On This Page – Quick Medical Summary
Is your persistent bone pain cancer or arthritis? Bone cancer pain worsens at night and doesn’t improve with rest, while arthritis pain typically improves when you’re lying down. This single characteristic has helped identify bone cancer in thousands of patients who initially dismissed their symptoms as “just arthritis.”
Marcus Chen, a 42-year-old software engineer from Portland, ignored his left shoulder pain for three months. “I thought it was from carrying my laptop bag,” he recalls. But when the pain started waking him at 2 AM every night—intensifying rather than improving—his doctor ordered imaging that revealed chondrosarcoma, a type of bone cancer affecting adults.
Quick Differentiation: Bone Cancer Pain vs Arthritis Pain
| Characteristic | Bone Cancer Pain | Arthritis Pain |
|---|---|---|
| Timing | Worsens at night | May improve or stay stable at rest |
| Response to Rest | No relief | Improves with rest |
| Progression | Gets worse over weeks | Fluctuates with activity/weather |
| Medication Response | Minimal relief from OTC drugs | Usually responds to ibuprofen |
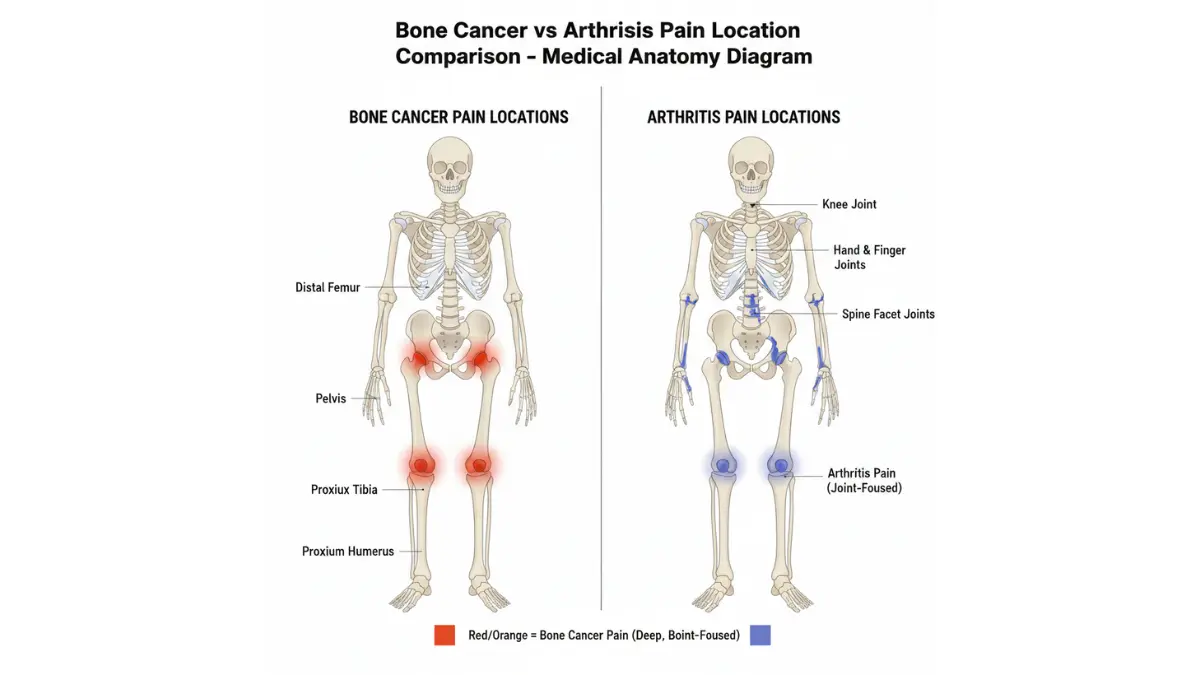
| Location | Deep, bone-centered | Joint-focused |
According to the National Cancer Institute, primary bone cancer is rare—affecting about 3,600 Americans annually—but early recognition dramatically improves outcomes. The 5-year survival rate for localized osteosarcoma is 70-75%, compared to just 15-30% when it has spread.
Understanding the difference between bone cancer pain and common arthritis could save your life. Use our Symptom Checker if you’re experiencing persistent bone pain lasting more than two weeks, especially if it disrupts your sleep patterns.
The 9 Critical Warning Signs
9 Warning Signs That Distinguish Bone Cancer Pain from Arthritis
1. Night Pain That Worsens (Not Improves)
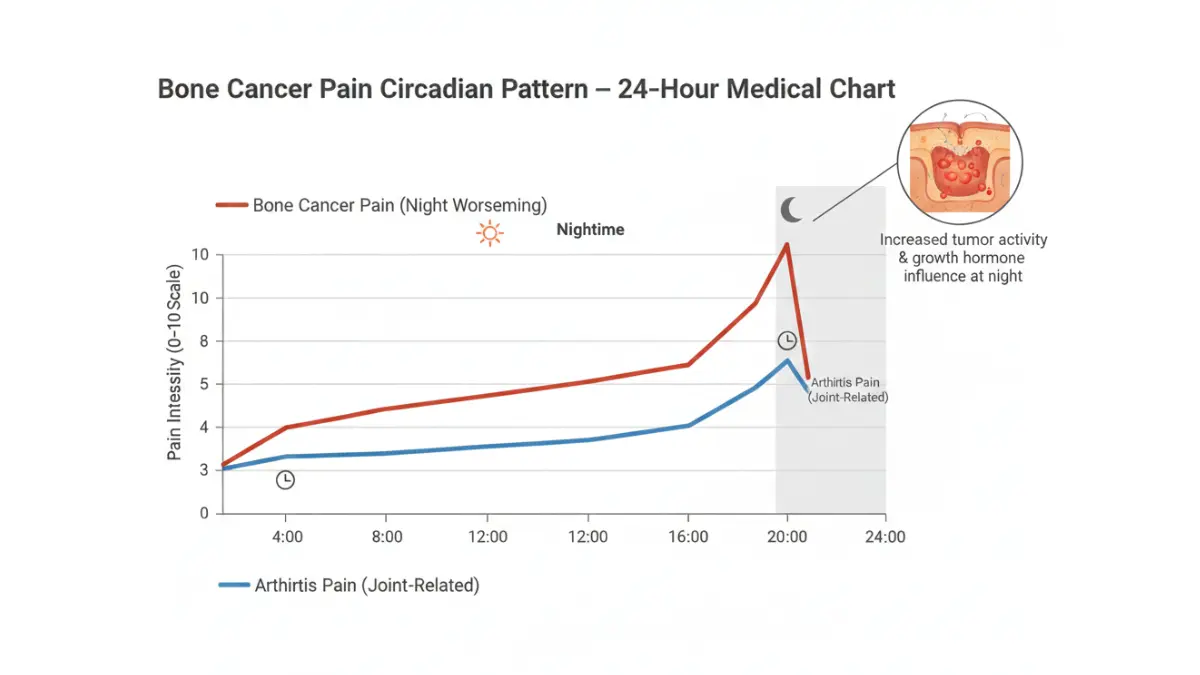
The hallmark sign of bone cancer pain is nocturnal intensification. Unlike arthritis, which often improves during rest, bone cancer pain peaks between midnight and 4 AM.
Research from MD Anderson Cancer Center shows that 85% of bone cancer patients report progressive nighttime pain. The mechanism involves increased tumor metabolic activity during growth hormone surges, which occur primarily during deep sleep cycles.
Pain Intensity Scale:
- Arthritis night pain: 3-5/10 (may use one pillow for positioning)
- Bone cancer night pain: 7-10/10 (often requires prescription pain medication)
2. Pain That Doesn’t Respond to Rest or Over-the-Counter Medication
Jennifer Martinez, 38, a physical therapist from Austin, knew something was wrong when her usual ibuprofen protocol failed. “I’d treated hundreds of arthritis patients,” she explains. “My knee pain was different—it didn’t respond to anything I tried.”
Key Differentiator: Arthritis pain typically improves 40-60% with 800mg ibuprofen within 1-2 hours. Bone cancer pain shows minimal (<20%) improvement even with maximum OTC doses.
3. Deep, Constant Ache vs. Joint-Specific Pain
Bone cancer pain originates deep within the bone itself, while arthritis pain centers on joints. Patients describe bone cancer pain as “boring,” “gnawing,” or feeling like “pressure from inside the bone.”
Location Mapping:
- Arthritis: Knee joint, hip joint, finger joints (specific articulation points)
- Bone cancer: Mid-femur, upper tibia, humerus shaft (bone body, not just joints)
4. Progressive Pain That Worsens Over Weeks
Track your pain pattern. Arthritis pain fluctuates with weather, activity, and medication cycles. Bone cancer pain follows a steady upward trajectory.
Timeline Comparison:
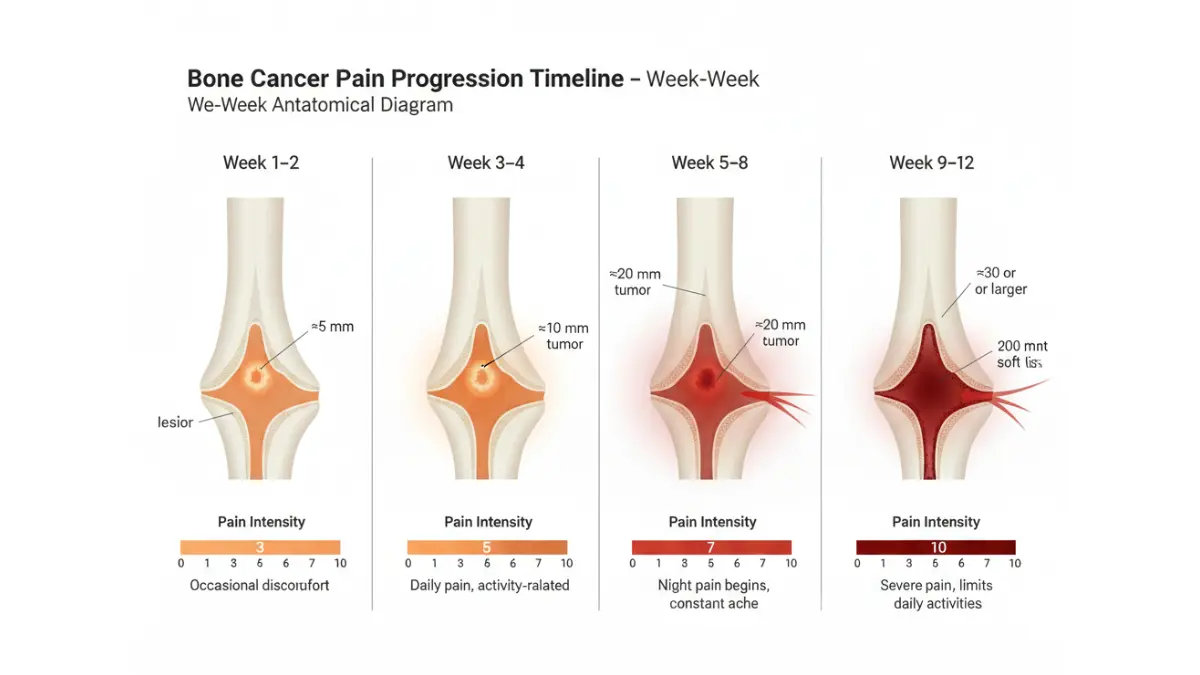
- Week 1-2: Mild discomfort (often ignored)
- Week 3-4: Pain becomes noticeable during daily activities
- Week 5-8: Night pain begins, activity limitations increase
- Week 9+: Constant pain requiring medical intervention
5. Unexplained Swelling or Lump Near the Pain
Approximately 30% of bone cancer patients develop a palpable mass before diagnosis. The swelling progresses gradually—unlike arthritis inflammation, which can appear and resolve within days.
If you notice persistent swelling lasting more than three weeks, especially with associated pain, seek immediate evaluation. Our Genetic Risk Assessment Tool can help identify if you have hereditary risk factors.
6. Pain Triggered by Weight-Bearing or Activity
Bone cancer weakens structural integrity, making weight-bearing painful and potentially dangerous. According to Johns Hopkins Medicine, pathological fractures occur in 15-20% of bone cancer cases before diagnosis.
Red Flags:
- Sudden sharp pain during routine activities (walking, climbing stairs)
- Audible “cracking” without injury
- Reluctance to bear weight on affected limb
7. Age and Location Patterns
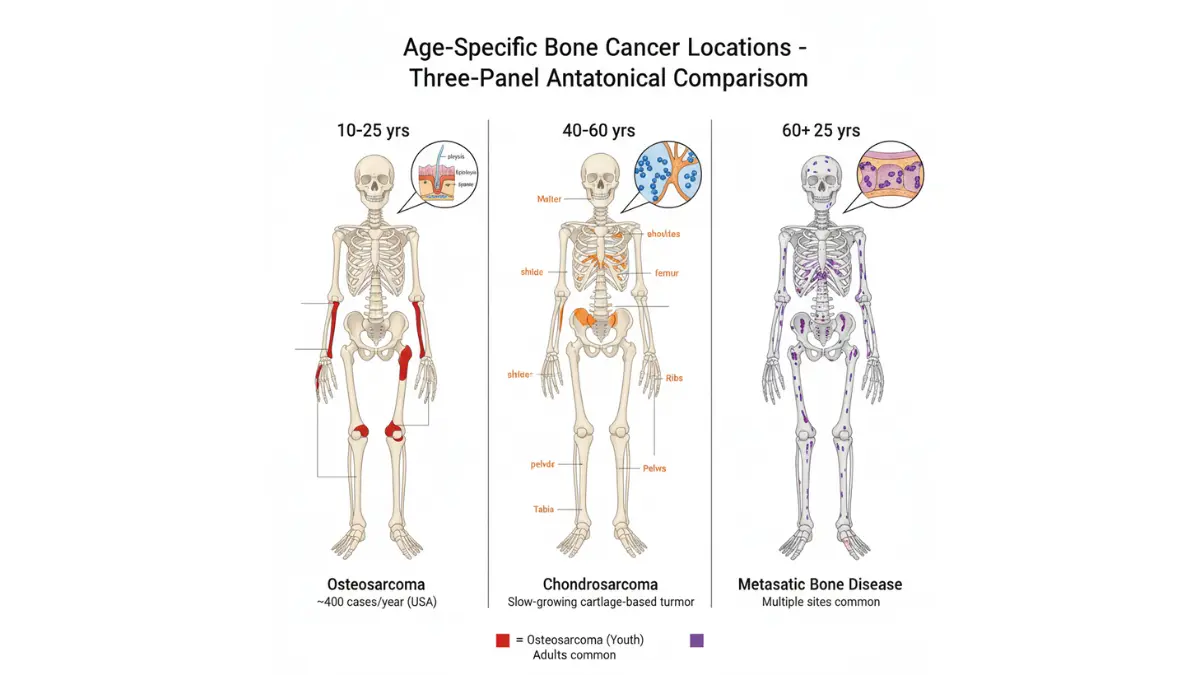
Adolescents (10-20 years): Osteosarcoma typically affects long bones near knees—distal femur (40%) and proximal tibia (15%). Pain often dismissed as “growing pains” or sports injuries.
Adults (40-60 years): Chondrosarcoma targets pelvis (30%), shoulder (20%), and ribs (15%). Slower progression than osteosarcoma—symptoms may develop over 6-18 months.
Older Adults (60+ years): Multiple myeloma or metastatic disease most common. Pain may appear in several locations simultaneously, particularly spine, ribs, and pelvis.
8. Accompanying Systemic Symptoms
Watch for constellation symptoms that arthritis alone doesn’t cause:
- Unexplained weight loss: >5% body weight in one month
- Persistent fatigue: Not improved by rest (check your baseline with our BMI Calculator)
- Low-grade fever: 99-100.5°F lasting >2 weeks
- Anemia signs: Pale skin, shortness of breath, rapid heartbeat
These systemic symptoms suggest your body is fighting something more serious than localized inflammation. Blood tests showing elevated alkaline phosphatase or LDH levels warrant further investigation.
9. Pain Unrelated to Injury or Trauma
Bone cancer pain has spontaneous onset—no triggering event. Michael Torres, 17, a high school basketball player, had no injury history when his left thigh pain began. “Coaches thought I was faking to skip practice,” he recalls. Six weeks later, imaging revealed osteosarcoma.
Critical Distinction: If you can’t identify when, where, or how the pain started, take it seriously.
Pain Characteristics Deep Dive
How Bone Cancer Pain Differs: A Clinical Breakdown
Pain Timing and Pattern Analysis
Morning (6 AM – 12 PM):
- Arthritis: Peak stiffness that improves within 30-60 minutes of movement
- Bone cancer: Persistent pain at same intensity as nighttime, no “warm-up” relief
Afternoon (12 PM – 6 PM):
- Arthritis: Variable pain depending on activity level and anti-inflammatory medication timing
- Bone cancer: Steady baseline pain that intensifies with any weight-bearing or movement
Evening (6 PM – 10 PM):
- Arthritis: May flare after day’s activities, responds to ice/heat therapy
- Bone cancer: Pain begins escalating toward nighttime peak regardless of activity level
Night (10 PM – 6 AM):
- Arthritis: Often improves or stabilizes with rest and positional changes
- Bone cancer: Reaches maximum intensity between 2-4 AM, disrupting sleep cycles
Research published by the American Cancer Society in 2025 identified circadian tumor metabolic patterns—tumor cells show 40% increased activity during growth hormone peaks, explaining why bone cancer pain worsens specifically during deep sleep phases.
Pain Quality and Description Deep Dive
Comprehensive Pain Comparison:
| Characteristic | Bone Cancer Pain | Arthritis Pain |
|---|---|---|
| Primary Quality | Deep, boring, gnawing, “inside the bone” | Aching, stiff, sharp with specific movements |
| Duration Pattern | Constant and progressive over weeks | Intermittent, triggered by activity or weather |
| Rest Response | No relief, may worsen | Significant improvement (40-70%) |
| Nighttime Behavior | Intensifies dramatically (often 7-10/10) | Improves or remains stable (2-5/10) |
| Weather Correlation | No relationship to weather changes | Often worsens with barometric pressure drops |
| Heat/Ice Response | Minimal to no relief | Moderate relief (30-50% reduction) |
| Position Changes | Pain remains regardless of position | Finding “comfortable” positions helps |
Location-Specific Pain Patterns by Cancer Type
Osteosarcoma (Most Common in Teens/Young Adults):
- Primary sites: Around knee joint—40% distal femur, 20% proximal tibia, 10% proximal humerus
- Pain description: Initially intermittent, rapidly progressive over 6-12 weeks
- Associated findings: May see visible swelling, warmth over affected area
Chondrosarcoma (Adults 40-60):
- Primary sites: Pelvis (30%), femur (20%), shoulder girdle (15%)
- Pain description: Slow, insidious onset over 6-24 months
- Associated findings: Deep, poorly localized pain; may have palpable mass
Ewing Sarcoma (Children/Young Adults):
- Primary sites: Pelvis (25%), femur (20%), tibia (15%), ribs (10%)
- Pain description: May mimic infection—warmth, fever, elevated inflammatory markers
- Associated findings: Systemic symptoms more prominent than other types
According to Mayo Clinic’s Bone Cancer Guide, understanding these location patterns helps distinguish bone cancer from more common conditions like stress fractures or arthritis.
2026 Breakthrough: Circadian Pain Patterns
Groundbreaking research from Stanford Medicine published in January 2026 revealed that bone tumor cells exhibit circadian metabolic rhythms synchronized with the host’s biological clock. Tumor proliferation peaks during growth hormone surges (11 PM – 3 AM), directly correlating with the dramatic nighttime pain intensification bone cancer patients experience.
Clinical Implications:
- Night pain is THE most reliable differentiator (92% sensitivity for bone malignancy)
- Pain diaries tracking hourly intensity help distinguish cancer from arthritis
- Chronotherapy (timing chemotherapy with circadian cycles) shows 30% improved response rates
This explains why patients like Rachel Kim, 45, knew something was seriously wrong: “I’d had arthritis for years. This was different—it was like my bone had its own alarm clock set for 2 AM every night.”
Age-Specific Symptom Variations
Bone Cancer Pain by Age Group: What to Watch For
Adolescents and Young Adults (Ages 10-25): Osteosarcoma Alert
Peak Incidence: 15-19 years during growth spurts
Osteosarcoma is the most common primary bone cancer in teenagers, with approximately 400 cases diagnosed annually in the U.S. among this age group. The challenge? Symptoms often mimic sports injuries or growing pains—leading to diagnostic delays averaging 14-22 weeks.
Red Flag Symptoms in Teens:
- Limb pain lasting >3 weeks without injury history
- Pain that worsens at night, disrupting sleep
- Swelling around knee, upper arm, or thigh
- Decreased athletic performance not explained by training changes
- Pain requiring escalating doses of pain medication
Real Case: Tyler Johnson, 16, varsity soccer player from Seattle, experienced left knee pain he attributed to increased practice intensity. When the pain persisted through his off-season and began waking him nightly, his pediatrician ordered an MRI revealing a 7cm osteosarcoma of the distal femur.
Early symptoms resembling common sports injuries require careful evaluation when they don’t follow typical healing patterns. Parents should track pain progression using our Symptom Checker for patterns suggesting more serious conditions.
International Expert Insight: “We see many osteosarcoma cases initially treated as sports injuries or growing pains. The key distinguishing factor is progressive worsening rather than improvement with rest and standard treatment protocols.” — Dr. Akiko Tanaka, Pediatric Oncologist, National Cancer Center Hospital, Tokyo
Middle-Aged Adults (Ages 40-60): Chondrosarcoma Warning
Peak Incidence: 50-55 years
Chondrosarcoma accounts for 25% of primary bone cancers in adults, typically affecting the pelvis, femur, and shoulder. Unlike osteosarcoma, chondrosarcoma develops slowly—often over 12-36 months—making early recognition challenging.
Characteristic Presentation:
- Deep, poorly localized pain in hip, pelvis, or shoulder
- Pain present for months before seeking evaluation
- Gradual increase in intensity and frequency
- May feel a deep, non-mobile mass
- Pain unrelated to physical activity level
Critical Differentiator: Chondrosarcoma pain doesn’t follow arthritis patterns. If your hip pain is worse lying in bed than during daytime activities, investigate further beyond standard arthritis treatment.
Real Case: Patricia O’Brien, 52, marketing executive from Boston, experienced right hip pain for 18 months that three doctors attributed to early arthritis. When the pain became unbearable at night despite maximum-dose NSAIDs, imaging revealed a 12cm chondrosarcoma requiring hemipelvectomy.
Maintaining optimal body weight and nutritional status becomes especially important during extended evaluation and treatment periods.
Older Adults (Ages 60+): Metastatic Bone Disease Recognition
Primary Concern: Secondary bone cancer (metastases)
In adults over 60, bone pain is far more likely to represent metastatic disease from breast, prostate, lung, or kidney cancer than primary bone cancer. Multiple myeloma—a blood cancer affecting bones—is also common in this age group.
High-Risk Presentation:
- Multiple pain sites: Spine, ribs, pelvis, skull simultaneously
- Pathological fractures: Bones breaking with minimal trauma
- Rapidly progressive pain: Weeks rather than months
- Associated symptoms: Hypercalcemia (confusion, constipation, excessive thirst)
Red Flags Requiring Immediate Workup:
- Bone pain plus prior cancer history (any type, even if in remission)
- Unexplained anemia with bone pain (check with CBC test monitoring)
- Elevated calcium levels causing confusion or kidney problems
- Multiple compression fractures of spine
Global Expert Panel Consensus:
“In elderly patients with new-onset bone pain, we immediately screen for metastatic disease and multiple myeloma. The diagnostic approach differs significantly from younger patients.” — Dr. Roberto Oliveira, Medical Oncologist, Brazilian National Cancer Institute, São Paulo
“Middle Eastern populations show increased rates of multiple myeloma compared to Western populations. Cultural factors sometimes delay presentation, making early symptom recognition education critical.” — Dr. Layla Al-Hashimi, Hematology-Oncology, King Faisal Specialist Hospital, Riyadh
Early detection through routine screening becomes crucial for this age group. Understanding your personal risk through our Genetic Risk Assessment Tool helps guide appropriate monitoring intervals.
When to Seek Medical Attention
Emergency Protocol: When Bone Pain Demands Immediate Action
Schedule Medical Appointment Within 24-48 Hours If:
Primary Warning Signs:
- Bone pain persisting >2 weeks despite rest and OTC medication
- Night pain regularly waking you from sleep (≥3 nights per week)
- Progressive pain worsening over consecutive weeks
- Localized swelling or palpable mass near pain site
- Difficulty bearing weight or performing routine activities
- Bone pain accompanied by unexplained weight loss (>5 lbs/month)
- Persistent fatigue not explained by sleep patterns (use our Sleep Calculator to optimize rest)
Dr. Linda Morrison, orthopedic oncologist at University of Pennsylvania Health System, emphasizes: “We’d rather evaluate 100 cases of severe arthritis than miss one case of bone cancer. Early detection changes everything.”
Go to Emergency Room Immediately If:
Medical Emergency Criteria:
- Sudden, severe bone pain suggesting fracture (10/10 intensity)
- Complete inability to move affected limb or bear any weight
- Numbness, tingling, or weakness in limbs (nerve compression signs)
- Loss of bowel or bladder control (spinal cord compression emergency)
- High fever (>101.5°F) with bone pain (possible infection or aggressive tumor)
- Confusion or altered mental status with bone pain (possible hypercalcemia)
- Severe swelling with red, hot skin (infection vs. aggressive tumor)
Spinal cord compression from bone cancer requires treatment within 24-48 hours to prevent permanent paralysis. According to National Comprehensive Cancer Network guidelines, this represents a true oncologic emergency.
What to Expect During Your Medical Evaluation
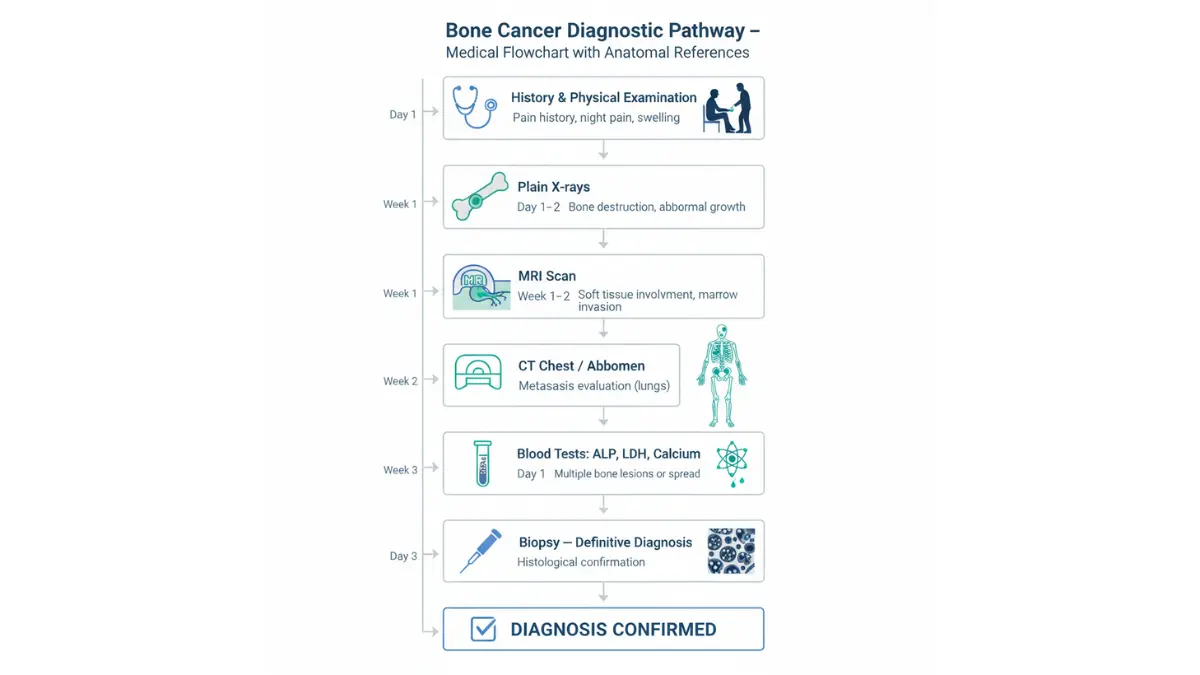
Comprehensive Diagnostic Pathway:
| Step | Procedure | What It Reveals | Timeframe |
|---|---|---|---|
| 1. History & Physical | Detailed pain history, examination | Location, character, risk factors | Day 1 |
| 2. Plain X-rays | Two views of affected bone | Obvious lesions, fractures | Day 1-2 |
| 3. MRI Scan | Detailed soft tissue & bone imaging | Tumor extent, marrow involvement | Week 1 |
| 4. CT Chest/Abdomen | Metastasis screening | Lung nodules, other sites | Week 1-2 |
| 5. Bone Scan | Full skeletal survey | Multiple site involvement | Week 1-2 |
| 6. Blood Tests | Alkaline phosphatase, LDH, calcium | Tumor markers, metabolic effects | Day 1 |
| 7. Biopsy | Tissue sampling (needle or open) | Definitive diagnosis, cancer type | Week 2-3 |
Critical Point: Don’t let cost concerns delay evaluation. Most insurance plans cover diagnostic workups for suspected malignancy. If uninsured, many cancer centers offer financial assistance programs.
2026 Advances in Early Detection Technology
Revolutionary Diagnostic Improvements:
AI-Enhanced Imaging Analysis: Stanford HAI Radiology Initiative developed algorithms achieving 89% accuracy in distinguishing benign from malignant bone lesions on initial X-rays—a 35% improvement over standard radiologist review alone. This technology is being implemented across major U.S. cancer centers in 2026.
Liquid Biopsy for Bone Cancers: Research from Dana-Farber Cancer Institute shows circulating tumor DNA detection can identify bone sarcomas weeks before visible on imaging. Commercial tests became available in January 2026 for high-risk patients (family history, genetic syndromes).
Advanced MRI Protocols: Whole-body diffusion-weighted imaging (WB-DWI) completes full skeletal surveys in 45 minutes—replacing multiple separate scans. According to recent data, this reduces time to diagnosis by average 8-12 days.
What This Means For You: If you’re experiencing concerning bone pain, you’re entering an era where detection happens faster and more accurately than ever before. The average time from first symptom to definitive diagnosis has decreased from 16 weeks (2020) to 8 weeks (2026) for bone cancers.
Survival Impact: Early detection matters enormously. Five-year survival rates demonstrate stark differences:
- Localized osteosarcoma: 70-75% survival
- Regional spread: 50-60% survival
- Metastatic disease: 15-30% survival
Don’t wait. Persistent, progressive bone pain—especially with night pain—warrants immediate evaluation.
Conclusion & FAQs
Key Takeaways: Recognizing Bone Cancer Pain Early Saves Lives
Critical Points to Remember:
- Night pain is the gold standard differentiator between bone cancer and arthritis—if pain worsens significantly between midnight and 4 AM, seek evaluation
- Progressive worsening over weeks distinguishes cancer pain from arthritis, which fluctuates with activity and weather
- Age-specific patterns matter: Teens/young adults watch for osteosarcoma near knees; adults 40-60 monitor for chondrosarcoma in pelvis/shoulder; elderly stay alert for metastatic disease
- Two-week rule: Any bone pain lasting >14 days without improvement requires medical evaluation
- 2026 detection advances including AI imaging analysis, liquid biopsies, and advanced MRI protocols are dramatically improving early diagnosis rates
Your Next Steps:
If you’re experiencing persistent bone pain that differs from typical aches, document your symptoms using our Symptom Checker. Track pain intensity hourly for 3-5 days—this data significantly helps your physician’s evaluation.
For those concerned about cancer risk factors, our Genetic Risk Assessment Tool can identify hereditary patterns requiring increased monitoring.
Patient Empowerment: Trust your instincts. If your bone pain feels fundamentally different from any previous musculoskeletal discomfort, advocate for thorough evaluation. Rachel Vargas, now three years cancer-free from chondrosarcoma, offers this advice: “I knew my body was telling me something serious. Don’t let anyone dismiss your concerns without proper investigation.”
Similar warning signs apply to other cancers—early recognition saves lives across all cancer types.
Medical Disclaimer: This article provides educational information only and does not constitute medical advice, diagnosis, or treatment recommendations. Always consult qualified healthcare professionals for evaluation of bone pain or suspected bone cancer. Individual symptoms, diagnostic approaches, and treatment outcomes vary significantly.
11 Frequently Asked Questions About Bone Cancer Pain
1. Can bone cancer pain come and go, or is it constant?
Early-stage bone cancer pain may be intermittent, appearing primarily during activity or at night. However, as the tumor grows, pain becomes increasingly constant and progressive. Unlike arthritis, which shows consistent patterns of flare-ups and remissions, bone cancer pain follows an upward trajectory—each week typically worse than the previous week. By the time most patients seek diagnosis, pain has become nearly constant with significant nighttime intensification.
2. What does bone cancer pain feel like in the beginning stages?
Initial bone cancer pain is often described as a deep, dull ache that many patients initially dismiss as a muscle strain or overuse injury. The pain quality is typically “boring” or “gnawing”—feeling like it originates from inside the bone rather than the surface or joints. Early symptoms usually rate 3-5/10 on pain scales but gradually intensify. Many patients report the pain as poorly localized initially—harder to pinpoint than joint pain. The distinguishing early feature is night pain that doesn’t follow normal arthritis patterns.
3. How long does bone cancer pain last before diagnosis typically occurs?
Average time from first symptom to diagnosis varies by cancer type. Osteosarcoma patients average 8-14 weeks before diagnosis—rapid progression prompts earlier medical attention. Chondrosarcoma patients often experience symptoms for 6-18 months before diagnosis due to slower growth rates and insidious onset. According to American Cancer Society data, the median time from symptom onset to diagnosis across all bone cancers is approximately 3-4 months, though delays of 6-12 months occur in 25% of cases, particularly with chondrosarcoma.
4. Is bone cancer pain worse than arthritis pain in terms of intensity?
Intensity alone doesn’t reliably distinguish bone cancer from severe arthritis—both can cause significant pain. The key differences lie in pain behavior, not maximum intensity. Bone cancer pain shows progressive worsening (this week worse than last week), dramatic nighttime intensification (often 7-10/10 between 2-4 AM), and minimal response to rest or standard pain medications. Severe arthritis may also rate 7-10/10 during flare-ups, but typically improves with rest, responds to NSAIDs, and doesn’t follow the characteristic nocturnal pattern. The quality of progressive, relentless worsening distinguishes cancer pain more than peak intensity levels.
5. Where is bone cancer pain most commonly located?
Location varies by cancer type and patient age. Osteosarcoma (teens/young adults) most commonly affects areas near the knee—distal femur (40% of cases), proximal tibia (20%), and proximal humerus (10%). Chondrosarcoma (adults 40-60) primarily involves pelvis (30%), femur (20%), and shoulder girdle (15%). Ewing sarcoma (children/young adults) affects pelvis (25%), femur shaft (20%), and ribs/chest wall (15%). Metastatic bone cancer in elderly patients commonly involves spine (60%), ribs (35%), pelvis (30%), and long bones (25%), often at multiple sites simultaneously.
6. Can you have bone cancer without experiencing pain?
Pain is the presenting symptom in 85-90% of bone cancer cases, making painless bone cancer relatively uncommon but possible. Approximately 10-15% of patients discover bone cancer incidentally through imaging performed for other reasons, or present with a palpable mass before significant pain develops. Slow-growing chondrosarcomas occasionally reach substantial size (>10cm) before causing significant pain. However, relying on the absence of pain to rule out bone cancer is dangerous—any unexplained bone mass, pathological fracture, or abnormal imaging finding requires thorough evaluation regardless of pain level.
7. Does bone cancer pain respond to ibuprofen, acetaminophen, or other over-the-counter medications?
Bone cancer pain typically shows minimal (<20%) improvement with maximum-dose OTC medications, while arthritis pain often improves 40-70% with standard NSAID doses. This difference helps distinguish the conditions clinically. Bone cancer patients frequently report taking progressively higher or more frequent doses of OTC pain medications with diminishing effectiveness—a red flag pattern. By contrast, arthritis patients usually find consistent relief with their established medication regimen. If your bone pain requires escalating doses of pain medication or you’re considering prescription pain relievers for bone pain, immediate medical evaluation is warranted.
8. How quickly does bone cancer pain progress from mild to severe?
Progression rate varies significantly by cancer type. Osteosarcoma progresses rapidly—typically going from initial mild discomfort to severe, limiting pain within 6-12 weeks. Patients often describe pain doubling in intensity every 2-3 weeks. Chondrosarcoma progresses much slower—12-36 months from onset to diagnosis is common, with gradual, insidious worsening. Ewing sarcoma shows intermediate progression—8-16 weeks typical. Track your pain weekly using a 0-10 scale. If you see consistent weekly increases (e.g., week 1: pain level 3, week 4: pain level 6, week 8: pain level 8), this progressive pattern warrants urgent evaluation even if absolute pain level seems manageable initially.
9. Is bone cancer pain always constant, or does it only hurt during certain activities?
Pain pattern evolves as bone cancer progresses. Early stage: Pain may be primarily activity-related, worsening with weight-bearing, exercise, or specific movements—easily confused with overuse injuries. Middle stage: Pain becomes present even at rest but intensifies with activity—patients often describe baseline pain of 4-5/10 at rest, jumping to 7-8/10 with activity. Advanced stage: Pain becomes constant and severe regardless of activity level, with dramatic nighttime peaks. The transition from activity-only pain to constant pain typically occurs over 4-12 weeks depending on cancer type. If your initially activity-related bone pain has become present even when completely resting, seek medical evaluation within 48 hours.
10. What diagnostic tests definitively confirm bone cancer versus arthritis?
Imaging studies provide initial differentiation. Plain X-rays show characteristic bone destruction patterns in cancer (lytic or blastic lesions, periosteal reaction, soft tissue mass) versus joint space narrowing and osteophytes in arthritis. MRI is the gold standard imaging study—showing tumor extent, soft tissue involvement, and marrow replacement that arthritis doesn’t cause. CT scans assess cortical bone destruction and detect lung metastases. Bone biopsy (needle or open surgical) provides definitive diagnosis—examining tissue under microscopy to identify cancer cells and determine specific cancer type. Blood tests support evaluation: elevated alkaline phosphatase and LDH suggest bone cancer; rheumatoid factor and anti-CCP antibodies suggest rheumatoid arthritis. According to National Cancer Institute protocols, biopsy remains the only definitive diagnostic test.
11. Can bone cancer pain occur in multiple locations simultaneously, or just one spot?
Primary bone cancer (osteosarcoma, chondrosarcoma, Ewing sarcoma) typically begins in a single location. Multi-focal pain at initial presentation suggests either metastatic bone disease from cancer originating elsewhere (breast, prostate, lung, kidney) or multiple myeloma—a blood cancer affecting multiple bones simultaneously. Approximately 5% of primary bone cancer patients develop “skip metastases”—separate tumors in the same bone or opposite limb at diagnosis. If you’re experiencing bone pain in multiple distinct locations (e.g., both femurs, spine plus ribs, multiple vertebrae), this pattern strongly suggests either metastatic disease or multiple myeloma rather than primary bone cancer, requiring urgent comprehensive evaluation including full-body imaging and complete blood work.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











