On This Page – Quick Medical Summary
What to expect with urine leakage after prostate surgery
If your catheter just came out and you’re leaking urine, the first thing to know is that this is expected after a radical prostatectomy — not a sign that something went wrong. For most men, bladder control returns gradually over the weeks and months that follow.
This guide meets you wherever you are. If your catheter was just removed, skip to the recovery timeline. If you’re preparing for surgery, the next two sections explain why leakage happens and which type to expect. If leakage has lasted many months, the treatment section covers your options. And if you’re a partner or caregiver, the self-management and warning-sign sections are written with you in mind.
What follows is grounded in guidance from the American Cancer Society and major cancer centers, with realistic timelines and honest numbers — because urinary incontinence after prostatectomy is one of the most common and most worried-about parts of recovery. You can see how it fits the bigger picture in our overview of prostate cancer treatment and recovery.
ℹ️ Medical Disclaimer: This article is general health education, not personalized medical advice. It does not diagnose any condition, prescribe or dose any medication, or recommend any specific procedure, device, or surgery for you. Decisions about managing incontinence, taking medication, or pursuing a sling or artificial urinary sphincter should be made with a board-certified urologist who knows your history. If you cannot urinate at all, or have signs of infection or significant bleeding, seek prompt medical care.
Why prostate surgery causes urine leakage
Continence depends on two valves, and prostate surgery removes one of them. Understanding that single fact makes the leakage far less frightening.
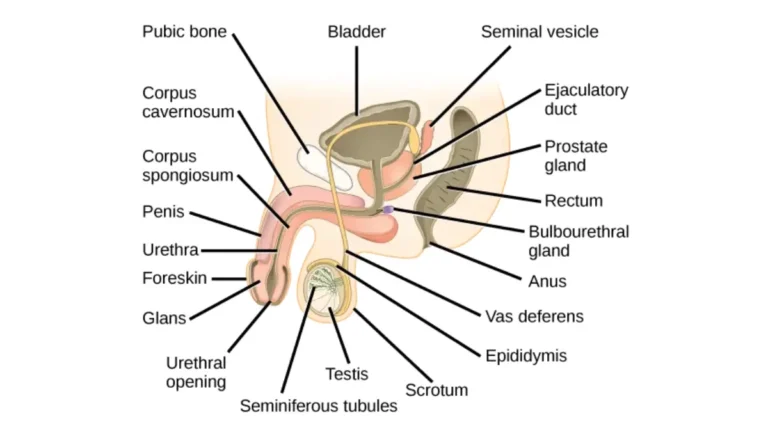
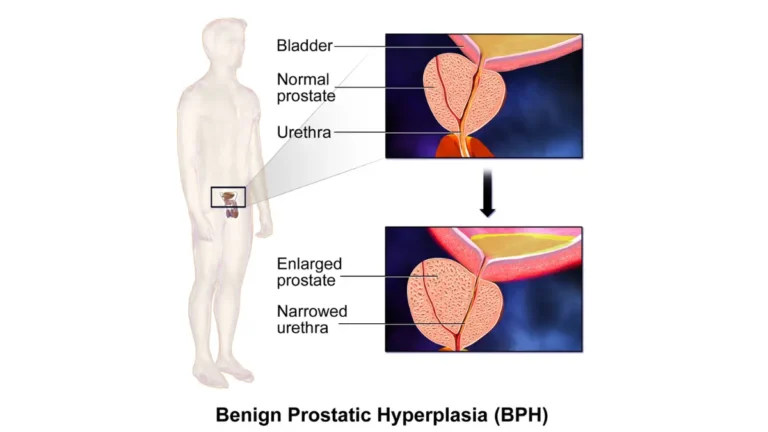
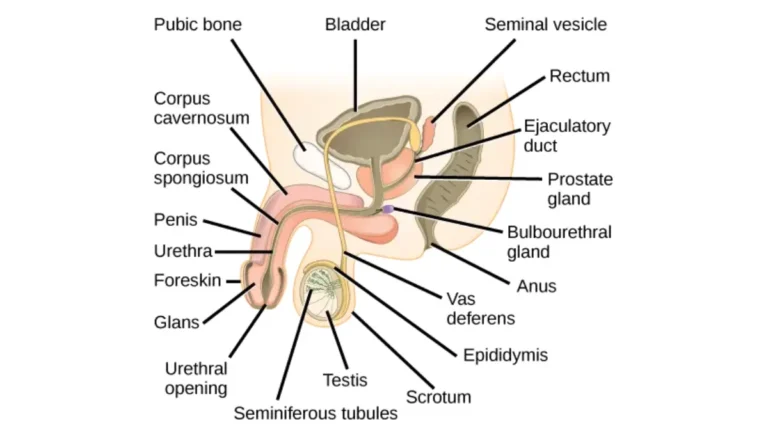
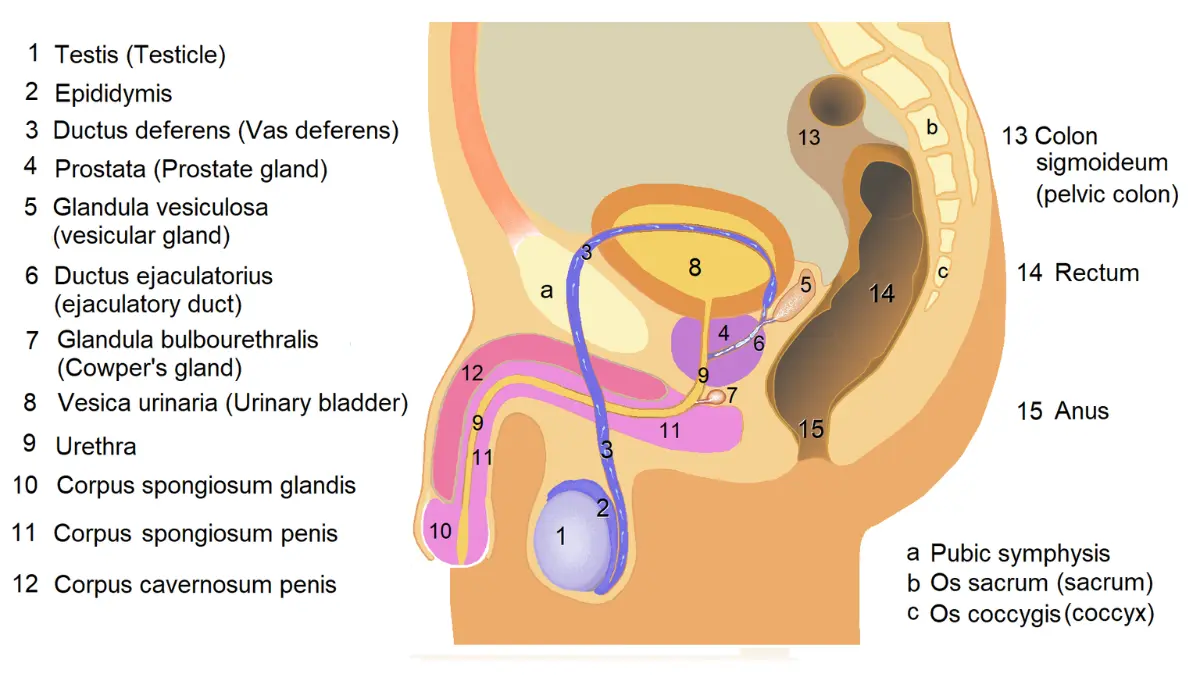
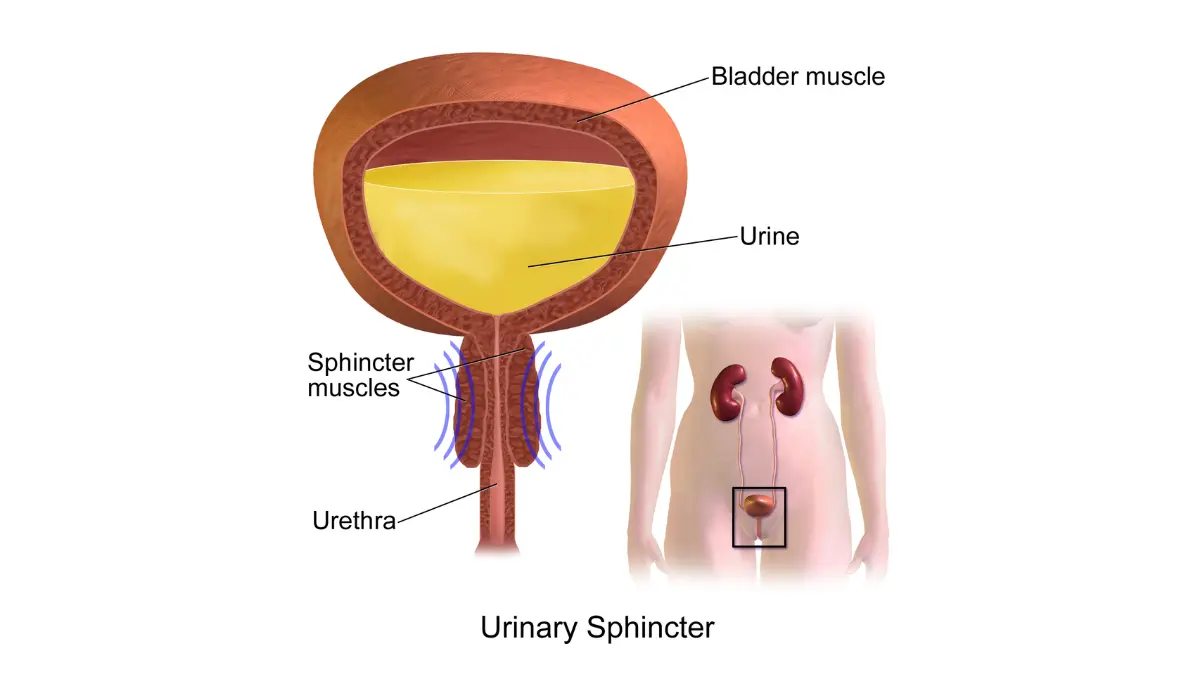
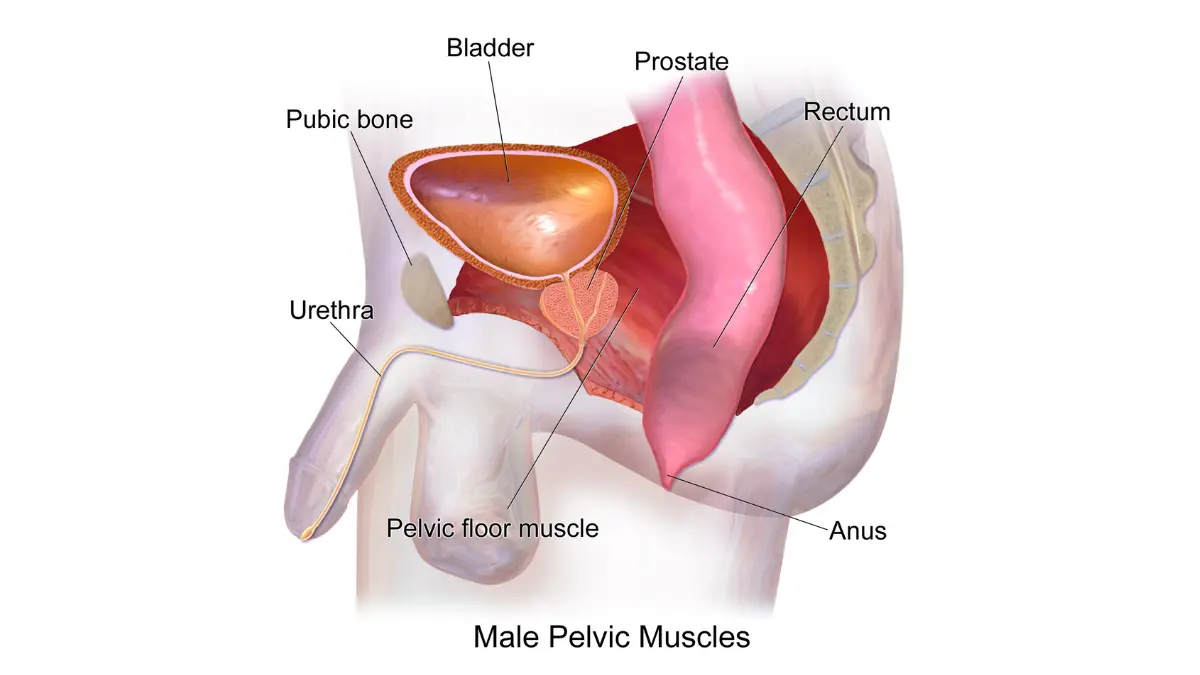
🔬 How It Works: You have two urinary sphincters. The internal urethral sphincter sits at the bladder neck, works automatically, and is removed along with the gland during surgery because it surrounds the top of the prostate. The external urethral sphincter sits just below where the prostate was — it’s the muscle you squeeze to stop your urine stream, and after surgery it becomes your primary continence control.
With the internal valve gone, your external sphincter and pelvic floor muscles do the whole job alone. According to the American Cancer Society’s overview of prostate surgery side effects, surgery can also bruise or stretch the nerves and muscle around this valve, which is why leakage is common at first and usually eases as those tissues recover. Surgeon experience matters too — the ACS notes that high-volume cancer centers generally report fewer long-term incontinence problems.
Does nerve-sparing surgery reduce leakage?
Nerve-sparing technique is linked to better continence recovery, though it isn’t a guarantee. Johns Hopkins Medicine reports that up to 30–50% of men with normal urinary function before surgery notice some increase in urinary symptoms or urgency afterward, and that this appears reduced when a nerve-sparing approach is used. The nerve bundles sit on either side of where the prostate was, which is why surgeons weigh nerve-sparing carefully against fully removing the cancer.
Stress vs. urge incontinence: which type do you have?
Knowing your leakage pattern matters, because the two main types behave differently and respond to different approaches. Many men have one type; some have a mix.
Stress incontinence is leakage triggered by effort — coughing, sneezing, laughing, lifting, or exercise — when abdominal pressure overwhelms the weakened external sphincter. Per the American Cancer Society, stress urinary incontinence is the most common type after prostate surgery.
Urge incontinence is a sudden, strong need to urinate that you can’t hold back, sometimes caused by bladder spasms (an overactive bladder). Unlike stress leakage, the urge type often responds to specific bladder-calming medications, because it reflects changes in how the bladder muscle behaves after surgery rather than a problem with the sphincter.
How doctors tell the types apart
Your care team usually identifies the type from your history and how much you leak, often tracked by pad use; in less clear cases, urodynamic testing measures bladder pressure and flow. The type matters because it changes the plan — the irritative, frequency-and-urgency pattern is also typical of urinary side effects of radiation therapy, which differ from surgery’s stress-leak pattern.
✅ Patient Action: At your follow-up, ask your urologist: “Is my leakage stress, urge, or mixed — and does that change what we try first?” The answer shapes whether pelvic floor work, bladder medication, or both make the most sense.
How long does urinary incontinence last after prostatectomy?
Most men improve steadily over the first several months, with the majority regaining bladder control by around the one-year mark. Here is the realistic stage-by-stage picture.
A urinary catheter stays in place for roughly 1–2 weeks (often about 7–10 days) after surgery, and leakage when it comes out is normal. From there, the American Cancer Society describes bladder control improving slowly over weeks to months. Memorial Sloan Kettering Cancer Center notes that for most men leakage almost fully resolves by 12 months — and that if it hasn’t improved by then, it’s time to see a urologist for further management.
📊 Clinical Data Point: In series from experienced surgeons, roughly 10–15% of men report frequent leakage or needing pads at 6 months, and fewer than 10% report using any pads by 3 years — Source: Johns Hopkins Medicine. Reported figures vary by source and by how “continence” is defined; some patient organizations cite higher early rates (around 25% at 6 months, per ZERO Prostate Cancer), reflecting different definitions rather than a contradiction.
What percentage of men fully recover?
Most do, but the exact number depends on how recovery is measured. Long-term persistent incontinence affects a minority of men — on the order of 5–6% in pooled studies. Your own odds are shaped by your surgical technique, your bladder function before surgery, and your age; the American Cancer Society notes older men tend to have more trouble than younger men. Recovery also isn’t always linear — good days and setback days are common, as covered in our guide to what recovery from prostate removal involves.
Pelvic floor exercises and daily habits that help recovery
The single most recommended first step is pelvic floor muscle training — strengthening the external sphincter and surrounding muscles that now carry your continence. These are also called Kegel exercises.
The first challenge is finding the right muscles. MedlinePlus describes the technique: imagine you’re urinating and then stop the flow — the muscles you squeeze are your pelvic floor. Use that only once to locate them, then exercise with an empty bladder rather than repeatedly stopping your stream. A simple routine is to tighten those muscles, hold 3–5 seconds, relax 3–5 seconds, and repeat — building up to about 10–15 repetitions, a few times a day, keeping your stomach, thighs, and buttocks relaxed.
⚠️ Clinical Warning: Do not do Kegel exercises while a catheter is in place. Memorial Sloan Kettering Cancer Center warns this can be painful and trigger bladder spasms — start once your catheter has been removed, unless your care team tells you otherwise.
Habits that support a drier recovery
Exercises work best alongside a few daily adjustments:
- Bladder training — urinating on a planned schedule rather than waiting for urgency, to retrain capacity.
- Fluid and diet management — limiting bladder irritants such as caffeine, alcohol, and carbonated drinks, and easing off fluids in the evening (estimate a sensible target with our daily water intake tool).
- Absorbent pads designed for men, which manage leakage and protect confidence while you recover.
- Pelvic floor physical therapy with biofeedback, which a therapist can use to confirm you’re engaging the correct muscles.
It’s worth being honest that the evidence for pelvic floor training is supportive but mixed across studies — it helps many men recover faster, but isn’t a guaranteed cure, which is exactly why it’s paired with the habits above and escalated when needed.
Some men find products like pelvic floor trainers or biofeedback devices helpful. These are general product suggestions, not a medical recommendation — ask your therapist or urologist whether a device fits your situation before buying one.
Treatments for incontinence that doesn’t improve
When leakage persists despite months of conservative effort, effective treatments exist — chosen in a stepwise way, generally after about 12 months when continence hasn’t returned on its own.
Medication plays a limited, specific role. For the urge or overactive-bladder component, certain bladder-calming medications can help that pattern. One medication (duloxetine) has been studied to speed recovery of post-surgical leakage, but it carries meaningful gastrointestinal and nervous-system side effects, is not FDA-approved for this use in the United States, and doesn’t reliably cure male stress incontinence — so any medication decision belongs with your clinician, not a general guide.
🩺 Physician Note: Guidelines emphasize trying conservative measures first and reserving surgery for leakage that persists and bothers you. The American Cancer Society’s guide to managing bladder incontinence outlines both the surgical and non-surgical options in plain language.
Surgery: male sling vs. artificial urinary sphincter
Two surgical options dominate when persistent stress leakage needs more than exercises:
| Option | How it works | Key clinical detail | Best for patient profile |
|---|---|---|---|
| Male sling | A strip of material supports and gently compresses the urethra | Minimally invasive; avoids a mechanical device | Mild-to-moderate leakage |
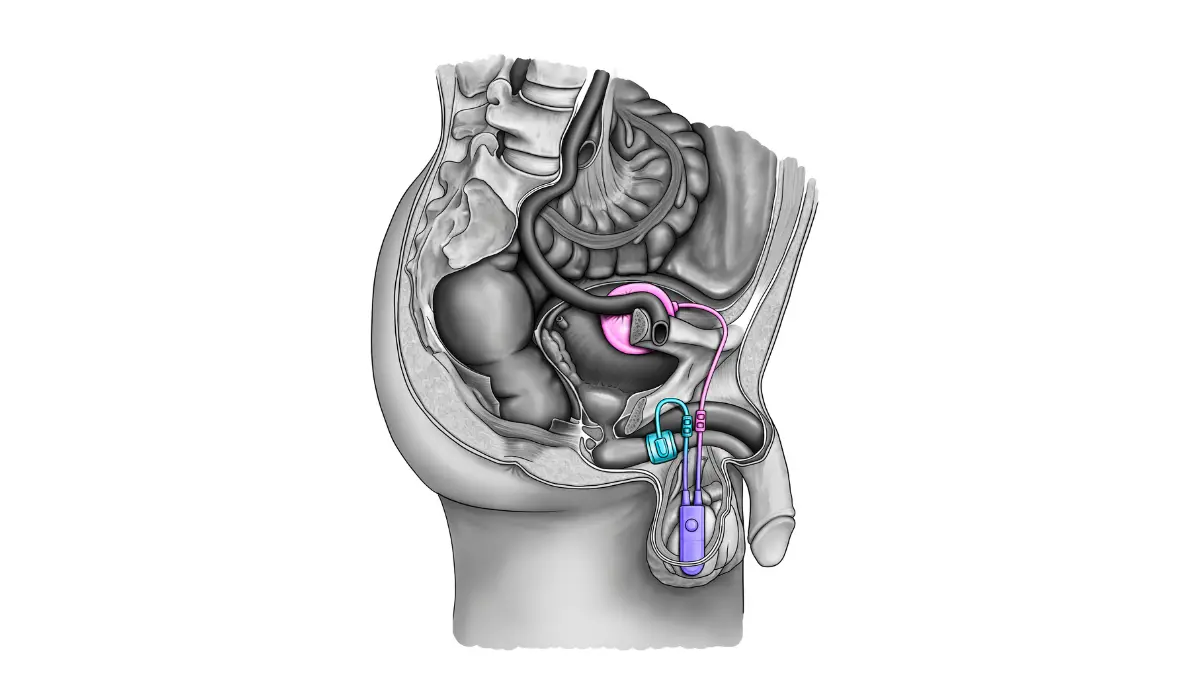
| Artificial urinary sphincter (AUS) | An implanted cuff encircles the urethra; a scrotal pump opens it to urinate | Gold-standard option; typically activated ~4–6 weeks after implant once swelling settles | Moderate-to-severe leakage |
Source: American Cancer Society; peer-reviewed urology literature.
📊 Clinical Data Point: The artificial urinary sphincter has long been regarded as the gold standard for moderate-to-severe male stress incontinence, with one meta-analysis reporting a success rate around 79% — Source: peer-reviewed meta-analysis (PLOS One, 2023). A systematic review comparing the male sling and AUS found both effective, with the choice guided by leakage severity and patient preference.
Incontinence and erectile dysfunction after prostate surgery are the two side effects men ask about most, and both have real treatment paths.
✅ Patient Action: If leakage is still affecting your life after about a year, ask for a referral to a urologist who specializes in male incontinence, and ask: “Am I a candidate for a sling or an artificial urinary sphincter, and what are the trade-offs for me?”
When urinary symptoms need medical attention
Most leakage during recovery is normal and improving. A few symptoms, though, mean you should contact your care team rather than wait.
Call your surgical or urology team promptly for signs of a urinary tract infection — Memorial Sloan Kettering Cancer Center lists a fever of 101°F (38.3°C) or higher, new pain at the surgical site, or blood in your urine as reasons to reach out. Burning with urination, or cloudy or foul-smelling urine, also warrants a call. Separately, leakage that is getting worse rather than better, or that hasn’t improved by around 12 months, should be evaluated by a urologist — not because something has gone wrong, but because that’s when the treatment options above become worth discussing.
⚠️ Clinical Warning: If you suddenly cannot urinate at all after your catheter is removed, this can signal urinary retention and needs prompt medical attention — don’t wait it out. Heavy or persistent bleeding, or signs of a blood clot, also warrant urgent evaluation.
Frequently asked questions about incontinence after prostatectomy
1. How long does urinary incontinence last after prostatectomy?
Most men leak when the catheter comes out, around 1–2 weeks after surgery, then improve over the following weeks to months. For the majority, urinary incontinence after prostatectomy almost fully resolves by about 12 months, while a minority have longer-term leakage. If yours hasn’t improved by a year, see a urologist.
2. Is incontinence permanent after prostate removal?
For most men it’s temporary, improving steadily over the first year. Pooled studies suggest only about 5–6% of men have long-term persistent leakage after prostatectomy, and even then, effective treatments exist. Talk with your urologist about your specific timeline and options if it isn’t improving as expected.
3. What percentage of men have incontinence after prostatectomy?
Nearly all men leak at first, then improve. In experienced-surgeon series, roughly 10–15% report frequent leakage at 6 months, dropping to fewer than 10% needing pads by 3 years (Johns Hopkins Medicine). Reported numbers vary because “continence” is defined differently across studies, so treat them as ranges.
4. When can I start Kegels after prostate surgery?
Start Kegel exercises once your catheter has been removed — not while it’s in place, since that can cause pain and bladder spasms. Many programs also have you practice before surgery to build familiarity. Confirm timing with your care team, and consider a pelvic floor therapist to check your technique.
5. What helps stop urine leakage after prostate surgery?
Pelvic floor (Kegel) exercises are the recommended first step, supported by bladder training, limiting caffeine and alcohol, and absorbent pads. Pelvic floor physical therapy with biofeedback helps confirm you’re using the right muscles. If leakage persists despite these measures, ask your urologist about medication or surgical options.
6. What is the difference between stress and urge incontinence?
Stress incontinence is leakage with effort — coughing, sneezing, lifting — and is the most common type after surgery. Urge incontinence is a sudden, hard-to-control need to urinate, often from bladder spasms, and may respond to specific medications. Some men have both. Your urologist can confirm which pattern you have.
7. Can incontinence after prostatectomy be cured?
Most men regain control within a year through exercises and time. For persistent leakage, treatments can substantially improve or resolve it — the artificial urinary sphincter, the gold-standard surgical option, reports success around 79% in one meta-analysis. Outcomes vary by severity and approach, so discuss expectations with a urologist.
8. What is an artificial urinary sphincter?
It’s a small implanted device with a cuff that encircles the urethra to keep it closed; when you need to urinate, you squeeze a pump placed in the scrotum to open it briefly. It’s typically activated about 4–6 weeks after surgery, once swelling settles. A urologist determines whether it’s appropriate for you.
9. Is leaking urine normal right after the catheter comes out?
Yes. Leakage when the catheter is removed, usually 1–2 weeks after surgery, is expected, because the muscles and nerves that control urine are still recovering. It typically improves over the following weeks and months. Having pads on hand helps; persistent or worsening leakage should be discussed with your care team.
10. Does nerve-sparing surgery reduce incontinence risk?
It’s associated with better continence recovery, though not a guarantee. Johns Hopkins Medicine notes the increase in urinary symptoms some men experience appears reduced with a nerve-sparing approach. Whether it’s possible depends on your cancer’s location and extent. Ask your surgeon whether nerve-sparing is appropriate in your case.
11. When should I see a doctor about leakage after prostatectomy?
Contact your team promptly for infection signs (fever of 101°F or higher, burning, blood in urine) or new surgical-site pain, and seek urgent care if you suddenly can’t urinate at all. Also see a urologist if leakage worsens or hasn’t improved by about 12 months, when treatment options become worth discussing.
The bottom line on your recovery
Leakage after prostate surgery is, for most men, a temporary stage with a clear arc: heaviest right after the catheter comes out, steadily better over the following months, and largely resolved for the majority by around a year. The reasons it happens are understood, the exercises that help are simple, and real treatments exist for the minority whose leakage lingers.
Your job right now is straightforward — start pelvic floor work once the catheter is out, manage fluids and irritants, keep pads handy, and bring specific questions to your urology follow-up. If leakage is still affecting your life after about a year, that’s your cue to ask about a sling or an artificial urinary sphincter rather than assume nothing more can be done.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.