On This Page – Quick Medical Summary
What Is Liquid Biopsy and Why Do Lung Cancer Patients Need to Know?
If your oncologist mentioned liquid biopsy and you left the appointment uncertain about whether it is accurate enough to stake a treatment decision on, you are asking the right question.
A liquid biopsy for lung cancer is a blood test that detects circulating tumor DNA (ctDNA) — fragments of DNA shed by cancer cells into the bloodstream — allowing oncologists to identify tumor-driving mutations without a surgical tissue sample.
This is not a cancer screening test. It is a precision diagnostic and monitoring tool for patients already in active lung cancer care. In the right clinical situation, it changes treatment.
For a complete orientation to how lung cancer develops, is staged, and is diagnosed, our complete guide to what lung cancer is and how it is treated is the right starting point. If unexplained symptoms are still driving your search, our lung cancer symptom checker can help you organize what to bring to a first oncology appointment.
ℹ️ Medical Disclaimer: The diagnostic criteria, mutation testing protocols, treatment approaches, medication references, and insurance coverage information discussed in this article reflect current clinical guidelines and are provided for educational purposes only. Individual diagnostic conclusions, treatment decisions, and medication choices depend on patient history, comorbidities, specific tumor characteristics, test results, and specialist assessment. Consult a board-certified thoracic oncologist before acting on any clinical information in this article.
Who Should Get a Liquid Biopsy for Lung Cancer?
Liquid biopsy is not appropriate for every lung cancer patient. The 2026 NCCN Non-Small Cell Lung Cancer Guidelines endorse it for specific clinical scenarios — and knowing whether your situation fits one of those scenarios is the most important thing you can accomplish before your next oncology appointment.
When initial mutation profiling calls for a liquid biopsy
The 2026 NCCN guidelines identify three primary indications for liquid biopsy as the preferred or concurrent biomarker testing strategy in NSCLC:
- Tissue is insufficient. The tissue sample obtained through bronchoscopy or CT-guided needle biopsy contains too few tumor cells for standard next-generation sequencing. This is not an uncommon finding — it occurs frequently enough that liquid biopsy is now the standard fallback, not an experimental option.
- Tissue biopsy is technically infeasible. The tumor is positioned near a major vessel, in a high-risk anatomical location, or too small to safely re-sample. In these patients, liquid biopsy is not an alternative — it is the only viable real-time molecular testing option.
- Treatment monitoring and resistance detection. After a patient begins targeted therapy, serial ctDNA testing can detect acquired resistance mutations — such as T790M in EGFR-mutant NSCLC — before clinical or radiological progression becomes visible on imaging.
Understanding how lung cancer is staged is essential context here — stage significantly affects whether liquid biopsy is recommended as an initial or concurrent testing strategy.
When tissue biopsy is still the required first step
Liquid biopsy cannot make a histologic diagnosis. If the clinical team has not yet confirmed whether the tumor is non-small cell, small cell, or squamous cell lung cancer, tissue is required. That histologic distinction drives the entire treatment pathway — and no ctDNA result can substitute for it.
Using liquid biopsy to monitor treatment and detect resistance
Once a patient is on targeted therapy, many oncologists order serial ctDNA testing at 8–12 week intervals or at signs of clinical progression. A rising ctDNA level frequently signals emerging resistance weeks before a CT scan shows new tumor growth — giving the treatment team time to pivot before progression becomes clinically apparent.
To understand your inherited cancer risk factors before your specialist appointment, our genetic cancer risk assessment tool provides a structured starting point. For context on population-level screening programs that precede diagnosis, our lung cancer screening guidelines article covers low-dose CT eligibility criteria.
✅ Patient Action: Before your next oncology appointment, ask specifically: “Based on my tumor stage, location, and the adequacy of my tissue sample, does the 2026 NCCN guideline support liquid biopsy as my initial or concurrent testing strategy?” This question has a different answer for different patients — your oncologist determines which scenario applies to your case.
How ctDNA Testing Works: From Blood Draw to Results
Understanding what happens between your blood draw and your mutation report gives you the context to ask informed questions about test quality, laboratory certification, and what your specific results mean.
🔬 How It Works: Tumor cells are constantly dying through a process called apoptosis. As they break down, they release fragments of their DNA into the bloodstream — including DNA carrying the mutations driving the cancer. These fragments, called cell-free DNA (cfDNA), circulate in the plasma alongside DNA released by normal healthy cells. The tumor-derived fraction of that cfDNA is ctDNA — and it carries the molecular fingerprint of the cancer. In advanced NSCLC, ctDNA represents a detectable fraction of total cfDNA. In early-stage disease, that fraction is much smaller, which is why sensitivity is lower and false negatives are more common outside of advanced disease.
How tumor cells release DNA into your bloodstream
One clinically important nuance every patient should understand: older patients and those who have received prior chemotherapy can develop clonal hematopoiesis of indeterminate potential (CHIP) — somatic mutations arising in white blood cells that are entirely unrelated to the lung tumor.
CHIP mutations appear in cfDNA and can mimic ctDNA signals, creating false-positive findings that could mislead treatment decisions. High-quality, CLIA-certified laboratories use paired white blood cell sequencing to distinguish tumor-derived mutations from CHIP artifacts. Ask whether the laboratory your oncologist is using performs this step — it is a marker of analytical rigor that directly affects the reliability of your result.
What happens in the lab: NGS sequencing and mutation calling
The ctDNA testing process follows these steps in order:
- Blood draw — a standard venous blood draw, typically 2–4 tubes
- Plasma separation — centrifugation isolates the plasma, which contains the cfDNA, from the cellular blood components
- cfDNA extraction — cfDNA fragments are purified from the plasma
- Library preparation — cfDNA fragments are prepared for sequencing through adapter ligation and amplification
- Next-generation sequencing (NGS) — the library is sequenced across millions of cfDNA reads simultaneously
- Mutation calling and VAF analysis — bioinformatics algorithms identify mutations present in the reads and calculate the variant allele frequency (VAF) — the proportion of reads at a given position that carry the mutation
Think of VAF as a signal-to-noise ratio. A VAF of 2.0% means 2 in every 100 cfDNA reads at that position carry the mutation. Most clinical laboratories require a VAF above a reporting threshold — typically 0.5% or higher — before calling a variant as a confirmed finding.
Understanding your liquid biopsy report: what the numbers mean
Your report will list each detected mutation, its VAF, and its classification — pathogenic, likely pathogenic, or variant of uncertain significance. A low VAF does not automatically mean clinical irrelevance. It may reflect low tumor burden, early treatment response, or the presence of a mutation in a small resistant subclone that your oncologist needs to monitor.
The NCI’s overview of liquid biopsy applications in cancer diagnosis and monitoring documents the clinical evidence base underpinning ctDNA testing.
For context on how liquid biopsy fits alongside other diagnostic tools, our article on how lung cancer is diagnosed covers imaging, tissue biopsy, and molecular testing together. Our lung biopsy for cancer article explains the traditional tissue biopsy procedure — useful for understanding exactly what liquid biopsy is and is not replacing.
🩺 Physician Note: “The most common misunderstanding patients bring to a liquid biopsy conversation is that the blood draw replaces all further tissue sampling. It does not. In my oncology practice, when a patient has adequate tissue, I want both — liquid biopsy and tissue NGS — because they answer different clinical questions. What liquid biopsy replaces is the need for repeat invasive sampling when tissue is insufficient, when re-biopsy carries prohibitive risk, or when I need real-time resistance monitoring without subjecting the patient to another procedure.” — Dr. Nathaniel J. Hargrove, MD (Oncology)
What Mutations Can Liquid Biopsy Detect in Lung Cancer?
The mutations detectable by liquid biopsy depend entirely on the platform your oncologist orders — not all FDA-authorized ctDNA platforms cover the same mutation panel, and the distinction matters for treatment selection.
The FDA-authorized ctDNA testing information page documents currently cleared platforms and their validated indications.
Targetable driver mutations found through liquid biopsy
These are the mutations your oncologist uses to match you to a specific targeted therapy at diagnosis or disease recurrence:
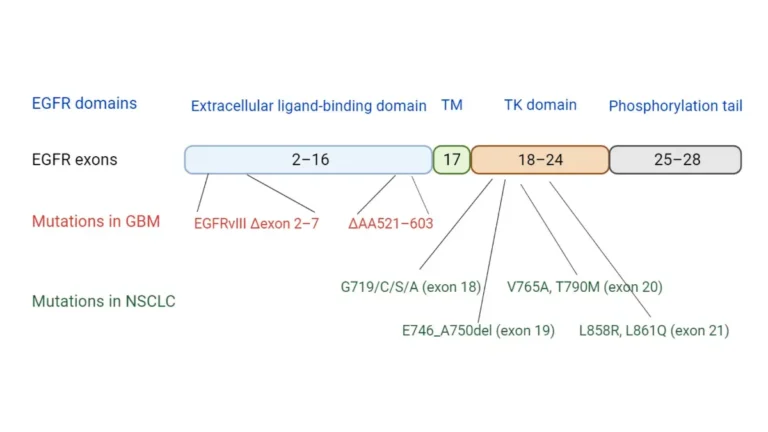
- EGFR exon 19 deletions and exon 21 L858R substitution — the most common targetable driver mutations in NSCLC; treated with osimertinib and other EGFR-specific tyrosine kinase inhibitors (TKIs)
- ALK rearrangements — detected via cfDNA-based fusion analysis; treated with alectinib, brigatinib, or lorlatinib depending on prior treatment history
- ROS1 fusions — treated with entrectinib and crizotinib
- KRAS G12C mutation — targetable with sotorasib and adagrasib following FDA approval; detectable in plasma with strong sensitivity in advanced disease
- MET exon 14 skipping mutations — treated with tepotinib and capmatinib
- RET fusions — treated with selpercatinib and pralsetinib
- BRAF V600E mutation — treated with the dabrafenib plus trametinib combination
Our article on lung cancer genetic testing and biomarker analysis explains how oncologists integrate liquid biopsy mutation results alongside histologic diagnosis to build a full molecular profile. For a complete breakdown of which targeted drugs are FDA-approved against each mutation in 2026, see our 2026 lung cancer FDA-approved treatments guide.
Resistance mutations: detecting why treatment stops working
This is where liquid biopsy offers its most clinically distinctive value — identifying acquired resistance before it becomes clinically or radiologically apparent:
- T790M mutation — the most common acquired resistance mechanism to first- and second-generation EGFR TKIs; liquid biopsy detects T790M with high sensitivity and can redirect treatment to osimertinib before the patient experiences overt clinical progression
- C797S mutation — an acquired resistance mechanism to osimertinib itself; signals the need for alternative strategies or clinical trial evaluation
- MET amplification — a resistance bypass mechanism that can develop during EGFR TKI therapy; detectable via NGS-based copy number analysis in plasma
- KRAS secondary mutations — emerging resistance signals in patients receiving KRAS G12C inhibitors
Once a targetable resistance mutation is identified, treatment options expand significantly. Our targeted therapy options for lung cancer by mutation type article explains how oncologists use both driver and resistance mutation profiles to select and sequence treatments.
How long liquid biopsy results take and what to expect
Standard turnaround time at CLIA-certified, CAP-accredited laboratories is 10–14 business days from sample receipt. Expedited processing on certain platforms shortens that to 5–7 business days for patients with urgent treatment planning timelines. Your oncologist’s office receives results electronically and will schedule a follow-up to review findings.
Choosing a CLIA-certified, FDA-authorized testing platform
Before your blood is drawn, ask your oncologist’s team specifically whether the receiving laboratory is CLIA-certified and CAP-accredited. These are not optional quality designations — they are the minimum analytical validation standards required for a ctDNA result to be used in a clinical treatment decision.
✅ Patient Action: Ask your oncology team specifically: “Which ctDNA testing platform does this institution use, is it FDA-authorized for my specific mutation type, and is the laboratory CLIA-certified and CAP-accredited?” Analytical sensitivity for specific mutations varies significantly between platforms — this is a question worth asking before your blood is drawn.
Liquid Biopsy vs. Tissue Biopsy: How Accurate Is Each?
Every newly diagnosed NSCLC patient eventually asks this question. It deserves a direct, data-anchored clinical answer — not a vague reassurance that both are “good options.”
The 2026 NCCN Non-Small Cell Lung Cancer Guidelines establish clearly: liquid biopsy and tissue biopsy are complementary tools, not interchangeable ones. Each has defined strengths and defined failure modes. Knowing both is what allows you to ask the right questions in your oncology appointments.
📊 Clinical Data Point: In patients with advanced NSCLC and sufficient tumor burden, liquid biopsy demonstrates high concordance with matched tissue NGS for key driver mutations including EGFR exon 19 deletions, L858R, ALK rearrangements, and KRAS G12C. Concordance is highest in Stage III–IV disease and declines substantially in Stage I–II, where lower ctDNA concentrations increase false negative rates. — Source: NCCN 2026 Non-Small Cell Lung Cancer Clinical Guidelines; 2026 peer-reviewed oncology literature
| Criterion | Liquid Biopsy | Tissue Biopsy | Best For Patient Profile |
|---|---|---|---|
| Invasiveness | Non-invasive (blood draw only) | Invasive (needle, bronchoscope, or surgery) | Patients where repeat biopsy carries procedural risk |
| Turnaround time | 5–14 business days | 7–21 days including processing | Time-sensitive treatment planning in advanced disease |
| Sensitivity — advanced NSCLC | High for established driver mutations with sufficient tumor burden | Gold standard sensitivity | Patients with Stage III–IV and high tumor burden |
| Sensitivity — early-stage NSCLC | Lower — reduced ctDNA levels near limit of detection | High | Early-stage patients requiring definitive profiling |
| Histologic assessment | Cannot assess tumor cell type or histologic transformation | Required for all histologic diagnosis | Any patient needing cell-type confirmation |
| Tumor heterogeneity sampling | Samples circulating DNA from multiple tumor regions simultaneously | Samples one anatomical tumor region only | Patients with suspected spatially heterogeneous tumors |
| Cost range (est.) | $1,800–$5,000 (comprehensive NGS panels) | $500–$3,000 (varies by approach) | Insurance-covered scenario preferred for both |
| NCCN 2026 preferred use | Tissue-insufficient; technically infeasible biopsy; resistance monitoring | Initial histologic diagnosis; early-stage profiling | Determined by stage, tissue adequacy, and tumor accessibility |
Source: NCCN 2026 Non-Small Cell Lung Cancer Clinical Practice Guidelines. Cost ranges are estimates
Concordance rate: how often liquid and tissue results agree
In advanced NSCLC with high tumor burden, agreement between liquid biopsy and tissue NGS for actionable driver mutations is clinically meaningful and sufficient to support treatment decision-making when tissue is inadequate. However, concordance is not 100%. Discordant results — where liquid biopsy is positive but tissue is negative, or vice versa — occur and require oncologist interpretation, not automatic action.
The most common source of false discordance is low tumor burden in the plasma sample. When a mutation is identified in tissue but not in a ctDNA result, the most likely explanation is that the ctDNA concentration falls below the platform’s limit of detection — not that the mutation is absent from the tumor.
False negatives: when liquid biopsy misses the mutation
A negative liquid biopsy result does not mean the tumor is mutation-free or that cancer is absent. False negative rates increase substantially in Stage I and II NSCLC, where lower tumor burden means lower ctDNA concentrations in plasma. The standard clinical protocol when liquid biopsy returns negative in the face of strong clinical suspicion: reflex to tissue biopsy. A negative ctDNA result is a signal to look harder — not a signal to stop.
When tissue biopsy is still required — and why
Two clinical scenarios require tissue regardless of liquid biopsy availability:
- Histologic diagnosis has not been established. Liquid biopsy cannot tell your oncologist whether the tumor is non-small cell, small cell, or squamous cell. That distinction determines the entire treatment framework — and no ctDNA result substitutes for it.
- Histologic transformation is suspected as a resistance mechanism. In EGFR-mutant NSCLC, small cell transformation is a documented acquired resistance pathway. Liquid biopsy detects acquired mutations but cannot detect a cell-type transformation — that requires tissue morphology assessment.
The NCCN 2026 Non-Small Cell Lung Cancer guidelines specify the precise scenarios where liquid biopsy is the preferred strategy and where tissue remains mandatory. Free NCCN account required.
For a complete overview of how mutation profiling translates into treatment selection, our lung cancer treatment options guide covers how oncologists use both driver and resistance mutation profiles across therapy lines.
✅ Patient Action: Before proceeding on a liquid biopsy result alone — positive or negative — ask your board-certified thoracic oncologist specifically: “Given my stage and tumor burden, does my clinical team recommend confirming this ctDNA result with a tissue sample before we finalize the treatment plan?” In advanced disease with confirmed high tumor burden, an experienced oncologist may proceed with targeted therapy on a liquid biopsy result. In early-stage or low-VAF findings, tissue confirmation is typically the safer clinical path.
Does Insurance Cover Liquid Biopsy for Lung Cancer?
The cost of liquid biopsy is one of the most common concerns patients never raise with their oncologist — because they assume the answer is either automatic approval or automatic denial. The reality is more navigable than either assumption, and knowing how to navigate it is the difference between accessing this test and going without it.
What Medicare covers for liquid biopsy in lung cancer
As of 2026, Medicare covers NGS-based liquid biopsy for eligible beneficiaries with advanced solid tumors — including advanced NSCLC — under the applicable Local Coverage Determination (LCD) for next-generation sequencing companion diagnostic testing. Coverage applies when the test is ordered by a treating oncologist, performed by a CLIA-certified and CAP-accredited laboratory, and accompanied by clinical documentation confirming the patient meets the coverage criteria.
📊 Clinical Data Point: Medicare’s 2026 coverage for ctDNA-based comprehensive genomic profiling applies to patients with advanced cancer (typically Stage III–IV) when the test is ordered for treatment selection or resistance monitoring and is performed by a laboratory meeting CMS quality standards. Coverage for early-stage MRD monitoring applications is more variable and plan-dependent — source: Medicare coverage database for next-generation sequencing.
Private insurance coverage: what criteria you need to meet
Most major commercial payers follow a framework similar to Medicare but layer in prior authorization requirements that vary significantly by plan. Standard documentation requirements include:
- A confirmed diagnosis of advanced NSCLC (typically Stage III or IV)
- Evidence that tissue biopsy was attempted and found insufficient, or was technically infeasible
- An ordering physician with board-certified oncology credentials
- A clinical rationale note referencing the applicable NCCN 2026 guideline support
Prior authorization denials on first submission are common — and commonly overturned on appeal when the oncologist’s team submits complete documentation. Do not treat an initial denial as final without requesting a peer-to-peer review between your oncologist and the insurer’s medical director.
Out-of-pocket cost ranges and access options without full coverage
Without insurance coverage, comprehensive NGS-based liquid biopsy panels cost approximately $1,800–$5,000 depending on the platform, the mutation panel scope, and whether expedited processing is required. Three access pathways exist for patients facing coverage gaps:
- Manufacturer patient assistance programs — most major ctDNA platform companies offer financial assistance for patients below income thresholds; your oncologist’s patient navigator can identify the relevant program for your specific platform.
- Clinical trial enrollment — many active trials provide liquid biopsy testing at no patient cost. Active trials are searchable by location, stage, and biomarker status at ClinicalTrials.gov’s lung cancer liquid biopsy registry. Our lung cancer clinical trials guide explains the enrollment process and what to ask trial coordinators.
- NCI-designated cancer center financial assistance — many centers offer institutional financial assistance programs for comprehensive biomarker testing that are not widely advertised; the cancer center’s social worker or financial counselor is the fastest path to this information.
✅ Patient Action: Before assuming your insurance will deny liquid biopsy, ask your oncologist’s billing coordinator specifically: “Can you submit a prior authorization request for this ctDNA platform under the CMS Local Coverage Determination for next-generation sequencing — and what documentation do you need from the oncologist to complete the submission?” A complete prior authorization with the oncologist’s clinical rationale and the NCCN 2026 guideline reference significantly improves first-submission approval rates.
What Your Oncologist Wants You to Know About Liquid Biopsy
If I had one conversation with every lung cancer patient before their liquid biopsy results arrived, I would cover three things — because these are the three misunderstandings that lead to the hardest post-result conversations.
Liquid biopsy is one of the most meaningful advances in lung cancer care in the past decade. It has made real-time resistance monitoring possible without repeat invasive procedures. It has changed how quickly we can identify a treatment change is needed. In the right clinical situation, it has saved patients from weeks of ineffective therapy.
And it has three limits you need to understand before you see your report.

Three things liquid biopsy cannot tell your oncologist
First: it cannot assess tumor histology. If your EGFR-mutant NSCLC has undergone small cell transformation — a documented acquired resistance mechanism — liquid biopsy cannot detect that transformation. A ctDNA panel showing no new mutations in a clinically progressing patient is sometimes a signal that the resistance mechanism is histologic, not molecular. That requires tissue.
Second: it cannot guarantee a complete mutation landscape. Different regions of the same tumor can carry different mutations — tumor heterogeneity is real and clinically significant. Liquid biopsy captures ctDNA shed from multiple tumor regions simultaneously, which often gives a broader view than a single-site tissue biopsy. But it can still miss mutations present only in spatially restricted subclones not releasing sufficient ctDNA into circulation.
Third: a negative result is not a clean bill of health. In patients with early-stage NSCLC or very low tumor burden, ctDNA may fall below the platform’s limit of detection even when active disease and targetable mutations are present. A negative result in that context means we need to look harder — with tissue or with repeat testing — not that the answer is reassuring.
How to use your liquid biopsy results in your care conversations
Bring your report to the appointment. Ask your oncologist to walk through every mutation listed, what each VAF tells them about tumor burden or treatment response, and what the absence of a mutation they expected means clinically. That specific conversation, grounded in your actual result, is where liquid biopsy delivers its value.
🩺 Physician Note: “What I want every patient to leave this conversation knowing: liquid biopsy is a powerful tool that my team interprets in clinical context — not a standalone verdict. When a patient brings their report and asks specific questions about each finding, we have our best, most productive treatment conversations. That engagement changes outcomes.” — Dr. Nathaniel J. Hargrove, MD (Oncology)
✅ Patient Action: Before acting on any liquid biopsy result — positive or negative — have a specific conversation with your board-certified thoracic oncologist about what the result means for your stage, mutation history, and treatment trajectory. Liquid biopsy results are always interpreted by a specialist in full clinical context. They are never interpreted from a laboratory report alone.
Liquid Biopsy for Lung Cancer: Frequently Asked Questions
Q1: What is liquid biopsy for lung cancer?
A liquid biopsy for lung cancer is a blood test that detects circulating tumor DNA (ctDNA) — fragments of DNA shed by cancer cells into the bloodstream. It allows oncologists to identify tumor-driving mutations without a surgical tissue sample. It is used for initial mutation profiling when tissue is inadequate, for monitoring treatment response, and for detecting acquired resistance mutations in patients on targeted therapy.
Q2: How does ctDNA testing work?
A standard blood draw collects plasma containing cell-free DNA (cfDNA), including any ctDNA shed by the tumor. The plasma is processed to isolate cfDNA, which undergoes next-generation sequencing (NGS). Bioinformatics algorithms then identify mutations in the sequencing reads and calculate the variant allele frequency (VAF) — the proportion of cfDNA reads carrying each mutation — to produce a clinical mutation report.
Q3: Is liquid biopsy as accurate as tissue biopsy for lung cancer?
In advanced NSCLC with sufficient tumor burden, liquid biopsy shows high concordance with tissue NGS for key driver mutations including EGFR, ALK, and KRAS G12C. Accuracy declines substantially in Stage I and II disease, where lower ctDNA concentrations increase false negative rates. Liquid biopsy cannot assess tumor histology under any circumstance. Consult a board-certified thoracic oncologist before making any treatment decision based on liquid biopsy results alone.
Q4: What mutations can liquid biopsy detect in lung cancer?
FDA-authorized ctDNA platforms for NSCLC detect driver mutations including EGFR exon 19 deletions and L858R, ALK rearrangements, ROS1 fusions, KRAS G12C, MET exon 14 skipping, RET fusions, and BRAF V600E. They also detect acquired resistance mutations including T790M, C797S, and MET amplification. The specific panel covered varies by platform — confirm with your oncologist which mutations are included before the test is ordered.
Q5: How long does liquid biopsy take to get results?
Standard turnaround time at most CLIA-certified, CAP-accredited laboratories is 10–14 business days from sample receipt. Expedited processing is available on certain FDA-authorized platforms in 5–7 business days for patients with urgent treatment planning needs. Your oncologist’s office receives results electronically and will contact you to schedule a results review appointment once findings are available.
Q6: Does insurance cover liquid biopsy for lung cancer?
As of 2026, Medicare covers NGS-based liquid biopsy for eligible advanced solid tumor patients, including advanced NSCLC, when ordered by a treating oncologist and performed by a CLIA-certified and CAP-accredited laboratory. Most major private insurers cover liquid biopsy for advanced NSCLC with prior authorization, requiring clinical documentation and a NCCN 2026 guideline reference. Coverage for early-stage monitoring applications is more variable and plan-dependent.
Q7: What is the difference between liquid biopsy and tissue biopsy?
Liquid biopsy detects ctDNA from a non-invasive blood draw and has a turnaround of 5–14 days. Tissue biopsy provides a physical tumor sample that allows histologic diagnosis and is required for initial cell-type confirmation. Liquid biopsy cannot assess tumor histology or detect histologic transformation; tissue biopsy cannot monitor real-time resistance as effectively. Neither replaces the other completely — they answer different clinical questions. Consult a board-certified thoracic oncologist to determine which approach your clinical situation requires.
Q8: Can liquid biopsy detect early-stage lung cancer?
Liquid biopsy is significantly less sensitive in Stage I and II NSCLC than in advanced disease. Lower tumor burden means lower ctDNA concentrations in plasma — often approaching or falling below the platform’s limit of detection. A negative liquid biopsy result in early-stage disease does not rule out the presence of targetable mutations. Tissue biopsy remains the preferred profiling strategy for resectable early-stage NSCLC where tissue is accessible.
Q9: What happens if liquid biopsy comes back negative?
A negative liquid biopsy result means no mutations were detected above the platform’s reporting threshold — it does not confirm the tumor is mutation-free or that cancer is absent. False negative rates are highest in Stage I and II disease due to low ctDNA concentrations. The standard clinical protocol at most NCI-designated cancer centers when liquid biopsy returns negative in the face of strong clinical suspicion is reflex tissue biopsy. Never interpret a negative ctDNA result as reassuring without your oncologist reviewing it in full clinical context. Consult a board-certified thoracic oncologist before drawing any treatment conclusions from a negative liquid biopsy result.
Q10: How much does liquid biopsy cost without insurance?
Without insurance coverage, comprehensive NGS-based liquid biopsy panels typically cost between $1,800 and $5,000 depending on the platform, mutation panel scope, and whether expedited processing is needed. Manufacturer patient assistance programs, clinical trial enrollment, and NCI-designated cancer center financial assistance programs are three access pathways available to patients without adequate coverage. Ask your oncology team’s patient navigator about all three options before paying out of pocket.
Q11: Who should get a liquid biopsy for lung cancer?
According to the 2026 NCCN Non-Small Cell Lung Cancer Guidelines, liquid biopsy is the preferred biomarker testing strategy when tissue is insufficient for NGS, when repeat tissue biopsy is technically infeasible, or when treatment monitoring and acquired resistance detection are the clinical objective. It is not appropriate as a standalone cancer screening tool. Consult a board-certified thoracic oncologist to determine whether your clinical situation meets the current guideline criteria for liquid biopsy.
Q12: Can liquid biopsy monitor lung cancer treatment response?
Yes. Serial ctDNA testing is used as a surrogate marker for treatment response in patients on targeted therapy. A declining or undetectable ctDNA level during treatment correlates with tumor response, while a rising level can signal emerging resistance weeks before radiological progression appears on imaging. Monitoring intervals typically range from every 8–12 weeks on active targeted therapy to at-progression testing. Your oncologist determines the appropriate monitoring schedule for your specific regimen.
Q13: What is ctDNA and how is it different from regular DNA?
Circulating tumor DNA (ctDNA) is the subset of cell-free DNA in blood plasma that is derived specifically from cancer cells rather than healthy cells. Regular germline DNA is inherited and stable in every cell of the body; ctDNA carries the somatic mutations driving the cancer and is shed into the bloodstream as tumor cells die. ctDNA has a plasma half-life of under two hours, making it a real-time molecular window into the tumor’s current mutation status.
Q14: Which labs perform liquid biopsy for lung cancer?
Clinical laboratories performing liquid biopsy must be CLIA-certified and CAP-accredited to meet the minimum quality standards required for clinical use. FDA-authorized ctDNA platforms are available through hospital-based molecular pathology laboratories and specialized commercial molecular diagnostics companies. Your oncologist’s institution typically works with an established laboratory. Ask specifically whether the receiving laboratory is CLIA-certified and whether the platform used is FDA-authorized for your specific mutation type before the test is submitted.
Q15: Can liquid biopsy replace tissue biopsy for lung cancer?
Liquid biopsy cannot replace tissue biopsy entirely. The 2026 NCCN Non-Small Cell Lung Cancer Guidelines recommend liquid biopsy when tissue is insufficient or biopsy is technically infeasible — not as a universal replacement. Tissue biopsy remains required for initial histologic diagnosis, for distinguishing NSCLC from SCLC, and when histologic transformation is suspected as an acquired resistance mechanism. Consult a board-certified thoracic oncologist before declining a tissue biopsy because liquid biopsy is available.
Q16: How often should lung cancer patients get liquid biopsy testing?
Monitoring frequency depends on treatment phase and clinical objective. Most oncologists order ctDNA testing every 8–12 weeks during active targeted therapy and at clinical or radiological progression to identify acquired resistance mutations. In post-surgical settings, ctDNA monitoring protocols for minimal residual disease (MRD) detection are being established through ongoing 2026 clinical trials. Your oncologist determines the appropriate interval for your specific treatment regimen and disease stage. Consult a board-certified thoracic oncologist before establishing or changing any monitoring schedule.
Q17: What are the main limitations of liquid biopsy for lung cancer?
The principal limitations are: reduced sensitivity in early-stage disease due to low ctDNA concentrations; false-positive signals from clonal hematopoiesis (CHIP) mutations in older patients; inability to assess tumor histology or detect histologic transformation; potential to miss spatially restricted mutations due to tumor heterogeneity; and a limit of detection threshold below which mutations are not reported even when present. All liquid biopsy results must be interpreted by a board-certified thoracic oncologist in the context of complete clinical, imaging, and pathologic data.
Your Next Step After Reading About Liquid Biopsy
You now understand what liquid biopsy is, who qualifies for it, what happens in the lab, which mutations it finds, how its accuracy compares to tissue biopsy, what it costs, and — critically — what it cannot do.
That understanding is the foundation of a better oncology appointment.
Your specific next step: bring three questions to your board-certified thoracic oncologist. First, whether liquid biopsy is guideline-recommended for your stage and tissue status. Second, which FDA-authorized platform your institution uses and whether it covers your specific mutation type. Third, what prior authorization documentation your billing team needs to secure insurance approval.
This article was written by Dr. Nathaniel J. Hargrove, MD, board-certified oncologist, and reviewed by two additional board-certified physicians as part of the mymedicineadvisor.com 54-member Global Medical Advisory Board — because the decisions you face deserve the same rigorous physician review your treatment team applies to your care.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.