On This Page – Quick Medical Summary
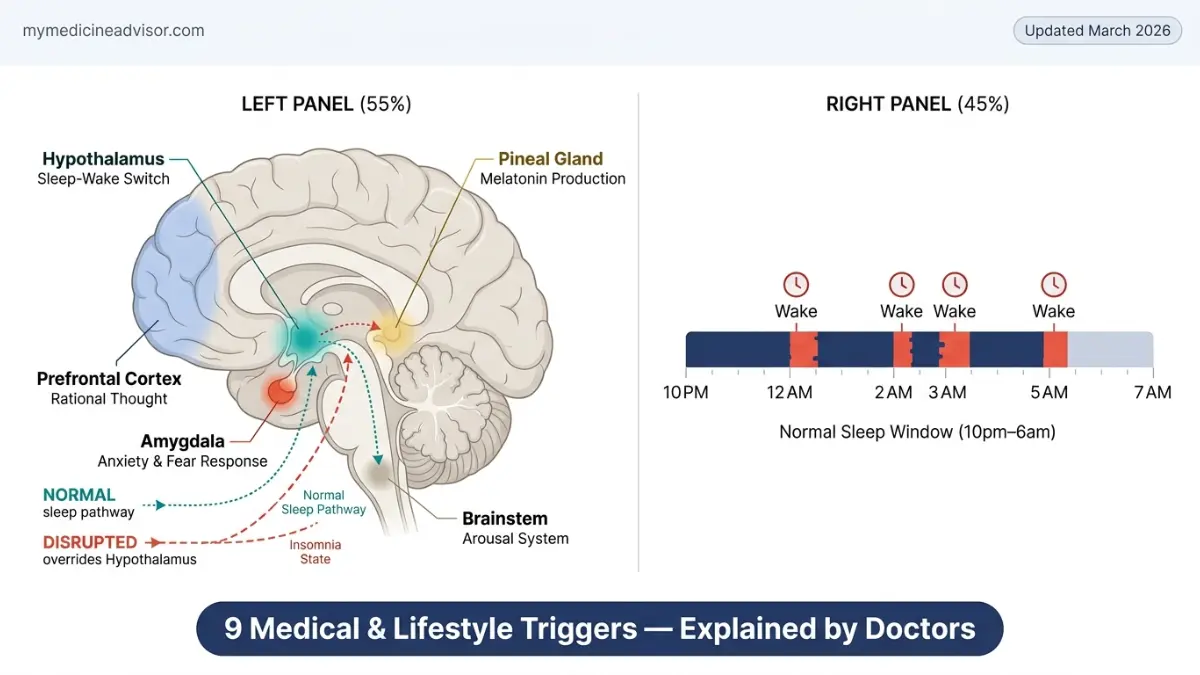
Insomnia is a sleep disorder that makes it hard to fall asleep, stay asleep, or wake up too early — leaving you exhausted even after hours in bed. It affects 35% of American adults, with over 12.8 million Google searches per year. The causes aren’t always obvious. Most people blame stress, but insomnia has 9 distinct medical and lifestyle triggers — and identifying yours is the first step to fixing it.
Use our free Sleep Calculator to map your optimal sleep window before diving in.
⚡ 2026 Research Alert: A landmark study published in March 2026 found that people with both insomnia and sleep apnea face a dramatically elevated risk of heart disease. Sleep problems are no longer just a quality-of-life issue — they are a cardiovascular emergency.
At a Glance: 9 Insomnia Triggers
| # | Trigger | Type |
|---|---|---|
| 1 | Anxiety & Depression | Medical |
| 2 | Chronic Pain & Illness | Medical |
| 3 | Hormonal Changes | Medical |
| 4 | Neurological & Genetic Conditions | Medical |
| 5 | Chronic Stress | Lifestyle |
| 6 | Caffeine, Alcohol & Nicotine | Lifestyle |
| 7 | Screen Time & Blue Light | Lifestyle |
| 8 | Irregular Sleep Schedule & Shift Work | Lifestyle |
| 9 | Medications | Lifestyle/Medical |
What Is Insomnia — and Why Does It Happen?
Marcus, a 44-year-old Chicago-based accountant, hadn’t slept through the night in six weeks. He’d tried melatonin, cutting back on coffee, even white noise machines. Nothing worked. His doctor eventually traced the problem to a beta-blocker he’d been prescribed three months earlier. No one had told him it could disrupt sleep.
This is the insomnia reality most people miss: it’s rarely just one thing.
Insomnia is classified as either:
- Acute insomnia — lasting less than 3 months, usually triggered by a specific event or change
- Chronic insomnia — persisting for 3 months or longer, occurring at least 3 nights per week
According to MedlinePlus (NIH), chronic insomnia is most often secondary — meaning it’s driven by an underlying condition, substance, or behavioral pattern. Approximately 75–90% of people with chronic insomnia have at least one comorbid medical disorder.
The consequence? Not just fatigue. Untreated insomnia raises the risk of depression, hypertension, diabetes, and — based on new 2026 data — significant cardiovascular disease. Understanding whether your insomnia is medical or lifestyle-driven changes everything about how you treat it.
4 Medical Conditions That Directly Trigger Insomnia
Trigger #1 — Anxiety and Depression: The Mental Hyperarousal Loop
This is the most common medical cause of insomnia, and it works in both directions.
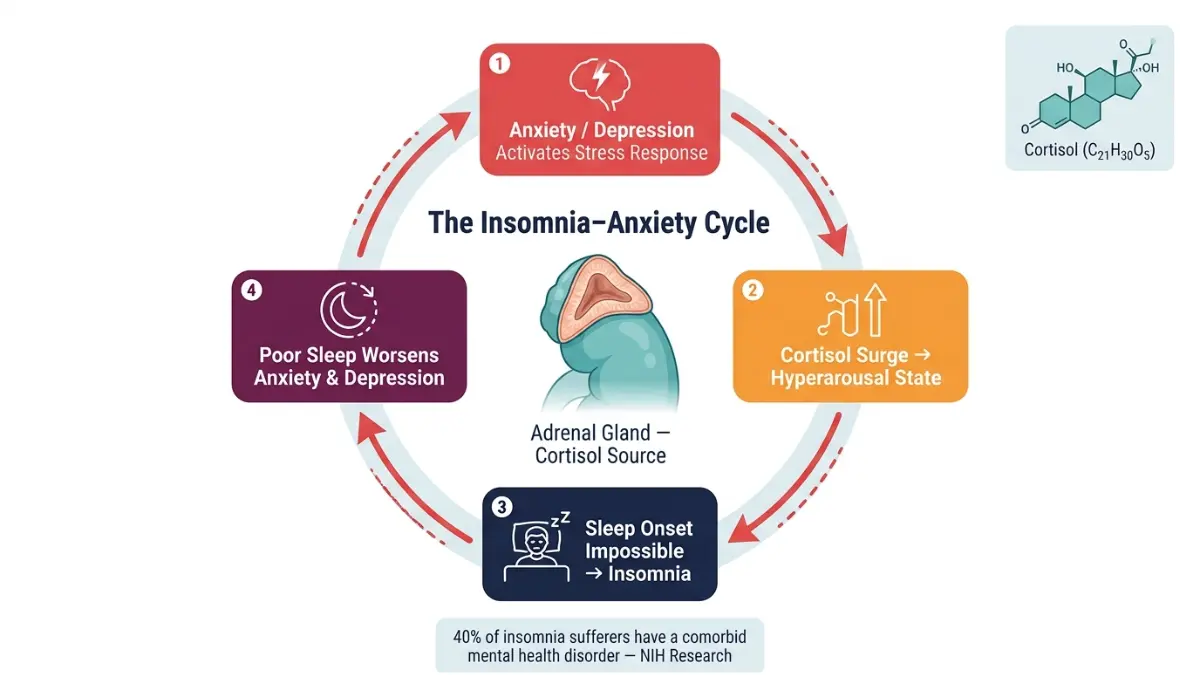
An estimated 40% of insomnia sufferers have a comorbid mental health disorder, according to NIH-published research on insomnia prevalence and etiology. Anxiety floods the body with cortisol — a stress hormone that raises alertness, elevates heart rate, and keeps the brain in a state of hyperarousal that makes sleep impossible to initiate.
Depression, meanwhile, disrupts the architecture of sleep itself. It reduces slow-wave deep sleep and fragments REM cycles, producing rest that feels shallow and unrestorative even when hours are adequate. Worse, poor sleep amplifies anxiety and depression the following day, creating a self-reinforcing cycle that is notoriously hard to break without intervention.
What This Means For You: If you’ve been told you have anxiety or depression, treating only the mental health condition without addressing the sleep disorder often fails both. CBT-I (Cognitive Behavioral Therapy for Insomnia) targets the cycle directly. Our guide on how to reduce anxiety naturally outlines evidence-based approaches that support both.
Trigger #2 — Chronic Pain and Physical Illness
Almost any condition that causes pain can make sleep impossible — not just because lying down is uncomfortable, but because pain activates the same neurological arousal pathways as stress.
Common pain-related insomnia drivers include:
- Arthritis (joint inflammation worsens at rest)
- Fibromyalgia (amplified pain perception disrupts sleep onset)
- GERD/acid reflux (symptoms intensify when lying flat)
- COPD and heart failure (breathlessness disrupts sleep architecture)
Research confirms that 75–90% of insomnia patients have an increased risk for comorbid medical disorders including conditions causing hypoxemia, dyspnea, and pain. Addressing the underlying condition is essential — insomnia cannot be resolved with sleep aids alone when chronic pain is the driver.
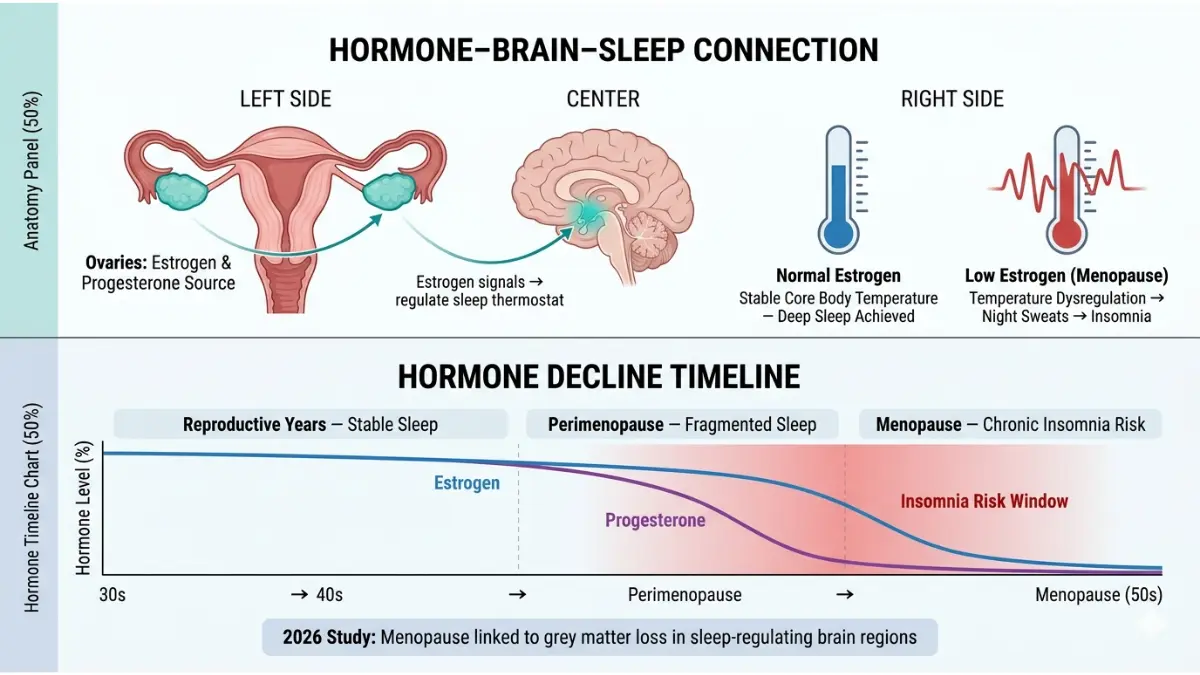
Trigger #3 — Hormonal Changes: The Underdiagnosed Trigger in Women
Hormonal fluctuations are one of the most underreported causes of insomnia in women — and 2026 research is redefining how seriously they should be taken.
A major study published in February 2026 linked menopause to structural brain changes — including grey matter loss in regions governing memory and emotional regulation — alongside dramatically elevated rates of anxiety, depression, and insomnia. This is not simply “hormonal moodiness.” These are measurable neurological changes that disrupt the sleep-wake system at a biological level.
Hormonal insomnia occurs most frequently during:
- Perimenopause and menopause (estrogen and progesterone decline disrupts thermoregulation and sleep quality)
- The luteal phase of the menstrual cycle (progesterone drop in the days before menstruation)
- Pregnancy (especially the third trimester — physical discomfort, frequent urination, anxiety)
Women managing pregnancy-related sleep changes may find our Pregnancy Weight Gain Calculator useful for tracking physical changes that impact rest.
Trigger #4 — Neurological and Genetic Conditions
Several neurological disorders directly compromise the brain’s sleep regulation systems:
- Restless Legs Syndrome (RLS): Involuntary urge to move the legs at night — one of the most underdiagnosed causes of insomnia in adults over 50
- Periodic Limb Movement Disorder (PLMD): Repetitive leg jerking during sleep, fragmenting rest without the person realizing it
- Parkinson’s disease: Dopamine dysregulation disrupts REM sleep
- Fatal Familial Insomnia: A rare genetic prion disease causing progressive, untreatable sleeplessness — included here for completeness, not alarm
Genetic predisposition plays a documented role in insomnia susceptibility. If multiple family members struggle with sleep disorders, use our Genetic Risk Assessment Tool to assess your inherited risk profile.
5 Lifestyle Triggers That Cause Insomnia (And How to Identify Yours)
Trigger #5 — Chronic Stress and Psychological Hyperarousal
“Why can’t I sleep?” is the most-searched sleep question in 46 of 50 U.S. states, with over 51,000 monthly searches nationally. The answer, in most cases, begins with stress.
Stress activates the hypothalamic-pituitary-adrenal (HPA) axis, flooding the body with cortisol and adrenaline. The body doesn’t distinguish between a work deadline and a physical threat — both produce the same arousal state that blocks sleep. Read our deep-dive on what adrenaline does to your body to understand the full cascade.
Research identifies a subset of people with high “sleep reactivity” — those whose sleep is disproportionately disrupted by stress. This trait is linked to underlying anxiety sensitivity and appears to have both genetic and behavioral components.
3-Step Stress Audit (Do This Tonight):
- Write down every active worry before bed — externalizing reduces hyperarousal
- Set a “worry window” earlier in the day — 15 minutes to process, then close the loop
- Use a body scan or 4-7-8 breathing technique within 20 minutes of sleep
Trigger #6 — Caffeine, Alcohol, and Nicotine
These three substances are responsible for a significant proportion of insomnia cases in the United States — and most people dramatically underestimate their impact.
| Substance | How It Disrupts Sleep |
|---|---|
| Caffeine | Blocks adenosine receptors (sleep pressure signal); half-life of 5–7 hours; coffee at 3pm = active stimulant at 10pm |
| Alcohol | Initial sedation → suppresses REM sleep → causes early waking at 2–4am as the sedative effect wears off |
| Nicotine | Stimulant that raises heart rate; nicotine withdrawal during sleep cycles causes micro-arousals |
The alcohol-insomnia paradox is particularly important: millions of Americans use a nightly drink to “wind down,” not realizing it is actually fragmenting their sleep architecture and causing the very early waking they’re trying to avoid.
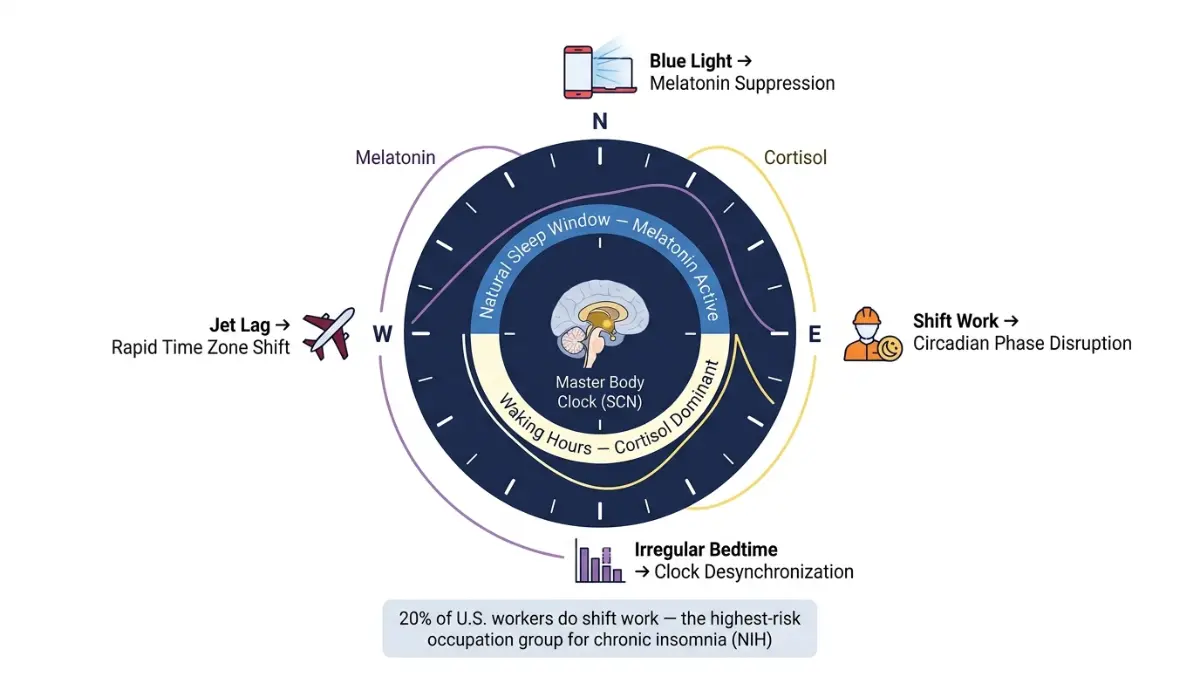
Trigger #7 — Screen Time and Blue Light Exposure
Blue light emitted by smartphones, tablets, and laptops suppresses melatonin production by up to 50%, according to Harvard Medical School research on sleep and circadian biology. Melatonin is the hormone that signals to the brain that darkness has arrived and sleep should begin.
Beyond blue light, social media use after 9pm has been independently associated with higher insomnia risk in a 2025 peer-reviewed study — separate from the light effect. The psychological arousal from social comparison, news consumption, and algorithmic stimulation keeps the brain alert at the precise moment it needs to power down.
What This Means For You:
- Set a hard screen cutoff 60–90 minutes before bed
- Use Night Mode or blue-light-blocking glasses if screen use is unavoidable
- Replace scrolling with a low-stimulation activity (reading, journaling, stretching)
For a deeper understanding of how your body regulates light and sleep cycles, read our guide on what circadian rhythm means and how disrupting it compounds insomnia risk.
Trigger #8 — Irregular Sleep Schedule and Shift Work
Your body runs on a circadian rhythm — a 24-hour internal clock governed by light, temperature, and behavioral cues. When your sleep and wake times shift unpredictably, this clock loses its anchor.
Approximately 20% of American workers are engaged in shift work, according to NCBI data on sleep loss and health consequences. Night shift workers are among the highest-risk groups for chronic insomnia, circadian rhythm disorder, and long-term metabolic dysfunction.
Even without shift work, chronotype mismatch — the gap between your natural sleep preference (early bird vs. night owl) and your required schedule — creates a form of “social jet lag” that compounds insomnia over time.
Use our Sleep Calculator to identify your optimal sleep window and align it with your chronotype. Consistency is the single most evidence-backed behavioral intervention for insomnia after CBT-I.
Trigger #9 — Medications: The Hidden Insomnia Trigger Most People Miss
This is the insomnia trigger that competitors consistently bury — or skip entirely. It may be affecting millions of Americans right now without their knowledge.
Drug classes commonly linked to insomnia include:
| Medication Class | Examples | Sleep Effect |
|---|---|---|
| Beta-blockers | Metoprolol, Atenolol | Suppress melatonin; cause vivid dreams and early waking |
| SSRIs/SNRIs | Sertraline, Venlafaxine | Cause sleep-onset delay; suppress REM sleep |
| Corticosteroids | Prednisone, Dexamethasone | Stimulant effect; cause night sweats and hyperarousal |
| Decongestants | Pseudoephedrine | Direct CNS stimulant |
| Antihistamines (non-sedating) | Fexofenadine, Cetirizine | Paradoxical stimulation in some individuals |
If you take any regular prescription or OTC medication and experience insomnia, use our Pill Identifier to review its documented side effects. Never stop a prescribed medication without consulting your doctor — but do raise the conversation. A simple timing adjustment (e.g., taking a corticosteroid in the morning instead of evening) can sometimes eliminate medication-induced insomnia entirely.
Who Is Most at Risk? A Clinical Risk Profile
Not everyone exposed to the same stressors, medications, or habits develops insomnia. Several factors increase biological vulnerability:
| Risk Factor | Relative Impact |
|---|---|
| Female sex | Up to 1.4× higher risk vs. males |
| Age 60+ | Elevated due to decline in sleep-regulating systems |
| African American heritage | Higher sleep latency and lower sleep quality (NIH data) |
| History of anxiety or depression | Up to 2× higher insomnia risk |
| Shift work / night work | Moderate-to-high risk |
| Family history of insomnia | Independent genetic risk factor |
Primary vs. Secondary Insomnia
- Primary insomnia: No identifiable underlying cause; often linked to long-standing stress, personality traits, or hyperarousal temperament
- Secondary insomnia: Caused by a medical condition, medication, or behavioral factor — the most common type
When to See a Doctor
Seek evaluation if you experience any of the following:
- Difficulty sleeping 3+ nights per week for more than 3 months
- Daytime impairment (concentration, mood, performance)
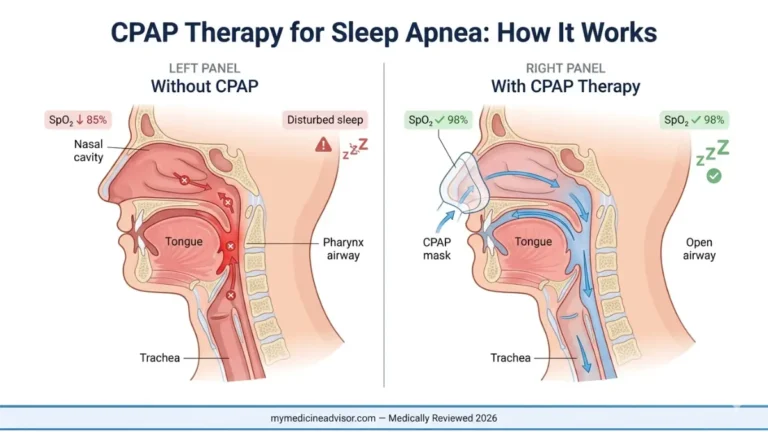
- Suspected sleep apnea (snoring, gasping, partner-reported pauses in breathing)
- Insomnia beginning with a new medication
Use our Symptom Checker to assess whether your sleep symptoms align with clinical insomnia criteria before your appointment. For related reading, our guide on warning signs of a sleep disorder covers the red flags most people miss.
How to Treat Insomnia Based on Its Root Cause
The biggest failure in standard insomnia advice is generic guidance — “exercise more,” “avoid caffeine,” “keep a consistent bedtime.” These steps matter, but they fail the majority of people because they don’t address the specific trigger driving the insomnia.
Trigger-Matched Treatment Table
| Root Cause | Evidence-Based First-Line Treatment |
|---|---|
| Anxiety / Depression | CBT-I + psychiatric evaluation; SSRIs where indicated |
| Chronic pain | Pain management protocol + sleep positioning strategies |
| Hormonal (menopause) | HRT assessment + CBT-I; discuss with gynecologist |
| Medications | Timing adjustment or prescriber review |
| Shift work / irregular schedule | Chronotherapy + strategic light exposure |
| Caffeine / alcohol / nicotine | Substance audit + elimination protocol |
| Screen time / blue light | Digital curfew + evening routine restructuring |
| Stress hyperarousal | CBT-I + mindfulness-based stress reduction (MBSR) |
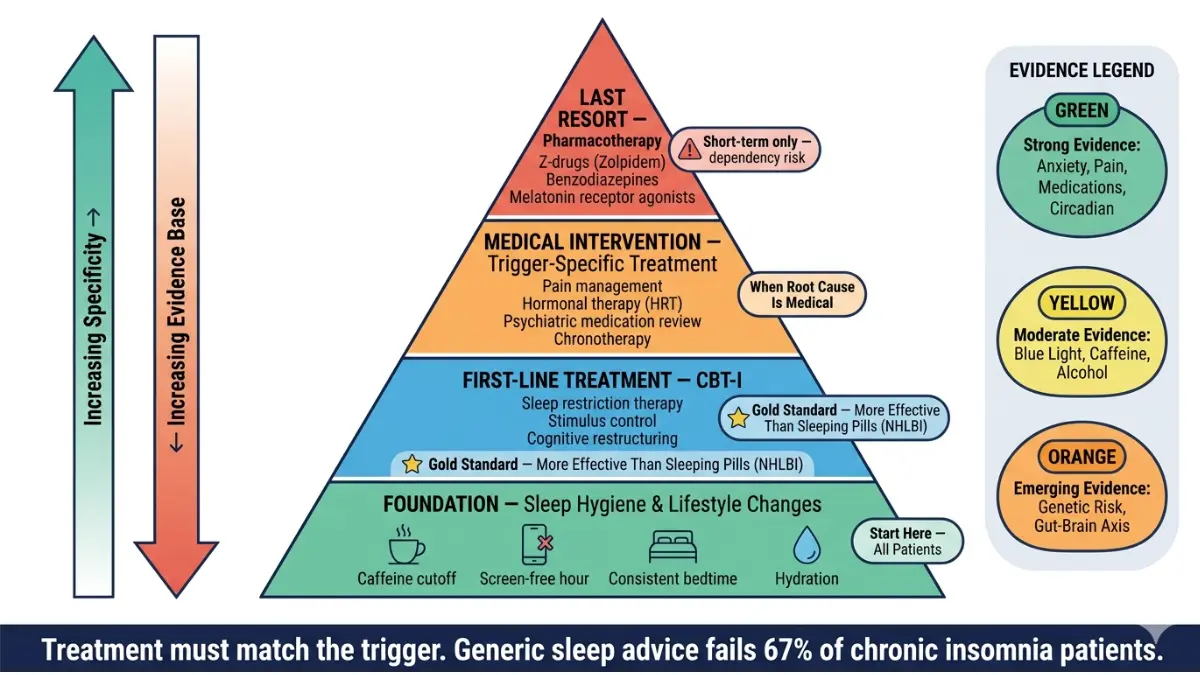
CBT-I is the gold standard for chronic insomnia — more effective than sleeping pills over the long term, with no dependency risk. The National Heart, Lung, and Blood Institute recommends it as the first-line treatment for adults with chronic insomnia disorder.
⚡ 2025–2026 Emerging Evidence
A December 2025 study found that chronic insomnia significantly reduces Natural Killer (NK) cell counts — the immune system’s rapid-response defense against infection and cancer. This adds immune suppression to the already documented cardiovascular, metabolic, and neurological consequences of untreated chronic insomnia.
What This Means For You — 3 Actions to Take This Week:
- Identify your trigger — use the table in Section 3 to self-audit
- Track your sleep for 7 days — bedtime, wake time, wake episodes, daytime impairment
- Book a GP appointment if symptoms meet chronic criteria (3+ nights/week, 3+ months)
Proper hydration also plays an underappreciated role in sleep quality. Use our Water Intake Calculator to ensure you’re adequately hydrated — dehydration increases cortisol and can worsen nighttime arousal.
What Sleep Experts Say — Global Medical Consensus on Insomnia (2026)
Our expert panel at mymedicineadvisor.com weighs in on the triggers most frequently missed in clinical practice:
Dr. Omar Hassan, MD — Internal Medicine:
“The most underdiagnosed insomnia trigger I see is medication-induced sleeplessness. Patients rarely connect a prescription they’ve taken for years to a sleep problem that started six months ago. The first clinical question should always be: what changed?”
Dr. Aditi Menon — Dermatology & Women’s Health:
“Hormonal insomnia in perimenopausal women is consistently undertreated. The 2026 data linking menopause to measurable brain changes should permanently shift how clinicians approach sleep complaints in women over 40.”
Dr. Vikram Nair — Endocrinology:
“Cortisol dysregulation and blood sugar instability are bidirectional drivers of insomnia that are rarely discussed together. Patients with diabetes or insulin resistance who experience early morning waking should have their nocturnal glucose patterns assessed.” Use our Blood Sugar Converter to track your glucose values in context.
Evidence Strength Summary
- 🟢 Strong evidence: Anxiety, depression, chronic pain, medications, circadian disruption, shift work
- 🟡 Moderate evidence: Blue light exposure, caffeine timing, alcohol fragmentation
- 🟠 Emerging evidence: Genetic predisposition, gut-brain axis disruption, NK cell suppression
📋 Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider for the diagnosis and treatment of insomnia or any sleep disorder. Do not discontinue any prescribed medication without medical supervision.
Frequently Asked Questions About Insomnia
1. What is the most common cause of insomnia?
Stress and anxiety are the most common triggers, driving psychological hyperarousal that prevents sleep onset. In clinical populations, approximately 40% of insomnia patients have a comorbid mental health condition.
2. Can anxiety cause insomnia every night?
Yes. Anxiety-driven cortisol elevation can sustain nightly hyperarousal indefinitely without treatment. CBT-I combined with anxiety management breaks this cycle most effectively.
3. Does stress cause insomnia?
Stress is the leading lifestyle cause of insomnia. It activates the HPA axis, elevating cortisol and adrenaline — both of which suppress sleep onset. For more on stress-insomnia physiology, read our article on sleep disorders: symptoms and causes.
4. What medical conditions cause insomnia?
Conditions most frequently linked to chronic insomnia include anxiety disorders, depression, chronic pain syndromes, GERD, COPD, heart failure, RLS, and hormonal disorders. Many have insomnia as a presenting — rather than secondary — symptom.
5. Can medications cause insomnia?
Yes. Beta-blockers, SSRIs, corticosteroids, decongestants, and some antihistamines are documented insomnia triggers. Always review your medication list with your prescriber if insomnia began or worsened after a new prescription.
6. Why do I wake up at 3am every night?
3am waking is frequently caused by alcohol metabolism (rebound arousal as sedative effects wear off), cortisol’s natural early-morning rise, or blood sugar dips. Our dedicated article on waking up at 3am every night covers every cause in detail.
7. Does alcohol help or hurt insomnia?
Alcohol initially sedates but actively worsens insomnia by suppressing REM sleep and triggering rebound arousal 3–5 hours after consumption. It is one of the most counterproductive sleep “remedies” in widespread use.
8. Can insomnia be caused by a hormone imbalance?
Yes. Estrogen and progesterone decline during perimenopause and menopause directly disrupt sleep architecture. Thyroid dysfunction (both hypo- and hyperthyroidism) is also a documented insomnia cause. Always check thyroid panels if insomnia is unexplained.
9. Is insomnia hereditary?
Partially. Family history of insomnia is an independent risk factor, with genetic components influencing sleep reactivity and circadian rhythm sensitivity. Use our Genetic Risk Assessment Tool to evaluate your inherited risk.
10. How do I know if my insomnia is chronic?
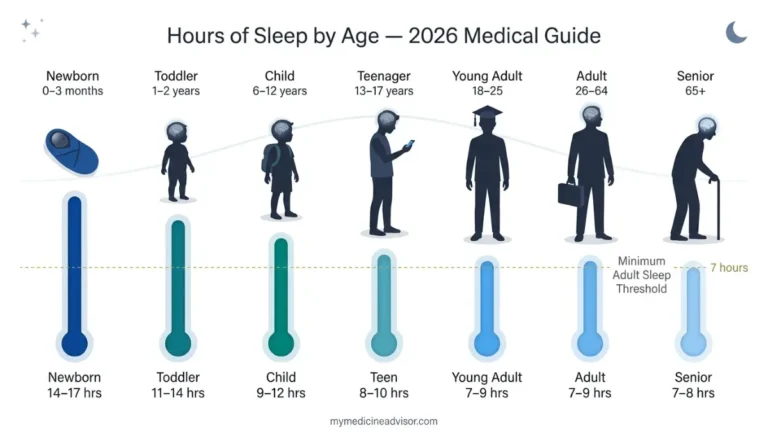
Chronic insomnia is defined as sleep difficulty occurring at least 3 nights per week for 3 or more months, accompanied by daytime impairment. If you meet these criteria, a clinical evaluation is warranted. See our guide on hours of sleep by age to benchmark your sleep against clinical norms.
11. Can improving sleep hygiene cure insomnia?
For mild, acute insomnia — yes. For chronic insomnia driven by medical conditions, medications, or deep-rooted anxiety, sleep hygiene alone is insufficient. It must be combined with trigger-specific treatment, ideally CBT-I. Think of sleep hygiene as the foundation, not the cure.
For more expert-verified health guidance, visit mymedicineadvisor.com.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.