On This Page – Quick Medical Summary
Melatonin is the fourth most popular natural supplement among American adults — and one of the most misunderstood. Millions take doses that are 5 to 20 times higher than their body naturally produces, at the wrong time, for the wrong reason.
This guide gives you the evidence-based facts: the correct dose by age and use case, the timing science most articles miss entirely, and the 2025 safety data that should change how you think about long-term use.
What Is Melatonin — And Does It Actually Make You Sleep?
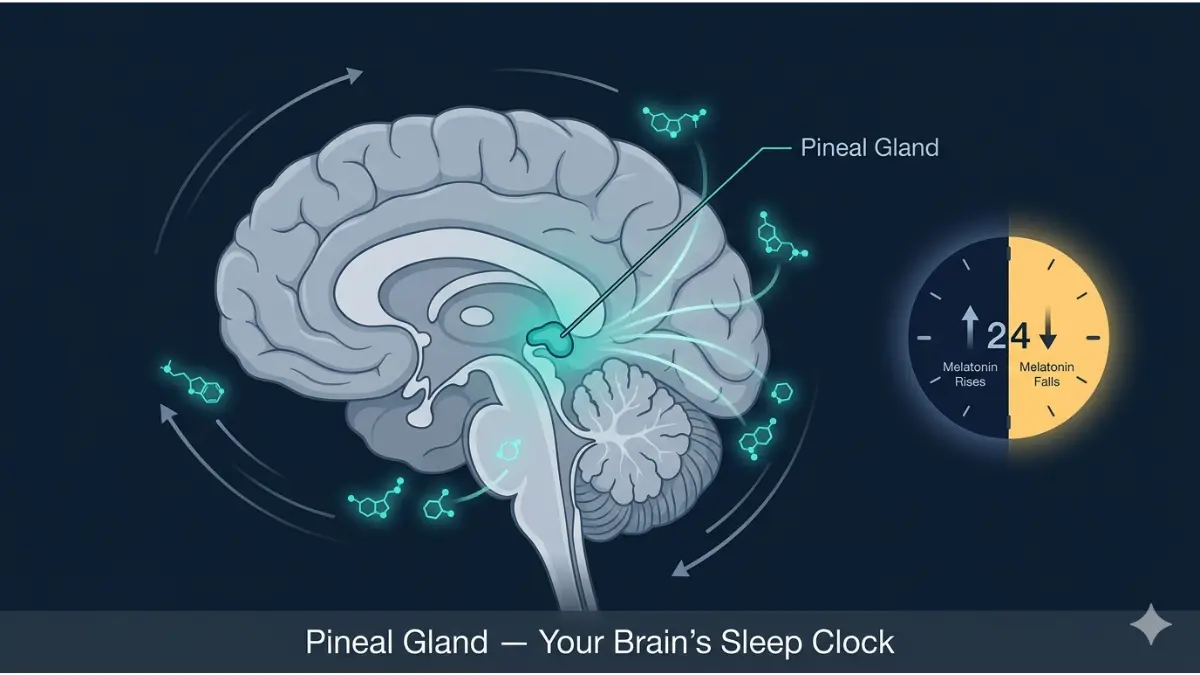
Melatonin is a hormone produced by the pineal gland — a pea-sized gland at the center of your brain. It doesn’t put you to sleep. It signals your body that sleep time is approaching.
Think of melatonin as your body’s biological sunset. As light fades in the evening, your brain ramps up melatonin production, telling every cell: “wind down, it’s night.” By early morning, production drops back to nearly zero.
Your Brain’s Natural Melatonin Schedule
- 6:00–8:00 PM: Melatonin begins rising as daylight fades
- 9:00–11:00 PM: Levels climb sharply, producing drowsiness
- 2:00–4:00 AM: Peak melatonin concentration
- 6:00–7:00 AM: Levels drop to near-zero; you wake feeling alert
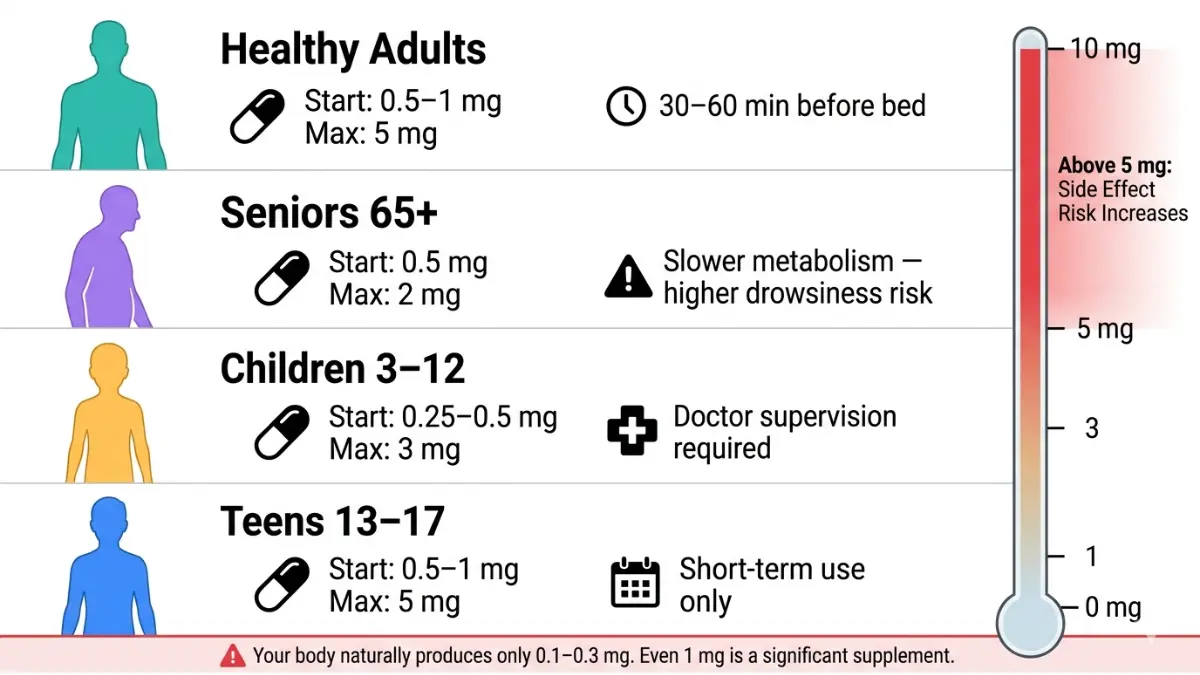
Your body naturally produces only about 0.1–0.3 mg of melatonin on its own. This matters enormously when you understand that most store-bought supplements start at 5mg — roughly 15 to 30 times your natural production.
Melatonin Is NOT a Sleeping Pill
This distinction is critical and all major competitors blur it. Melatonin does not sedate you. It shifts your internal clock. That’s why a 10mg dose doesn’t make you sleep twice as well — it often makes things worse by flooding your system far beyond what any natural signal requires.
If you’re struggling with deeper sleep issues, understanding what causes insomnia is an essential first step before reaching for any supplement. You can also use our Sleep Calculator to find your ideal sleep and wake windows based on your schedule.
To understand how your circadian biology actually drives sleep quality, see our detailed guide on what is circadian rhythm and sleep stages explained.
Melatonin Dosage — The Complete Age-by-Age, Use-Case Guide
Here is the fact no supplement company wants you to know: lower doses are almost always more effective than higher ones.
A 2024 dose-response meta-analysis published in the Journal of Pineal Research — covering 26 randomized controlled trials and 1,689 participants — found that melatonin’s sleep-promoting effects peaked at just 4 mg/day, with no additional benefit beyond that threshold.
The “Start Low, Go Slow” Principle
Your body produces roughly 0.3mg naturally. Even 0.5mg is a significant supplemental increase. Starting at 5mg or 10mg — as many gummy products are dosed — can overwhelm your system, cause next-day grogginess, and over time suppress your own melatonin production.
Start at 0.5–1 mg. Wait one week. Increase only if needed.
Master Melatonin Dosage Table (2026)
| Who | Starting Dose | Effective Range | Maximum | Notes |
|---|---|---|---|---|
| Healthy Adults | 0.5–1 mg | 1–3 mg | 5 mg | Escalate by 1mg weekly if needed |
| Seniors (65+) | 0.5 mg | 0.5–2 mg | 2 mg | Slower clearance; higher drowsiness risk |
| Children (ages 3–12) | 0.25–0.5 mg | 0.5–3 mg | 3 mg | Doctor supervision required |
| Teens (ages 13–17) | 0.5–1 mg | 1–3 mg | 5 mg | Short-term only; watch puberty timing |
| Jet Lag (eastward travel) | 0.5–3 mg | 1–3 mg | 5 mg | Timing is more important than dose |
| Shift Workers | 0.5–3 mg | 1–3 mg | 5 mg | Take 30–60 min before daytime sleep |
| Short-term Insomnia | 1–3 mg | 1–5 mg | 5 mg | CBT-I preferred; see below |
The Supplement Label Crisis — A Warning Every American Needs to See
A 2023 study published in JAMA tested 25 over-the-counter melatonin gummies. The findings were alarming:
- 88% of products were inaccurately labeled
- Actual melatonin content ranged from 74% to 347% of the stated dose
- Some products also contained undisclosed serotonin — a hormone with significant neurological effects
What this means for you: That “5mg” gummy you’re taking could contain anywhere from 3.7mg to over 17mg of actual melatonin. If you’re unsure about what’s in your supplement, use our Pill Identifier to verify the form and look for USP-verified or NSF-certified brands only.
According to the National Center for Complementary and Integrative Health (NCCIH) at the NIH, melatonin is classified as a dietary supplement in the US — meaning it is regulated far less strictly than pharmaceutical drugs by the FDA.
When to Take Melatonin — The Timing Science Competitors Ignore
Most melatonin guides tell you: “Take it 30 minutes before bed.”
A landmark 2024 meta-analysis says that advice may be costing you results.
The Research-Backed Timing Revelation
Researchers at the University of Pisa analyzed 26 randomized controlled trials and built dose-response models to identify the optimal melatonin schedule. Their conclusion, published in the Journal of Pineal Research:
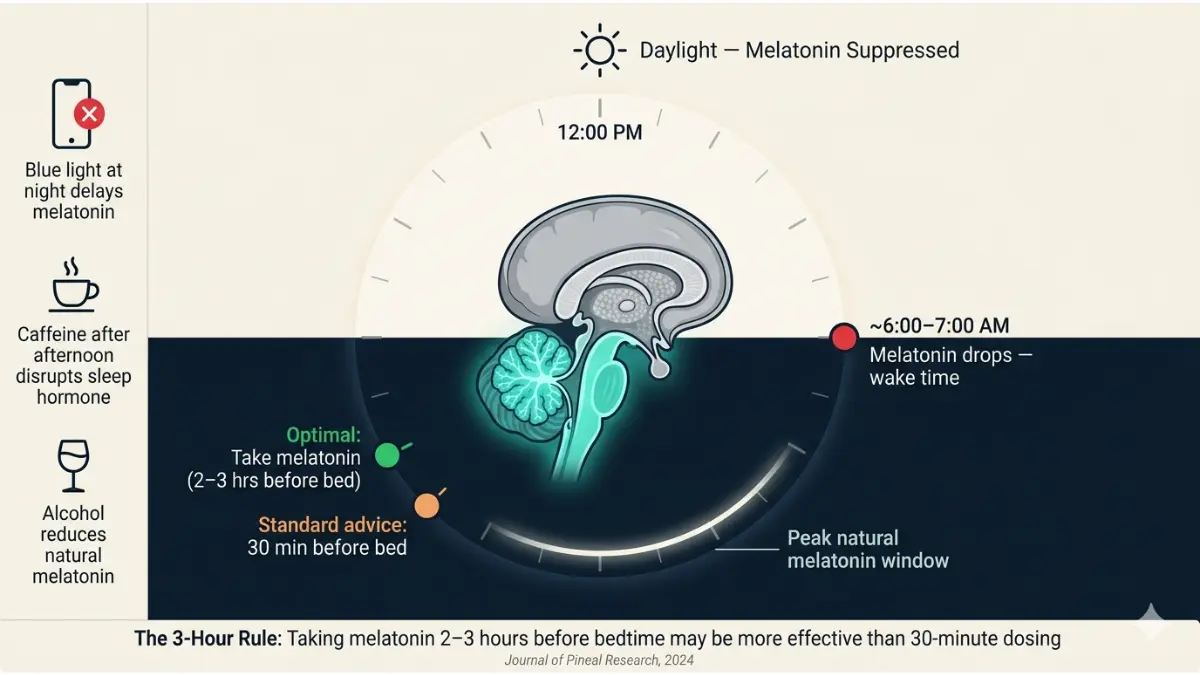
Taking melatonin 2–3 hours before your target bedtime — not 30 minutes — produces significantly better reductions in sleep onset latency.
The standard clinical practice of “2mg, 30 minutes before bed” was compared against an optimized protocol of “4mg, taken 3 hours earlier.” The optimized protocol outperformed across sleep onset and total sleep time metrics.
Timing Guide by Use Case
| Situation | Optimal Timing | Notes |
|---|---|---|
| General insomnia | 1–2 hours before target bedtime | Earlier = more effective circadian shift |
| Delayed sleep phase | 2–3 hours before desired bedtime | The biggest timing gap needed |
| Jet lag — eastward flights | Day of arrival at local bedtime | Continue for 3–4 nights |
| Jet lag — westward flights | At new local bedtime, night 1–2 only | Less critical than eastward |
| Shift work (daytime sleep) | 30–60 min before your sleep window | Use blackout curtains too |
| Surgery anxiety | As directed by physician | Do not self-dose |
The Hidden Timing Saboteur: Blue Light
You can take melatonin at the perfect time and still undermine it completely. Blue light emitted from phones, tablets, and TVs suppresses your brain’s natural melatonin production — and it works fast.
Research shows that just 2 hours of evening screen use can delay melatonin onset by up to 3 hours. If you take a 1mg supplement at 9pm but scroll your phone until 10:30pm, you’ve largely cancelled the effect.
Practical rule: Stop screen use at least 60–90 minutes before your target sleep time. If you must use devices, enable night mode and reduce brightness to minimum.
Our guide on does caffeine disrupt sleep covers another major timing saboteur worth understanding alongside melatonin use.
Melatonin Safety — Side Effects, Drug Interactions & the 2025 Heart Warning
Short-term melatonin use at low doses is well-tolerated by most healthy adults. But three areas demand your attention in 2026: common side effects, drug interactions, and critical new long-term safety data.
Common Side Effects (Short-Term Use)
Most side effects occur at doses above 3mg and include:
- Morning grogginess — the most common complaint; often a sign your dose is too high
- Vivid dreams or nightmares — particularly at doses ≥5mg
- Headache and dizziness — especially in sensitive individuals
- Nausea — typically dose-dependent
- Daytime drowsiness — the Mayo Clinic advises not driving within 5 hours of taking melatonin
The melatonin “hangover” is a real phenomenon. High-dose supplements stay active in the bloodstream far longer than your body’s natural hormone does — causing lingering sedation the next morning.
Drug Interactions — A Critical Safety Table
Melatonin interacts with several common medications. If you take any of the following, consult your doctor before using melatonin:
| Medication Class | Interaction | Action Required |
|---|---|---|
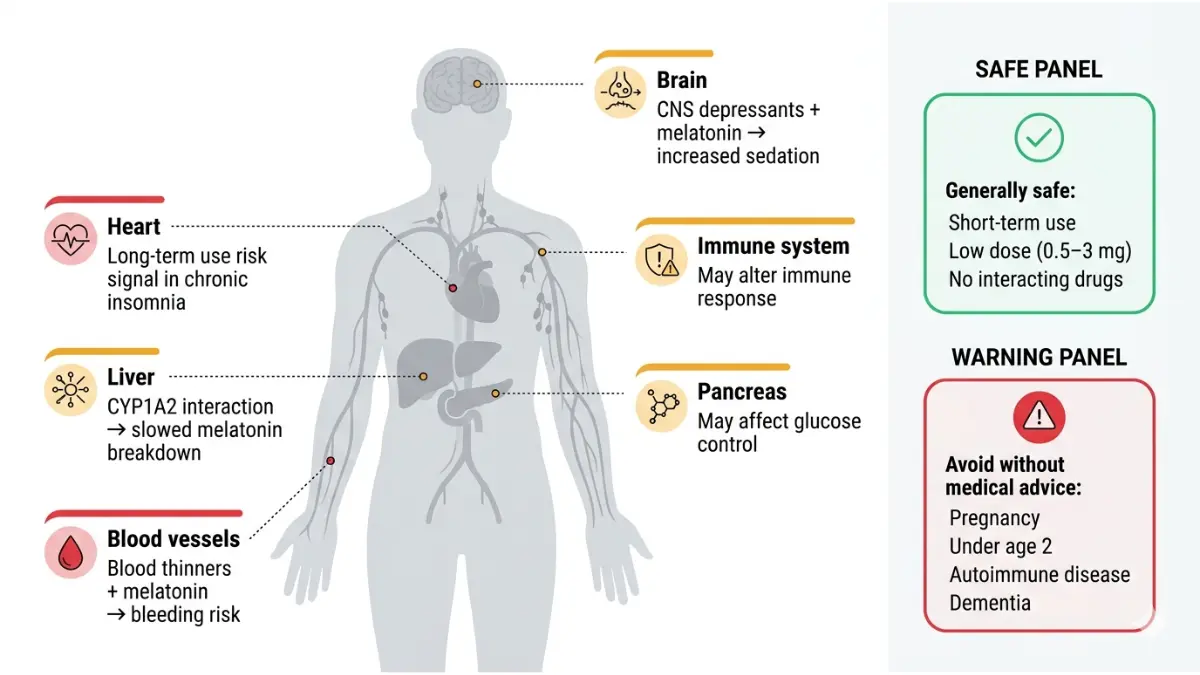
| Blood thinners (e.g., warfarin) | Increased bleeding risk | Avoid or monitor under supervision |
| Diabetes medications (insulin, metformin) | May alter blood glucose control | Doctor supervision required |
| Blood pressure drugs | May worsen hypertension in some | Use with caution; monitor BP |
| Immunosuppressants | Melatonin may stimulate immune response | Avoid |
| Oral contraceptives | Additive sedation; may raise melatonin levels | Use minimum effective dose |
| CNS depressants (benzodiazepines, sedatives) | Compounding sedation risk | Avoid combination |
| Fluvoxamine (Luvox, for OCD) | Dramatically increases melatonin blood levels | Avoid |
| Seizure medications | May lower seizure threshold | Avoid without medical supervision |
For a broader view of supplement and medication interactions, see our drug interactions list.
🚨 The 2025 AHA Heart Failure Finding — What It Actually Means
In November 2025, researchers presented preliminary findings at the American Heart Association’s Scientific Sessions in New Orleans that sent shockwaves through the sleep medicine community.
The study reviewed 5 years of electronic health records from 130,828 adults with chronic insomnia. Key findings:
- Adults using melatonin for 1+ year were more likely to develop heart failure than non-users
- Those taking melatonin long-term were 3.5 times more likely to be hospitalized for heart failure
- All-cause mortality risk was also elevated in the long-term melatonin group
Critical context: This study is observational and has not yet been peer-reviewed. Several sleep experts note that the elevated risk likely reflects the consequences of untreated chronic insomnia itself — which is already linked to cardiovascular disease — rather than melatonin directly.
Bottom line: This data does not prove melatonin causes heart failure. But it is a strong signal that long-term use requires medical oversight and that treating the underlying sleep disorder matters more than masking it with supplements.
When Melatonin Won’t Work — And What Actually Does
This is the section no supplement company wants published. For millions of Americans, melatonin will not solve your sleep problem — and continuing to use it may delay the treatment that actually works.
Melatonin’s Evidence Gap for Chronic Insomnia
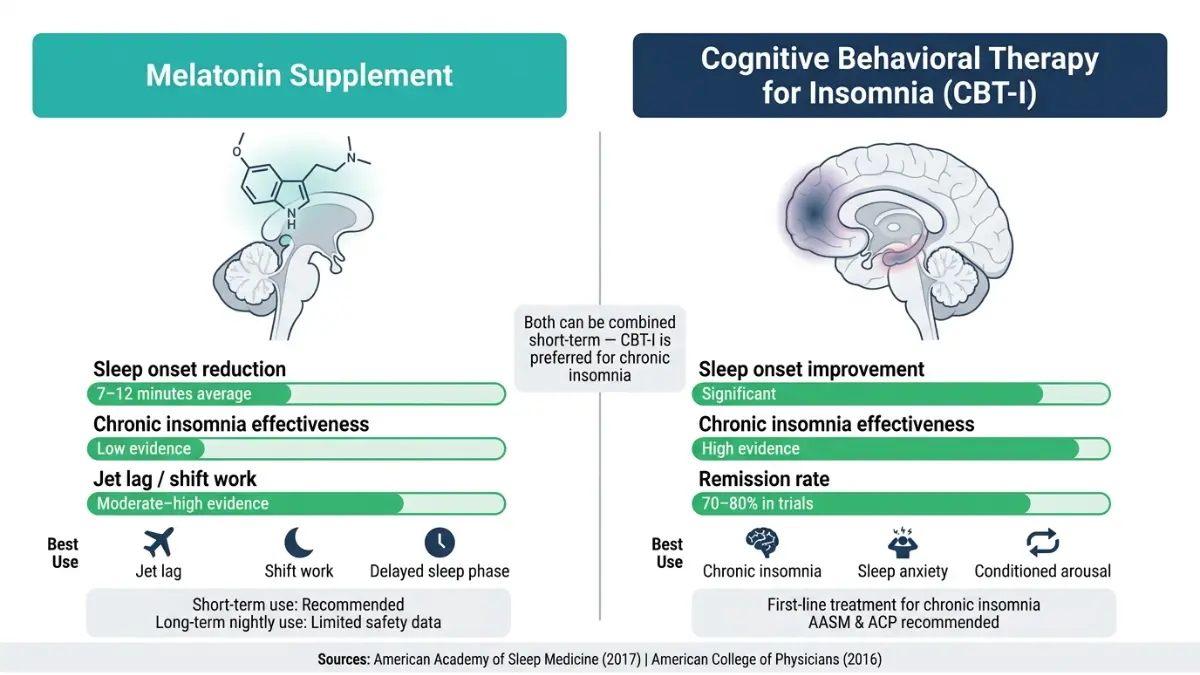
Both the American Academy of Sleep Medicine (2017) and the American College of Physicians (2016) concluded there is insufficient evidence to recommend melatonin for chronic insomnia.
Chronic insomnia — defined as trouble sleeping 3+ nights per week for 3+ months — has psychological and behavioral drivers that melatonin cannot address. A supplement that shifts your circadian clock by 20–30 minutes does nothing for the racing thoughts, conditioned arousal, or sleep anxiety driving your insomnia.
CBT-I: The Treatment That Actually Works
Cognitive Behavioral Therapy for Insomnia (CBT-I) is the most effective treatment for chronic insomnia, with remission rates of 70–80% in clinical trials — far exceeding any sleep medication or supplement.
CBT-I targets the thought patterns and behaviors that perpetuate insomnia. It requires 4–8 sessions with a trained therapist or a validated digital program. Our detailed guide on cognitive behavioral therapy for insomnia covers exactly how it works and where to access it in the US.
For those considering prescription options, see our evidence-based review of sleep medications — including how they compare to melatonin and CBT-I.
Non-Negotiable Sleep Hygiene Principles
Before any supplement, these evidence-backed behaviors improve sleep quality for most people:
- Consistent sleep and wake time — even on weekends; the most powerful circadian reset tool available
- No screens 60–90 minutes before bed — blue light suppresses melatonin production regardless of what supplement you take
- Cool, dark bedroom — optimal sleep temperature is 60–67°F (15–19°C)
- Caffeine cutoff at 2pm — caffeine has a 5–7 hour half-life; that 3pm coffee is still 50% active at 8pm
- No alcohol as a sleep aid — alcohol reduces natural melatonin production by up to 20% and fragments REM sleep
- Eating cutoff 2–3 hours before bed — late eating raises core body temperature, disrupting sleep onset; use our Intermittent Fasting Calculator to structure an eating window that supports your sleep
If you’re waking frequently through the night, the problem may be more than melatonin can address — explore warning signs of a sleep disorder to know when to seek professional evaluation.
The Evidence-Based Melatonin Protocol — Expert Summary
Our expert panel at mymedicineadvisor.com has reviewed the current literature and synthesized the following clinical guidance for US adults in 2026.
The Melatonin Protocol That Works
| Step | Action |
|---|---|
| Dose | Start at 0.5–1mg. Increase by 1mg weekly only if needed. Stay at or below 5mg. |
| Timing | Take 1–2 hours before your target bedtime (3 hours for delayed sleep phase) |
| Duration | Maximum 1–2 months continuously. Reassess after stopping. |
| Quality | Choose USP Verified or NSF Certified supplements only. |
| Screen use | Stop all blue-light screens 60–90 minutes before your target sleep time |
| Alcohol | Avoid on nights you take melatonin — it directly counteracts it |
✅ Melatonin Works Best For:
- Jet lag (especially eastward travel)
- Shift work disorder
- Delayed sleep-wake phase disorder
- Short-term insomnia (situational, not chronic)
- Circadian rhythm disorders in blind individuals
❌ Melatonin Is Unlikely to Help With:
- Chronic insomnia lasting 3+ months
- Sleep maintenance (waking in the middle of the night)
- Sleep apnea — this requires medical evaluation; see how sleep apnea is diagnosed
- Depression-related sleep disruption; explore our guide on does depression cause sleep problems
Who Should NOT Use Melatonin Without Medical Supervision:
- Pregnant or breastfeeding women (safety data does not exist)
- Children under age 2
- Adults with autoimmune conditions
- Anyone with dementia (AASM advises against it)
- Anyone on blood thinners, immunosuppressants, or seizure medications
For comprehensive sleep health resources, visit our health library or use our Symptom Checker if you’re experiencing unusual symptoms alongside sleep disruption.
For authoritative clinical guidance, the NCCIH at the National Institutes of Health maintains an up-to-date evidence summary on melatonin that we recommend bookmarking.
Frequently Asked Questions About Melatonin
1. How much melatonin should I take for sleep?
Start with 0.5–1mg, taken 1 hour before your target bedtime. Most adults achieve good results at 1–3mg. Rarely exceed 5mg.
2. When is the best time to take melatonin?
1–2 hours before your intended sleep time. For delayed sleep phase disorder, research supports taking it 2–3 hours before desired bedtime for maximum effectiveness.
3. Can I take melatonin every night?
Short-term use of 1–2 months appears safe for most adults. There is insufficient data on the safety of nightly long-term use, and the 2025 AHA study adds reason for caution.
4. Is 10mg of melatonin too much?
For almost everyone, yes. High doses cause grogginess, vivid nightmares, and may suppress your body’s natural melatonin production over time. Start low.
5. Does melatonin work for insomnia?
It reduces sleep onset time by 7–12 minutes on average — modest benefit. For chronic insomnia, CBT-I is the evidence-based first-line treatment, not melatonin.
6. Can children take melatonin?
Only under a doctor’s supervision. Starting dose: 0.25–0.5mg. Never give to children under 2. Concerns exist about effects on puberty timing with long-term pediatric use.
7. Does melatonin interact with medications?
Yes — significantly with blood thinners, diabetes medications, blood pressure drugs, antidepressants (especially fluvoxamine), and seizure medications. Always inform your doctor.
8. What happens if you take too much melatonin?
Next-day grogginess, vivid nightmares, headache, and nausea are common. Chronically high doses may suppress your own natural production, worsening sleep long-term.
9. Is melatonin safe during pregnancy?
Safety data does not exist. Avoid during pregnancy and breastfeeding unless specifically directed by your OB-GYN.
10. How long does melatonin take to work?
Most people notice effects within 30–60 minutes. Lower doses (0.5–1mg) often take effect faster than high doses because they more closely mirror your body’s natural signal.
11. Can long-term melatonin use affect your heart?
A preliminary 2025 study presented at the American Heart Association found an association between 1+ year of melatonin use and elevated heart failure risk in people with chronic insomnia. The research is not yet peer-reviewed and does not prove causation — but it underscores that melatonin is not risk-free for chronic long-term use.
This article is for educational purposes only and does not constitute medical advice. If you are experiencing persistent sleep problems, please consult a licensed healthcare provider.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.