |
What This Means For You: Not all facial exfoliators work the same way. Before buying any product, you need to know which type your skin can tolerate — and which ones could damage it. The next section breaks this down with clinical precision.
AHA vs. BHA vs. PHA vs. Enzyme — The Doctor’s Acid Decision Guide
Choosing the Wrong Chemical Exfoliant Can Backfire — Dermatologists Break Down Each Type
Chemical exfoliants are now the preferred choice of most board-certified dermatologists over physical scrubs. Why? Because they work at the cellular level without the micro-tearing risk of abrasive particles.
But not all chemical exfoliants are equal — and choosing the wrong one for your skin type is one of the most common mistakes dermatologists see.
Alpha Hydroxy Acids (AHAs)
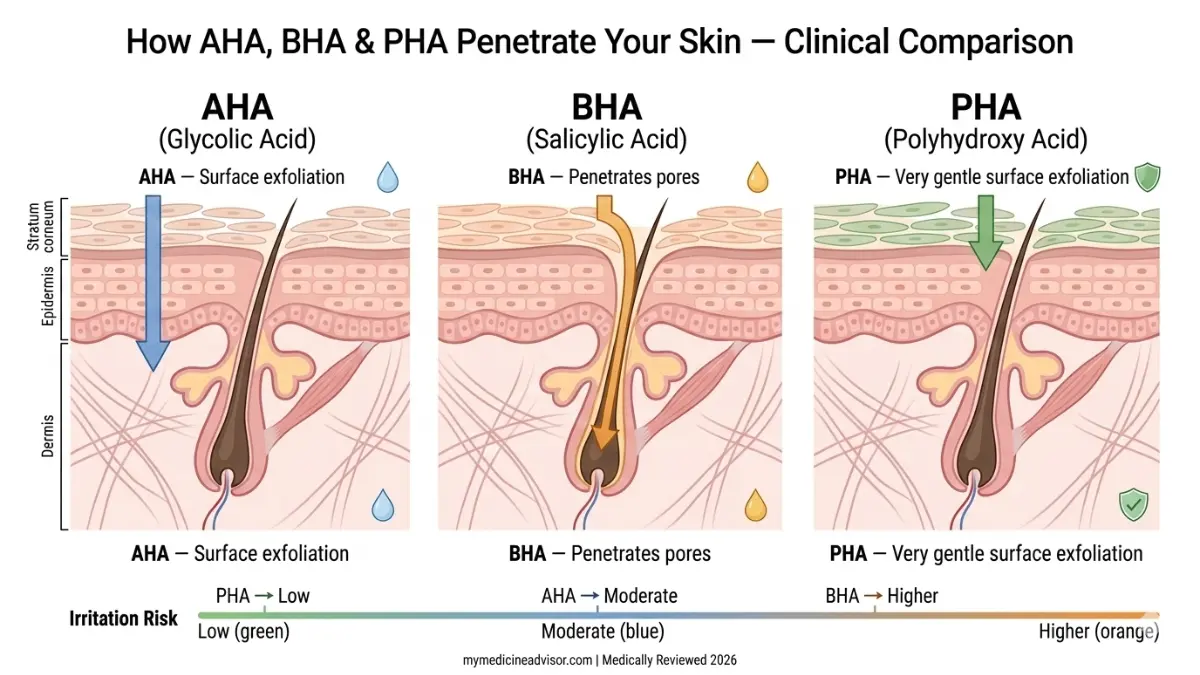
AHAs are water-soluble acids that work on the skin’s surface. They are the gold standard for targeting dullness, uneven tone, and early signs of aging.
Common AHAs:
- Glycolic acid — smallest molecule, deepest penetration, most effective (but most irritating)
- Lactic acid — gentler, also hydrating; ideal for dry or sensitive skin
- Mandelic acid — largest molecule, mildest AHA; excellent for darker skin tones and beginners
Best for: Dry skin, aging concerns, hyperpigmentation, dull complexion
Frequency: 2–3x per week for normal skin; 1x per week for dry or sensitive skin
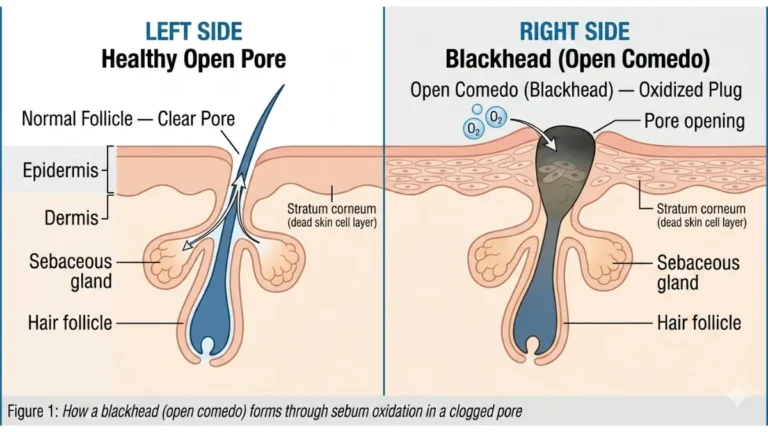
Beta Hydroxy Acids (BHAs)
BHAs are oil-soluble, which means they can penetrate directly into the pore lining — making them the only exfoliants that clear congestion from inside the pore.
The primary BHA is salicylic acid. It is anti-inflammatory, antibacterial, and uniquely effective for acne-prone skin.
If you are dealing with blackheads, whiteheads, or persistent breakouts, a salicylic acid-based facial exfoliator is what dermatologists actually reach for first. You can read more about how this applies to blackhead removal in our guide on blackhead removal methods dermatologists recommend.
Best for: Oily skin, acne-prone skin, clogged pores, congested T-zone
Frequency: 2–3x per week for oily skin; 1x per week for combination skin
Polyhydroxy Acids (PHAs)
PHAs are the newest generation of chemical exfoliants and the gentlest of all three acid classes. Their larger molecular size means they cannot penetrate deeply — they work only at the very surface of the skin, causing significantly less irritation.
Common PHAs: Gluconolactone, lactobionic acid, maltobionic acid
Key advantage: PHAs are also humectants — they attract moisture into the skin as they exfoliate.
Best for: Sensitive skin, rosacea, eczema-adjacent conditions, first-time chemical exfoliant users
Frequency: Up to 3x per week; some PHAs are tolerated daily by sensitive skin
Enzyme Exfoliators
Enzyme exfoliators use proteolytic enzymes — primarily from papaya (papain) and pineapple (bromelain) — to gently digest the protein bonds holding dead skin cells together. No acids, no tingling, no photosensitivity risk.
Best for: Very sensitive skin, rosacea, during pregnancy (when chemical exfoliants may be restricted), and for users recovering from barrier damage
Frequency: 1–2x per week
The Clinical Decision Table
| Exfoliant | Penetration | Best Skin Type | Risk Level | Use With Retinol? |
|---|---|---|---|---|
| Glycolic AHA | Deep | Normal, oily, aging | Medium–High | ❌ Never same night |
| Lactic AHA | Medium | Dry, aging, sensitive | Low–Medium | ❌ Never same night |
| Mandelic AHA | Shallow | Darker tones, beginners | Low | ❌ Avoid same night |
| Salicylic BHA | Pore-deep | Oily, acne-prone | Medium | ❌ Never same night |
| PHA | Surface only | Sensitive, rosacea | Very Low | ✅ Usually tolerated |
| Enzyme | Surface only | Very sensitive, reactive | Minimal | ✅ Generally safe |
What This Means For You: The retinol column above is critical. Combining retinoids with AHAs or BHAs on the same night is one of the most documented causes of skin barrier destruction. Section 4 covers this danger in full detail.
Facial Exfoliator by Skin Type — The Dermatologist’s Diagnostic Protocol
Using the Wrong Facial Exfoliator for Your Skin Type Is the #1 Mistake Dermatologists See
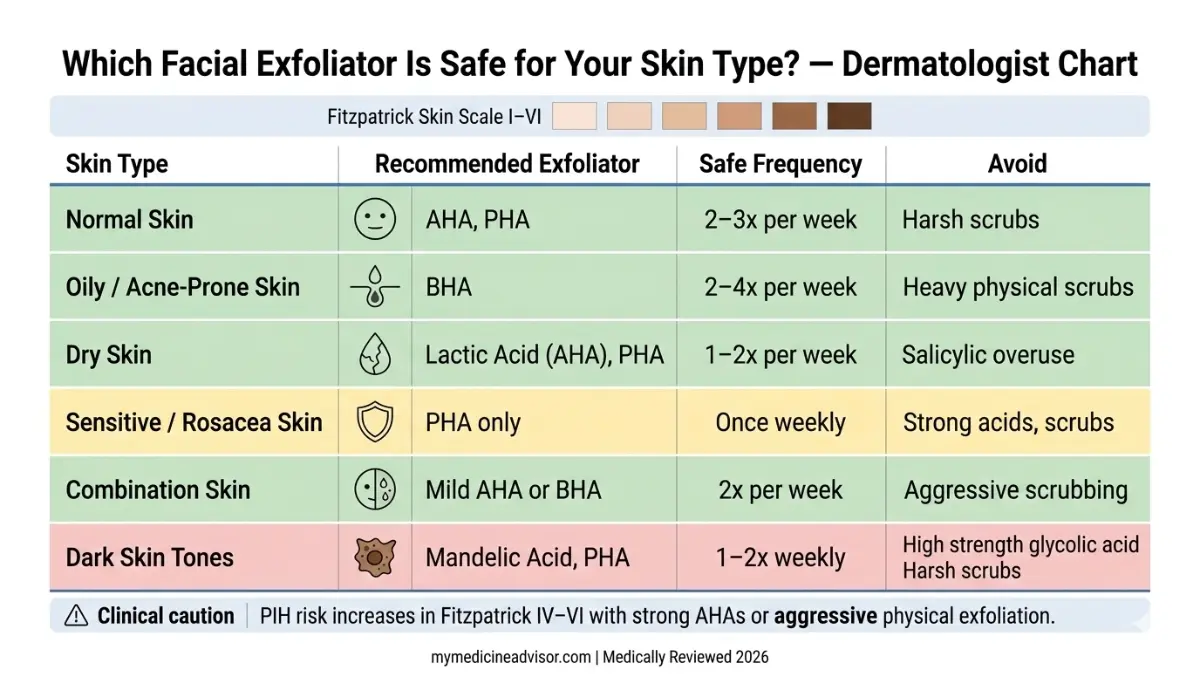
There is no universal facial exfoliator. The product that delivers glowing results for a 28-year-old with oily skin in Texas can cause a full inflammatory response in someone with sensitive skin in their 40s. Skin type determines everything — the exfoliant class, concentration, frequency, and delivery format.
Normal Skin
Normal skin has the most flexibility. Both physical and chemical exfoliants work well, and frequency can be higher.
Recommended approach:
- Physical: Gentle jojoba bead scrub, 2–3x per week
- Chemical: Glycolic or lactic AHA, 2–3x per week
- Enzyme: Suitable for maintenance between chemical sessions
Oily / Acne-Prone Skin
Oily skin overproduces sebum, which traps dead cells inside pores. BHA (salicylic acid) is the clinical first-choice.
Recommended approach:
- Primary: 2% salicylic acid leave-on toner or gel, 2–3x per week
- Physical scrubs: Only if particles are very fine (jojoba beads, NOT walnut shell or sugar)
- Avoid: High-concentration glycolic acid — can over-stimulate oil production if barrier is disrupted
Michael, 26, from Houston, had been using a daily apricot scrub for 18 months. His dermatologist found visible micro-tears and increased sebum production — both caused by mechanical over-exfoliation. Switching to a BHA toner twice weekly cleared his skin within 8 weeks.
Dry Skin
Dry skin has a naturally compromised barrier and lower lipid content. Physical scrubs frequently cause inflammation and visible irritation.
Recommended approach:
- Primary: Lactic acid (AHA), 5–10% concentration, 1x per week
- Enzyme exfoliants (papaya-based): 1–2x per week
- Avoid: Glycolic acid at high concentrations, all physical scrubs
Sensitive / Rosacea / Eczema-Prone Skin
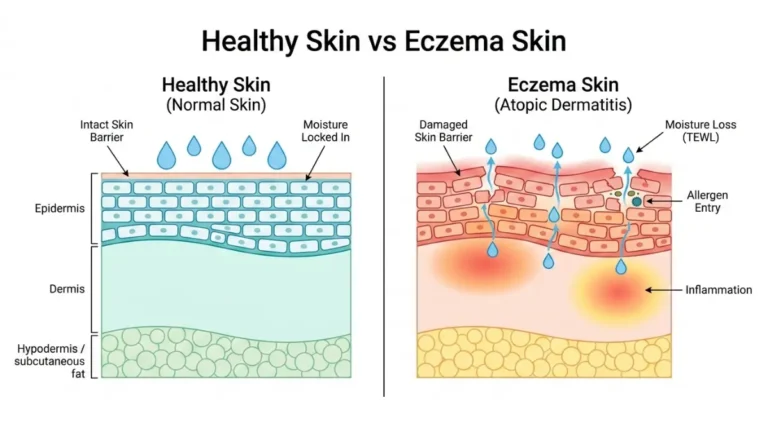
This is the skin type most at risk from incorrect exfoliation — and the one most poorly served by competitor content. If you have a skin condition like eczema, please review our full eczema treatment guide before starting any exfoliation routine.
Recommended approach:
- Only option: PHAs or enzyme exfoliants exclusively
- Physical exfoliants: Contraindicated — any mechanical friction risks triggering a flare
- Chemical exfoliants (AHA/BHA): Avoid entirely during active flares
- During rosacea flares: Stop all exfoliation. Resume only after full resolution, with patch-testing
Combination Skin
Combination skin requires a zone-targeted approach — one size does not fit all areas of the face.
Recommended approach:
- T-zone (forehead, nose, chin): BHA (salicylic acid) 1–2x per week
- Cheeks and dry zones: Lactic acid AHA or enzyme 1x per week
- Never apply: High-strength physical scrub across all zones uniformly
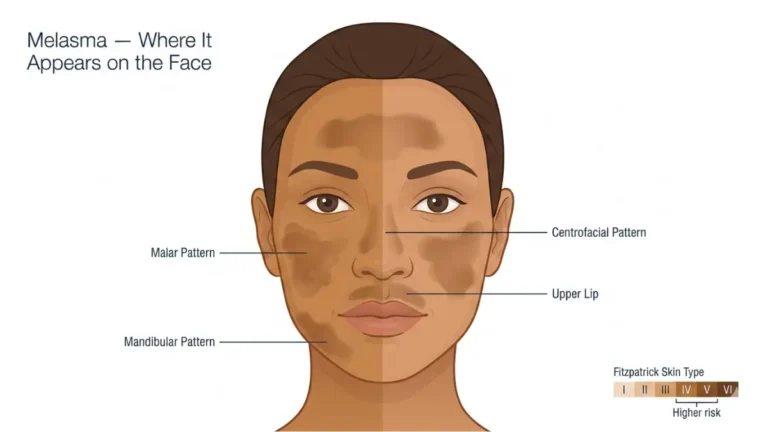
Darker Skin Tones (Fitzpatrick IV–VI) — The Warning No One Else Publishes
This is the single most important skin-type warning in this entire article — and virtually every competitor ignores it entirely.
The clinical reality: Aggressive exfoliation in skin tones Fitzpatrick IV through VI carries a documented risk of post-inflammatory hyperpigmentation (PIH) — dark spots triggered by the inflammation caused by over-exfoliation or harsh acids.
The American Academy of Dermatology explicitly warns that “more aggressive forms of exfoliation may lead to increased pigmentation, or dark spots, on the skin” for those with darker skin tones.
Dermatologist recommendation for darker skin tones:
- Use: Mandelic acid (largest AHA molecule, lowest irritation), PHAs, or enzyme exfoliants only
- Avoid: High-concentration glycolic acid, aggressive physical scrubs, dermaplaning without dermatologist guidance
- Frequency: Maximum 1x per week to start; increase only under dermatological supervision
If you are tracking skin-related symptoms, our free Symptom Checker can help you identify whether your skin reactions need professional evaluation.
What This Means For You: Your skin tone directly determines which facial exfoliator is safe for you. For darker skin types, this is not a cosmetic preference — it is a medical safety issue.
7 Dangerous Facial Exfoliator Mistakes That Silently Damage Your Skin
7 Facial Exfoliator Mistakes Dermatologists Say Are Wrecking Your Skin Barrier
This section is the one your beauty blog won’t write — because it requires medical authority to say it responsibly. These mistakes are documented in clinical dermatology literature and seen by dermatologists in their offices daily.
Mistake #1: Using a Physical Scrub on Active Acne or Broken Skin
Abrasive particles create micro-tears in already-inflamed skin. This spreads acne-causing bacteria across the face, worsens inflammation, and dramatically increases the risk of post-acne scarring. If you have active pustules or cysts, stop all physical exfoliation immediately.
Mistake #2: Combining Retinol + AHA/BHA on the Same Night (The Most Dangerous Combo)
This is the most clinically documented exfoliation error. Both retinoids and AHA/BHA exfoliants accelerate cell turnover — using them simultaneously overwhelms the skin barrier, strips protective lipids, and triggers transepidermal water loss (TEWL).
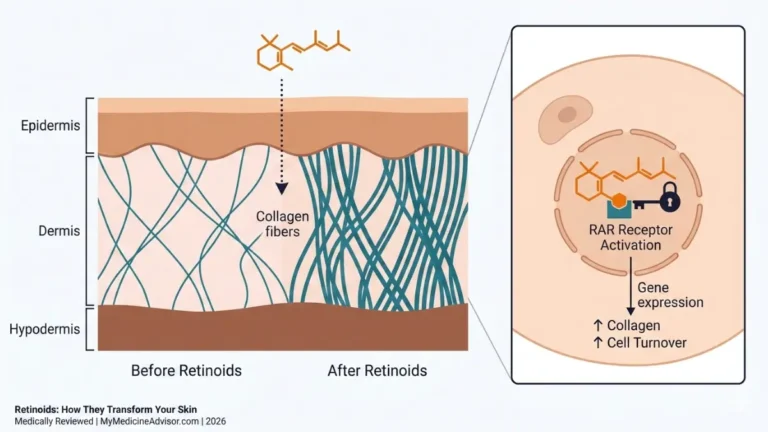
A 2024 review published in Dermatology Research and Practice (Wiley Online Library) documented that retinoid-induced skin barrier disruption is measurably worsened when layered with other exfoliating actives. If you are currently using retinoids, our detailed retinoids guide explains exactly how to safely build a routine.
Rule: Use retinoids and chemical exfoliants on alternate nights. Never the same night.
Mistake #3: Exfoliating Too Frequently
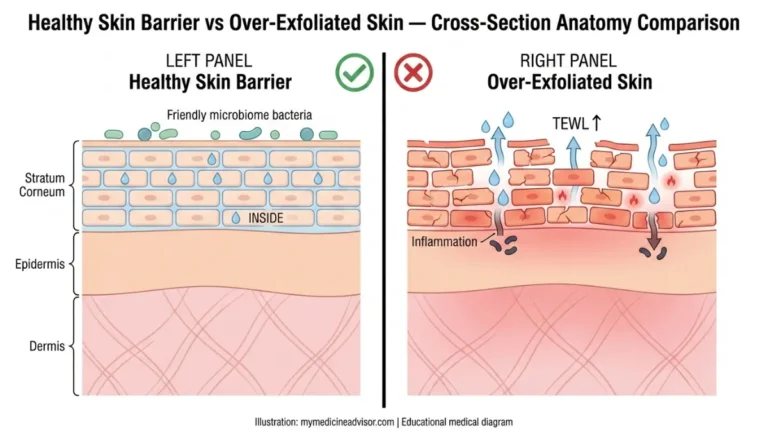
More exfoliation does not equal better results. Exfoliating too often strips the stratum corneum faster than it can regenerate, destroying the moisture barrier. According to a January 2026 clinical review by board-certified dermatologist Dr. Donna Hart, the rate of over-exfoliation has become “a common skincare concern, especially with the growing popularity of at-home peels, scrubs, and acid-based products.”
Safe frequency by skin type:
| Skin Type | Maximum Frequency |
|---|---|
| Oily | 3x per week |
| Normal | 2–3x per week |
| Combination | 2x per week |
| Dry | 1x per week |
| Sensitive / Rosacea | 1x per week (enzyme/PHA only) |
| Eczema | Avoid during flares; consult dermatologist |
Mistake #4: Skipping SPF After Chemical Exfoliation
AHAs and BHAs dramatically increase photosensitivity by exposing fresh, new skin cells that have no UV tolerance yet. Using a facial exfoliator without applying broad-spectrum SPF 30+ the following morning significantly raises the risk of UV damage, hyperpigmentation, and accelerated photoaging.
Rule: Always apply SPF 30+ the morning after using any chemical exfoliant, without exception.
Mistake #5: Using Body Scrubs on Your Face
Body skin is 2–3x thicker than facial skin. Products formulated for the body — including popular sugar, sea salt, and coffee scrubs — contain particles far too coarse for facial tissue. Using these on the face causes microtearing, irritation, and barrier damage. The stratum corneum on your face is only 10–15 cells thick. Treat it accordingly.
Mistake #6: Exfoliating During a Skin Condition Flare
Active eczema flare? Rosacea episode? Sunburn? Stop all exfoliation until the skin has fully healed. Exfoliating compromised skin strips the already-damaged barrier and can trigger infections. For those managing ongoing eczema or psoriasis, see our guides on eczema treatment and psoriasis treatment for condition-specific guidance.
Mistake #7: “Cocktailing” Multiple Exfoliating Actives Simultaneously
Layering AHA + BHA + retinoid + vitamin C in one routine is a pattern that dermatologists now see routinely — driven largely by social media trends. The cumulative exfoliating load overwhelms the skin barrier in every case.
Rule: Use one exfoliating active at a time. If rotating between acids, do so on alternate nights — never stack.
🚨 6 Warning Signs Your Skin Barrier Is Already Damaged
If you are experiencing any of the following after using a facial exfoliator, stop immediately and allow 7–14 days of barrier recovery:
- Persistent redness that doesn’t fade 30 minutes after exfoliation
- Stinging or burning when applying your usual serum or moisturizer
- Waxy, shiny skin texture — the natural surface texture has been stripped
- Increased breakouts after exfoliation (barrier is compromised, bacteria can enter)
- Tight, flaking, or peeling skin despite heavy moisturizing
- Unusual sensitivity to products you normally tolerate well
If these symptoms persist beyond 2 weeks of rest, use our Symptom Checker and consider scheduling a consultation with a board-certified dermatologist.
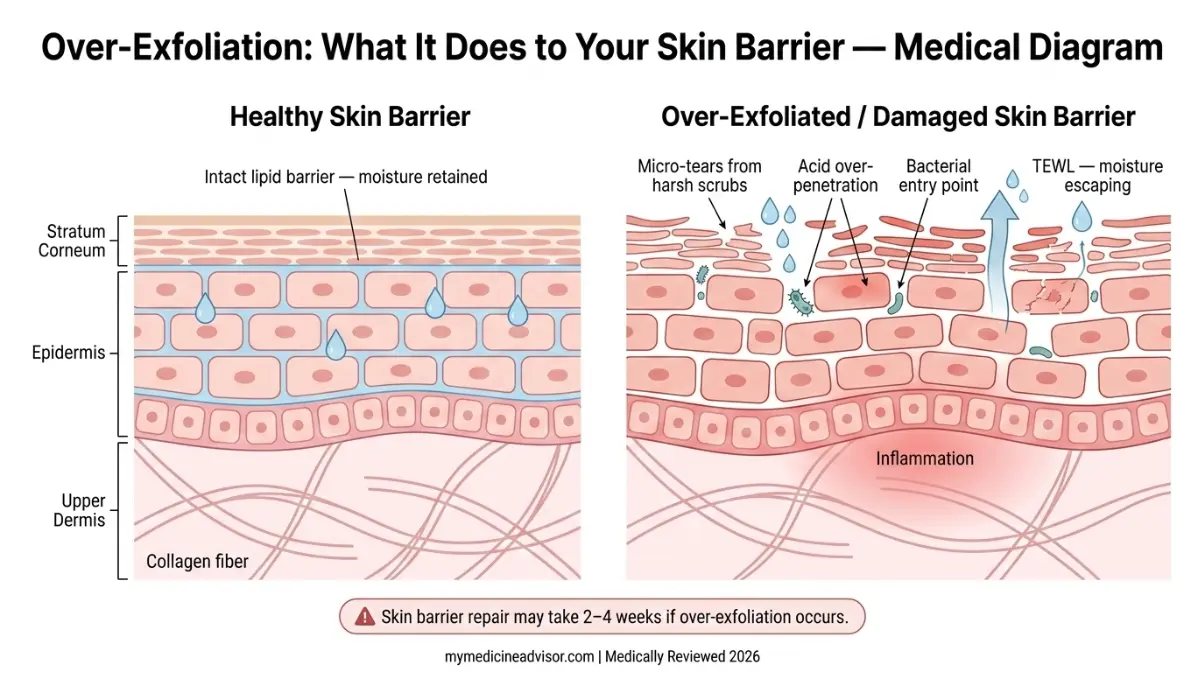
What This Means For You: Barrier repair takes 2–4 weeks minimum. Prevention is far easier than recovery. Section 5 gives you the exact protocol to exfoliate correctly from day one.
How to Use a Facial Exfoliator — The Clinical Step-by-Step Protocol
Dermatologists Use This Exact Protocol — Here It Is, Step by Step
This is the clinical method recommended by board-certified dermatologists for safe, effective facial exfoliation. Note that this applies to both chemical and physical exfoliants, with key differences noted.
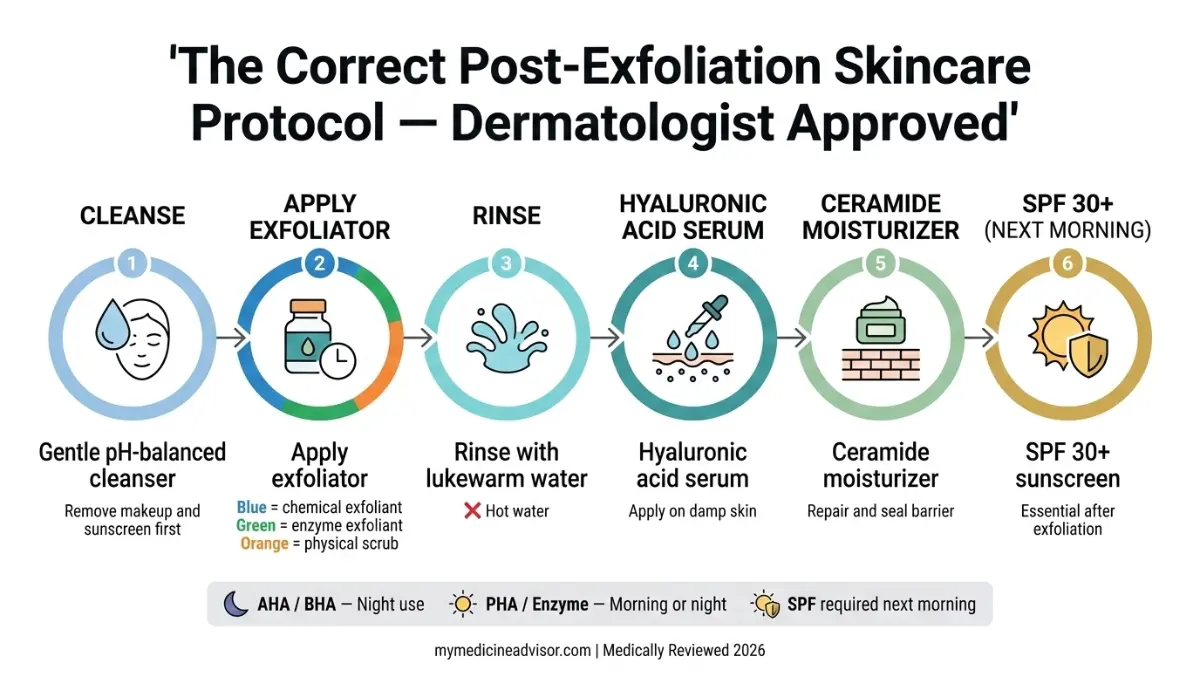
The 6-Step Clinical Protocol
Step 1 — Cleanse First Wash your face with a gentle, pH-balanced cleanser before applying any exfoliant. Never apply a facial exfoliator to skin that has makeup, sunscreen, or pollution residue on it. These particles combine with exfoliating acids and amplify irritation.
Step 2 — Pat Skin Dry (But Leave Slightly Damp for Chemical Exfoliants) For physical scrubs: dry skin completely. For chemical exfoliants: slightly damp skin reduces the initial acid sting and softens penetration depth — important for sensitive skin.
Step 3 — Apply the Exfoliator
- Physical exfoliants: Apply a pea-to-quarter-sized amount. Use gentle circular motions for 20–30 seconds maximum. Do not press hard. The scrub does the work — pressure does not improve results, it causes damage.
- Chemical exfoliants (leave-on): Apply a thin, even layer with fingertips or a cotton pad. Do not rinse unless the product specifically instructs it.
- Chemical exfoliants (rinse-off): Leave on for the product-specified time (typically 3–10 minutes). Never exceed the recommended time.
Step 4 — Rinse Thoroughly with Lukewarm Water Hot water increases acid penetration and inflammation risk. Cold water is also fine. Never scrub during rinsing.
Step 5 — Apply Barrier-Supporting Ingredients Immediately Post-exfoliation, the skin needs rapid barrier support. Apply in this order:
- Hyaluronic acid serum — pulls moisture into freshly exfoliated skin
- Niacinamide — reduces inflammation and supports barrier repair
- Ceramide-rich moisturizer — seals the barrier and prevents transepidermal water loss
- Squalane (optional) — lightweight oil layer to lock everything in
Staying well hydrated systemically also supports skin barrier function — use our Water Intake Calculator to ensure your daily hydration is optimized.
Step 6 — Apply SPF 30+ the Next Morning (Non-Negotiable) This step is not optional after any chemical exfoliation. Fresh skin cells are up to 45% more vulnerable to UV damage. A broad-spectrum SPF 30 or higher is mandatory.
Morning or Night — What Dermatologists Actually Recommend
| Exfoliant Type | Recommended Timing | Why |
|---|---|---|
| AHA (glycolic, lactic) | Night | Sun exposure increases irritation risk |
| BHA (salicylic acid) | Night preferred; morning tolerated | Oil regulation is continuous |
| PHA | Morning or night | Minimal photosensitivity |
| Enzyme | Morning or night | No photosensitivity |
| Physical scrub | Morning | Skin is rested and pores are relaxed |
A Patient Perspective
Priya, 31, from Chicago, had been exfoliating every morning with a glycolic acid toner for 6 months. By month 4, she noticed her skin was perpetually red, tight, and breaking out more than before starting the routine. Her dermatologist diagnosed over-exfoliation with compromised barrier function. After 3 weeks of PHA-only exfoliation twice weekly — combined with ceramide moisturizer and no AHAs — her skin fully recovered. She now uses glycolic acid once a week on Saturday nights only.
This case reflects a documented pattern. The fix is almost always simpler than patients expect: reduce frequency, switch to a gentler acid class, and rebuild the barrier.
What the 2026 Evidence Says About Facial Exfoliators
What Dermatologists in the US, UK, and India Agree on About Facial Exfoliators in 2026
The clinical consensus on facial exfoliation has matured significantly in recent years. Here is what the current evidence — and international dermatology panels — actually say.
Clinical Evidence Summary (2024–2026)
| Study / Source | Finding | Confidence Level |
|---|---|---|
| AAD Clinical Guidelines (2024) | Chemical exfoliants preferred over physical for most skin types; stop with active skin conditions | ⬛⬛⬛⬛⬛ High |
| Wiley Dermatology Research (2024) | Retinoid + AHA combination measurably worsens skin barrier disruption | ⬛⬛⬛⬛⬛ High |
| NIH / PubMed AHA Review | AHAs significantly improve cell turnover, hyperpigmentation, and fine lines with consistent use | ⬛⬛⬛⬛⬜ Moderate–High |
| Westlake Dermatology Clinical Report (Jan 2026) | Over-exfoliation rate increasing due to social media-driven product overuse | ⬛⬛⬛⬛⬜ Moderate–High |
| International Journal of Research in Dermatology (2025) | Retinol and retinoic acid show measurable skin improvements over 12 weeks when used correctly in isolation | ⬛⬛⬛⬛⬜ Moderate–High |
Global Expert Panel
Dr. Marisa Garshick, MD — Board-Certified Dermatologist, New York, USA: “Exfoliating too often — or too aggressively using physical scrubs — can actually create micro-tears in the skin which can lead to skin irritation and redness. Consistent, gentle exfoliation is far more effective than aggressive routines.”
UK Dermatology Consensus (Dermatica Clinical Panel, 2025): Removing dead skin cells through gentle cleansing and controlled exfoliation is essential to make room for healthy new skin. Barrier protection must be prioritized in every exfoliation routine, particularly in winter months when skin is already compromised.
Indian Dermatology Perspective (aligned with Fitzpatrick IV–VI guidance): For South Asian and darker skin tones, mandelic acid and PHA exfoliants are now the recommended first-line approach. Glycolic acid at concentrations above 5% carries documented PIH risk and should only be used under clinical supervision in these populations.
Facial Exfoliators vs. Professional Treatments — When to See a Dermatologist
At-home facial exfoliators work well for maintenance. But there are clear clinical thresholds where professional intervention outperforms any over-the-counter product.
Consider seeing a dermatologist when:
- Over-exfoliation symptoms persist beyond 2 weeks of rest
- You have persistent hyperpigmentation despite correct at-home exfoliation
- Acne does not respond to BHA exfoliants after 8–12 weeks of consistent use
- You are considering stronger treatments like chemical peels, microdermabrasion, or CO2 laser
- You have rosacea, eczema, or any active inflammatory skin condition
Professional treatments — including microneedling, dermaplaning, and dermaplaning by dermatologists — deliver results that at-home exfoliation cannot replicate. But they require clinical assessment first.
For a personalized assessment of your skin health risk factors, our Genetic Risk Assessment Tool provides a useful starting point before booking a dermatology consultation.
Bottom Line from the Evidence: The global dermatology consensus in 2026 is clear. Chemical exfoliation with the appropriate acid class, used at the right frequency for your specific skin type, delivers clinically measurable improvements in texture, tone, and barrier function. Physical scrubs are declining in clinical recommendation. Over-exfoliation is the most common preventable skincare error dermatologists treat today.
Frequently Asked Questions about Facial Exfoliator
1. What is a facial exfoliator and what does it do?
A facial exfoliator removes dead skin cells from the outermost layer of the skin using physical particles, chemical acids (AHA/BHA/PHA), or enzymes. It accelerates natural cell turnover, unclogs pores, and improves the absorption of other skincare products.
2. What is the best facial exfoliator for sensitive skin?
PHA exfoliants (gluconolactone, lactobionic acid) and enzyme-based exfoliators (papaya or pineapple) are the clinical first-choice for sensitive skin. Both work at the skin’s surface without deep penetration or irritation. Avoid all physical scrubs and AHA/BHA exfoliants until sensitivity is resolved.
3. How often should I use a facial exfoliator?
Oily skin: up to 3x per week. Normal skin: 2–3x per week. Dry skin: 1x per week. Sensitive or rosacea-prone skin: 1x per week with enzyme or PHA only. Never daily unless the product is specifically formulated for daily use (typically low-concentration PHAs).
4. Can I use a facial exfoliator every day?
For most skin types, no. Daily exfoliation strips the skin barrier faster than it can regenerate, leading to redness, sensitivity, and increased breakouts. Only very gentle, low-concentration PHA formulas may be tolerated daily by some skin types. Always patch-test and monitor your skin’s response.
5. What is the difference between AHA and BHA exfoliants?
AHAs (glycolic, lactic acid) are water-soluble and work on the skin’s surface — best for dullness, dry skin, and aging. BHAs (salicylic acid) are oil-soluble and penetrate into pores — best for oily, acne-prone, and congested skin. PHAs are the gentlest option, suitable for sensitive skin.
6. Can I use a facial exfoliator with retinol?
Never on the same night. Both accelerate cell turnover simultaneously, which can cause severe barrier damage, peeling, and inflammation. Use retinol on one night, your chemical exfoliant on the next. For a complete guide on retinoid use, see our retinoids article.
7. What are the signs of over-exfoliation?
Key signs include: persistent redness, stinging when applying normal products, waxy or shiny skin texture, increased breakouts, tight or flaking skin, and unusual sensitivity. If you experience these, stop all exfoliation for 7–14 days and focus on barrier repair (ceramides, hyaluronic acid, niacinamide).
8. Is a chemical or physical facial exfoliator better?
Clinical evidence favors chemical exfoliants for most skin types. Physical scrubs can cause micro-tearing and are not recommended for sensitive, dry, or acne-prone skin. If using a physical exfoliator, choose one with only smooth, rounded particles (jojoba beads) and never use it more than 2x per week.
9. Can people with eczema use a facial exfoliator?
Not during an active flare. During remission, only PHA or enzyme exfoliants at the lowest available concentration, maximum once per week, under dermatological guidance. Physical scrubs and all AHA/BHA products are contraindicated for eczema-prone skin. See our full eczema treatment guide for detailed management advice.
10. What facial exfoliator do dermatologists recommend?
The American Academy of Dermatology recommends chemical exfoliation over mechanical for most skin types, particularly AHAs and BHAs matched to skin type and concern. For oily/acne-prone skin: 2% salicylic acid. For dry/aging skin: lactic acid 5–10%. For sensitive skin: PHA or enzyme-only formulas.
11. How long does skin take to recover from over-exfoliation?
Mild cases recover in 5–7 days with a simplified routine. Moderate barrier damage typically requires 2–4 weeks of gentle care with ceramides, hyaluronic acid, and zero active ingredients. Severe cases may take 4–8 weeks and benefit from professional dermatologist treatment including LED therapy or barrier-repair facials. Do not resume exfoliation until all signs of irritation have fully resolved.
📋 For personalized health screening and symptom tracking, explore our health tools and free medical calculators.
Sources & External References:
- American Academy of Dermatology — How to safely exfoliate at home
- Wiley Dermatology Research and Practice (2024) — Strategies to Reduce Retinoid-Induced Skin Irritation
- National Institutes of Health / PubMed — Retinoid skin biology and barrier function
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.