On This Page – Quick Medical Summary
What Is Basal Cell Cancer?
The Truth About America’s Most Common Cancer
Michael Chen, a 38-year-old software engineer from San Diego, noticed a small pearly bump on his nose in early 2025. Like many Americans, he ignored it for six months, assuming it was just a pimple. When the bump began bleeding after shaving, his dermatologist diagnosed basal cell cancer—the same diagnosis 4.3 million Americans receive annually.
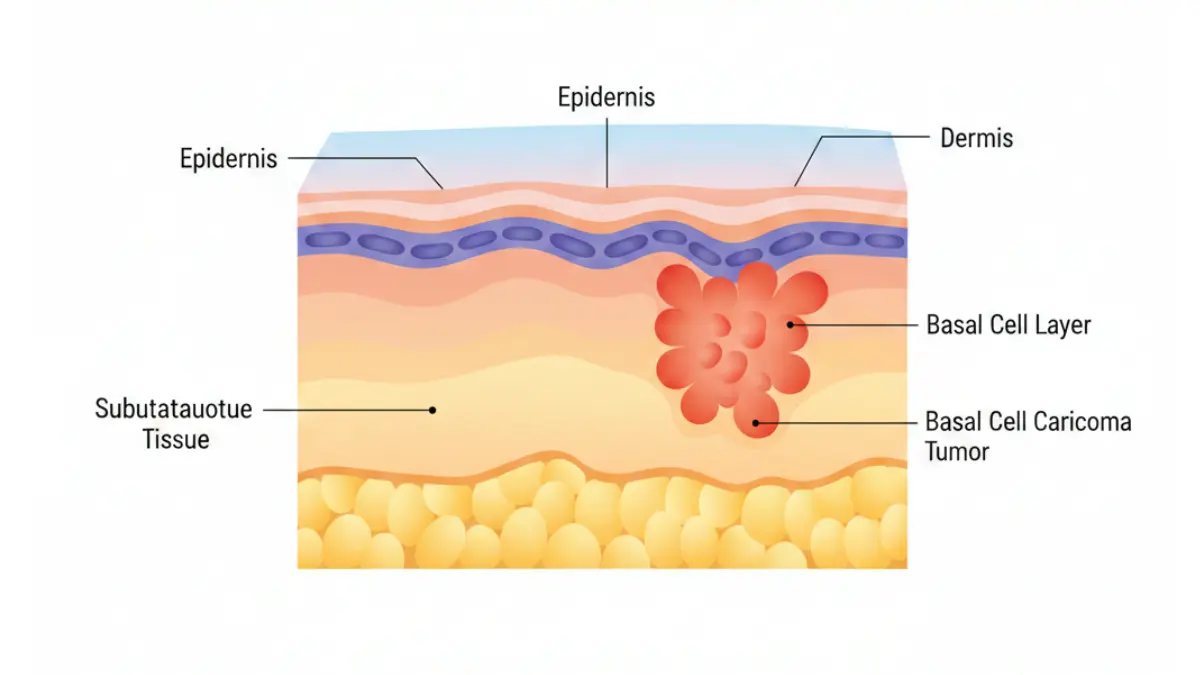
Here’s what you need to know immediately: Basal cell cancer has a 98% cure rate when detected and treated early. This skin cancer originates in the basal cells of your epidermis (outer skin layer) and grows slowly, rarely spreading beyond the original site. Unlike aggressive melanoma, basal cell cancer is highly treatable, with most patients achieving complete recovery through simple outpatient procedures.
The 2026 statistics reveal encouraging trends. According to the National Cancer Institute, over 5.4 million cases of non-melanoma skin cancers are diagnosed yearly in the United States, with basal cell cancer representing approximately 80% of these cases. What makes this diagnosis less frightening than other cancers is the exceptional survival rate—99.9% of patients survive five years or longer after treatment.
Why 98% of Patients Survive Basal Cell Cancer
The high cure rate stems from three critical factors. First, basal cell cancer grows extremely slowly, often taking years to reach just one centimeter in diameter. This gradual progression gives patients and doctors ample time for detection and intervention. Second, advanced treatment options like Mohs micrographic surgery offer cure rates approaching 99% for primary tumors. Third, the cancer’s biological behavior differs dramatically from aggressive malignancies—metastasis (spreading to distant organs) occurs in less than 0.1% of cases.
Key takeaway: If you’re reading this after a basal cell cancer diagnosis, understand that you have one of the most curable forms of cancer known to medicine. Early treatment leads to minimal scarring and excellent long-term outcomes.
2026 Update: New FDA-Approved Treatments
The treatment landscape evolved significantly in 2025-2026. The FDA expanded approval for Hedgehog pathway inhibitors, including sonidegib and vismodegib, for patients with advanced or metastatic basal cell cancer. These targeted therapies work by blocking the molecular signals that fuel cancer cell growth, offering hope for the small percentage of patients whose tumors cannot be surgically removed.
Additionally, immunotherapy trials using checkpoint inhibitors show promising results, with some advanced-stage patients achieving complete remission. If you’re concerned about your overall cancer risk profile, consider using a genetic risk assessment tool to understand your hereditary predisposition to various cancers, including skin malignancies.
What This Means For You: Modern medicine offers multiple pathways to cure basal cell cancer. Your treatment plan will depend on tumor size, location, and subtype—but cure is the expected outcome in nearly all cases.
How to Identify Basal Cell Cancer: 5-Second Self-Check
6 Visual Signs You Shouldn’t Ignore
Basal cell cancer appears differently than most people expect. Forget the textbook images of large, obvious tumors—early basal cell cancer often masquerades as harmless skin changes.
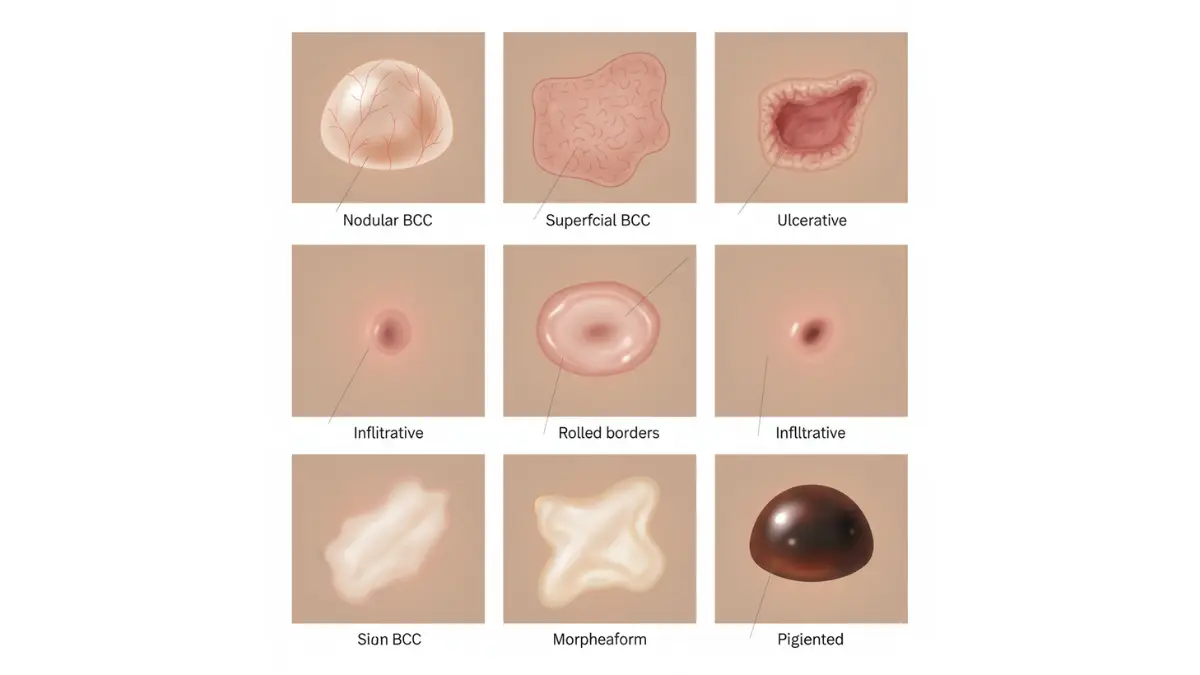
Watch for these warning signs:
- Pearly or waxy bumps: Small, translucent nodules with visible blood vessels (telangiectasias) running across the surface, typically flesh-colored, pink, or slightly red
- Flat, scaly patches: Brown, flesh-colored, or pink lesions that feel rough to touch and don’t heal within 4-6 weeks
- Sores that won’t heal: Open wounds that bleed, ooze clear fluid, crust over, then repeat this cycle for months
- Pink growths with rolled edges: Raised bumps with a central depression, resembling a tiny crater
- Scar-like areas: White, yellow, or waxy patches with poorly defined borders appearing without prior injury
- Shiny bumps: Dome-shaped growths that look like small pearls, especially on darker skin tones where they may appear brown or black
Jennifer Rodriguez, a 52-year-old nurse from Miami, discovered her basal cell cancer using the modified ABCDE method adapted for non-melanoma skin cancers. Unlike melanoma screening, which focuses on mole changes, basal cell detection requires attention to new growths and non-healing sores.
Basal Cell Cancer vs. Normal Skin Spots (Comparison Table)
| Feature | Basal Cell Cancer | Normal Age Spot | Acne Scar |
|---|---|---|---|
| Texture | Pearly, waxy, or scaly | Flat, smooth | Flat or depressed |
| Color | Pink, flesh-colored, brown, or black | Tan or brown | Pink fading to white |
| Borders | Rolled, raised edges | Uniform, flat | Irregular but stable |
| Changes | Bleeds, crusts, won’t heal | Stable over time | Gradually fades |
| Blood vessels | Visible tiny vessels | None visible | None visible |
| Growth rate | Slowly enlarges over months | No growth | No growth |
Early Stage vs. Advanced: What’s the Difference?
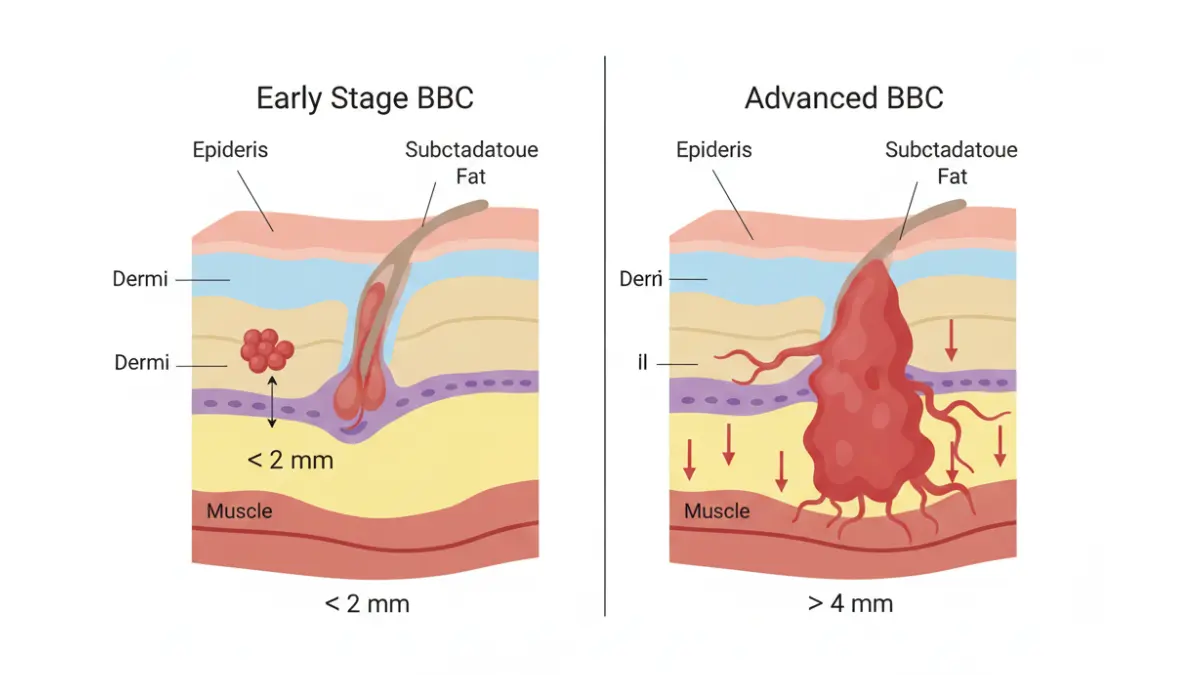
Early-stage basal cell cancer (Stage 0-1) appears as small lesions under 2 centimeters with no invasion into deeper tissues. These account for approximately 85% of diagnoses and respond excellently to minimally invasive treatments with cure rates exceeding 99%.
Advanced-stage disease (Stage 2-4) involves tumors larger than 2 centimeters or those invading into cartilage, muscle, or bone. According to Harvard Medical School research, advanced cases represent fewer than 5% of diagnoses but require more aggressive intervention, including radiation therapy or systemic medications.
The progression timeline varies dramatically. Some basal cell cancers remain stable for 5-10 years, while aggressive subtypes (morpheaform, infiltrative) can double in size within 12-18 months. This unpredictability underscores why immediate dermatologic evaluation matters.
When to See a Dermatologist (Urgency Framework)
Seek same-day or next-day evaluation if you notice:
- Sudden rapid growth of any skin lesion (doubling in size within weeks)
- Profuse bleeding that doesn’t stop with pressure
- Severe pain or tenderness in a previously painless bump
- Signs of infection (spreading redness, warmth, pus, fever)
Schedule an appointment within 1-2 weeks for:
- New pearly or translucent bumps, especially on sun-exposed areas
- Sores that don’t heal after 6 weeks
- Spots that bleed with minimal trauma (shaving, washing)
- Changing moles or growths with irregular borders
Routine annual skin checks for:
- Fair-skinned individuals over age 40
- Anyone with family history of skin cancer
- Previous basal cell cancer survivors (40% develop new primary lesions)
- Outdoor workers or those with extensive sun exposure history
Use a symptom checker if you’re uncertain whether your skin changes warrant professional evaluation, but remember—when in doubt, get it checked out. The five-minute dermatology appointment could save you from months of complex treatment later.
What Causes Basal Cell Cancer? (2026 Research Update)
Top 7 Risk Factors for Basal Cell Cancer
Understanding causation helps with both prevention and risk assessment. The primary driver remains ultraviolet radiation exposure, but genetic and lifestyle factors play supporting roles.
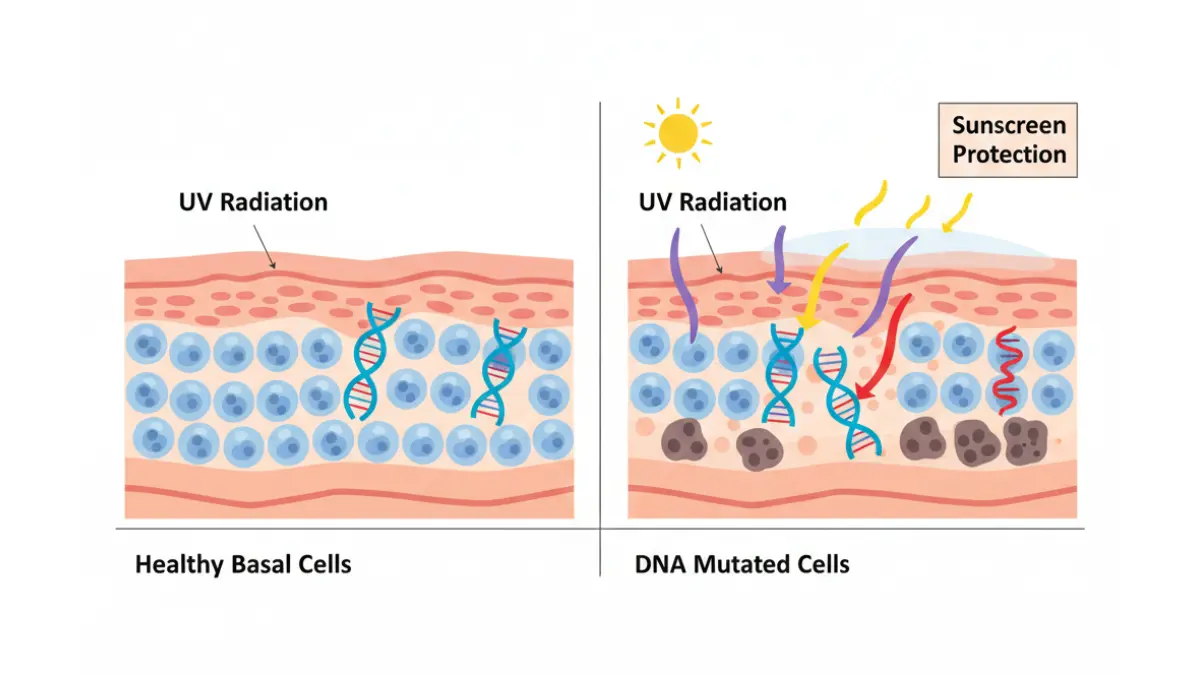
1. Chronic UV Radiation (80% of Cases)
Cumulative sun exposure over decades damages the DNA in basal cells, triggering malignant transformation. The Centers for Disease Control and Prevention confirms that just five severe sunburns in youth double your lifetime risk. Unlike melanoma, which correlates with intermittent intense exposure, basal cell cancer links to chronic daily UV exposure—think outdoor workers, golfers, and gardeners.
2. Age-Related Risk Escalation
Your risk multiplies with each passing decade. Data shows:
- Under 30: Extremely rare (less than 2% of cases)
- Ages 40-50: Risk begins climbing, especially in sun-damaged individuals
- Ages 60+: Peak incidence, with 1 in 5 Americans developing basal cell cancer by age 70
- Ages 80+: Highest risk group, though aggressive treatment remains highly effective
3. Skin Type and Ethnicity
Fair-skinned individuals of Northern European descent face 10-20 times higher risk than those with darker complexions. The Fitzpatrick skin type classification reveals that Types I-II (always burns, never or rarely tans) carry maximum vulnerability. However, basal cell cancer does occur in all ethnic groups, and darker-skinned patients often experience delayed diagnosis due to atypical presentations.
4. Genetic Mutations (New 2026 Research)
Groundbreaking studies published in Nature Genetics identified specific gene variants that triple basal cell cancer susceptibility. Mutations in the PTCH1 gene (part of the Hedgehog signaling pathway) and TP53 tumor suppressor gene significantly elevate risk. Consider using a genetic risk assessment tool if multiple family members have skin cancer diagnoses.
5. Family History
Having a first-degree relative (parent, sibling) with basal cell cancer increases your risk 2.5-fold. This genetic component operates independently of shared environmental exposures, suggesting inherited DNA repair deficiencies.
6. Immunosuppression
Organ transplant recipients taking anti-rejection medications face 10-16 times higher basal cell cancer rates. Similarly, patients with chronic lymphocytic leukemia or HIV/AIDS show elevated incidence. The National Institutes of Health documents that immunosuppressive drugs impair the body’s ability to eliminate precancerous cells.
7. Previous Radiation Exposure
Childhood radiation therapy for acne, ringworm, or cancer increases basal cell cancer risk decades later. Even diagnostic X-rays performed repeatedly on the same body area may contribute to cumulative DNA damage.
Genetic Testing: Should You Get Screened? (NEW 2026)
Commercial genetic testing panels now include basal cell cancer risk variants. The American Academy of Dermatology recommends testing for:
- Individuals with 3+ basal cell cancers before age 40
- Those with family history of basal cell nevus syndrome (Gorlin syndrome)
- Multiple family members across generations with skin cancers
Testing costs range from $250-$600 and is sometimes covered by insurance with appropriate documentation. Results guide prevention strategies and surveillance frequency.
Sun Protection 2.0: Beyond Sunscreen
Traditional advice—”apply SPF 30 and reapply every two hours”—remains valid but insufficient. The 2026 dermatology consensus recommends a multi-layered approach:
Comprehensive UV Protection:
- Broad-spectrum sunscreen: SPF 50+ with zinc oxide or titanium dioxide applied 30 minutes before sun exposure
- Physical barriers: Wide-brimmed hats (3+ inch brim), UV-blocking sunglasses, long-sleeved UPF 50+ clothing
- Timing strategies: Avoid outdoor activities between 10 AM – 4 PM when UV index peaks
- Shade-seeking behavior: Position yourself under structures whenever possible during peak hours
- Window film: Install UV-blocking film on car and home windows (up to 99% UV reduction)
- Chemical avoidance: Skip tanning beds permanently—they contribute to 400,000+ skin cancer cases annually
AI-Assisted Early Detection Apps (2026 Review)
Smartphone applications using artificial intelligence can now identify suspicious lesions with 85-90% accuracy. Top-rated options include:
SkinVision (FDA-registered, $30/year): Analyzes photos using machine learning algorithms, provides risk assessment, and tracks changes over time. Clinical validation studies show 95% sensitivity for melanoma, 87% for basal cell cancer.
MoleScope ($99 device + app): Attachable dermatoscope connects to smartphones, offering 10x magnification with dermoscopic imaging capabilities previously available only in clinics.
DermAI (Free basic version): Uses neural networks trained on 100,000+ dermatologist-verified images to flag high-risk lesions requiring professional evaluation.
Important caveat: These tools supplement but never replace professional dermatologic examination. Use them for monthly self-monitoring between annual doctor visits, similar to how you might use a BMI calculator to track general health metrics between physical exams.
Basal Cell Cancer Treatment: 2026 Complete Guide
98% Cure Rate Breakdown by Treatment Type
Treatment selection depends on tumor size, location, subtype, and patient factors. Here’s what the evidence shows for first-time (primary) basal cell cancers:
| Treatment Method | 5-Year Cure Rate | Best Candidates | Typical Cost (2026) |
|---|---|---|---|
| Mohs Micrographic Surgery | 99% | Facial tumors, recurrent cases, aggressive subtypes | $2,000-$5,000 |
| Standard Excision | 95% | Low-risk tumors on trunk, arms, legs | $800-$2,500 |
| Electrodesiccation & Curettage | 92% | Small, superficial tumors on low-risk areas | $600-$1,500 |
| Radiation Therapy | 90% | Elderly patients, surgical contraindications | $4,000-$12,000 |
| Topical Medications | 85% | Superficial BCC only, multiple lesions | $400-$1,200 |
| Cryotherapy | 85% | Very small, superficial lesions | $300-$800 |
| Photodynamic Therapy | 87% | Multiple superficial BCCs | $1,000-$3,000 |
These statistics come from American Academy of Dermatology clinical practice guidelines updated in January 2026.
Mohs Surgery vs. Standard Excision: Which Is Right for You?
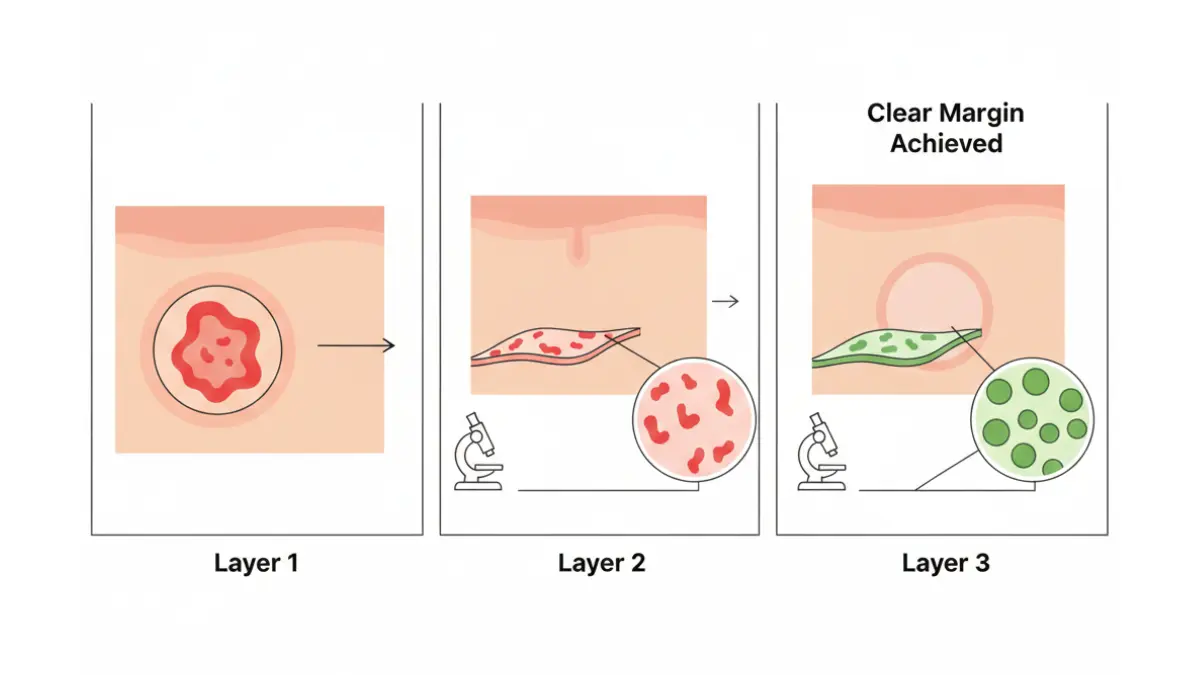
Mohs micrographic surgery offers the highest cure rate by examining 100% of the tumor margin microscopically during the procedure. The surgeon removes tissue layer by layer, checking each for cancer cells in real-time, stopping only when margins are clear. This tissue-sparing approach minimizes scarring while maximizing cure rates.
Choose Mohs for:
- Tumors on cosmetically sensitive areas (face, ears, eyelids, nose, lips)
- Recurrent basal cell cancers (previously treated tumors returning)
- Aggressive histologic subtypes (morpheaform, infiltrative, micronodular)
- Tumors larger than 2 centimeters
- Poorly defined borders on clinical examination
David Park, a 61-year-old accountant from Boston, underwent Mohs surgery for a 1.5-centimeter basal cell cancer on his left cheek. The procedure took three hours, required two tissue layers removed, and resulted in a barely visible scar after six months of healing. His insurance covered 80% of the $4,200 cost.
Standard surgical excision removes the visible tumor plus a safety margin of normal-appearing tissue (typically 4-6 millimeters). Pathologists examine the entire specimen after removal to confirm clear margins.
Choose standard excision for:
- Low-risk tumors on the trunk, shoulders, arms, or legs
- Nodular subtype basal cell cancers smaller than 1 centimeter
- Well-defined lesion borders
- Lower-cost preference when Mohs not medically necessary
Treatment Costs in 2026 (Full Transparency)
Real-world costs vary dramatically based on geography, insurance status, and facility type. Here’s what Americans actually paid in 2025-2026:
With Commercial Insurance:
- Typical copay: $100-$500 for outpatient surgery
- Out-of-pocket maximum contribution: $1,000-$3,000 annually
- Pathology fees: Usually covered after deductible met
With Medicare:
- Part B covers 80% of Medicare-approved amounts
- Patient responsibility: 20% coinsurance plus Part B deductible ($240 in 2026)
- Mohs surgery average Medicare payment: $1,800-$2,400
- Patient pays approximately: $360-$480
Without Insurance:
- Cash-pay discounts: 20-40% off billed charges if paid upfront
- Payment plans: Most dermatology practices offer 12-24 month interest-free financing
- Charity care: Hospital-based facilities may provide financial assistance for low-income patients
CPT billing codes for insurance claims:
- 17311-17315: Mohs surgery (per stage)
- 11640-11646: Excision of malignant lesions (by size)
- 96567: Photodynamic therapy
- 17004: Cryotherapy
For context on managing healthcare finances, understanding your overall health profile through tools like a calorie deficit calculator can help optimize your wellness and potentially reduce long-term medical costs through prevention.
Celebrity Cases: What Kevin Jonas & John Cena Did
Kevin Jonas, member of the Jonas Brothers, publicly shared his May 2023 basal cell cancer diagnosis and subsequent Mohs surgery on Instagram. He documented the process to raise awareness, showing the small forehead lesion and post-surgical healing. His dermatologist detected the cancer during a routine full-body skin exam—a practice Kevin now advocates for all adults.
WWE superstar John Cena revealed in January 2024 that he’d been diagnosed and treated for basal cell cancer twice before age 45. Both instances occurred on his face after decades of outdoor training and filming without adequate sun protection. Cena’s public disclosure emphasized that even athletes at peak physical condition face skin cancer risk without proper UV protection habits.
These celebrity cases highlight a critical point: basal cell cancer affects successful, health-conscious individuals who simply didn’t prioritize skin protection earlier in life. Their stories normalize seeking dermatologic care and demonstrate excellent outcomes with prompt treatment.
Recovery Timeline: What to Expect Week-by-Week
Week 1 Post-Surgery:
- Swelling and bruising peak days 2-3, especially for facial procedures
- Pain typically mild (managed with acetaminophen or ibuprofen)
- Stitches remain in place (7-14 days depending on location)
- Wound care: Gentle cleaning with soap and water, antibiotic ointment, bandage changes
Weeks 2-3:
- Sutures removed (face: 5-7 days, body: 10-14 days)
- Redness persists but begins fading
- Return to normal activities (avoid heavy lifting or straining for facial surgeries)
- Scar begins forming—appears pink, slightly raised initially
Weeks 4-8:
- Scar remodeling phase begins
- Color gradually fades from pink to lighter shades
- Massage techniques and silicone gel sheets can improve cosmetic outcome
- Sun protection absolutely critical (SPF 50+ on healing wound prevents hyperpigmentation)
Months 3-12:
- Continued scar maturation and flattening
- Final cosmetic result typically visible by 12 months
- Some patients opt for laser resurfacing or dermabrasion if unsatisfied with appearance
Scar Prevention & Minimization Strategies
Emerging evidence supports several interventions that improve surgical scar outcomes:
Evidence-based approaches:
- Silicone gel sheets: Applied 12+ hours daily for 3-6 months, reduce scar thickness by 30-50%
- Massage therapy: Gentle pressure and circular motions 2-3 times daily starting week 2
- Vitamin E topical: Mixed evidence, may help in some individuals but can cause allergic contact dermatitis
- Sunscreen rigidity: SPF 50+ broad-spectrum on scar for minimum 12 months prevents permanent darkening
- Laser treatment: Pulsed dye laser or fractional CO2 laser at 3-6 months post-surgery for persistent redness or texture irregularities
- Steroid injections: For hypertrophic (raised, thick) scars developing despite preventive measures
The National Library of Medicine published comprehensive scar management guidelines showing that early intervention (starting within 2 weeks post-surgery) yields superior cosmetic results compared to waiting until scars fully mature.
Basal Cell Cancer Prognosis: Long-Term Outlook
Survival Rates: What the Numbers Really Mean
The prognosis for basal cell cancer stands unmatched among malignancies. Updated 2026 data from cancer registries confirms:
5-year relative survival rate: 99.9%
This means that 999 out of 1,000 people diagnosed with basal cell cancer survive at least five years. The 0.1% who don’t typically have either extremely advanced disease at diagnosis or die from unrelated causes rather than the cancer itself.
10-year survival rate: 98.7%
Even a decade out, outcomes remain exceptional. The small percentage who experience disease-related deaths almost exclusively fall into the advanced/metastatic category—representing fewer than 1,000 cases annually in the United States.
Death rate from basal cell cancer: 0.12 per 100,000 population
To contextualize, you’re statistically more likely to die from a bee sting, lightning strike, or choking on food than from basal cell cancer. This isn’t medical dismissiveness—it’s statistical reality that should provide reassurance while still motivating prompt treatment.
Recurrence Risk: How to Prevent Second Cancers
Here’s the reality that surprises many patients: 40-50% of people with basal cell cancer develop a new primary tumor within 5 years. This doesn’t mean the original cancer returned—it means sun-damaged skin generated a completely separate malignancy elsewhere.
Recurrence patterns:
- Same-site recurrence: 5-10% within 5 years (higher for incomplete excisions or aggressive subtypes)
- New primary tumors: 40-50% develop at least one additional basal cell cancer
- Multiple primaries: 20% develop 3 or more separate basal cell cancers over their lifetime
Research from Stanford Medicine explains this phenomenon: the same UV exposure that caused the first cancer damaged surrounding skin cells. Think of your sun-exposed skin as a field of potential cancer cells, not just isolated problem spots.
Elizabeth Tran, a 68-year-old retiree from Phoenix, had five separate basal cell cancers removed over 12 years. Each was caught early through vigilant six-month dermatology appointments. She now uses smartphone app reminders and has her dermatologist photograph her entire body at each visit for comparison—a practice that’s identified two lesions at the pre-cancerous stage (actinic keratosis) before they progressed.
Life After Treatment: Monitoring & Follow-Up
Dermatologist surveillance schedule:
Year 1-2 post-treatment:
- Every 3-6 months for high-risk patients (recurrent tumors, immunosuppressed, multiple primaries)
- Every 6-12 months for average-risk patients
Year 3-5 post-treatment:
- Every 6-12 months regardless of risk category
Year 6+ onwards:
- Annual examinations minimum, more frequently if new lesions develop
Home monitoring protocol:
- Monthly full-body self-exams using the ABCDE method
- Partner-assisted checks for hard-to-see areas (scalp, back, buttocks)
- Photo documentation of concerning spots (smartphone apps like SkinVision)
- Immediate appointment scheduling for new/changing lesions
Many survivors report that connecting general wellness habits—like tracking nutrition through a macro calculator or maintaining fitness routines—helps them stay engaged with their overall health monitoring, including skin surveillance.
Insurance Coverage & CPT Codes (2026 Guide)
Understanding billing codes helps navigate insurance approvals and out-of-pocket costs. Basal cell cancer treatment falls under diagnostic and therapeutic CPT (Current Procedural Terminology) codes recognized by Medicare, Medicaid, and commercial insurers.
Key CPT codes:
- 17311-17315: Mohs micrographic surgery (billed per stage, most require 1-3 stages)
- 11640-11646: Excision of malignant lesions, face/ears/eyelids/nose/lips (by size increments)
- 11620-11626: Excision of malignant lesions, scalp/neck/hands/feet/genitals
- 11600-11606: Excision of malignant lesions, trunk/arms/legs
- 96567: Photodynamic therapy
- 17000-17004: Cryosurgery codes
Prior authorization requirements:
Most commercial insurers require pre-approval for:
- Mohs surgery (submit photos, pathology reports, medical necessity documentation)
- Radiation therapy
- Systemic medications (vismodegib, sonidegib)
Medicare Part B covers Mohs surgery without prior authorization when performed by qualified physicians. Submit claims with diagnosis code C44._ (malignant neoplasm of skin) specifying anatomic site.
Appeal denied claims by:
- Obtaining letter of medical necessity from dermatologist
- Providing photographs showing tumor location
- Citing American Academy of Dermatology appropriate use criteria
- Including pathology reports confirming aggressive histologic subtype
Key Takeaways & FAQs
5-Point Action Plan If You Suspect Basal Cell Cancer
Step 1: Document the lesion Take clear, well-lit photos from multiple angles. Include a ruler or coin for size reference. Note when you first observed it and any changes since.
Step 2: Schedule dermatology appointment within 1-2 weeks Don’t delay months “to see if it goes away.” Basal cell cancer doesn’t spontaneously resolve. Early detection enables simpler treatment with better cosmetic outcomes.
Step 3: Prepare for your appointment List all medications, previous skin cancer history, radiation exposure, and family history. Bring photos of the concerning lesion showing progression over time if available.
Step 4: Ask about biopsy at first visit Most dermatologists perform same-day biopsy if basal cell cancer is suspected. Results typically return within 5-10 business days.
Step 5: Begin sun protection immediately Start rigorous UV avoidance and SPF 50+ application even before diagnosis confirmation. This prevents additional DNA damage to already vulnerable skin.
What This Means For You
If you’ve just been diagnosed with basal cell cancer, remember these facts:
- You have one of the most curable cancers in medicine (98% cure rate)
- Treatment is typically a single outpatient procedure taking 30-90 minutes
- You’ll likely return to normal activities within 1-2 weeks
- Long-term survival is virtually guaranteed with appropriate treatment
- The diagnosis should prompt lifelong skin protection, not lifelong fear
For ongoing health monitoring beyond skin checks, tools like our symptom checker can help you track various health concerns and determine when professional evaluation is warranted.
11 Most-Asked Questions About Basal Cell Cancer (2026)
1. Can basal cell cancer kill you?
While technically capable of causing death, basal cell cancer fatalities are extraordinarily rare. Deaths occur in approximately 0.12 per 100,000 people—fewer than 2,000 annually in the United States. These cases almost exclusively involve patients who ignored extensive tumors for years or decades, allowing invasion into vital structures like the brain or major blood vessels. With timely treatment, lethality is essentially zero.
2. Is basal cell cancer dangerous if untreated?
Yes, untreated basal cell cancer continues growing, potentially invading into cartilage, bone, muscle, and nerves. Advanced untreated cases can cause disfigurement, vision loss (if near eyes), hearing impairment (if in ear canal), and chronic non-healing wounds. However, “untreated” typically means years of neglect—even patients who delay 6-12 months usually still achieve excellent outcomes.
3. How fast does basal cell cancer grow?
Growth rates vary dramatically by subtype. Nodular basal cell cancer (most common) grows slowly, often taking 2-5 years to double in size. Aggressive subtypes like morpheaform or infiltrative can grow faster, potentially doubling within 12-18 months. Location also matters—facial tumors sometimes appear to grow quicker due to closer self-monitoring, while trunk lesions may go unnoticed for years.
4. What is the best treatment for basal cell cancer?
“Best” depends on individual factors. Mohs micrographic surgery offers the highest cure rate (99%) and is considered gold standard for facial tumors, recurrent cancers, and aggressive subtypes. Standard excision works excellently for low-risk tumors on the body. Topical medications suit superficial BCC when surgery isn’t ideal. Discuss options with a board-certified dermatologist who will tailor recommendations to your specific tumor characteristics and preferences.
5. Does insurance cover basal cell cancer removal?
Yes, basal cell cancer treatment is medically necessary and covered by Medicare, Medicaid, and virtually all commercial insurance plans. Mohs surgery may require prior authorization with some insurers. Typical out-of-pocket costs with insurance range from $100-$1,000 depending on your deductible and coinsurance. Medicare Part B covers 80% of approved amounts after the annual deductible is met.
6. Can basal cell cancer come back after Mohs surgery?
Recurrence after Mohs surgery occurs in approximately 1% of primary (first-time) basal cell cancers and 3-5% of recurrent tumors. These rates are significantly lower than other treatment modalities. When recurrence happens, it typically appears within 3 years and can be successfully re-treated. Risk factors for recurrence include aggressive histologic subtype, large tumor size (>2cm), and incomplete removal despite Mohs technique.
7. What’s the difference between basal cell and melanoma?
These represent opposite ends of the skin cancer spectrum. Basal cell cancer grows slowly, rarely metastasizes (<0.1% of cases), and has a 98-99% cure rate. Melanoma arises from pigment cells, grows rapidly, metastasizes in 15-20% of cases if not caught early, and carries significantly higher mortality risk. Visually, melanomas are typically dark brown or black with irregular borders, while basal cell cancers are often pink, pearly, or flesh-colored.
8. Should I get genetic testing for basal cell cancer?
Genetic testing makes sense for specific situations: multiple basal cell cancers before age 40, family history of basal cell nevus syndrome (Gorlin syndrome), or 3+ first-degree relatives with skin cancer. The test identifies mutations in genes like PTCH1 and TP53 that increase risk. Results guide surveillance frequency and may qualify you for enhanced screening protocols. Cost runs $250-$600 and may be insurance-covered with medical necessity documentation. Access our genetic risk assessment tool for preliminary risk evaluation.
9. How much does basal cell cancer treatment cost in 2026?
Costs vary by treatment type and insurance status. With commercial insurance, expect $100-$500 copays for outpatient surgery. Medicare beneficiaries typically pay 20% coinsurance ($360-$960 for Mohs surgery). Uninsured cash-pay costs range from $800-$5,000 depending on procedure complexity. Many dermatology practices offer payment plans. Hospital-based charity care may cover low-income patients. Never delay treatment due to cost concerns—discuss financial options with your provider’s billing department.
10. Can you prevent basal cell cancer from spreading?
Basal cell cancer “spreading” happens in two ways. Local spread into surrounding tissue is prevented through complete surgical removal—this is why treatment matters. Metastatic spread (to lymph nodes or distant organs) is extraordinarily rare but can be prevented by treating even advanced local disease with surgery, radiation, or systemic therapy. The key is not delaying treatment—basal cell cancer won’t spread if removed when small, and even large tumors rarely metastasize if treated appropriately.
11. When should I get a second opinion for basal cell cancer?
Seek a second opinion if:
– Recommended treatment differs significantly from standard-of-care (Mohs for facial tumors, excision for low-risk body lesions)
– Tumor is in cosmetically or functionally critical location (eyelid, nose, ear) and you want surgical options compared
– You’re offered only radiation or topical therapy for a tumor that appears surgically accessible
– Dermatologist recommends “watch and wait” for a confirmed basal cell cancer
– You feel uncomfortable with the proposed treatment plan for any reason
Most dermatologists welcome second opinions and will provide records promptly. Major cancer centers like MD Anderson, Memorial Sloan Kettering, and Mayo Clinic offer expedited consultations for complex cases.
Final Thoughts
Basal cell cancer, while frightening to hear diagnosed, represents one of the most treatable malignancies in all of medicine. The 98% cure rate isn’t marketing—it’s statistical reality backed by decades of outcome data. Early detection through vigilant skin monitoring, prompt treatment with appropriate modalities, and lifelong sun protection form your comprehensive strategy for not just surviving, but thriving after this diagnosis.
Stay proactive with your skin health, attend regular dermatology appointments, and remember—this cancer is highly beatable. For ongoing health optimization strategies, explore our health tips section for evidence-based wellness guidance.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











