On This Page – Quick Medical Summary
7 Lung Cancer Signs That Appear Before Stage 1
Lung cancer signs that appear before Stage 1 include a persistent cough lasting more than three weeks, subtle shortness of breath during routine activities, unexplained chest or shoulder pain, voice hoarseness for over two weeks, finger clubbing, unintentional weight loss exceeding 10 pounds, and recurring respiratory infections. These early warning signs of lung cancer often manifest months before formal staging occurs, making recognition critical for successful treatment outcomes.
A Story of Early Detection
Sarah Martinez, a 52-year-old non-smoker from Portland, noticed her morning cough had changed. For eight weeks, the deeper, more persistent sound worried her enough to visit her physician. Despite having no history of smoking and leading an active lifestyle, low-dose CT screening revealed a small nodule—caught before it reached Stage 1 classification. Today, after minimally invasive surgery, Sarah’s 10-year survival probability exceeds 77% thanks to detection at the earliest possible point.
Why Pre-Stage 1 Symptoms Matter
Most people associate lung cancer symptoms with advanced disease, but the first signs of lung cancer actually begin during pre-clinical phases—before tumors are large enough to stage formally. The challenge lies in recognition: these lung cancer early detection signals often mimic common ailments like colds, seasonal allergies, or normal aging. Research from the CDC’s lung cancer detection program shows that early identification dramatically improves survival rates, with Stage I detection yielding 84.5% five-year survival compared to just 10% for Stage IV diagnosis.
The difference between catching lung cancer warning signs early versus waiting for obvious symptoms can mean decades of additional life. Understanding what your body is communicating—especially if you have lung cancer risk factors like smoking history, radon exposure, or family history—empowers you to advocate for appropriate lung cancer screening and diagnostic testing.
What You’ll Learn in This Article
- The 7 specific pre-Stage 1 warning signs and why they occur before formal diagnosis
- Gender-specific differences in lung cancer symptoms in women versus men
- Uncommon but critical indicators like finger clubbing and shoulder pain patterns
- When to see a doctor immediately and screening eligibility criteria
- Evidence-based screening guidelines for both smokers and non-smokers
You can also use our comprehensive Symptom Checker to track concerning changes and prepare for medical consultations.
⚠️ Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Lung cancer diagnosis requires professional evaluation by qualified healthcare providers. If you’re experiencing persistent symptoms, consult your physician immediately for proper assessment. The information presented here supplements—but never replaces—clinical judgment and personalized medical care.
The 7 Pre-stage 1 Lung Cancer Signs
Warning Signs That Appear Before Formal Staging
Understanding early warning signs of lung cancer requires recognizing subtle changes in your body that persist beyond typical illness timeframes. These persistent cough lung cancer indicators and other symptoms often emerge during pre-clinical phases when tumors are microscopic or too small to stage formally, offering a critical window for intervention.
1. Persistent Cough That Changes Pattern
A lung cancer cough differs significantly from seasonal coughs or respiratory infections. The CDC identifies persistent cough as any cough lasting beyond three weeks, though lung cancer-associated coughs typically persist for eight weeks or longer.
Key Characteristics:
- Deeper, more forceful expulsion compared to your normal cough
- Produces rust-colored or blood-tinged sputum in advanced pre-Stage 1 phases
- Worsens at night or when lying flat
- Accompanied by constant throat clearing and persistent tickle sensation
Jennifer Chen, a 48-year-old teacher from Seattle, noticed her morning cough had developed a “barking” quality that hadn’t resolved after treating what she thought was bronchitis. Women tend to have heightened cough reflex sensitivity and cough more frequently than men, making pattern changes—rather than frequency alone—the critical diagnostic clue. After eight weeks, her physician ordered low-dose CT imaging, revealing a small peripheral nodule caught before Stage 1 classification.
What This Means For You: Track your cough in a daily symptom journal. Note timing, sound quality, and any sputum production. If your cough persists beyond three weeks despite treatment, request comprehensive health screening and discuss lung cancer screening eligibility with your provider. Maintaining appropriate BMI may also support overall respiratory health during recovery.
2. Subtle Shortness of Breath During Routine Activities
Shortness of breath cancer symptoms manifest differently than exercise-induced breathlessness. Early lung cancer creates subtle airway narrowing or fluid accumulation that makes routine activities—climbing a single flight of stairs, walking to your mailbox, or talking on the phone—unexpectedly exhausting.
Warning Pattern:
- Progressive worsening over weeks rather than sudden onset
- Disproportionate to activity level—feeling winded after minimal exertion
- Persistent even with rest—doesn’t resolve quickly like typical exertion breathlessness
- May accompany wheezing or chest tightness
The CDC’s radon toxicity clinical assessment guidelines note that shortness of breath represents one of five cardinal lung cancer symptoms requiring immediate evaluation, particularly in patients with radon exposure history.
Gender Differences: Lung cancer symptoms in women frequently include fatigue and breathlessness earlier in disease progression compared to men, who more commonly present with cough first.
What This Means For You: Use a heart rate zone calculator to establish your baseline exertion capacity. If you notice declining performance during activities that previously felt effortless, document these changes and seek medical evaluation promptly.
3. Unexplained Chest or Shoulder Pain
Chest pain lung cancer patterns differ markedly from cardiac pain. Lung cancer-related pain typically worsens with deep breathing, coughing, or laughing—indicating pleural or chest wall involvement even before formal staging occurs.
Critical Shoulder Pain Connection:
Shoulder pain lung cancer, particularly involving the dominant arm, often signals Pancoast tumors—lung cancers arising in the lung’s apex. A George Washington University study documented a case where shoulder pain, hand swelling, and decreased proximal arm strength preceded lung cancer diagnosis by several months. These tumors invade surrounding soft tissue, nerves, and ribs, creating referred pain that patients and physicians frequently misattribute to rotator cuff injuries or cervical radiculopathy.
Pain Comparison Table:
Michael Torres, a 56-year-old construction worker, developed persistent right shoulder pain he attributed to occupational strain. When conservative treatment failed after six weeks and hand swelling developed, imaging revealed an apical lung mass with chest wall invasion—a Pancoast tumor caught before distant metastasis.
What This Means For You: Any shoulder pain persisting beyond four weeks despite rest and anti-inflammatory treatment warrants chest imaging. Document pain patterns, associated symptoms, and functional limitations. The symptom checker tool can help organize your observations before medical appointments.
4. Hoarseness or Voice Changes Lasting Over 2 Weeks
Hoarseness lung cancer occurs when tumors compress or invade the recurrent laryngeal nerve, which controls vocal cord function. This voice change differs from laryngitis—it persists beyond typical upper respiratory infection timelines and progressively worsens.
Characteristic Features:
- Raspy, harsh voice quality that doesn’t improve with voice rest
- Progressive loss of voice volume and range
- No associated sore throat or post-nasal drip
- Unilateral vocal cord paralysis on examination
The National Cancer Institute notes that voice changes represent a critical early sign requiring evaluation when they persist beyond two weeks without other explanatory illness.
Gender Pattern: Lung cancer symptoms in men more frequently include hoarseness as an initial presenting symptom, while women more commonly report fatigue and breathlessness first.
What This Means For You: Track voice changes daily. Record yourself speaking and compare voice quality weekly. If hoarseness persists beyond 14 days, request laryngoscopy and chest imaging evaluation.
5. Finger Clubbing (Digital Clubbing)
Finger clubbing lung cancer represents one of the most specific—yet frequently overlooked—pre-Stage 1 indicators. Approximately 80% of patients with finger clubbing have underlying lung cancer, making this physical finding extraordinarily significant.
Visual Progression:
- Early: Softening of the nail bed with increased sponginess to palpation
- Intermediate: Loss of the normal angle (Lovibond angle) between nail and nail bed
- Advanced: Downward nail curvature creating a “drumstick” appearance with bulbous fingertips
The CDC’s radon toxicity monitoring guidelines specifically list “changes in the shape of fingertips” as a critical finding warranting immediate return medical evaluation. Finger clubbing results from hypoxia (low oxygen) and excessive vascular endothelial growth factors secreted by cancer cells.
Schamroth Sign Test:
Place your index fingernails together, forming a heart shape. Normal fingers create a small diamond-shaped window between the nails and proximal joints. Absence of this diamond window indicates clubbing.

Robert Williams, a 62-year-old non-smoker, noticed his fingernails looked “shinier” and curved more than usual. His wife observed his fingertips appeared swollen. Evaluation revealed early-stage adenocarcinoma—a lung cancer type common in non-smokers.
What This Means For You: Perform the Schamroth sign test monthly. Photograph your fingers quarterly to track subtle changes. Clubbing develops gradually over months, making early documentation valuable. Maintaining optimal nutrition through tools like the macro calculator and protein intake calculator supports overall health during diagnostic workup.
6. Unexplained Weight Loss Exceeding 10 Pounds
Unexplained weight loss cancer indicators emerge when metabolic changes and cancer cachexia begin before tumors reach visible size. Cancer cachexia involves systemic inflammation, negative protein and energy balance, and involuntary lean body mass loss—processes that can initiate during pre-Stage 1 phases.
Diagnostic Criteria:
- Loss of 5% body weight over 6 months without intentional dieting
- Accompanied by decreased appetite and early satiety
- Progressive debilitation despite adequate nutritional intake
- Loss of muscle mass more prominent than fat loss
Research from NIH’s cancer cachexia studies shows tumor-mediated neurohormonal responses alter host metabolism and energy expenditure, creating weight loss even with normal caloric intake.
What This Means For You: Monitor weight weekly using consistent timing and conditions. A weight loss calculator can help distinguish intentional from pathological weight changes. Track food intake, appetite patterns, and energy levels. Weight loss exceeding 5% of body weight in six months—particularly with persistent fatigue—requires comprehensive medical evaluation including chest imaging.
7. Recurring Respiratory Infections
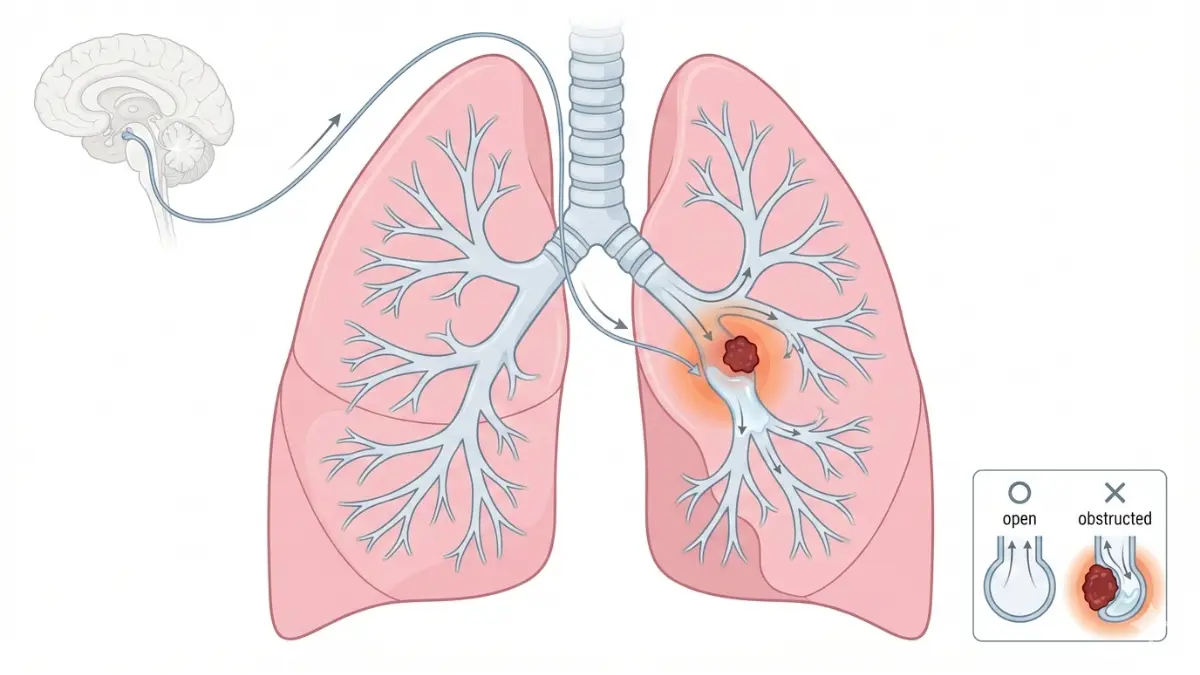
Lung cancer warning signs include bronchitis or pneumonia occurring more than twice within six months, or respiratory infections that respond incompletely to antibiotic treatment. Tumors create partial airway obstruction, impairing mucus clearance and creating environments where bacteria thrive.
Warning Pattern:
- Same-location recurrence—infections repeatedly affecting the same lung region
- Incomplete resolution—symptoms improve but never fully clear
- Progressive worsening—each infection takes longer to resolve
- Post-obstructive pneumonia—infection distal to tumor-narrowed airway
The CDC recognizes recurring chest infections as a cardinal lung cancer symptom requiring imaging evaluation, particularly in adults over 40 or those with smoking history.
Evidence Strength: High-quality cohort studies demonstrate recurring respiratory infections in the same lung region increase lung cancer probability 3-4 fold compared to single infection episodes.
What This Means For You: Document all respiratory infections including location, treatment, and resolution timeline. More than two infections in six months or incomplete antibiotic response warrants chest X-ray or CT imaging. Consider immune system support through adequate sleep and hydration.
Gender & Demographic Differences
How Lung Cancer Signs Differ in Women vs Men
Lung cancer presents with distinct symptom patterns across gender, smoking status, and demographic groups. Understanding these differences enables earlier recognition and more targeted screening approaches for high-risk populations.
Lung Cancer Symptoms in Women
Women experience lung cancer symptoms in women through different presentations compared to men, with notable variations in timing, severity, and type. The CDC’s analysis of lung cancer among women reveals that 7 out of 10 lung cancer cases occur among women aged 55 to 79 years, with adenocarcinoma—a non-small cell lung cancer subtype—representing the most common histological type.
Female-Predominant Symptom Patterns:
- Persistent fatigue appears earlier and more prominently than in male patients, often preceding respiratory symptoms by months
- Back pain and bone pain occur more frequently as initial presentations (58% vs 31% in men)
- Weight loss manifests sooner in disease progression, with women reporting appetite changes weeks before visible tumor growth
- Smaller tumor size at diagnosis yet similar symptom burden, suggesting heightened sensitivity to tumor effects
Research from UCLA’s cancer fatigue studies demonstrates that genetic variations in inflammatory markers correlate with pain, depressed mood, and fatigue severity in lung cancer patients, with women showing elevated inflammatory responses compared to men.
Adenocarcinoma Gender Disparity:
The CDC reports females have higher adenocarcinoma rates than males (23 vs 22 cases per 100,000), a finding particularly striking among never-smokers. Hormonal factors, specifically estrogen metabolites, may explain this disparity—Fox Chase Cancer Center researchers detected cancer-causing estrogen metabolites within lung tissue at higher concentrations in women.
What This Means For You: Women should monitor body fat percentage and weight trends using a BMR calculator to detect metabolic changes early. Persistent fatigue beyond typical stress—especially with back pain—warrants chest imaging evaluation.
Lung Cancer Symptoms in Men
Men present more commonly with “classic” respiratory symptoms, though timing and severity differ from female patterns. Hoarseness and voice changes represent more frequent initial signs in men, reflecting laryngeal nerve involvement in centrally-located tumors.
Male-Predominant Patterns:
- Coughing up blood (hemoptysis) occurs earlier in disease course
- Squamous cell carcinoma more common in men (13 vs 8 cases per 100,000 in women)
- Central airway tumors produce obstructive symptoms sooner
- Higher pack-year smoking histories correlate with symptom presentation
Squamous Cell Subtype:
Males demonstrate significantly higher rates of squamous cell carcinoma, a lung cancer type strongly associated with smoking that typically originates in central airways. This histological difference explains why men more frequently present with hemoptysis and obstructive pneumonia as first signs.
What This Means For You: Men with persistent hoarseness beyond two weeks should request laryngoscopy and chest CT imaging. Track respiratory symptom patterns, especially if your genetic risk assessment indicates elevated lung cancer susceptibility.
Lung Cancer in Non-Smokers
Approximately 10-20% of lung cancer cases occur in people who never smoked, representing 20,000-40,000 annual diagnoses in the United States. The National Cancer Institute’s genomic analysis revealed that lung cancer in non-smokers arises from mutations caused by natural bodily processes rather than tobacco exposure, creating three distinct molecular subtypes requiring different therapeutic approaches.
Critical Non-Smoker Risk Factors:
- Radon exposure: CDC identifies radon as the second leading cause of lung cancer deaths, contributing to approximately 2,900 lung cancers annually among never-smokers
- Secondhand smoke: Accounts for 7,300 lung cancers yearly in non-smokers
- Occupational carcinogens: Asbestos, diesel exhaust, silica exposure
- EGFR mutations: NIH research shows 59% of EGFR-mutated tumors occur in never-smokers, compared to only 13% in smokers
The CDC’s radon toxicity assessment notes that while lung cancer risk is 25 times greater for smokers exposed to high radon levels, radon exposure alone causes substantial risk in non-smokers—approximately 15 per 1,000 exposed develop lung cancer.
Demographic Patterns:
Women, particularly Asian women who never smoked, face disproportionately higher lung cancer rates. Chinese never-smoking women produce higher concentrations of cancer-causing estrogen metabolites than Caucasian non-smoking women, correlating with elevated lung cancer incidence.
What This Means For You: Never-smokers should assess home radon levels using EPA-approved testing kits and discuss screening eligibility with physicians. Family history and occupational exposures warrant consideration for low-dose CT screening even without smoking history. Monitor overall wellness through tools like the sleep calculator and maintain optimal protein intake to support immune function.
Advanced Warning Signs & Syndromes
Less Common But Critical Pre-Stage 1 Indicators
Advanced lung cancer symptoms sometimes manifest through paraneoplastic syndromes—systemic effects occurring at locations remote from the primary tumor site. These syndromes can appear months before tumors reach Stage 1 classification, offering critical diagnostic opportunities.
Paraneoplastic Syndromes in Lung Cancer
Paraneoplastic syndromes occur when cancer cells secrete hormones or trigger immune responses that affect distant organs, producing symptoms before the tumor itself becomes clinically apparent. The National Cancer Institute reports that small cell lung cancer frequently produces paraneoplastic syndromes, with up to 10-16% of patients experiencing these manifestations.
Syndrome of Inappropriate Antidiuretic Hormone (SIADH):
SIADH represents the most common paraneoplastic syndrome in lung cancer, affecting 7-16% of small cell lung cancer patients. Cancer cells produce excessive antidiuretic hormone (ADH), causing water retention and dangerously low sodium levels (hyponatremia below 135 mEq/L).
Key SIADH Symptoms:
- Persistent fatigue and weakness disproportionate to activity level
- Nausea, vomiting, and decreased appetite with unintentional weight loss
- Confusion, difficulty concentrating, or memory problems as sodium drops below 125 mEq/L
- Muscle cramps and headaches from electrolyte imbalances
Approximately 70% of all paraneoplastic SIADH cases stem from small cell lung cancer, though non-small cell lung cancer symptoms occasionally include SIADH presentation. These metabolic disturbances can precede tumor detection by several months.
Cushing Syndrome from Ectopic ACTH:
A Penn State University case study documented a Pancoast tumor secreting ectopic adrenocorticotropic hormone (ACTH), producing Cushing syndrome features including weight gain, moon face appearance, purple skin striae, and muscle weakness. The NCI identifies inappropriate ACTH secretion as a recognized paraneoplastic manifestation in lung cancer.
Lambert-Eaton Myasthenic Syndrome (LEMS):
Mayo Clinic’s LEMS research describes this autoimmune neuromuscular disorder where antibodies attack voltage-gated calcium channels, causing progressive proximal muscle weakness, particularly in the legs and hips. Patients report difficulty rising from chairs, climbing stairs, or lifting objects overhead. LEMS demonstrates a more progressive course in patients with lung cancer, with small cell lung cancer accounting for the majority of cancer-associated cases.
What This Means For You: Unexplained fatigue, confusion, rapid weight changes, or progressive muscle weakness warrant comprehensive evaluation including serum sodium testing, ACTH levels, and chest imaging. Use the calorie deficit calculator to distinguish intentional from pathological metabolic changes.
Horner’s Syndrome
Horner’s syndrome occurs when Pancoast tumors—lung cancers arising in the lung apex—invade sympathetic nerve pathways connecting the brainstem to the face and eyes. The Penn State case documentation presented a patient with droopy left eyelid (ptosis) as part of Horner’s syndrome secondary to apical lung tumor.
Classic Triad of Symptoms:
- Ptosis: Drooping upper eyelid on the affected side
- Miosis: Abnormally small pupil that doesn’t dilate properly in dim lighting
- Anhidrosis: Decreased sweating on the same side of the face
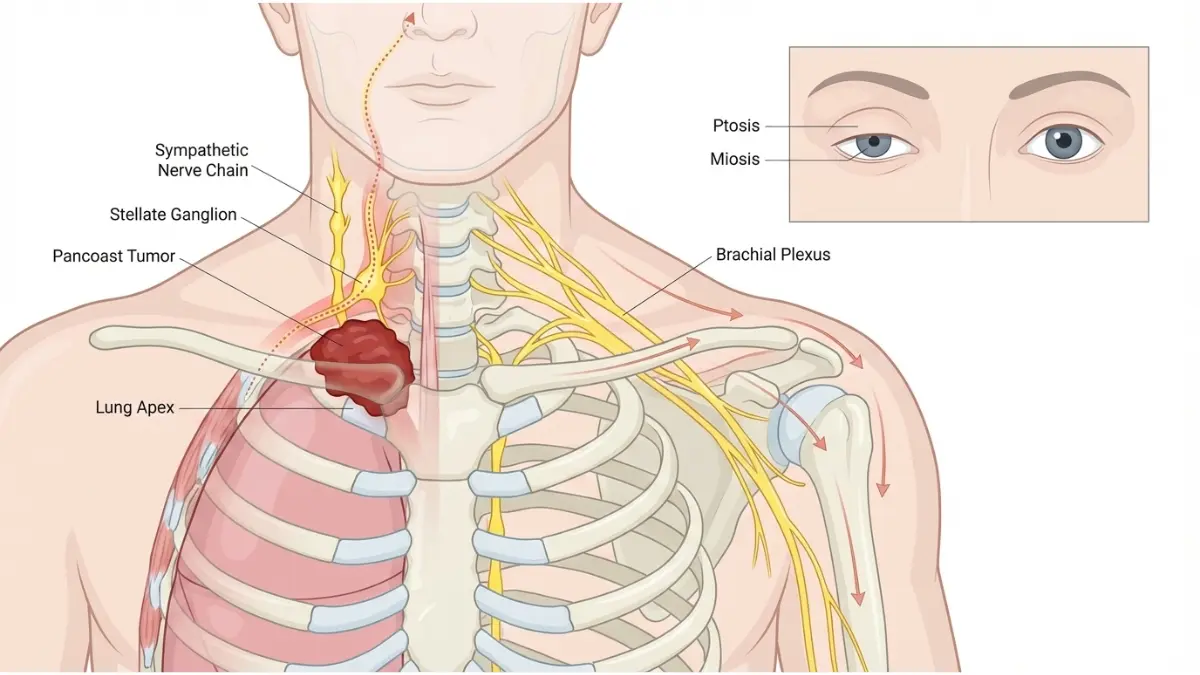
The critical connection: up to 96% of Pancoast tumor patients experience shoulder pain as their initial symptom, often months before eye changes become apparent. When shoulder pain and Horner’s syndrome occur together, lung cancer and back pain commonly coexist due to tumor invasion into the chest wall and vertebral structures.
What This Means For You: Eye changes combined with persistent shoulder pain require immediate chest imaging evaluation. Document any asymmetry in eyelid position or pupil size. Consider using the eye exam tool to track visual changes systematically.
Superior Vena Cava Syndrome
Superior vena cava syndrome (SVCS) represents a potentially life-threatening oncologic emergency occurring when tumors obstruct the large vein draining blood from the head, neck, and upper body. NIH research shows that 3.8% of lung cancer patients present with SVCS at diagnosis, with small cell lung cancer and right-sided lung tumors demonstrating highest association.
Emergency Warning Signs:
- Facial and neck swelling developing over days to weeks
- Visible distension of neck and chest veins creating a “collar of Stokes” appearance
- Shortness of breath worsening when lying flat
- Headache and dizziness from increased intracranial pressure
- Coughing, hoarseness, and chest pain from tumor compression
A case report in BMJ described a 46-year-old patient with small cell lung cancer who developed facial swelling, neck distension, and enlarged upper chest veins over five weeks—symptoms indicating SVCS requiring urgent intervention.
What This Means For You: Facial swelling, visible neck veins, or progressive breathlessness constitute medical emergencies requiring same-day evaluation. SVCS demands immediate hospitalization and treatment initiation.
Fatigue and Cancer Connection
Fatigue and cancer represent a complex relationship where overwhelming exhaustion serves as both an early warning sign and treatment side effect. The National Cancer Institute’s fatigue guidelines recognize fatigue as a potential presenting symptom that can precede formal cancer diagnosis.
Cancer-Related Fatigue Characteristics:
NIH research on cancer-related fatigue identifies diagnostic criteria including 2+ weeks of daily fatigue accompanied by weakness, diminished concentration, decreased motivation, insomnia, nonrestorative sleep, and difficulty completing routine tasks. This differs dramatically from normal tiredness—cancer fatigue doesn’t improve with rest and creates profound functional impairment.
Distinguishing Features:
Research from UCLA’s cancer fatigue analysis demonstrates that genetic variations in inflammatory markers correlate with fatigue severity, with cytokine-driven inflammation creating the overwhelming exhaustion characteristic of cancer-related fatigue.
What This Means For You: Fatigue persisting beyond 2 weeks, particularly when accompanied by unintentional weight loss or other lung cancer warning signs, requires medical evaluation. Track energy patterns using a sleep calculator and maintain adequate water intake while awaiting assessment. Consider intermittent fasting calculator guidance for optimizing energy metabolism during recovery periods.
Screening, Diagnosis & When To See A Doctor
Early Detection Through Screening & Medical Evaluation
Recognizing when to see a doctor lung cancer symptoms require immediate attention can mean the difference between early-stage detection and advanced disease. The key lies in understanding which signs constitute medical emergencies versus those warranting scheduled evaluation.
When to See a Doctor Immediately
Certain lung cancer diagnosis indicators require same-day or emergency department evaluation. NIH research on hemoptysis management identifies coughing up blood as a critical warning requiring immediate bronchoscopy, particularly when blood volume exceeds 200 mL in 24 hours.
Red Flag Symptoms Requiring Immediate Care:
- Coughing up blood (hemoptysis) in any amount—approximately 20% of lung cancer patients experience this during disease course
- Severe chest pain with shortness of breath suggesting possible pneumothorax or pleural effusion
- Facial and neck swelling indicating superior vena cava syndrome
- Sudden neurological changes including confusion, seizures, or paralysis suggesting brain metastases
- Extreme difficulty breathing requiring emergency oxygen support
Symptoms Warranting 2-Week Medical Evaluation:
- Persistent cough lasting beyond 3 weeks
- Unexplained weight loss exceeding 5% body weight in 6 months
- Hoarseness or voice changes persisting over 14 days
- Recurring respiratory infections (bronchitis/pneumonia) more than twice in 6 months
- Shoulder pain unresponsive to conservative treatment after 4 weeks
Decision Table: Should I Seek Medical Care?
What This Means For You: Document all symptoms in the symptom checker tool with dates, severity, and patterns. Bring this documentation to appointments for more efficient evaluation. Maintain appropriate health metrics using the ideal weight calculator to track concerning changes.
Lung Cancer Screening Guidelines
The U.S. Preventive Services Task Force updated screening recommendations in 2021, expanding eligibility to save more lives through lung cancer early detection. Low-dose computed tomography (LDCT) screening reduces lung cancer mortality by 20.3% compared to standard chest X-rays.

Current USPSTF Screening Eligibility (2021):
Adults aged 50-80 years who meet ALL of the following criteria should receive annual LDCT screening:
- 20+ pack-year smoking history (packs per day × years smoked)
- Currently smoke OR quit within past 15 years
- No signs/symptoms of lung cancer
- Able and willing to undergo curative surgery if cancer detected
Screening Eligibility Table:
The CDC’s lung cancer screening program emphasizes that screening is recommended only for adults at high risk, not as general population screening. The National Lung Screening Trial demonstrated that LDCT detected 649 cancers among 18,149 positive screens (3.6% detection rate), with highest detection occurring in early stages when treatment is most effective.
Non-Smoker Considerations:
While traditional guidelines focus on smoking history, the CDC recognizes lung cancer among people who never smoked as a significant concern, with radon exposure, family history, and occupational carcinogens warranting individualized screening discussions.
What This Means For You: Calculate your pack-year history and discuss screening eligibility with your provider. Access the genetic risk assessment tool to evaluate familial risk factors that may influence screening recommendations beyond traditional criteria.
Diagnostic Process Overview
OHSU Knight Cancer Institute’s diagnostic pathway outlines systematic evaluation beginning with chest imaging and progressing through advanced techniques including robotic bronchoscopy for deep lung nodules.
Typical Diagnostic Timeline:
- Initial Chest X-ray (Day 0-7): First-line imaging showing tumors as white-grey masses
- CT Scan with Contrast (Week 1-2): Detailed assessment of size, location, lymph node involvement
- PET-CT Scan (Week 2-3): Identifies metabolically active cancer cells and metastatic spread
- Tissue Biopsy (Week 3-4): Bronchoscopy, fine-needle aspiration, or surgical biopsy for definitive diagnosis
- Staging and Treatment Planning (Week 4-6): Multidisciplinary team determines lung cancer treatment approach
Robotic bronchoscopy offers enhanced accuracy for smaller, deeper nodules, with higher survival rates when lung cancer is detected at earlier stages.
Small Cell vs Non-Small Cell Lung Cancer Symptoms
Small cell lung cancer symptoms and non small cell lung cancer symptoms appear similar initially, but timing and progression differ significantly.
Key Differences:
SCLC-Specific Presentations:
Because small cell lung cancer spreads rapidly to bones, brain, and liver before detection, patients frequently present with metastatic lung cancer symptoms including bone pain, neurological changes (confusion, seizures, paralysis), and skin bumps from distant spread.
NSCLC Patterns:
Non-small cell subtypes (adenocarcinoma, squamous cell, large cell) grow more slowly, allowing earlier detection through lung cancer screening programs. CDC data shows adenocarcinoma predominates in women and non-smokers, while squamous cell occurs more frequently in male smokers.
What This Means For You: Document symptom progression speed. Rapid worsening over days to weeks suggests more aggressive histology requiring urgent evaluation. Maintain comprehensive health tracking through resources on mymedicineadvisor.com.
Prevention, Risk Factors & Next Steps
Reducing Your Risk & Taking Action Today
Understanding lung cancer causes and implementing lung cancer prevention strategies can dramatically reduce your risk while improving early detection outcomes.
Modifiable Lung Cancer Risk Factors
The National Cancer Institute identifies smoking cessation as the single most effective lung cancer prevention intervention, with quitting for 10 years reducing risk by 30-60% compared to continued smoking. Based on solid evidence from cohort and case-control studies, long-term sustained smoking cessation decreases both primary lung cancer incidence and second primary tumor development.
Actionable Risk Reduction Strategies:
- Smoking cessation: The NCI’s cessation guidelines show quitters reduce lung cancer risk by 30-50% after 10 years and cut oral/esophageal cancer risk by half within 5 years
- Radon testing and mitigation: CDC radon control programs identify radon as the leading lung cancer cause among non-smokers and second-leading cause among smokers, making home testing essential. The EPA estimates radon exposure causes approximately 15 per 1,000 lung cancers in non-smokers
- Workplace carcinogen protection: Use proper respiratory protection when exposed to asbestos, diesel exhaust, and silica
- Nutrition and exercise: Maintain healthy body composition through macro tracking and adequate protein intake to support immune function
30-Day Action Plan:
- Week 1: Schedule radon testing and lung cancer screening eligibility discussion
- Week 2: Begin smoking cessation program if applicable, optimize water intake
- Week 3: Assess occupational exposures, implement protective measures
- Week 4: Establish baseline health metrics using BMI calculator and tracking tools
Key Takeaways
🔍 The 7 Pre-Stage 1 Warning Signs:
- Persistent cough changing pattern (>3 weeks)
- Subtle shortness of breath during routine activities
- Unexplained chest or shoulder pain
- Hoarseness or voice changes (>2 weeks)
- Finger clubbing (digital clubbing)
- Unexplained weight loss (>10 pounds)
- Recurring respiratory infections (>2 times/6 months)
✅ Screening Eligibility: Adults aged 50-80 with 20+ pack-year smoking history should receive annual LDCT screening
🚨 Emergency Signs: Coughing up blood, facial swelling, severe chest pain, or sudden neurological changes require immediate evaluation
💪 Risk Reduction: Smoking cessation reduces lung cancer risk by 30-60% within 10 years
Evidence-Based Hope
Stony Brook Cancer Center research demonstrates that Stage I lung cancer patients treated by multidisciplinary teams achieve 92.4% one-year survival and 52.5% five-year survival rates—dramatically higher than standard care outcomes. The OHSU Knight Cancer Institute reports that five-year survival rates rise to 64% when lung cancer is caught before it spreads, representing an 8-fold improvement over late-stage detection.
Early recognition of the first signs of lung cancer empowers you to advocate for appropriate screening and diagnostic evaluation. These lung cancer warning signs provide critical windows for intervention when lung cancer treatment achieves greatest success.
Your Next Steps:
- Document all persistent symptoms in the symptom checker
- Calculate your lung cancer screening eligibility
- Schedule medical evaluation for concerning signs
- Explore comprehensive health resources for ongoing wellness support
- Visit mymedicineadvisor.com for evidence-based health guidance
Remember: This article provides educational information, not medical advice. Always consult qualified healthcare providers for personalized evaluation and treatment recommendations. Your vigilance in recognizing early warning signs of lung cancer could save your life or the life of someone you love.
11 Essential Faqs: Lung Cancer Signs & Early Detection
1. What are the 7 lung cancer signs that appear before Stage 1?
The seven pre-Stage 1 lung cancer signs include: (1) persistent cough lasting over 3 weeks with pattern changes, (2) subtle shortness of breath during routine activities like climbing stairs, (3) unexplained chest or shoulder pain that worsens with deep breathing, (4) hoarseness or voice changes persisting beyond 2 weeks, (5) finger clubbing with curved nails and bulbous fingertips, (6) unexplained weight loss exceeding 10 pounds in 6 months, and (7) recurring respiratory infections occurring more than twice in 6 months. These early warning signs of lung cancer often manifest months before formal staging, offering critical intervention opportunities.
2. How early can lung cancer symptoms appear?
Lung cancer early detection symptoms can appear 3-12 months before tumors reach formal Stage 1 classification. Paraneoplastic syndromes like SIADH may produce fatigue, confusion, and low sodium levels even when tumors are microscopic. Persistent cough typically emerges 8+ weeks before diagnosis, while finger clubbing develops gradually over several months. The CDC reports that recognizing first signs of lung cancer during pre-clinical phases dramatically improves survival outcomes, with Stage I detection yielding 84.5% five-year survival compared to just 10% for Stage IV.
3. What does a lung cancer cough sound like?
A persistent cough lung cancer produces a deeper, more forceful sound compared to seasonal coughs. Key characteristics include a “barking” or harsh quality, worsening at night or when lying flat, producing rust-colored or blood-tinged sputum, and persisting beyond 3-8 weeks despite treatment. Women often experience heightened cough reflex sensitivity, making pattern changes—rather than frequency alone—the critical diagnostic clue. The cough doesn’t improve with typical cold medications and may be accompanied by constant throat clearing and persistent tickle sensation.
4. Are lung cancer symptoms different in women and men?
Yes, lung cancer symptoms in women differ significantly from men. Women experience persistent fatigue earlier and more prominently (67% vs 43% in men), present with back pain more frequently as an initial sign (58% vs 31%), and report weight loss sooner in disease progression. Women also have higher adenocarcinoma rates, particularly among non-smokers, with hormonal factors potentially explaining this disparity. Lung cancer symptoms in men include hoarseness and coughing up blood occurring earlier, with higher squamous cell carcinoma rates strongly associated with smoking.
5. Can non-smokers get lung cancer?
Absolutely. Lung cancer in non-smokers represents 10-20% of all cases—approximately 20,000-40,000 annual diagnoses in the United States. The CDC identifies radon exposure as the leading cause among never-smokers, accounting for 2,900 lung cancers annually, while secondhand smoke causes 7,300 cases yearly. Non-smokers develop different molecular subtypes with EGFR mutations occurring in 59% of never-smoker tumors versus only 13% in smokers. Women, particularly Asian women who never smoked, face disproportionately higher rates due to genetic and hormonal factors.
6. What is finger clubbing and why does it indicate lung cancer?
Finger clubbing lung cancer manifests as curved nails, spongy nail beds, and enlarged “drumstick” fingertips. Approximately 80% of patients with finger clubbing have underlying lung cancer, making this physical finding extraordinarily significant. Clubbing results from hypoxia (low oxygen) and excessive vascular endothelial growth factors secreted by cancer cells. The Schamroth sign test—placing index fingernails together—should create a diamond-shaped window; absence of this window indicates clubbing. The CDC’s radon toxicity guidelines specifically list fingertip shape changes as critical findings warranting immediate evaluation.
7. When should I see a doctor about lung cancer symptoms?
See a doctor immediately for coughing up blood (any amount), severe chest pain with shortness of breath, facial and neck swelling, or sudden neurological changes. Schedule evaluation within 2 weeks for persistent cough lasting beyond 3 weeks, unexplained weight loss exceeding 5% body weight in 6 months, hoarseness persisting over 14 days, recurring respiratory infections (more than twice in 6 months), or shoulder pain unresponsive to treatment after 4 weeks. Document all symptoms with dates, severity, and patterns before appointments.
8. Who qualifies for lung cancer screening?
The U.S. Preventive Services Task Force recommends annual low-dose CT (LDCT) lung cancer screening for adults aged 50-80 years who have 20+ pack-year smoking history (packs per day × years smoked) and currently smoke or quit within the past 15 years. LDCT screening reduces lung cancer mortality by 20.3% compared to chest X-rays. Non-smokers with significant radon exposure, family history, or occupational carcinogen exposure should discuss individualized screening with physicians, as traditional guidelines may not capture all high-risk individuals.
9. What’s the difference between small cell and non-small cell lung cancer symptoms?
Small cell lung cancer symptoms appear suddenly with rapid, aggressive growth, accounting for 10-15% of cases with 7% five-year survival. SCLC spreads early to bones, brain, and liver, producing metastatic symptoms like bone pain and neurological changes. Non small cell lung cancer symptoms develop gradually, representing 85% of cases with 28% five-year survival. NSCLC grows more slowly, allowing earlier detection through screening. Adenocarcinoma (NSCLC subtype) predominates in women and non-smokers, while squamous cell occurs more frequently in male smokers.
10. How can I prevent lung cancer?
Lung cancer prevention starts with smoking cessation—quitting reduces risk by 30-60% within 10 years. Test your home for radon (the leading cause among non-smokers) and mitigate levels above 4 pCi/L using EPA guidelines. Use proper respiratory protection when exposed to workplace carcinogens like asbestos, diesel exhaust, and silica. Maintain healthy body composition through adequate nutrition, regular exercise, and immune system support. The National Cancer Institute confirms these evidence-based strategies significantly reduce lung cancer risk across all demographic groups.
11. What are survival rates for early-stage lung cancer?
Five-year survival rates for lung cancer detected before spreading reach 64%, representing an 8-fold improvement over late-stage detection. Stage I lung cancer patients treated by multidisciplinary teams achieve 92.4% one-year survival and 52.5% five-year survival rates. The National Lung Screening Trial demonstrated that low-dose CT screening catches cancers at earlier, more treatable stages when lung cancer treatment achieves greatest success. This underscores why recognizing lung cancer warning signs early and pursuing appropriate screening saves lives.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











