On This Page – Quick Medical Summary
What does a lung cancer prognosis really mean for you?
If you were just diagnosed, start with the survival rates section — it will give you the stage-specific data your oncologist will reference. If you are preparing for your first oncology appointment, jump to Section 4 for a precise look at how prognosis is assessed clinically. If you have already received a stage and want to understand what biomarkers mean for your individual outlook, Section 5 is where the most important information for you lives.
Lung cancer prognosis is the medical assessment of how a patient’s disease is likely to progress over time — including the probability of long-term survival — based on cancer type, stage, and individual clinical factors. It is not a fixed number pulled from a chart.
Why your prognosis is not the same as a statistic
Population survival statistics describe thousands of patients diagnosed across all stages, cell types, and treatment eras — including eras when targeted therapy and modern immunotherapy were not yet available.
Your prognosis reflects your specific tumor biology, your stage, your biomarker profile, and the treatments accessible to you in 2026. Those are four variables that the population average cannot account for.
How this guide is organized for you
This guide covers the six most clinically significant prognostic factors, stage-specific survival rates, how your oncologist calculates an individual prognosis, and how biomarker-guided therapy is reshaping outcomes for specific patient subgroups.
For foundational context on how lung cancer develops and is classified, see our complete lung cancer guide. If you are still evaluating unexplained symptoms before a formal diagnosis, our Symptom Checker can help you organize what to bring to a clinical appointment.
ℹ️ Medical Disclaimer: The diagnostic criteria, survival statistics, treatment options, and medication information in this article reflect current clinical guidelines and are provided for educational purposes only. Individual prognosis, treatment decisions, and medication choices depend on cancer stage, pathology results, biomarker profile, ECOG performance status, comorbidities, and specialist assessment. Consult a board-certified medical oncologist or thoracic oncologist before acting on any clinical information in this article. This article does not constitute a diagnosis or a treatment recommendation for any individual patient.
The key factors that shape lung cancer prognosis
Six clinical variables shape lung cancer prognosis more than any others. Understanding each one is the foundation for a precise, informed conversation with your oncologist.
Cancer stage: why it is the single most powerful prognostic variable
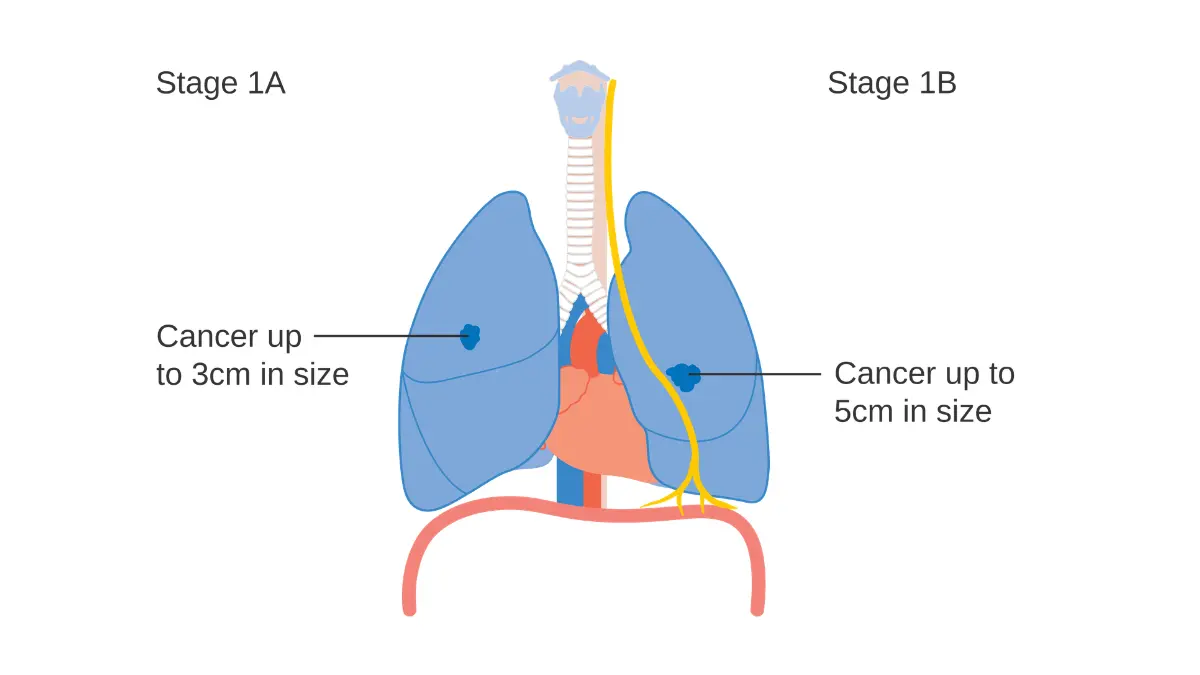
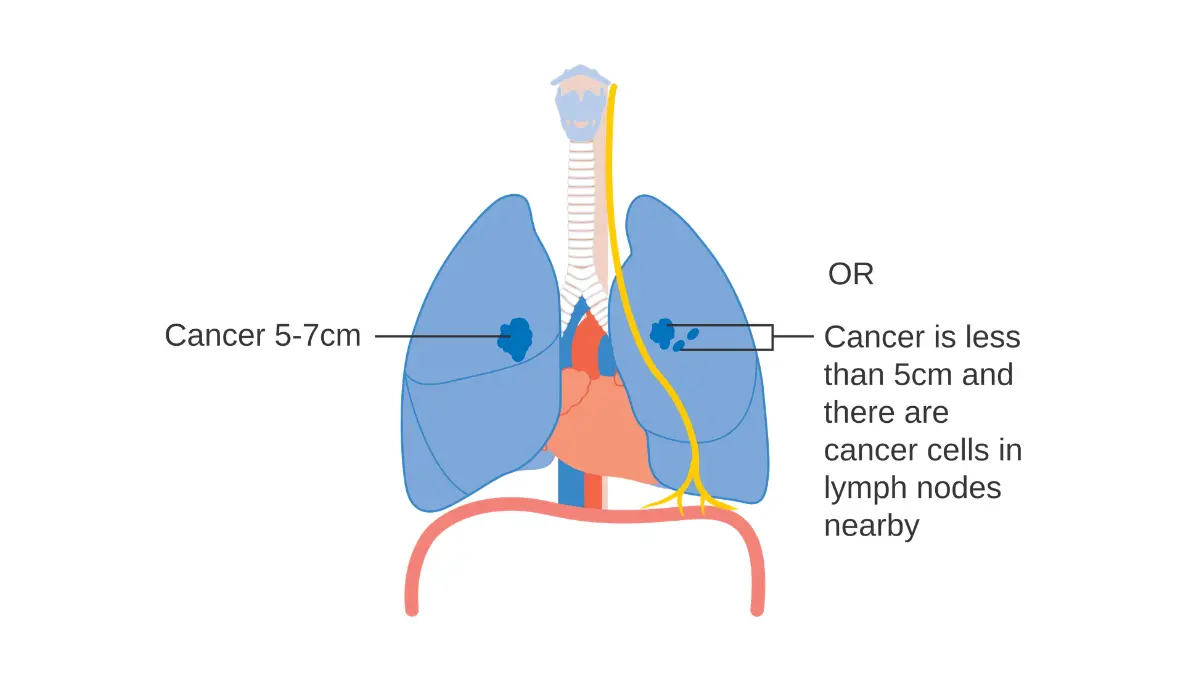
Stage at diagnosis remains the strongest independent predictor of lung cancer outcome. The TNM staging system classifies tumors by primary tumor size (T), regional lymph node involvement (N), and presence of distant metastasis (M) — and each component carries distinct prognostic weight.
A patient with Stage I NSCLC confined to the lung and eligible for surgical resection faces a fundamentally different clinical trajectory than a Stage IV patient with distant metastatic spread. Stage determines surgical eligibility, radiation intent, systemic therapy sequencing, and whether the treatment goal is curative or disease-control.
Histological type: NSCLC vs. SCLC and what each means for your outlook
Non-small cell lung cancer (NSCLC) accounts for approximately 84% of all lung cancer diagnoses and includes adenocarcinoma, squamous cell carcinoma, and large cell carcinoma. It is staged I through IV and generally grows more slowly than SCLC, with more actionable biomarker targets.
Small cell lung cancer (SCLC) is classified as limited-stage (confined to one hemithorax) or extensive-stage (spread beyond). SCLC is biologically aggressive, frequently disseminated at diagnosis, and carries a more limited prognosis than most NSCLC subtypes despite high initial chemotherapy sensitivity. For a detailed comparison of how these two cancer types differ in staging, symptoms, and treatment response, see the clinical differences between NSCLC and SCLC.
Biomarker mutations: the factor that can change everything
In NSCLC specifically, actionable biomarker mutations are the single variable most likely to dramatically alter a patient’s prognosis in 2026. EGFR mutations, ALK rearrangements, ROS1 fusions, KRAS G12C mutations, and others each determine eligibility for targeted therapies that produce substantially longer survival than standard chemotherapy in biomarker-matched patients.
PD-L1 expression determines immunotherapy eligibility — specifically whether pembrolizumab monotherapy or a combination regimen is indicated. These are not secondary considerations. They are primary treatment-selection variables in modern thoracic oncology.
🔬 How It Works: A biomarker is a molecular feature of your tumor — a specific gene mutation or protein expression pattern — that tells oncologists whether your cancer cells will respond to a targeted drug. An EGFR mutation, for example, means your tumor cells carry an error in the gene that controls cell growth and division. Osimertinib (Tagrisso) is designed to block precisely that error. Without the mutation, there is no target for the drug to act on.
Tumor location and lymph node spread
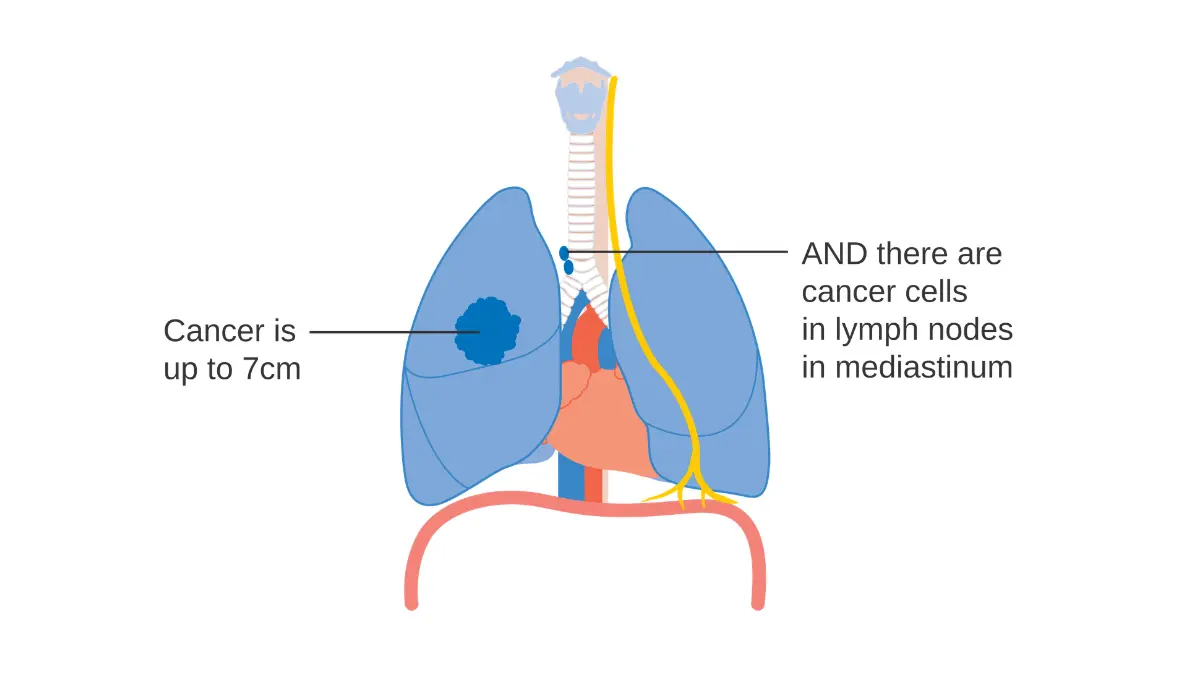
Mediastinal lymph node involvement — particularly N2 disease (ipsilateral mediastinal nodes) and N3 disease (contralateral or supraclavicular nodes) — significantly reduces surgical eligibility and shifts treatment intent from resection to concurrent chemoradiation.
Central tumors adjacent to major airways carry higher procedural complexity than peripheral lesions. Malignant pleural effusion is classified as M1a distant metastatic disease in NSCLC staging and changes both the pathological stage and the prognosis accordingly.
✅ Patient Action: If your oncologist has not yet ordered reflex next-generation sequencing (NGS) of your tumor for EGFR, ALK, ROS1, KRAS G12C, BRAF V600E, MET exon 14, RET, and PD-L1 expression — ask specifically before your next treatment planning appointment whether this testing is indicated. Per NCCN 2026 Clinical Practice Guidelines, comprehensive biomarker testing is standard of care for all newly diagnosed NSCLC patients regardless of stage.
Lung cancer survival rates by stage: what the 2026 data shows
Five-year relative survival rates for lung cancer vary dramatically by stage and cancer type. A patient diagnosed with localized Stage I NSCLC faces a statistical outlook that is not a marginal improvement over Stage IV — it is a difference measured in decades of life. Understanding this separation is the first step toward interpreting your own prognosis accurately.
NSCLC survival rates by stage (I through IV)
The table below presents five-year relative survival rates for non-small cell lung cancer by stage category, referenced from NCI SEER data. These rates represent the percentage of NSCLC patients alive five years after diagnosis relative to the general population.
| NSCLC Stage | 5-Year Relative Survival | Key Clinical Characteristics | Best for Patient Profile |
|---|---|---|---|
| Stage I (localized) | ~63–82%* | Tumor confined to lung, no lymph node involvement | Surgical candidates — lobectomy or segmentectomy |
| Stage II | ~36–52%* | Limited regional lymph node involvement possible | Surgery ± adjuvant therapy; adjuvant osimertinib if EGFR-positive |
| Stage III | ~12–28%* | Mediastinal lymph node involvement; surgery complex | Concurrent chemoradiation ± consolidation immunotherapy |
| Stage IV | ~7–9%* | Distant metastasis confirmed | Systemic therapy — targeted agent or immunotherapy if biomarker-eligible |
📊 Clinical Data Point: Five-year relative survival rates for NSCLC range from approximately 63–82% for Stage I localized disease to approximately 7–9% for Stage IV distant disease. These figures reflect the overall NSCLC population and do not isolate biomarker-positive patients on targeted therapy, who may substantially outperform these benchmarks — Source: NCI SEER Database, 2026 (NCI SEER lung cancer survival statistics).
For a full clinical definition of each stage and what it means for treatment eligibility, see how each lung cancer stage is defined and classified.
SCLC survival rates: limited vs. extensive disease
Small cell lung cancer uses a two-category staging system — limited-stage and extensive-stage — because it behaves as a systemic disease from early on.
| SCLC Stage | 5-Year Relative Survival | Key Clinical Detail |
|---|---|---|
| Limited-stage | ~20–30%* | Confined to one hemithorax; concurrent chemoradiation is standard |
| Extensive-stage | ~5–7%* | Spread beyond hemithorax at diagnosis; systemic chemotherapy + immunotherapy |
📊 Clinical Data Point: Approximately 60–70% of SCLC patients are diagnosed at extensive stage — a distribution that substantially lowers population survival averages for this cancer type and underscores why early detection matters — Source: American Cancer Society 2026 Cancer Facts & Figures (American Cancer Society lung cancer statistics).
For a comprehensive breakdown of SCLC-specific outcomes and treatment cost data, see our guide to small cell lung cancer survival rates and treatment.
Why survival statistics don’t define your individual outcome
🩺 Physician Note: “When a newly diagnosed patient asks me what a survival rate means for them personally, I give the same answer every time: those statistics describe a historical population, not your specific tumor in 2026. The SEER cohort includes patients diagnosed when osimertinib, lorlatinib, and consolidation durvalumab were not yet standard of care. A patient with EGFR-mutant Stage IIIB NSCLC being treated today is not the same patient as someone in that historical cohort. The statistics are a compass direction — not your destination.” — Dr. Nathaniel J. Hargrove, MD, Oncology
The SEER database captures data from patients diagnosed several years before the statistics are published — meaning the survival rates widely cited today largely reflect treatment regimens from 2018–2022. A 2026 patient with access to biomarker-guided targeted therapy, third-generation ALK inhibitors, and immunotherapy consolidation protocols may significantly outperform those benchmarks. For a deeper look at how these statistics are calculated and what they actually measure, see our detailed guide to lung cancer statistics and survival rates.
How your oncologist determines your individual prognosis
Prognosis is not a single test result. It is a clinical synthesis — assembled from staging workup findings, pathology, biomarker data, and a direct assessment of your functional health status. Understanding this process prepares you to participate in it actively.
The staging workup: CT, PET, and biopsy
Complete staging begins with a contrast-enhanced CT scan of the chest, abdomen, and pelvis. A PET-CT scan follows in most cases to detect metabolic activity in lymph nodes and distant sites — a critical step for identifying metastasis that CT alone can miss in approximately 10–20% of cases.
Tissue biopsy confirms cell type and provides the material for next-generation sequencing (NGS) — the molecular profiling step that identifies every actionable mutation and determines targeted therapy eligibility.
Performance status and why it affects your treatment options
Your ECOG performance status is a 0–5 functional scale that governs treatment eligibility more directly than age alone. ECOG 0 means fully active. ECOG 1 means restricted in strenuous activity but ambulatory. ECOG 2 means ambulatory and capable of self-care but unable to carry out work.
ECOG 0–1 is the threshold for most aggressive treatment protocols — including concurrent chemoradiation, immunotherapy combinations, and major surgical resection. ECOG ≥2 significantly narrows the treatment menu. An accurate performance status assessment by your oncologist changes which therapies are on the table.
✅ Patient Action: Before your first oncology appointment, confirm with your referring physician whether your imaging included a PET scan and whether biopsy tissue has been sent for NGS. These two data points are essential for a clinically precise, individualized prognosis — and without them, your oncologist is working with an incomplete picture.
To understand how your baseline genetic risk profile may inform your oncologist’s assessment of hereditary risk factors alongside your diagnosis, use our Genetic Risk Assessment Tool.
How tumor boards shape prognosis conversations
Most major cancer centers present newly diagnosed lung cancer cases to a multidisciplinary tumor board — a panel of thoracic surgeons, medical oncologists, radiation oncologists, and pulmonologists who review staging, pathology, and biomarker data together.
The prognosis a patient receives at a tumor board center reflects more clinical input than a single-physician assessment. This is one reason seeking care at an NCI-designated cancer center matters — the prognosis conversation itself is a richer, more complete one.
How biomarkers and targeted therapy are changing lung cancer prognosis
Biomarker-guided therapy has fundamentally shifted lung cancer outcomes for specific NSCLC subgroups. This is not an incremental improvement. For patients with actionable mutations, it represents a transformation of the prognosis conversation.
EGFR and ALK mutations: the strongest prognosis-changing biomarkers in NSCLC
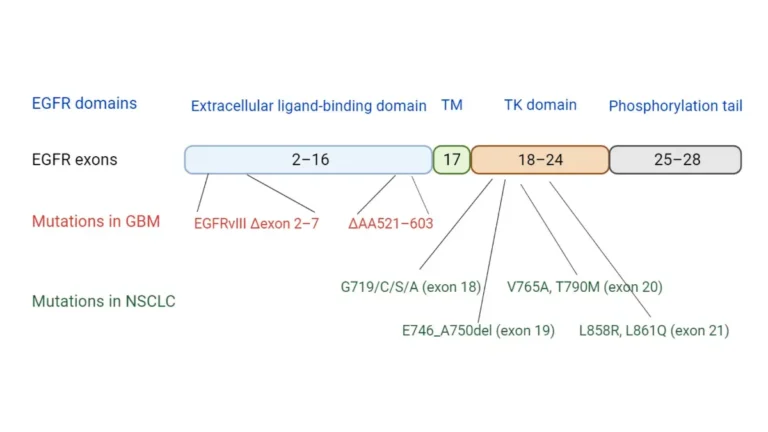
EGFR mutations — particularly exon 19 deletions and exon 21 L858R point mutations — occur in approximately 10–15% of NSCLC patients in the United States. These patients are eligible for osimertinib (Tagrisso), a third-generation EGFR inhibitor now established as the first-line standard of care for metastatic EGFR-mutant NSCLC per NCCN 2026 guidelines.
ALK rearrangements affect approximately 3–5% of NSCLC patients. Alectinib (Alecensa) and lorlatinib (Lorbrena) are current first-line and sequential ALK inhibitor options, with lorlatinib preferred in certain settings for its central nervous system penetration.
📊 Clinical Data Point: Osimertinib demonstrated median progression-free survival of approximately 18.9 months versus 10.2 months for first-generation EGFR inhibitors in the FLAURA trial — Source: FLAURA trial, New England Journal of Medicine.
For a detailed patient guide to how targeted therapy works and which mutations qualify patients for each agent, see targeted therapy for EGFR and ALK-positive lung cancer.
PD-L1 and immunotherapy: what your TPS score means for your outlook
PD-L1 tumor proportion score (TPS) is reported as a percentage and determines immunotherapy eligibility in three clinically distinct tiers. This is not a binary positive/negative result — the number itself changes your treatment:
- TPS ≥50%: Pembrolizumab (Keytruda) monotherapy is first-line standard for patients without actionable mutations — chemotherapy is not required
- TPS 1–49%: Pembrolizumab plus platinum-based chemotherapy is the combination standard
- TPS <1%: Chemotherapy backbone is required; pembrolizumab monotherapy is not indicated in this subgroup
🔬 How It Works: PD-L1 is a protein on cancer cells that functions as a “don’t kill me” signal to the immune system, preventing T-cells from attacking the tumor. Pembrolizumab blocks the PD-1 receptor on T-cells, removing that protective signal and allowing the immune system to recognize and destroy cancer cells. A high PD-L1 TPS means more cancer cells are displaying that signal — and more targets exist for the drug to act on.
For a comprehensive overview of how immunotherapy affects prognosis and what patients experience during treatment, see how immunotherapy works for lung cancer.
KRAS G12C and emerging targets: the next wave of prognosis-altering therapies
KRAS G12C mutations — present in approximately 13% of NSCLC adenocarcinomas — became actionable with the FDA approvals of sotorasib (Lumakras) and adagrasib (Krazati), the first drugs ever approved for KRAS-mutant solid tumors.
Both agents have produced objective response rates in patients who progressed on prior platinum-based chemotherapy, opening a treatment option in a historically undruggable mutation. For the full list of currently FDA-approved agents for lung cancer as of 2026, see our article on FDA-approved lung cancer drugs and treatment options in 2026.
📊 Clinical Data Point: Sotorasib and adagrasib received FDA approval for KRAS G12C-mutant NSCLC following progression on prior systemic therapy — Source: FDA drug approvals (FDA-approved targeted therapies for non-small cell lung cancer).
✅ Patient Action: Before any treatment plan is finalized, ask your board-certified oncologist: “Has my tumor been tested for all NCCN-recommended biomarkers via NGS — specifically EGFR, ALK, ROS1, KRAS G12C, BRAF V600E, MET exon 14 skipping, RET rearrangement, and PD-L1 expression?” Per the NCCN 2026 Clinical Practice Guidelines for lung cancer (NCCN requires free registration), this comprehensive testing is standard of care for all newly diagnosed NSCLC patients regardless of stage.
Patient health factors that independently affect your lung cancer outlook
Beyond tumor biology, four patient-level variables independently shape prognosis: functional status, comorbidities, smoking history, and access to clinical trials.
Age, sex, and performance status as independent prognostic variables
ECOG performance status and comorbidity burden predict treatment eligibility more accurately than chronological age alone. Patients aged 70 or older are not automatically excluded from aggressive treatment — they are evaluated on the basis of functional reserve, organ function, and concurrent medical conditions.
Sex appears as an independent prognostic variable in population data. Women with NSCLC demonstrate modestly higher overall survival than men at equivalent stages — a difference partly explained by higher EGFR mutation prevalence and never-smoker status among women with adenocarcinoma, both of which correlate with better targeted therapy response.
Comorbidities: how COPD, heart disease, and diabetes affect treatment tolerance
Moderate-to-severe COPD directly governs surgical eligibility. Predicted postoperative FEV1 — a pulmonary function measure — determines whether a patient can tolerate lobectomy without prohibitive respiratory risk.
Active cardiovascular disease and recent myocardial infarction affect immunotherapy eligibility, as immune checkpoint inhibitors carry cardiac toxicity risks that require co-management with cardiology. Oncologists and cardiologists frequently collaborate on treatment planning for patients with concurrent cardiac conditions.
✅ Patient Action: If you have moderate-to-severe COPD, recent cardiac events, or an active autoimmune condition, ask your oncologist whether a joint evaluation with a pulmonologist, cardiologist, or rheumatologist should precede any treatment decision — particularly if surgery, concurrent chemoradiation, or immunotherapy is being considered.
Smoking cessation after diagnosis: does it change prognosis?
Smoking cessation after a lung cancer diagnosis consistently improves surgical outcomes, reduces treatment-related complication risk, and may enhance response to systemic therapies. It does not reverse the underlying cancer — but it reduces the competing physiological burden during treatment and recovery.
For evidence-based cessation strategies specifically relevant to lung cancer patients, see quitting smoking after a lung cancer diagnosis.
Clinical trial access as a prognosis pathway
For patients whose disease has progressed beyond standard therapies, enrollment in a clinical trial is a legitimate and sometimes prognosis-altering option — not a last resort. Patients at NCI-designated cancer centers have measurably higher access to novel agents and combination strategies than those treated exclusively in community oncology settings.
Search for active protocols through active lung cancer clinical trials on ClinicalTrials.gov. You can also review lung cancer screening criteria and guidelines to understand how early detection — the single strongest prognostic factor of all — is governed.
Body weight and nutritional status are increasingly recognized as independent prognostic variables in lung cancer. Use our BMI Calculator to assess your current baseline as one component of the broader health picture your oncologist evaluates.
Dr. Hargrove’s clinical perspective: prognosis in the era of precision oncology
What 2026 changes about the prognosis conversation
🩺 Physician Note: “Earlier this year, I saw a patient referred to me with clinical Stage IIIA NSCLC, already scheduled to begin concurrent chemoradiation. Reflex NGS testing came back with an EGFR exon 19 deletion — and the entire treatment conversation changed that day. We went from a curative-intent chemoradiation protocol to first-line osimertinib with a fundamentally different survival trajectory. That patient left my office with a different prognosis than the one they arrived with. That is what precision oncology looks like in 2026. No newly diagnosed NSCLC patient should begin treatment without a complete biomarker profile in hand.” — Dr. Nathaniel J. Hargrove, MD, Oncology
The single most important structural shift in lung cancer prognosis over the past decade is not any one drug. It is the standard of reflex biomarker testing — the expectation that every newly diagnosed NSCLC patient receives comprehensive molecular profiling before a treatment plan is finalized. Patients who receive biomarker-matched targeted therapy in 2026 are not the same population as the SEER historical cohort that generated the survival statistics on most other websites.
Questions every patient should ask their oncologist about prognosis
Bring these five questions to your next appointment:
- What is my exact pathological stage, and does it reflect all imaging and biopsy findings?
- Has my tumor undergone complete NGS biomarker testing — and have the results been reviewed by the full oncology team?
- Am I eligible for targeted therapy, immunotherapy, or a clinical trial based on my biomarker profile?
- How do my comorbidities affect my treatment eligibility and expected treatment tolerance?
- Is the goal of this treatment curative intent, disease control, or quality-of-life preservation?
For a full overview of every approved treatment category now available, including surgical, systemic, and radiation options, see lung cancer treatment options.
✅ Patient Action: If you were initially evaluated by a general oncologist, ask specifically for a referral to a board-certified thoracic oncologist or medical oncologist with subspecialty lung cancer experience — particularly if a complete biomarker panel has not yet been ordered. Access to a lung cancer specialist significantly affects which treatment options and clinical trial protocols are presented to you.
Taking the next step with your lung cancer prognosis
Lung cancer prognosis in 2026 is not a number on a website.
It is a dynamic clinical assessment shaped by your stage, your tumor’s biomarker profile, your functional status, and the treatments now available to you. No population statistic captures your individual case — and no oncologist can give you a precise prognosis before the complete molecular picture is in hand.
The most powerful action available to you right now is preparation. Bring the five questions from Section 7. Confirm biomarker testing has been completed. Ask about clinical trials. Ask about second opinions at an NCI-designated cancer center.
In Dr. Hargrove’s words: you are not your statistics. You are a patient in 2026 — and this is a meaningfully different era in lung cancer care than any that came before it.
Frequently asked questions about lung cancer prognosis
1. What is the survival rate for lung cancer?
Lung cancer five-year survival rates vary significantly by stage and type. Stage I NSCLC carries approximately 63–82% five-year survival; Stage IV NSCLC drops to approximately 7–9%. Limited-stage SCLC is approximately 20–30%; extensive-stage SCLC approximately 5–7%. Biomarker-positive patients receiving targeted therapy may substantially outperform these population averages. Consult a board-certified oncologist for a prognosis specific to your stage and biomarker profile.
2. What stage of lung cancer is considered curable?
Stage I and selected Stage II NSCLC are potentially curable with complete surgical resection — lobectomy or anatomic segmentectomy. Stage IIIA NSCLC can be approached with curative intent using concurrent chemoradiation followed by consolidation durvalumab in patients with adequate performance status. Stage IV is generally managed to extend survival and quality of life, with rare exceptions in oligometastatic disease. Consult a board-certified thoracic oncologist regarding surgical eligibility.
3. How does an EGFR mutation affect lung cancer prognosis?
EGFR-mutant NSCLC — specifically exon 19 deletions and exon 21 L858R mutations — responds to osimertinib (Tagrisso) with substantially longer median progression-free survival than platinum-based chemotherapy. EGFR mutations occur in approximately 10–15% of US NSCLC patients and are more prevalent in women, never-smokers, and adenocarcinoma histology. Mutation subtype — exon 19 deletion versus exon 21 — influences response duration. Consult a board-certified oncologist about your specific EGFR mutation and targeted therapy options.
4. What is the life expectancy for stage 4 lung cancer?
Stage IV NSCLC median overall survival has improved substantially for biomarker-positive patients — in EGFR-mutant populations treated with osimertinib, median overall survival now exceeds three years in published trial data. Unselected Stage IV NSCLC median survival is typically measured in months without targeted or immunotherapy eligibility. Individual prognosis depends heavily on biomarker status, performance status, and treatment access. Consult a board-certified medical oncologist for an individualized prognosis discussion.
5. Does smoking history affect lung cancer prognosis?
Smoking history influences tumor histology — heavy smokers more commonly develop squamous cell carcinoma, while never-smokers more often develop adenocarcinoma with actionable EGFR or ALK mutations. Never-smoker status correlates with higher biomarker positivity rates and stronger targeted therapy eligibility. Smoking cessation after diagnosis consistently improves treatment tolerance and reduces surgical complication risk. Consult a board-certified oncologist for a complete assessment of how smoking history affects your specific treatment options and prognosis.
6. How does immunotherapy improve lung cancer prognosis?
Pembrolizumab (Keytruda) significantly improves outcomes in NSCLC patients with PD-L1 TPS ≥50%, replacing chemotherapy as the first-line standard of care in this subgroup. In PD-L1 1–49% patients, pembrolizumab plus platinum-based chemotherapy is the combination standard. Durvalumab (Imfinzi) improves outcomes as consolidation therapy after concurrent chemoradiation in unresectable Stage III NSCLC. PD-L1 TPS testing is required before initiation. Consult a board-certified oncologist regarding your PD-L1 score and immunotherapy eligibility.
7. What is the difference between NSCLC and SCLC prognosis?
NSCLC accounts for approximately 84% of lung cancers and carries stage-dependent prognosis ranging from favorable at Stage I to limited at Stage IV — with significant upside for biomarker-positive patients. SCLC is more biologically aggressive, frequently diagnosed at extensive stage, and has lower five-year survival rates despite high initial chemotherapy sensitivity. SCLC also has fewer actionable biomarker targets currently. Consult a board-certified oncologist to understand your specific cancer type and what it means for treatment planning.
8. Can targeted therapy cure lung cancer?
Targeted therapy is not considered curative in metastatic NSCLC but significantly extends progression-free and overall survival in biomarker-matched patients. In early-stage EGFR-mutant NSCLC, adjuvant osimertinib following complete surgical resection has demonstrated meaningful improvement in disease-free survival — the closest current evidence for curative-intent targeted therapy use. Neoadjuvant targeted therapy before surgery is under active investigation. Consult a board-certified thoracic oncologist to discuss whether adjuvant targeted therapy is indicated following resection.
9. How does age affect lung cancer prognosis?
Age alone is not the primary determinant of lung cancer prognosis or treatment eligibility. ECOG performance status and comorbidity burden are clinically more meaningful predictors. Patients aged 70 or older with ECOG 0–1 performance status are often candidates for surgery, targeted therapy, or immunotherapy. Age-adjusted survival differences in population data partly reflect access disparities rather than purely biological differences. Consult a board-certified oncologist for an age-appropriate and performance-status-appropriate treatment eligibility assessment.
10. What does ECOG performance status mean for lung cancer?
ECOG performance status is a 0–5 functional scale: ECOG 0 is fully active; ECOG 1 is restricted in strenuous activity but ambulatory; ECOG 2 is ambulatory but unable to carry out work; ECOG 3 means limited self-care capacity; ECOG 4 means completely disabled. ECOG 0–1 qualifies patients for most aggressive treatment protocols. ECOG ≥2 significantly restricts eligibility for surgery, concurrent chemoradiation, and certain immunotherapy combinations. Consult a board-certified oncologist about how your current performance status affects your specific treatment options.
11. Is stage 3 lung cancer curable?
Stage IIIA NSCLC can be approached with curative intent using concurrent chemoradiation followed by consolidation durvalumab (Imfinzi) in patients with adequate pulmonary function and ECOG performance status. Stage IIIB and IIIC disease is generally treated with multimodal therapy rather than primary surgical resection. Long-term survival is achievable in a meaningful subset of Stage III patients. Outcomes vary significantly by substage and biomarker profile. Consult a board-certified thoracic oncologist for a specific assessment of your Stage III disease and curative-intent eligibility.
12. How accurate are lung cancer survival statistics?
NCI SEER survival statistics reflect patients diagnosed several years before publication, meaning current patients benefit from therapies absent from the historical cohort. Patients receiving biomarker-guided targeted therapy in 2026 may substantially outperform population averages derived from 2015–2022 treatment eras. Population survival rates are a directional reference, not an individual prediction. Consult a board-certified oncologist about how the most recent treatment advances in targeted therapy and immunotherapy apply specifically to your stage and biomarker profile.
13. What is the prognosis for early-stage lung cancer?
Stage I NSCLC — particularly Stage IA tumors under 2 cm with no lymph node involvement — carries the highest five-year survival rates of any lung cancer category, ranging from approximately 77–82% for the smallest localized tumors. Complete surgical resection remains the standard treatment. Adjuvant osimertinib is now standard of care for EGFR-mutant Stage IB–IIIA NSCLC following resection. Early-stage diagnosis remains the single strongest predictor of favorable long-term outcomes. Consult a board-certified thoracic surgeon and oncologist regarding resection and adjuvant therapy eligibility.
14. Does lung cancer prognosis differ by sex?
Clinical data indicate modestly higher overall survival in women compared to men with lung cancer at equivalent stages. This difference is partly explained by higher EGFR mutation prevalence and never-smoker status among women with adenocarcinoma — both of which correlate with better targeted therapy eligibility and response. These are population-level observations, not individual predictions. Consult a board-certified oncologist to understand how your specific biomarker profile and stage, rather than sex alone, determine your individual prognosis.
15. How do biomarkers affect lung cancer treatment and prognosis?
Comprehensive NGS biomarker testing identifies actionable mutations — EGFR, ALK, ROS1, KRAS G12C, BRAF V600E, MET exon 14, RET, and PD-L1 — that determine eligibility for targeted therapy and immunotherapy. Patients with matched targeted agents typically achieve longer progression-free survival than those receiving standard chemotherapy alone. NCCN 2026 guidelines recommend reflex NGS for all newly diagnosed NSCLC patients regardless of stage. Consult a board-certified oncologist immediately if your tumor has not yet undergone complete biomarker testing.
16. What questions should I ask my oncologist about my prognosis?
Bring these five questions: (1) What is my exact pathological stage and what does it mean for my individual prognosis? (2) Has my tumor been tested for all NCCN-recommended biomarkers via NGS? (3) Am I eligible for targeted therapy, immunotherapy, or a clinical trial? (4) How do my comorbidities affect my treatment eligibility and tolerance? (5) Is this treatment curative intent, disease control, or quality-of-life focused? A board-certified thoracic oncologist or subspecialty lung cancer oncologist is the right specialist for this conversation.
17. Can lung cancer go into remission?
Complete remission — no detectable evidence of disease on imaging — is achievable in early-stage NSCLC following complete surgical resection. In advanced NSCLC, partial or complete response to targeted therapy or immunotherapy represents active disease control, monitored with serial CT imaging and, increasingly, circulating tumor DNA (ctDNA) testing. Remission in advanced-stage disease is not equivalent to cure in most cases. Consult a board-certified oncologist about how treatment response is defined, monitored, and communicated for your specific cancer type and stage.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.