On This Page – Quick Medical Summary
When James, a 48-year-old contractor from Ohio, heard “Stage 2 melanoma,” he immediately assumed the worst. His dermatologist’s next sentence stopped him cold: “We caught it before it reached your lymph nodes. Your 5-year survival odds are above 80%.”
Melanoma staging is not a verdict. It is a map.
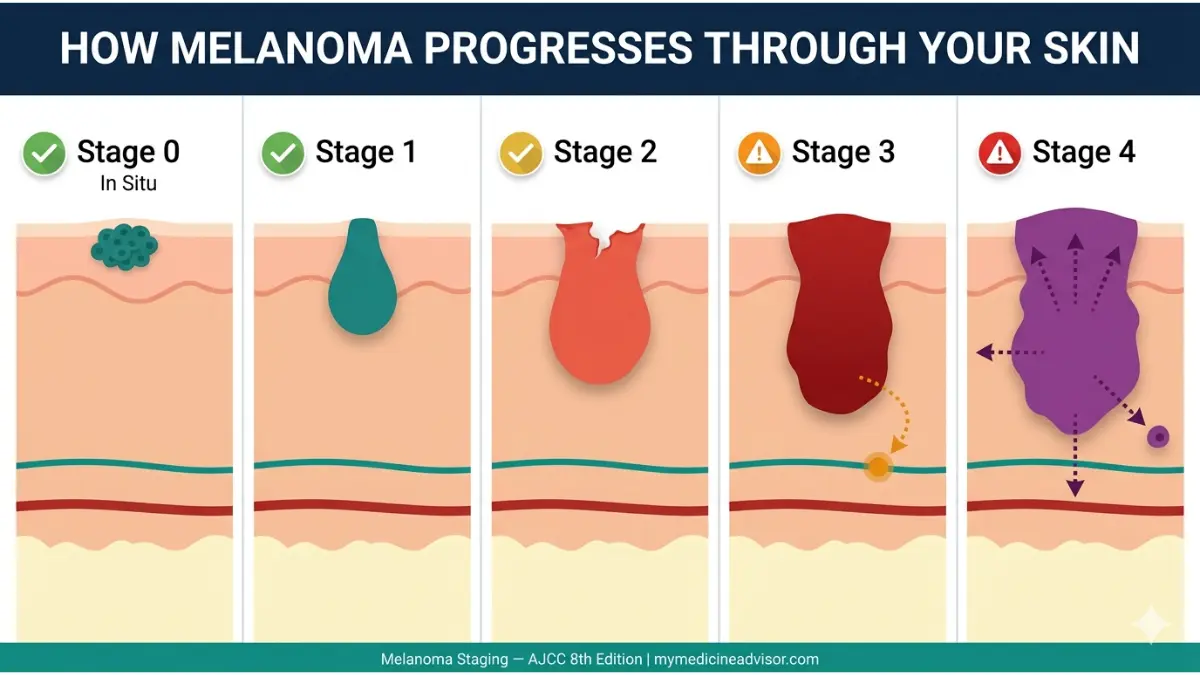
Melanoma is staged from 0 to 4 based on three core factors: how deep the tumor has grown, whether cancer cells have reached nearby lymph nodes, and whether the cancer has spread to distant organs. Stage 0 is nearly 100% curable. Even Stage 4 — once considered a death sentence — now carries 5-year survival rates exceeding 50% in patients treated with modern combination immunotherapy, according to 2026 data from the NCI’s SEER database.
Use our Symptom Checker if you’ve noticed unusual skin changes — early detection is the single most powerful factor in melanoma outcomes.
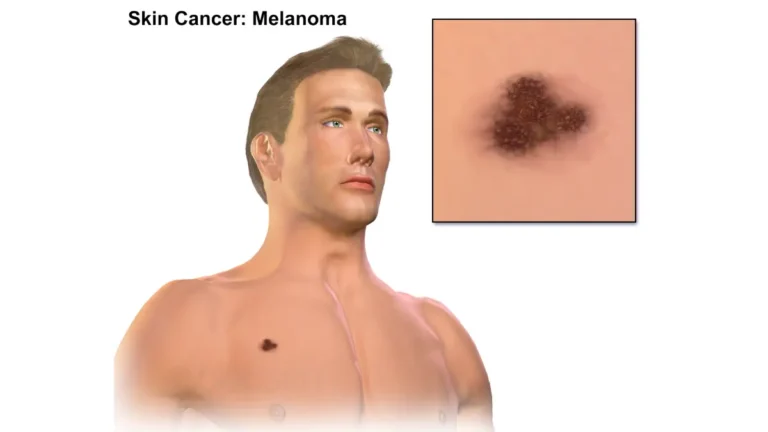
What Is Melanoma Staging — And Why It Changes Everything
The AJCC Staging System, Decoded Simply
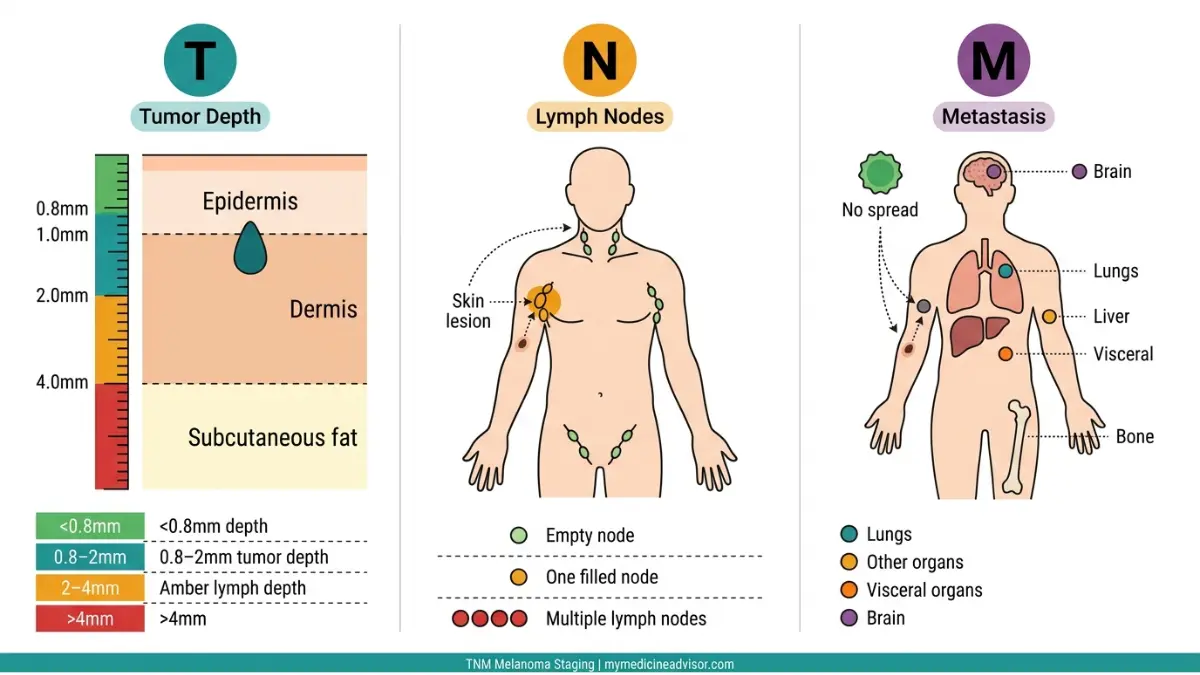
Doctors use the AJCC (American Joint Committee on Cancer) 8th Edition system to stage melanoma. Every stage is built on three measurements, summarized as TNM:
| Factor | What It Means | Why It Matters |
|---|---|---|
| T (Tumor) | Depth and thickness of the primary tumor | Deeper = more aggressive |
| N (Nodes) | Whether cancer reached nearby lymph nodes | Signals regional spread |
| M (Metastasis) | Whether cancer spread to distant organs | Determines advanced stage |
The NCI’s complete cancer staging guide explains how TNM scores combine to produce a final stage number from 0 to 4.
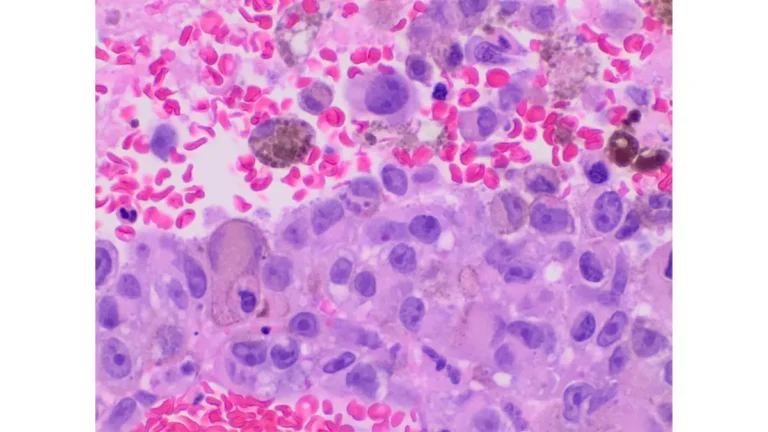
The 3 Factors That Determine Your Melanoma Stage
- Breslow thickness — measured in millimeters, how deep the tumor penetrates skin layers
- Ulceration — whether the tumor surface has broken down (increases stage severity)
- Sentinel lymph node status — whether the first draining lymph node tests positive for cancer cells
What This Means For You: Your stage is not determined by how a mole “looks.” It requires a biopsy, pathology report, and sometimes a sentinel lymph node biopsy. Read our full guide on how melanoma is diagnosed to understand every step of that process.
If you have a family history of melanoma, use our Genetic Risk Assessment Tool to evaluate your personal risk profile before your next dermatology appointment.
Melanoma Stage 0 and Stage 1 — The Early Stages
Stage 0 Melanoma (Melanoma In Situ) — Confined, Curable, Critical to Catch
Stage 0 means the cancer is entirely within the top layer of the skin (epidermis). It has not invaded deeper tissue, has not touched a blood vessel, and has zero lymph node involvement.
- Treatment: Wide local excision with clear margins
- 5-year survival rate: ~99–100%
- Recurrence risk: Low, but annual skin checks remain essential
The American Academy of Dermatology confirms that Stage 0 melanoma, when fully excised, is among the most successfully treated cancers in existence.
What This Means For You: If your biopsy returns Stage 0, surgery alone is almost always curative. Your most important next step is establishing a lifelong annual skin surveillance schedule with a board-certified dermatologist.
Stage 1 Melanoma — Thin Tumors, Excellent Outcomes
Stage 1 melanoma has invaded deeper skin layers but has not spread to lymph nodes or distant organs.
| Substage | Breslow Thickness | Ulceration | 5-Year Survival |
|---|---|---|---|
| Stage 1A | < 0.8mm | No | ~97–98% |
| Stage 1B | 0.8–2.0mm | Possibly | ~92–95% |
Treatment approach:
- Wide local excision (primary surgery)
- Sentinel lymph node biopsy (SLNB) — recommended for Stage 1B to check microscopic spread
- No routine adjuvant therapy for most Stage 1A patients
What This Means For You: Stage 1 melanoma is highly survivable with prompt surgical treatment. The key risk factor to discuss with your oncologist is whether SLNB is indicated based on your specific Breslow thickness and mitotic rate.
Bold Takeaway: Melanoma caught at Stage 0 or 1 is among the most survivable cancers in existence. Annual skin checks — and knowing the ABCDE warning signs of melanoma — are the difference between Stage 0 and Stage 3.
Melanoma Stage 2 and Stage 3 — The Critical Middle Ground
Stage 2 Melanoma — Deeper, But Still Localized
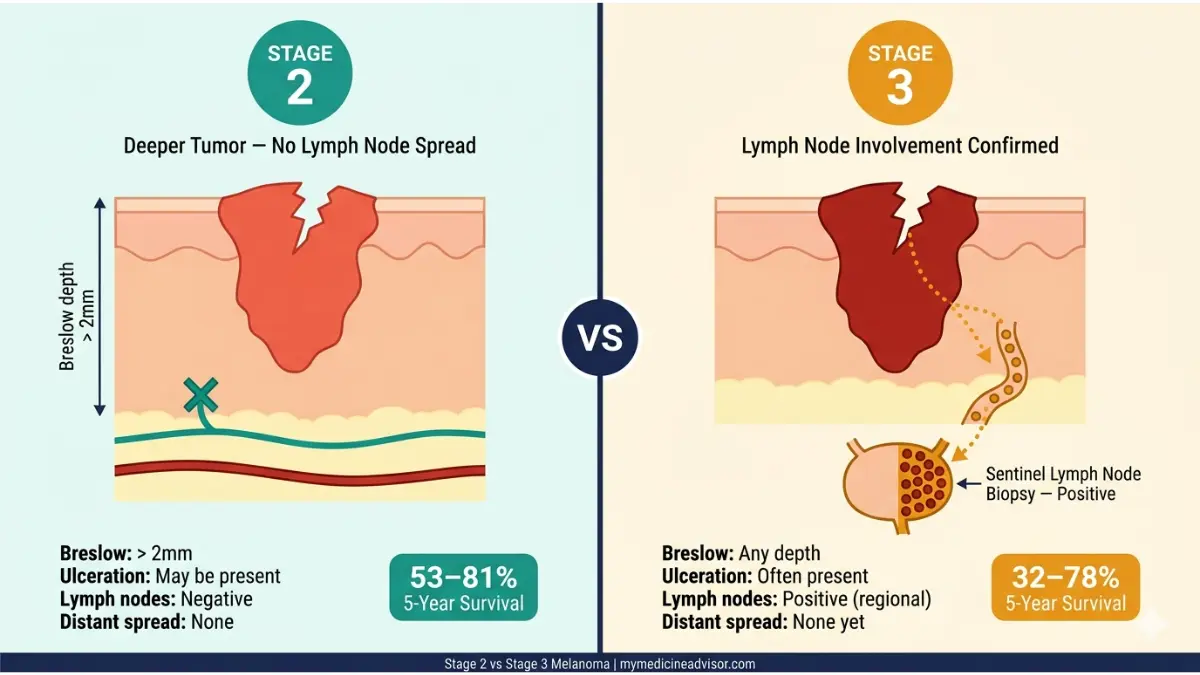
Stage 2 melanoma is thicker than Stage 1 and may show ulceration, but crucially — it has not yet reached lymph nodes. This localized status is what keeps survival odds relatively strong.
| Substage | Breslow Thickness | Ulceration | 5-Year Survival |
|---|---|---|---|
| Stage 2A | 1.0–2.0mm (ulcerated) or 2.0–4.0mm | No | ~81% |
| Stage 2B | 2.0–4.0mm (ulcerated) or > 4.0mm | No | ~70% |
| Stage 2C | > 4.0mm | Yes | ~53–65% |
Treatment at Stage 2:
- Wide local excision with 2cm margins
- Sentinel lymph node biopsy — strongly recommended
- Adjuvant immunotherapy (pembrolizumab) is now FDA-approved for high-risk Stage 2 patients as of 2022, reflecting improved understanding of recurrence risk
According to the American Cancer Society’s melanoma staging resource, Stage 2C has a meaningfully higher recurrence risk, making close surveillance critical.
What This Means For You: At Stage 2, the conversation with your oncologist must include adjuvant therapy eligibility. Don’t accept a “wait and see” approach without discussing pembrolizumab trials for Stage 2C.
Stage 3 Melanoma — When Lymph Nodes Are Involved
Stage 3 is a turning point. Cancer has spread to nearby lymph nodes or lymphatic vessels — but has not yet reached distant organs. This is where treatment intensity escalates significantly.
Stage 3 has four substages (3A, 3B, 3C, 3D) determined by the number of lymph nodes involved, microscopic vs. macroscopic spread, and whether satellite lesions are present.
Treatment options for Stage 3 melanoma:
- Complete lymph node dissection (in selected cases)
- Adjuvant immunotherapy: Nivolumab or pembrolizumab for 12 months post-surgery
- Targeted therapy: Dabrafenib + trametinib for BRAF V600E-mutated tumors
- Radiation therapy for high-risk regional disease
2026 survival data by substage:
| Stage 3 Substage | 5-Year Survival Rate |
|---|---|
| 3A | ~78% |
| 3B | ~59% |
| 3C | ~40–48% |
| 3D | ~32% |
Source: SEER Cancer Statistics, 2026 Update
💬 Expert Perspective: Dr. Alexander van Houten, Oncology, Netherlands Cancer Institute: “Stage 3 melanoma patients who receive adjuvant pembrolizumab now show relapse-free survival improvements of 35–40% compared to observation alone. Immunotherapy has fundamentally changed what Stage 3 means.”
What This Means For You: Stage 3 melanoma is not a death sentence. The Melanoma Research Foundation’s stage guide outlines patient-specific treatment decision trees that your oncologist should walk through with you.
Learn more about how melanoma warning signs and symptoms can appear differently at each stage — especially when lymph node involvement begins.
Melanoma Stage 4 — Advanced Disease, New Hope
What “Metastatic Melanoma” Actually Means
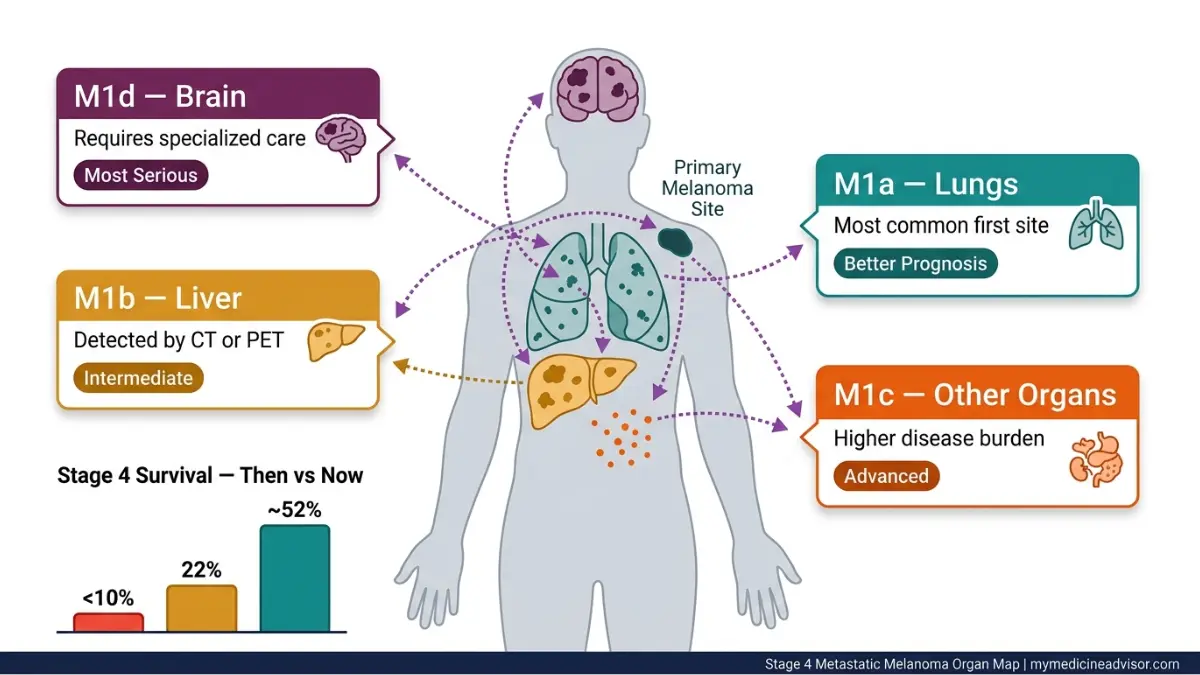
Stage 4 melanoma means cancer has spread beyond the lymph nodes to distant organs. The most common metastatic sites are:
- Lungs (M1a — best prognosis in Stage 4)
- Liver, abdomen (M1b)
- Other organs (M1c)
- Brain (M1d — most complex to treat)
Symptoms at Stage 4 may include unexplained weight loss, persistent headaches, shortness of breath, and fatigue — though some patients remain asymptomatic early in distant metastasis.
Stage 4 Melanoma Survival Rates — The 2026 Reality
This is the statistic that changes everything for newly diagnosed patients:
| Era | Stage 4 Median Survival | 5-Year Survival |
|---|---|---|
| Pre-2011 (chemotherapy era) | 6–9 months | < 10% |
| 2015–2019 (early immunotherapy) | 18–24 months | ~22% |
| 2024–2026 (combination immunotherapy) | >3 years | ~50–52% |
The combination of ipilimumab + nivolumab (CheckMate 067 trial, 10-year follow-up) now shows 10-year survival rates approaching 43% in Stage 4 patients — a figure that was unimaginable just 15 years ago.
The NIH’s research summary on combination immunotherapy documents this landmark shift in metastatic melanoma outcomes.
Treatment Options for Stage 4 Melanoma in 2026
1. Checkpoint Inhibitor Immunotherapy
- Nivolumab (Opdivo) + Ipilimumab (Yervoy) — first-line combination
- Pembrolizumab (Keytruda) — monotherapy or combination
2. Targeted Therapy (BRAF-mutated tumors only)
- ~50% of melanomas carry a BRAF V600E mutation
- Dabrafenib + trametinib: rapid tumor shrinkage, but resistance develops in most patients
- Use our Pill Identifier to look up any melanoma medication your oncologist prescribes
3. Clinical Trials
- CAR-T cell therapy for melanoma is in Phase 2 trials as of 2026
- TIL (tumor-infiltrating lymphocyte) therapy received FDA breakthrough designation
- Search active trials at ClinicalTrials.gov melanoma listings
4. Brain Metastasis (M1d) Treatment
- Stereotactic radiosurgery (SRS) + immunotherapy combination
- Significantly improved M1d outcomes since 2022
Our dedicated guide to Stage 4 melanoma survival and therapy options covers every 2026-approved treatment pathway in full detail.
What This Means For You: If you or a loved one has been diagnosed with Stage 4 melanoma, ask your oncologist specifically about: (1) BRAF mutation testing, (2) PD-L1 expression level, and (3) eligibility for combination immunotherapy. These three questions could change your treatment path entirely.
🔑 Bold Takeaway: Stage 4 melanoma survival has improved more in the past 10 years than in the previous 50 combined. A 2026 diagnosis carries meaningfully different odds than a 2015 diagnosis.
Melanoma Staging Master Reference Table + Progression Timeline
The Complete 2026 Melanoma Stages at a Glance
| Stage | Substages | Tumor Depth | Lymph Nodes | Distant Spread | 5-Year Survival | Primary Treatment |
|---|---|---|---|---|---|---|
| 0 | In Situ | Epidermis only | No | No | ~100% | Excision |
| 1 | 1A, 1B | < 2mm | No | No | 92–98% | Surgery ± SLNB |
| 2 | 2A, 2B, 2C | > 2mm | No | No | 53–81% | Surgery + Adjuvant |
| 3 | 3A, 3B, 3C, 3D | Any | Regional | No | 32–78% | Surgery + Immunotherapy |
| 4 | M1a–M1d | Any | Any | Yes | ~25–52% | Immunotherapy + Targeted |
Data sourced from SEER Program, National Cancer Institute and AJCC 8th Edition guidelines.
How Fast Does Melanoma Progress Between Stages?
This is one of the most searched questions on Google — and one that almost no competitor answers directly.
The honest answer: Progression speed depends on melanoma subtype.
- Superficial spreading melanoma (most common, ~70% of cases): Can remain in Stage 0–1 for months to years before invasive growth
- Nodular melanoma (~15% of cases): Can progress from Stage 1 to Stage 3 in weeks to months — this subtype is the most dangerous due to rapid vertical growth
- Lentigo maligna melanoma: Very slow-growing; often Stage 0 for years in older patients
- Acral lentiginous melanoma: More common in darker skin tones; often diagnosed at later stages due to atypical locations
What This Means For You: If your biopsy returns nodular melanoma histology, your oncologist should prioritize expedited staging workup. Delays are costlier for this subtype than any other.
Review the latest melanoma statistics for 2026 including subtype incidence breakdowns and demographic survival disparities.
The ASCO Cancer.net staging guide provides the clinical framework oncologists use to restage patients after systemic therapy begins.
Just Diagnosed? Your Stage-by-Stage Action Plan
Questions to Ask Your Oncologist — By Stage Group
For Stage 0 and Stage 1:
- What is my exact Breslow thickness and mitotic rate?
- Is sentinel lymph node biopsy recommended in my case?
- What surveillance schedule do you recommend post-surgery?
- What are my recurrence risk factors?
For Stage 2 and Stage 3:
- Am I eligible for adjuvant pembrolizumab or nivolumab?
- Should I be tested for BRAF V600E mutation?
- What imaging surveillance (CT, PET, MRI) do you recommend and how often?
- Are there clinical trials I should consider?
For Stage 4:
- What are my PD-L1 expression results?
- Do I have a BRAF mutation — and if so, should I start targeted therapy or immunotherapy first?
- Is combination ipilimumab + nivolumab appropriate for my case?
- Are there brain metastasis-specific protocols I need?
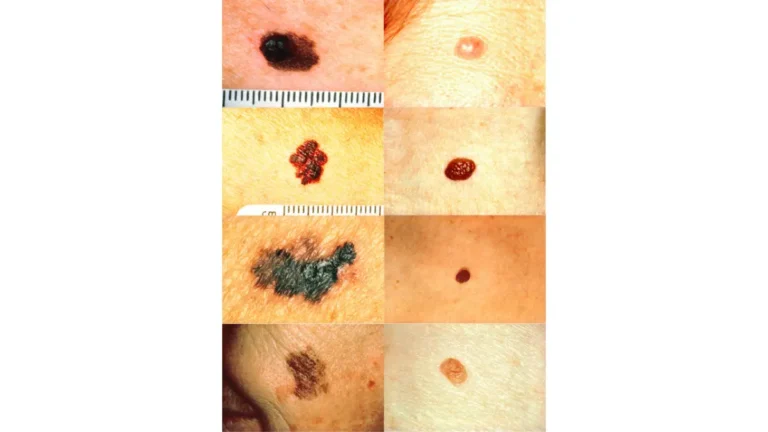
The ABCDE Rule — Your First Line of Defense
Before staging, detection comes first. The ABCDE rule identifies suspicious moles that warrant immediate dermatologist review:
- A — Asymmetry: One half doesn’t match the other
- B — Border: Irregular, ragged, or blurred edges
- C — Color: Multiple shades of brown, black, red, or white within one lesion
- D — Diameter: Larger than 6mm (about the size of a pencil eraser)
- E — Evolution: Any change in size, shape, color, or new symptoms like bleeding
The Skin Cancer Foundation’s melanoma awareness resource provides photographic examples of each ABCDE criterion — bookmarking it is strongly recommended.

Follow-Up Schedule After Melanoma Treatment
| Stage | Year 1 | Years 2–5 | Year 5+ |
|---|---|---|---|
| Stage 0–1 | Every 6 months | Annually | Annually |
| Stage 2 | Every 3–4 months | Every 6 months | Annually |
| Stage 3 | Every 3 months | Every 3–4 months | Every 6 months |
| Stage 4 | Every 6–8 weeks | Every 3 months | Every 3–6 months |
Follow-up typically includes physical exam, dermoscopy, and imaging (CT/PET) for Stage 3–4 patients.
Understanding whether melanoma has a hereditary component is critical for first-degree relatives of diagnosed patients — CDKN2A gene mutations significantly elevate familial risk.
For a comprehensive overview of everything from early symptoms to treatment pathways, our complete melanoma guide is your definitive starting point.
What This Means For You: Your melanoma stage is a starting point, not a finish line. The single most important thing you can do today — at any stage — is establish care with a melanoma specialist, not just a general oncologist. Specialized centers have access to trials, combination protocols, and expertise that general practices do not.
The NCI’s melanoma treatment PDQ is updated regularly and outlines every evidence-based treatment option by stage — it is required reading for any newly diagnosed patient or caregiver.
💙 “Your stage is not your story. It is your starting point. The tools available in 2026 are unlike anything patients had a decade ago — and they are improving every year.”
Frequently Asked Questions About Melanoma Stages
Q1: What are the stages of melanoma?
Melanoma has five stages: Stage 0 (in situ, epidermis only), Stage 1 (thin, localized), Stage 2 (deeper, still localized), Stage 3 (lymph node involvement), and Stage 4 (distant metastasis).
Q2: Is Stage 4 melanoma always fatal?
No. Thanks to combination immunotherapy, 5-year survival for Stage 4 melanoma now exceeds 50% in some patient groups — a dramatic improvement from under 10% in the pre-2011 chemotherapy era.
Q3: What is the survival rate for each melanoma stage?
Stage 0: ~100% | Stage 1: ~92–98% | Stage 2: ~53–81% | Stage 3: ~32–78% | Stage 4: ~25–52%. Rates vary by substage and treatment received.
Q4: How quickly can melanoma progress from Stage 1 to Stage 4?
It depends on the subtype. Nodular melanoma can progress rapidly — within weeks to months. Superficial spreading melanoma may remain early-stage for years. Any changing lesion warrants urgent evaluation.
Q5: What does Stage 3 melanoma mean for life expectancy?
Stage 3A carries a 78% 5-year survival rate. Stage 3D is closer to 32%. Modern adjuvant immunotherapy has significantly improved all Stage 3 substage outcomes since 2019.
Q6: Can Stage 0 melanoma come back after treatment?
It can recur locally or as a new primary melanoma. Annual full-body skin examinations are essential for all patients, even those treated for Stage 0.
Q7: What is the difference between Stage 2 and Stage 3 melanoma?
The key difference is lymph node involvement. Stage 2 is localized to the primary tumor site. Stage 3 means cancer has spread to at least one regional lymph node.
Q8: What is TNM staging in melanoma?
TNM stands for Tumor depth (T), lymph Node status (N), and distant Metastasis (M). These three scores are combined to assign a final AJCC stage from 0 to 4.
Q9: How does a doctor determine my melanoma stage?
Through biopsy (Breslow thickness measurement), sentinel lymph node biopsy (SLNB), and imaging studies (CT, PET scan, MRI) to assess for distant spread.
Q10: What new melanoma treatments are available in 2026?
TIL (tumor-infiltrating lymphocyte) therapy received FDA Breakthrough Device designation. CAR-T cell therapy trials for melanoma are in Phase 2. Combination immunotherapy protocols continue to improve Stage 4 outcomes. Check active trials at ClinicalTrials.gov.
Q11: Is melanoma staging the same across all skin tones?
The AJCC staging system is universal, but presentation differs. Acral lentiginous melanoma — more common in people with darker skin — is frequently diagnosed at later stages due to atypical locations (palms, soles, nail beds) and lower clinical suspicion. Awareness in all populations is essential.
📌 Related Reading: What Causes Melanoma — Risk Factors Explained | Melanoma 2026: AI Screening and Survival Advances
📊 Explore more health data and tools at mymedicineadvisor.com
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.