On This Page – Quick Medical Summary
When James, a 47-year-old teacher from Ohio, heard his dermatologist say “we need to check your lymph nodes,” his mind went straight to the worst. What followed wasn’t the terrifying ordeal he imagined — it was a same-day outpatient procedure that gave him and his oncologist the exact information needed to build his treatment plan.
If you’ve been diagnosed with melanoma and your doctor has recommended a sentinel lymph node biopsy, you’re in the right place. This guide covers exactly what happens during the procedure, what positive and negative results actually mean for your future, and a day-by-day recovery timeline no other source gives you.
What Is a Sentinel Lymph Node Biopsy for Melanoma?
The “Gatekeeper” Concept Explained Simply
Your lymphatic system is a network of vessels and nodes that filter fluids throughout your body. When melanoma spreads, it almost always travels to nearby lymph nodes first — before reaching distant organs.
The sentinel lymph node is the very first node in that drainage pathway from the melanoma tumor. Think of it as the gatekeeper. If cancer cells are going to escape the original tumor site, this is where they go first.
A sentinel lymph node biopsy (SLNB) is a minimally invasive surgical procedure that removes this specific node — or a small cluster of them — to test whether melanoma cells have migrated beyond the original tumor. It was first developed in 1992 by Dr. Donald Morton and has since become the global standard of care for early-stage melanoma staging, endorsed by the NCCN, AAD, ESMO, and Cancer Council Australia.
According to the National Cancer Institute, a negative SLNB result means cancer has likely not spread to nearby lymph nodes or other organs — a profoundly important piece of information for treatment planning.
Who Needs a Sentinel Lymph Node Biopsy for Melanoma? (2026 NCCN Guidelines)
Not every melanoma patient requires SLNB. Your eligibility is determined primarily by Breslow thickness — the depth of your melanoma measured in millimeters.
| Melanoma Stage | Breslow Thickness | SLNB Recommendation (2026 NCCN) |
|---|---|---|
| T1a | < 0.8 mm, no ulceration | Not recommended |
| T1b | 0.8–1.0 mm, or < 0.8 mm with ulceration | Discuss with your doctor (5–10% SLN positivity risk) |
| T2 | 1.0–2.0 mm | Recommended |
| T3 | 2.0–4.0 mm | Strongly recommended (15% positivity rate) |
| T4 | > 4.0 mm | Recommended after risk/benefit discussion (30–40% positivity rate) |
If you want to assess your personal skin cancer risk factors alongside your melanoma history, our Genetic Risk Assessment Tool can help you identify hereditary variables worth discussing with your specialist.
For a deeper understanding of how your melanoma was classified before this step, see our complete guide on how melanoma is diagnosed.
The SLNB Procedure — Step-by-Step
Before Surgery: Lymphatic Mapping
SLNB begins before you enter the operating room, usually the morning of surgery.
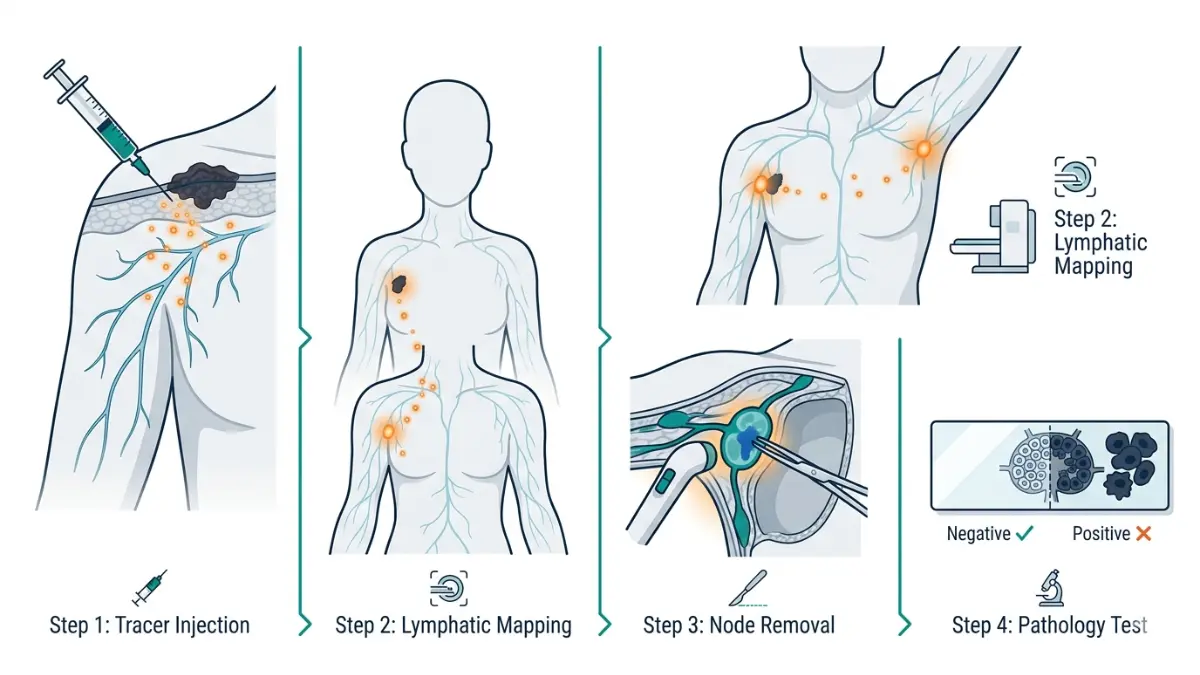
Step 1 — Radioactive Tracer Injection: A nuclear medicine technician injects a small amount of radioactive material (technetium-99m sulfur colloid) near the melanoma site. This tracer travels through your lymphatic vessels to the sentinel node(s), lighting them up for the surgeon.
Step 2 — Lymphoscintigraphy: A scan (lymphoscintigraphy) creates an image showing exactly which lymph nodes have absorbed the tracer. This gives your surgical team a precise map before making any incision.
Step 3 — Blue Dye Injection (In Some Cases): Many surgeons also inject a blue dye (isosulfan blue or methylene blue) near the tumor. This provides a visual confirmation during surgery — the sentinel node literally turns blue.
What to expect before the procedure:
- Fast for 6–8 hours before general anesthesia
- Blood and urine tests may be required
- Inform your team of any dye allergies
- Arrange transport home — you cannot drive after anesthesia
During Surgery: Inside the Operating Room
The actual surgical portion of a sentinel lymph node biopsy for melanoma typically takes 30–45 minutes.
How the surgeon finds the sentinel node:
- A handheld gamma probe detects the radioactive signal inside your body
- The blue dye provides visual identification
- One to five nodes are typically removed — the exact number depends on your tumor location and lymphatic anatomy
What happens to the removed nodes:
- Nodes are sent to a pathologist immediately
- In some centers, a frozen section analysis provides a preliminary result within 30 minutes
- Final definitive pathology takes 1–4 weeks
As the Cleveland Clinic explains, if your test results come back positive during surgery, your surgeon may remove additional lymph nodes the same session — sparing you a second procedure.
💡 Key Takeaway: SLNB is almost always performed simultaneously with wide local excision (removal of the melanoma tumor itself) — meaning one anesthesia, one recovery.
After Surgery: Recovery Room and Same-Day Discharge
- Most SLNB patients are discharged the same day
- You’ll spend 1–3 hours in post-operative monitoring
- A dressing covers the incision site
- The radioactive tracer clears safely through urine within 24–48 hours
- You may notice blue-green discoloration in urine for up to 24 hours — this is normal
Understanding Your SLNB Results — Positive vs. Negative
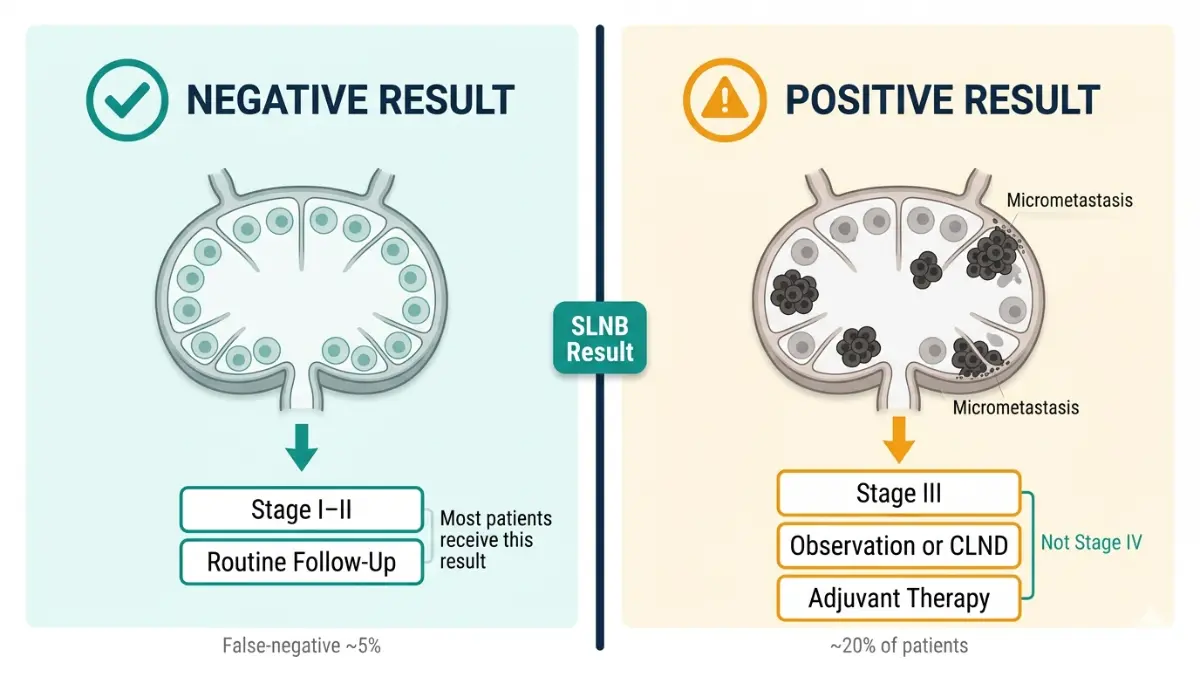
Negative SLNB Result: What It Means
A negative result means no cancer cells were found in your sentinel lymph node(s).
This is the most favorable outcome. It indicates:
- Melanoma has not spread to your regional lymph nodes
- You are unlikely to require further lymph node surgery
- Your melanoma stage remains Stage I or II
What happens next after a negative result:
- Regular follow-up monitoring for 5 years (every 3–6 months)
- Imaging (PET/CT) may still be recommended for T3–T4 melanomas
- A small 3–4% chance exists that melanoma may recur in a different lymph node — this is why ongoing surveillance matters
According to Cancer Research UK, a negative SLNB is not a guarantee, but it is the most important positive prognostic indicator available for early-stage melanoma.
Positive SLNB Result: What It Means — And What It Doesn’t
A positive result means cancer cells were detected in the sentinel node. This does NOT automatically mean Stage IV or terminal cancer.
It means:
- Melanoma has begun spreading through the lymphatic system
- Your melanoma is reclassified as Stage III
- Additional treatment options are now available and recommended
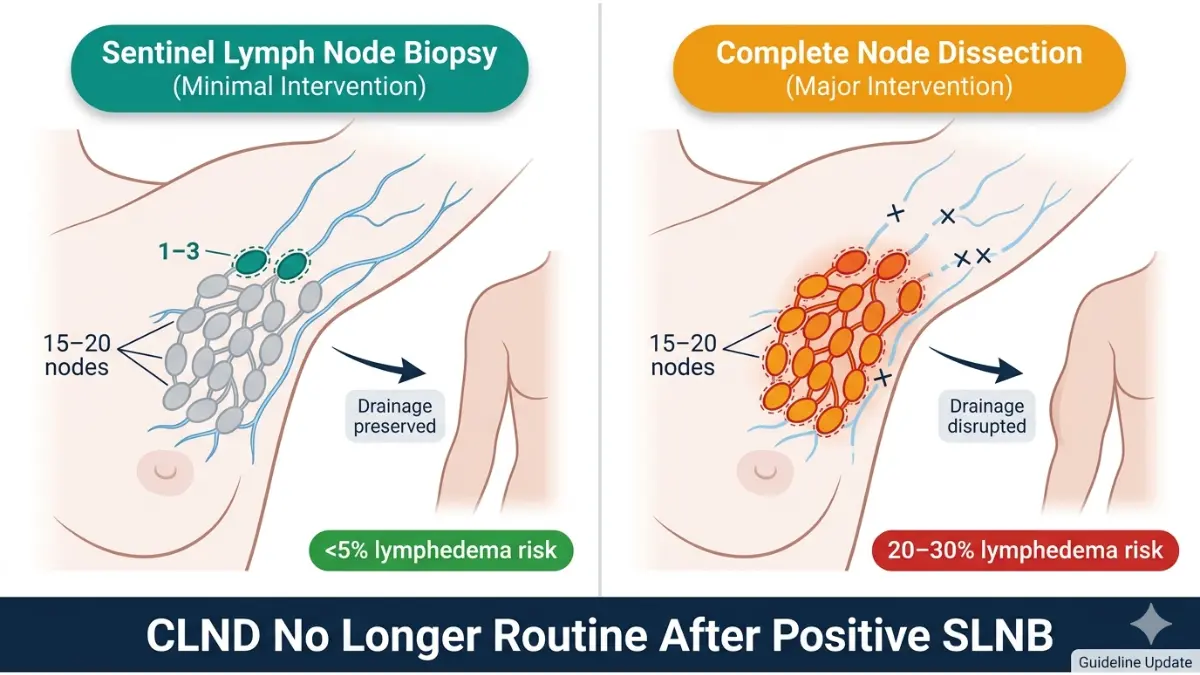
2025–2026 Updated Treatment Approach After Positive SLNB:
Based on landmark trials (MSLT-II and DeCOG-SLT), complete lymph node dissection (CLND) is no longer automatically recommended. The current standard offers two paths:
| Option | Who It’s For | What It Involves |
|---|---|---|
| Active Observation | Low-risk micrometastasis | Regular ultrasound + imaging surveillance |
| CLND + Adjuvant Therapy | Higher-risk disease | Removal of remaining nodes + immunotherapy |
Modern adjuvant therapies available in 2026:
- Pembrolizumab (Keytruda) — PD-1 immunotherapy
- Nivolumab (Opdivo) — PD-1 immunotherapy
- Dabrafenib + Trametinib — targeted therapy for BRAF V600-mutant melanoma
To understand how these therapies function at a cellular level, our guide on how immunotherapy works provides an in-depth explanation.
For patients navigating Stage III outcomes, our detailed resource on Stage 4 melanoma survival and therapy covers the full treatment landscape.
How Long Do SLNB Results Take?
| Result Type | Timing |
|---|---|
| Intraoperative frozen section | Same day (30–60 minutes, preliminary only) |
| Final pathology report | 1–4 weeks |
| UK NHS standard (Melanoma Focus) | Up to 4 weeks |
Waiting for results is one of the most psychologically challenging parts of the process. Our comprehensive guide on biopsy results timelines walks you through exactly what to expect during this period.
The False-Negative Risk: What Patients Are Rarely Told
SLNB is highly accurate — but not perfect.
- False-negative rate: approximately 5%
- This means in about 1 in 20 cases, cancer cells are present but were not detected in the sentinel node
- A meta-analysis of 71 studies involving 25,240 patients confirmed the regional recurrence risk after a negative SLNB remains at 5% or less
This is why continued monitoring after a negative result remains essential — not optional.
Risks, Complications, and Accuracy
Common Short-Term Side Effects
Most patients experience mild side effects that resolve within days to weeks:
- Soreness and tenderness at the incision site
- Swelling and bruising around the biopsy area
- Mild fatigue from anesthesia
- Temporary skin discoloration from blue dye (can persist 1–3 months on the skin surface)
Rare but Serious Complications
| Complication | Frequency | Notes |
|---|---|---|
| Lymphedema (arm/leg swelling) | < 5% for SLNB | Much lower than CLND risk of 20–30% |
| Seroma (fluid collection) | Uncommon | Usually resolves on its own |
| Wound infection | < 3% | Managed with antibiotics |
| Allergic reaction to blue dye | < 1% | Anaphylaxis is rare but possible |
| Nerve sensitivity changes | Occasional | Usually temporary |
SLNB vs. Complete Lymph Node Dissection: Why SLNB Wins
| Factor | SLNB | Complete Lymph Node Dissection (CLND) |
|---|---|---|
| Lymphedema risk | < 5% | 20–30% |
| Hospital stay | Same-day discharge | 2–5 days |
| Recovery time | 2–4 weeks | 4–8 weeks |
| Invasiveness | Minimal | Major surgery |
| Staging accuracy | > 95% | Used only after positive SLNB |
| Survival benefit | Equivalent | No added survival benefit shown |
This comparison is backed by the published findings of the PMC clinical review on SLNB in cutaneous melanoma, which confirmed SLNB has shifted from a therapeutic role to a precision staging tool — making CLND avoidable in most patients.
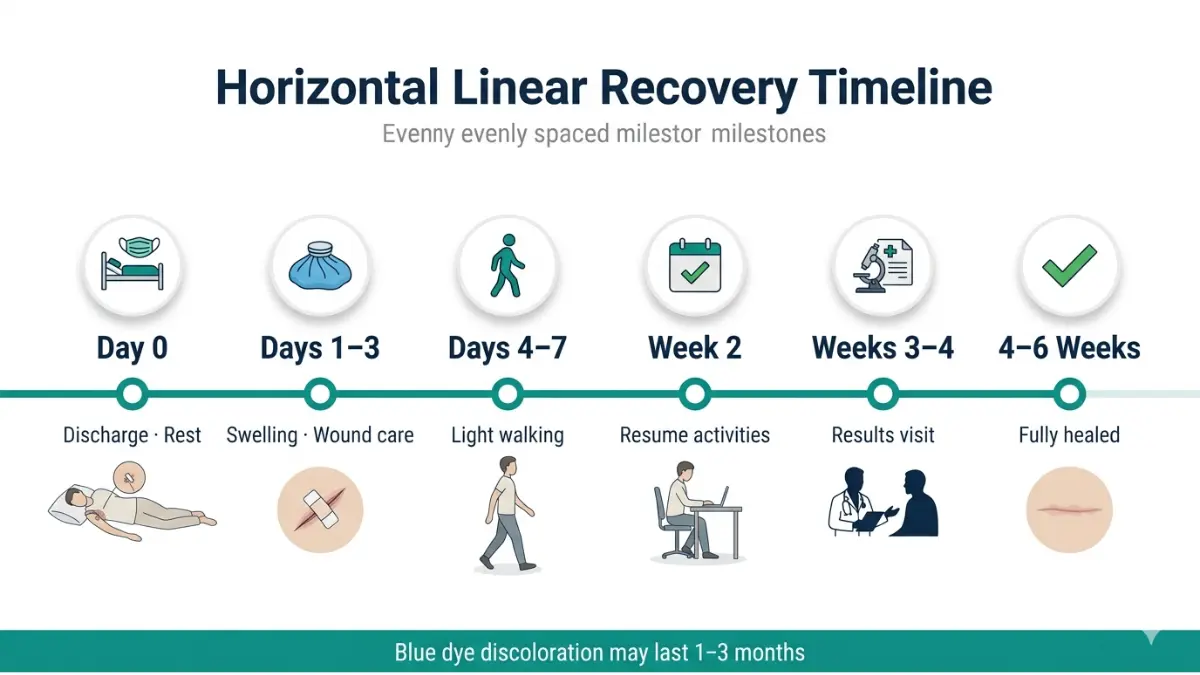
Sentinel Lymph Node Biopsy Recovery — Complete Day-by-Day Timeline
This is the section no major competitor provides. Most articles say “recovery takes a few weeks.” Here’s what actually happens.
Full Recovery Timeline
| Timeframe | What to Expect | Action Steps |
|---|---|---|
| Day of Surgery | Soreness, drowsiness from anesthesia, wound dressing in place | Rest at home, avoid driving, have someone with you |
| Days 1–2 | Swelling peaks, mild bruising, possible blue-tinged urine/skin | Keep wound dry, ice pack for 15-min intervals, take prescribed pain relief |
| Days 3–5 | Soreness begins to ease, light activity possible | Short walks encouraged; avoid lifting > 5 lbs |
| Days 5–7 | Most patients feel significantly better | Resume light desk work; continue wound monitoring |
| Week 2 | Swelling mostly resolved; incision healing | Return to most normal daily activities |
| Weeks 3–4 | Awaiting final pathology; follow-up appointment | Attend clinic review; discuss results with oncologist |
| Weeks 4–6 | Incision fully healed for most patients | Resume exercise gradually; full return to physical work |
Wound Care Instructions
Follow these steps to prevent infection and promote healing:
- Keep the wound dry for 48 hours after surgery
- After 48 hours, gently clean with mild soap and pat dry
- Change dressings as instructed (usually daily)
- Watch for: redness spreading beyond the wound, warmth, pus, fever above 100.4°F (38°C)
- Avoid submerging in pools, baths, or hot tubs for at least 2 weeks
The Mayo Clinic’s sentinel node biopsy guide confirms most patients return to regular activities within a few days and experience full incision healing within several weeks.
When Can You Return to Normal Activities?
| Activity | Typical Return Timeline |
|---|---|
| Driving | 24–48 hours after anesthesia clears |
| Desk/office work | 5–7 days |
| Light exercise (walking) | Day 3–5 |
| Gym / weight training | 2–3 weeks |
| Swimming / hot tub | 2 weeks minimum |
| Heavy physical labor | 3–4 weeks |
The Blue Dye: What Nobody Warns You About
Many patients are alarmed when they notice blue-green skin discoloration after SLNB. This is completely normal and expected.
- Skin: Blue-green tint at or near the injection site can last 1–3 months
- Urine: May appear blue-green for up to 24 hours post-surgery
- This is caused by the isosulfan blue dye used during lymphatic mapping — it is not harmful
The American Cancer Society’s SLNB overview confirms this is an expected cosmetic effect that self-resolves without treatment.
💡 What This Means For You: Recovery from a sentinel lymph node biopsy is significantly easier than most patients expect. Your main role during weeks 3–4 is managing the psychological weight of waiting for final pathology results.
Quality sleep during recovery is critical for immune function and healing. If stress is disrupting your rest, use our Sleep Calculator to optimize your sleep schedule during the recovery period.
Melanoma Staging, Next Steps, and Expert Consensus
How SLNB Determines Your Melanoma Stage
Your SLNB result is the single most important variable in determining whether you have Stage II or Stage III melanoma. This staging drives every treatment decision that follows.
| SLNB Result | Melanoma Stage | 5-Year Survival Rate (AJCC 8th Ed.) |
|---|---|---|
| Negative | Stage I–II | 85–99% |
| Positive (micrometastasis) | Stage IIIA–IIIB | 63–78% |
| Positive (macrometastasis) | Stage IIIC–IIID | 32–53% |
| With distant metastasis | Stage IV | 15–20% (improving with immunotherapy) |
For a complete breakdown of all melanoma stages and their survival data, our dedicated guide on melanoma stages covers every classification in detail.
If Your SLNB Is Positive: Modern Treatment in 2025–2026
A positive sentinel lymph node biopsy now opens the door to highly effective adjuvant therapies that have transformed Stage III melanoma outcomes. Current clinical trials listed on ClinicalTrials.gov continue to refine who benefits most from each approach.
Your oncologist will discuss:
- Whether observation alone is sufficient (low-burden micrometastasis)
- Adjuvant pembrolizumab or nivolumab (18-cycle immunotherapy protocols)
- Targeted BRAF/MEK therapy if your tumor tests BRAF V600E positive
- Whether additional imaging (PET/CT) is warranted to rule out distant spread
The Melanoma Research Alliance emphasizes that SLNB helps some patients avoid more extensive lymph node surgery entirely — a major quality-of-life advance.
Global Expert Consensus: What Every Major Organization Says
| Organization | SLNB Position (2025–2026) |
|---|---|
| NCCN (USA) | Recommended for T2–T4; discuss for T1b |
| ESMO (Europe) | Standard of care for eligible patients |
| AAD (USA) | Endorsed for staging and treatment planning |
| Cancer Council Australia | Recommended per national guidelines |
| NICE (UK) | Standard practice per 2022 updated guidelines |
The Melanoma Focus sentinel node biopsy resource — a specialist charity — notes that a positive node is found in approximately 20% (1 in 5) of patients offered the procedure. This means 80% of patients receive negative results and avoid more invasive surgery entirely.
For those navigating melanoma from diagnosis onward, our comprehensive melanoma pillar article covers the full disease journey from first symptoms to advanced treatment. You can also explore the latest in AI-assisted melanoma screening and survival data for 2026.
Frequently Asked Questions
1. What is a sentinel lymph node biopsy for melanoma?
A sentinel lymph node biopsy (SLNB) is a minimally invasive surgical procedure that removes the first lymph node(s) connected to a melanoma tumor to test whether cancer cells have spread beyond the original site.
2. Who needs a sentinel lymph node biopsy for melanoma?
SLNB is generally recommended for melanomas with a Breslow thickness greater than 1.0 mm (T2–T4). It may also be considered for T1b melanomas (0.8–1.0 mm) with ulceration or other high-risk features per 2026 NCCN guidelines.
3. How long does a sentinel lymph node biopsy take?
The surgical portion takes approximately 30–45 minutes. If performed alongside wide local excision, add another 30–45 minutes. Most patients are discharged the same day.
4. Does a positive sentinel lymph node mean melanoma has spread everywhere?
No. A positive result means cancer cells have reached nearby lymph nodes — classifying you as Stage III. It does not mean distant metastasis. Modern adjuvant therapies offer strong outcomes at this stage.
5. What does a negative SLNB result mean for melanoma?
It means there is no evidence of cancer spread to regional lymph nodes. You’ll still require monitoring for 5 years since a 3–4% recurrence risk remains.
6. How accurate is sentinel lymph node biopsy for melanoma?
SLNB has a detection accuracy exceeding 95%. The false-negative rate is approximately 5%, based on a meta-analysis of 71 studies involving over 25,000 patients.
7. What is the recovery time for sentinel lymph node biopsy?
Most patients return to light activities within 3–5 days and full activity within 3–4 weeks. The incision fully heals within 4–6 weeks.
8. Is sentinel lymph node biopsy painful?
Discomfort is typically mild to moderate and well-managed with over-the-counter pain relievers. Most patients rate the recovery as much easier than anticipated.
9. What happens after a positive sentinel lymph node biopsy for melanoma?
Your oncologist will discuss active surveillance or complete lymph node dissection (CLND), followed by adjuvant immunotherapy (pembrolizumab or nivolumab) or targeted therapy based on BRAF mutation status.
10. How long do sentinel lymph node biopsy results take?
A preliminary intraoperative result can be available the same day. Final definitive pathology typically takes 1–4 weeks.
11. Can melanoma spread even after a negative sentinel lymph node biopsy?
Yes, in approximately 3–5% of cases. This is why 5-year follow-up monitoring remains standard even after a negative result, and why using our Symptom Checker to track any new skin or lymph node changes is valuable between appointments.
⚕️ Reviewed and compiled in accordance with 2026 NCCN, ESMO, AAD, and NICE guidelines. This article is for educational purposes only. Always consult a board-certified oncologist or dermatologist for personalized medical advice.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.