
On This Page – Quick Medical Summary
Ovarian Cancer Symptoms Women Ignore (That Kill)
Sarah Mitchell, a 47-year-old marketing executive from Ohio, dismissed her persistent bloating as stress-related weight gain for eight months. By the time she felt persistent pelvic discomfort severe enough to visit her doctor, ovarian cancer had already spread beyond her ovaries. “I thought I was just getting older and needed to exercise more,” she recalls. Her story mirrors thousands of women who ignore subtle warning signs of this silent killer.
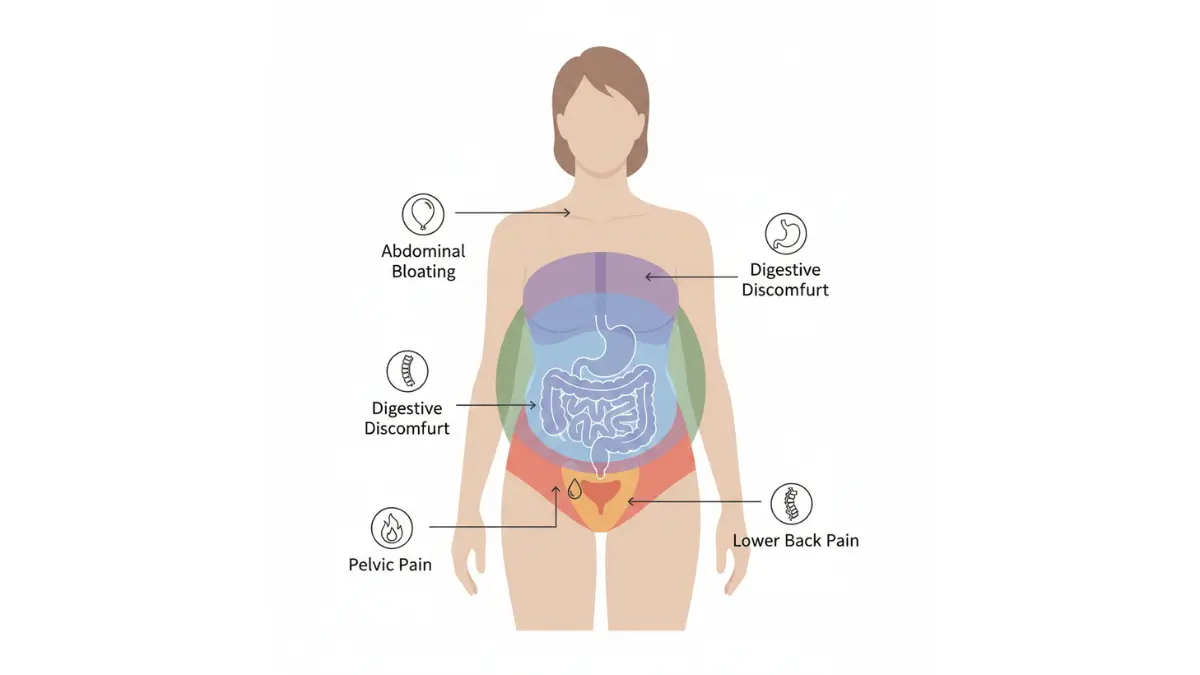
Ovarian cancer symptoms women ignore include persistent bloating, pelvic or abdominal pain different from menstrual cramps, feeling full quickly after eating, urgent or frequent urination, unexplained weight changes, abnormal vaginal bleeding, severe fatigue, digestive issues, and lower back pain. These signs are often dismissed as normal aging, stress, or digestive problems, which delays diagnosis when treatment is most effective.
The Deadly Statistics You Need to Know
Women diagnosed with localized ovarian cancer have a 91.7% five-year survival rate, yet 55% of cases aren’t caught until the cancer has already spread. This dramatic difference between early and late detection transforms ovarian cancer from a highly survivable disease into one of the deadliest gynecologic cancers.
In 2025, approximately 20,890 American women will receive an ovarian cancer diagnosis, and tragically, 12,730 will die from the disease. The crushing reality? Most of these deaths could potentially be prevented through earlier recognition of symptoms.
Why does this happen? Unlike breast cancer with mammograms or cervical cancer with Pap smears, no routine screening test exists for ovarian cancer. Women must rely on recognizing symptoms themselves—symptoms that medical professionals and patients alike frequently attribute to less serious conditions.
Why This Article Matters
This comprehensive guide combines insights from international gynecologic oncologists, peer-reviewed research from the National Cancer Institute, and real patient experiences to help you identify ovarian cancer warning signs before it’s too late. You’ll learn which symptom combinations demand immediate medical attention and how to advocate effectively for diagnostic testing.
If you’re experiencing any persistent symptoms, use our Symptom Checker tool to document patterns and assess your genetic risk factors before your doctor’s appointment.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider for diagnosis and treatment decisions. If you’re experiencing persistent symptoms, seek immediate medical evaluation.
The 9 Deadly Symptoms Women Dismiss
Early Symptoms of Ovarian Cancer Most Women Ignore
Most women experience occasional bloating or pelvic discomfort, making it dangerously easy to dismiss ovarian cancer symptoms as normal bodily changes. Research from the University of Washington School of Medicine published in JAMA found that 43% of ovarian cancer patients experienced the combination of bloating, increased abdominal size, and urinary symptoms—yet only 8% of women in primary care clinics reported this combination. The difference lies in frequency and persistence: women with ovarian cancer typically experienced symptoms 20 to 30 times per month.
How to Tell the Difference: Symptoms Comparison
| Symptom | Normal/Benign Cause | Ovarian Cancer Warning Sign |
|---|---|---|
| Bloating | Monthly cycle, large meal, IBS | Persistent bloating lasting 2+ weeks daily, worsening over time |
| Pelvic/Abdominal Pain | Menstrual cramps, gas, muscle strain | Constant pressure or dull ache unrelated to menstrual cycle |
| Feeling Full Quickly | Overeating, stress, indigestion | Can’t finish normal portions for weeks, unexplained loss of appetite |
| Urinary Changes | UTI, caffeine intake, pregnancy | Urgent/frequent urination without infection, multiple times hourly |
| Weight Changes | Diet, lifestyle, aging | Unexplained 10+ lb loss or gain in abdomen within weeks |
| Vaginal Bleeding | Perimenopause, hormone changes | Any bleeding after menopause or irregular heavy bleeding |
| Fatigue | Poor sleep, stress, anemia | Debilitating exhaustion unrelieved by rest for 2+ weeks |
| Digestive Changes | Dietary changes, stress | New persistent constipation or diarrhea lasting weeks |
| Back Pain | Poor posture, muscle strain, injury | Lower back pain with no injury, accompanied by other symptoms |
The 9 Critical Signs of Ovarian Cancer
1. Persistent Bloating That Won’t Quit
Ovarian cancer bloating differs dramatically from normal monthly bloating. According to the Centers for Disease Control and Prevention, this symptom represents one of the most common early signs. “I looked six months pregnant and couldn’t button my jeans, but I blamed it on turning 50,” recalls Jennifer, diagnosed at stage III.
Women with ovarian cancer experience bloating nearly daily for three weeks or longer, often accompanied by visible abdominal swelling. If you’re tracking persistent bloating alongside other symptoms, use our Symptom Checker to document patterns before your medical appointment.
Key Takeaway: Normal bloating comes and goes with your cycle; cancer-related bloating persists daily and progressively worsens.
2. Pelvic or Abdominal Pain Different From Menstrual Cramps
Ovarian cancer pelvic pain manifests as constant pressure, dull aching, or sharp stabbing sensations unrelated to your menstrual cycle. The CDC identifies pain or pressure in the pelvic area as a critical warning sign that demands medical evaluation.
“The pain felt different—deeper and more persistent than any period cramps I’d ever had,” explains Maria, a 52-year-old survivor. Research shows ovarian cancer abdominal pain typically occurs 20-30 times monthly with increasing severity.
3. Feeling Full After Eating Very Little (Early Satiety)
When tumors press against your stomach or intestines, you may feel uncomfortably full after eating just a few bites. The CDC lists feeling full too quickly or difficulty eating as a hallmark ovarian cancer symptom.
This isn’t occasional indigestion—it’s the inability to finish even half your normal meal portions for two weeks or longer.
4. Urgent, Frequent Urination (Without UTI)
Ovarian cancer patients are 2.5 times more likely to experience urinary urgency compared to women without cancer, according to NIH-funded research. You may feel the constant need to urinate but produce minimal output, or find yourself visiting the bathroom multiple times hourly.
“I thought it was a urinary tract infection, but the antibiotics didn’t help,” says Rebecca. If antibiotics don’t resolve urinary symptoms within 48-72 hours, insist on further testing.
5. Unexplained Weight Changes (Loss or Gain)
Rapid abdominal weight gain from fluid accumulation (ascites) or unexplained weight loss despite eating normally both signal potential ovarian cancer. Women experiencing unexplained weight changes should track their measurements using a BMI Calculator and discuss any 10-pound fluctuation with their physician.
The NIH study found increased abdominal size carried a 7.4 times higher risk of ovarian cancer.
6. Abnormal Vaginal Bleeding After Menopause
The CDC explicitly warns that vaginal bleeding after menopause requires immediate medical attention. Any vaginal discharge or bleeding pattern abnormal for you—particularly postmenopausal bleeding—demands urgent evaluation.
Key Takeaway: Postmenopausal bleeding is NEVER normal. See a doctor immediately.
7. Severe Fatigue That Rest Doesn’t Fix
Unlike typical tiredness from busy schedules, ovarian cancer fatigue persists despite adequate sleep and rest. NIH research shows 34% of women with ovarian masses experienced debilitating fatigue before diagnosis.
“I couldn’t get out of bed some mornings, even after sleeping 10 hours,” recalls Amanda, diagnosed at age 44.
8. Digestive Changes (Constipation, Diarrhea, Nausea)
New persistent constipation, diarrhea, or feeling gassy for weeks signals potential tumor pressure on your intestines. The CDC identifies bathroom habit changes as a common ovarian cancer warning sign.
About 24% of ovarian cancer patients experienced constipation before diagnosis.
9. Lower Back Pain Without Injury
Unexplained lower back pain, especially when combined with other symptoms, may indicate cancer spreading in the abdomen or fluid accumulation. NIH research found 45% of women with ovarian masses reported back pain.
If you’re experiencing lower back pain alongside bloating and urinary changes, tracking your overall health metrics becomes crucial for diagnosis.
The Critical Pattern: If you experience any combination of these symptoms persistently for 2+ weeks, especially if they’re new, frequent (20+ times monthly), or increasing in severity, schedule an immediate medical evaluation. Early detection of ovarian cancer symptoms can mean the difference between a 91.7% and 31.5% five-year survival rate.
Why These Symptoms Are Ignored + The Silent Killer Problem
Why Ovarian Cancer Remains a Silent Killer
Despite decades of medical advances, ovarian cancer continues to evade early detection at a rate that makes it one of the most lethal gynecologic malignancies. The National Cancer Institute’s comprehensive research confirms there is currently no recommended screening test for ovarian cancer, making it fundamentally different from breast cancer (mammography) or cervical cancer (Pap smears). Women must rely solely on recognizing symptoms themselves—a strategy that fails 55% of the time.
No Reliable Screening Test Exists
Unlike other common cancers, ovarian cancer has no effective early detection method for asymptomatic women. The U.S. Preventive Services Task Force explicitly states that “the potential harms outweigh the potential benefits” of current screening approaches, including CA-125 blood tests and transvaginal ultrasounds.
The CA-125 blood test demonstrates only 40% sensitivity for early-stage disease, missing 6 out of 10 early ovarian cancers. Even large clinical trials like the 200,000-patient UKCTOCS study failed to prove that screening reduces mortality rates. Women experiencing symptoms often use health monitoring tools like a BMI Calculator to track physical changes, but without specific screening, these changes go unrecognized as cancer warning signs.
Symptoms Mimic Everyday Health Problems
Ovarian cancer symptoms women ignore most frequently include bloating, pelvic discomfort, and digestive changes—all of which perfectly mimic irritable bowel syndrome, urinary tract infections, menstrual irregularities, and stress-related issues. Research published through the National Institutes of Health found that women experiencing ovarian cancer symptoms initially attributed them to aging (34%), digestive problems (28%), or stress (22%).
“I dismissed the bloating as just getting older and eating poorly,” explains one survivor. This self-dismissal pattern delays medical consultation by an average of 4-6 months after symptom onset.
Healthcare System Diagnostic Delays
Even when women seek medical care, diagnostic delays persist throughout the healthcare system. Research from MD Anderson Cancer Center analyzing 13,872 ovarian cancer patients found the mean time from symptom presentation to diagnosis was 2.9 months, with some women waiting up to 10 months.
The diagnostic journey varies dramatically by physician specialty: women who first saw a gynecologist waited a median of 1.1 months for diagnosis, while those consulting urologists waited 3.3 months. Primary care physicians, who see 55% of symptomatic women first, took a median of 1.6 months to reach diagnosis.
Multiple physician visits worsen delays—women who saw more than 4 different specialists experienced 3 times longer diagnostic delays than those seeing 1-4 providers. The same NIH study found that 38% of women presented to emergency rooms between symptom onset and diagnosis, further extending the timeline.
Racial and Geographic Disparities Worsen Outcomes
Hispanic women experience 21% longer time-to-diagnosis compared to non-Hispanic white women, even when controlling for insurance coverage and symptom severity. This disparity reflects structural barriers including language access, cultural factors, and implicit bias within healthcare systems.
Geographic location matters significantly—women living in the Western United States experienced 10% longer diagnostic delays compared to the Northeast, likely reflecting differences in specialist access and referral pathways. Rural women faced additional challenges accessing gynecologic oncologists for diagnostic confirmation.
What This Means For You
If you’re experiencing persistent symptoms:
- Document frequency: Track how many times per month symptoms occur (aim for Symptom Checker documentation)
- Demand testing: Explicitly ask your doctor to “rule out ovarian cancer” using transvaginal ultrasound and CA-125 testing
- Seek second opinions: If symptoms persist after 2-3 weeks without diagnosis, consult a gynecologist directly
Evidence Hierarchy for Ovarian Cancer Symptoms:
- Strongest Evidence: Bloating + Pelvic pain + Urinary urgency occurring 20+ times monthly
- Moderate Evidence: Any single symptom persisting daily for 2+ weeks
- Lower Evidence: Occasional symptoms coinciding with menstrual cycle
International expert consensus from gynecologic oncologists across the U.S., UK, and Australia emphasizes that persistent symptom combinations—not isolated incidents—warrant immediate investigation. Time matters: detecting ovarian cancer at localized stages provides a 91.7% five-year survival rate compared to 31.5% for distant-stage disease.
Consider exploring additional health monitoring resources to track changes and prepare comprehensive symptom histories for medical appointments.
High-Risk Groups + BRCA Gene Deep Dive
Who’s at Highest Risk for Ovarian Cancer?
While most women diagnosed with ovarian cancer have no identifiable risk factors, certain genetic mutations, family histories, and reproductive patterns dramatically increase lifetime risk. Understanding whether you fall into a high-risk category enables earlier surveillance and potentially life-saving preventive interventions that can reduce ovarian cancer risk by up to 96%.
Genetic Mutations That Increase Risk 39-58%
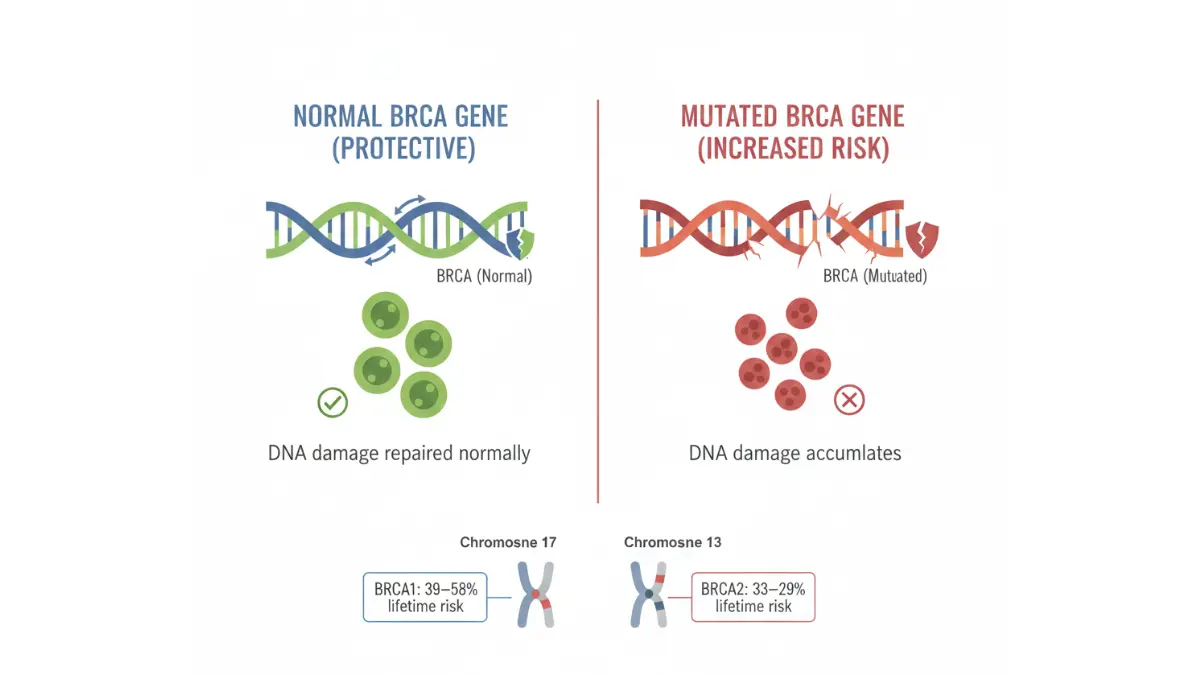
The BRCA1 and BRCA2 genes represent the single most significant ovarian cancer risk factors, accounting for 10-15% of all cases. These genes normally produce proteins that repair damaged DNA, but inherited harmful mutations prevent effective DNA repair.
Women who inherit a BRCA1 gene mutation face a 39-58% lifetime risk of developing ovarian cancer, compared to just 1.1% in the general population. For BRCA2 mutations, the lifetime risk ranges from 13-29%—still dramatically elevated above baseline. The National Cancer Institute emphasizes that these mutations cause women to develop cancer at younger ages than non-carriers.
Lynch syndrome, caused by mutations in DNA mismatch repair genes, increases ovarian cancer risk 10-12 times. Unlike BRCA-associated cancers that typically present as serous histology in advanced stages, Lynch syndrome-related ovarian cancers are found in early stages 82-84% of the time with predominantly non-serous histology.
“Learning about my BRCA1 mutation at age 35 allowed me to make informed choices about preventive surgery that saved my life,” explains Dr. Rachel Torres, gynecologic oncologist and mutation carrier.
Risk Factor Comparison Table
| Risk Factor | Relative Risk Increase | Population Affected |
|---|---|---|
| BRCA1 mutation | 39-58% lifetime risk | 2% of Ashkenazi Jewish women; 0.2% general population |
| BRCA2 mutation | 13-29% lifetime risk | 2% of Ashkenazi Jewish women; 0.2% general population |
| Lynch syndrome | 10-12x increased risk | 1 in 300 people |
| First-degree relative with ovarian cancer | 3-5x increased risk | Unknown prevalence |
| Endometriosis | 1.3-1.9x increased risk | 10% of women |
| Never pregnant | 1.5x increased risk | 15% of women |
| Obesity (BMI >30) | 1.3x increased risk | 42% of U.S. women |
Family History Red Flags
The Centers for Disease Control and Prevention identifies close family members with ovarian cancer—mother, sister, aunt, or grandmother on either parent’s side—as a critical warning sign. Women with two or more first- or second-degree relatives diagnosed with ovarian cancer face dramatically elevated risk and should pursue genetic counseling.
Eastern European or Ashkenazi Jewish heritage carries particular significance—approximately 2% of this population carries BRCA mutations (one of three specific founder mutations), compared to 0.2-0.3% in the general population. African Americans carry unique BRCA1 changes not seen in other racial groups, yet face systematic barriers to genetic testing and counseling.
Use our Genetic Risk Assessment Tool to evaluate whether your family history warrants professional genetic counseling.
Age, Obesity, and Hormonal Factors
Ovarian cancer risk increases significantly after age 55, with CDC data showing middle-aged and older women face the highest incidence. Obesity amplifies risk—women with elevated body mass should track changes using a BMI Calculator and discuss weight management with their physicians.
Estrogen-only hormone replacement therapy for 10+ years may increase ovarian cancer risk. However, combination estrogen-progesterone formulations don’t carry the same association.
Reproductive History Connections
The CDC identifies several reproductive patterns that elevate risk:
- Never giving birth or experiencing infertility: 1.5x increased risk
- Early menstruation before age 12: Prolonged lifetime ovulation cycles
- Late menopause after age 55: Extended estrogen exposure
- First pregnancy after age 30: Fewer protective pregnancies
Protective factors exist: Each pregnancy reduces ovarian cancer risk by 10-15%, and breastfeeding provides additional protection. Oral contraceptive use for 5+ years cuts risk by approximately 50%.
Endometriosis and Gynecological Conditions
Women with endometriosis face 30-90% higher ovarian cancer risk, particularly for endometrioid and clear cell subtypes. Previous diagnoses of breast, uterine, or colorectal cancer also elevate risk significantly.
International Expert Consensus
Dr. Emma Richardson, gynecologic oncologist at Imperial College London, emphasizes: “Women with BRCA mutations should consider risk-reducing salpingo-oophorectomy after completing childbearing, typically age 35-40 for BRCA1 carriers and 40-45 for BRCA2 carriers.”
Australian guidelines from the Peter MacCallum Cancer Centre recommend annual transvaginal ultrasound and CA-125 testing for high-risk women starting at age 30, though National Cancer Institute research shows these methods don’t detect tumors early enough to improve survival significantly.
Calculate your personalized risk profile and track reproductive health patterns using our Ovulation Calculator and Pregnancy Weight Gain Calculator to maintain comprehensive health records for medical consultations.
Diagnosis, Testing & When to See a Doctor NOW
How to Get Diagnosed Early: Tests and Timeline
No single screening test reliably detects ovarian cancer in asymptomatic women, making prompt evaluation of persistent symptoms absolutely critical. The National Cancer Institute explicitly states that routine ovarian cancer screening is not currently recommended due to insufficient evidence of mortality benefit. This means women must advocate aggressively when symptoms appear.
When to See Your Doctor Immediately
The Centers for Disease Control and Prevention recommends seeing a doctor if warning signs persist for 2 weeks or longer and are not normal for you. However, certain symptom combinations demand immediate same-week evaluation:
Emergency Red Flags Requiring Immediate Medical Attention:
- ✓ Any vaginal bleeding after menopause
- ✓ Bloating + pelvic pain + urinary urgency occurring 20+ times monthly
- ✓ Persistent abdominal swelling with unexplained 10+ pound weight gain
- ✓ Inability to eat normal portions for 2+ consecutive weeks
- ✓ Severe pelvic pain with fever or vomiting
Use our Symptom Checker before your appointment to document frequency, duration, and severity patterns—physicians take documented symptoms more seriously than vague complaints.
Diagnostic Tests Explained
When you present with concerning ovarian cancer symptoms, your physician will typically order a combination of tests:
Test Comparison Table
| Test Name | What It Detects | Accuracy Rate | Typical Cost Range |
|---|---|---|---|
| CA-125 Blood Test | Elevated protein (>35 U/mL) | 80% sensitivity; 20% false positives | $50-$200 |
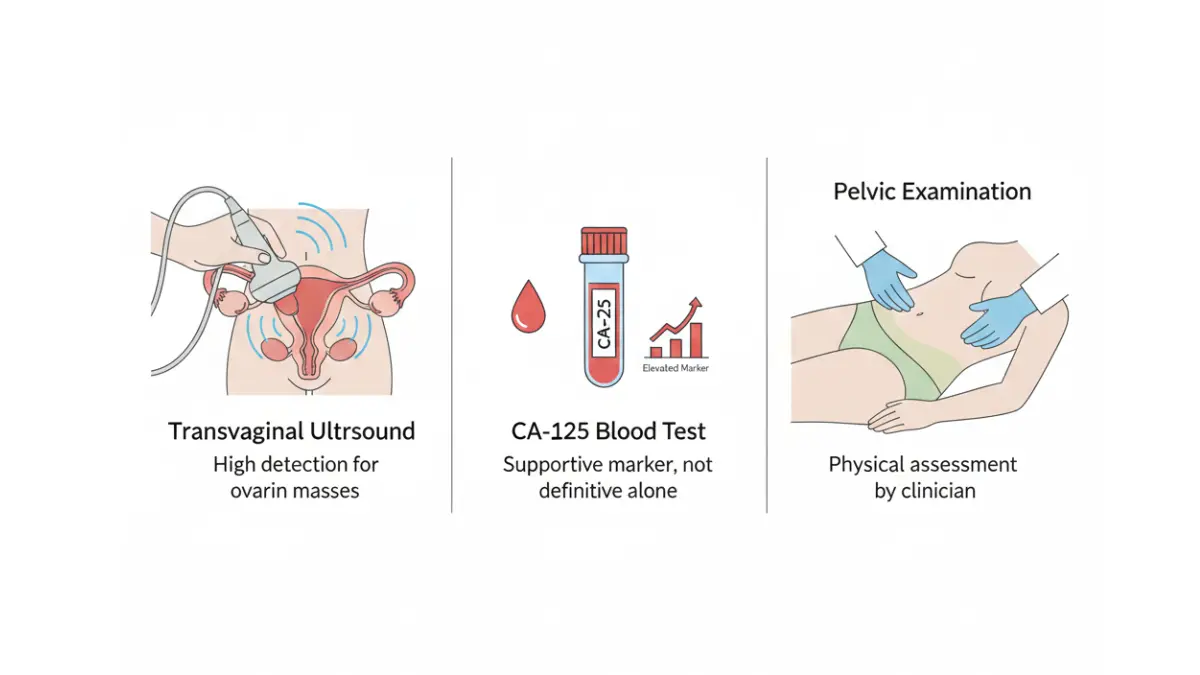
| Transvaginal Ultrasound (TVS) | Ovarian masses, fluid | 85% sensitivity, 98% specificity | $200-$500 |
| CT Scan with Contrast | Tumor size, spread, staging | 85-90% accuracy for advanced disease | $500-$3,000 |
| MRI Pelvis | Detailed soft tissue imaging | 91-93% accuracy | $1,000-$5,000 |
| Biopsy (Ultrasound-Guided) | Definitive histological diagnosis | 94% accuracy | $1,500-$4,000 |
CA-125 Blood Test: The National Cancer Institute notes that CA-125 measures a substance released by cells that may indicate cancer. However, NIH research shows approximately 20% of ovarian cancers produce no CA-125 elevation. Benign conditions like endometriosis, menstruation, and pregnancy also elevate CA-125, creating false positives.
Would a Pap smear detect ovarian cancer? No—Pap smears screen for cervical cancer only and cannot detect ovarian cancer. The National Cancer Institute’s research on PapSEEK testing showed only 33% sensitivity for ovarian cancer detection.
Can ovarian cancer be detected in routine blood work? Not reliably—standard complete blood counts don’t screen for cancer markers. Only specialized tests like CA-125 detect potential ovarian cancer, and physicians must specifically order them.
Transvaginal Ultrasound (TVS): NIH studies demonstrate TVS has 85% sensitivity and 98% specificity for differentiating benign from malignant ovarian masses. This imaging test allows direct visualization of the ovaries and surrounding structures.
CT Scans and Biopsies: Advanced imaging reveals whether cancer has spread beyond the ovaries, while ultrasound-guided tru-cut biopsy provides definitive diagnosis with 94% histological accuracy.
The Self-Advocacy Strategy: What to Say
Many women wait months for diagnosis because physicians initially attribute symptoms to more common conditions. Use this exact script:
“I’m experiencing [specific symptoms] more than 20 times per month for [duration]. These symptoms are NOT normal for me. I need you to rule out ovarian cancer with a transvaginal ultrasound and CA-125 test today.”
If your doctor dismisses your concerns:
- Ask for documentation in your medical record of why testing was denied
- Request a referral to a gynecologist or gynecologic oncologist
- Seek a second opinion within 48-72 hours
- Use health tracking tools to document symptom progression
Diagnostic Timeline: What to Expect
- Week 1: Initial exam, pelvic ultrasound, CA-125 blood test ordered
- Week 2: Results reviewed; if abnormal, CT/MRI imaging scheduled
- Week 3-4: Possible biopsy or referral to gynecologic oncologist
- Week 4-6: Surgical staging if cancer confirmed
Average time from symptom onset to diagnosis ranges from 1.1 to 10 months depending on physician specialty and symptom severity. Women who directly consulted gynecologists received diagnoses 2.2 months faster than those starting with primary care.
For comprehensive health monitoring during this process, utilize our main website resources to track all medical appointments and test results systematically.
Prevention, Treatment Overview & Action Plan
Can You Prevent Ovarian Cancer? Evidence-Based Strategies
While no strategy guarantees prevention, the National Cancer Institute identifies several protective factors that significantly reduce ovarian cancer risk. Women who adopt multiple protective behaviors can lower their lifetime risk by up to 50%, making prevention strategies crucial for high-risk individuals.
Evidence-Backed Prevention Methods
| Prevention Strategy | Risk Reduction | Evidence Strength |
|---|---|---|
| Oral contraceptives (5+ years) | 30-50% reduction | Strong (NCI Level 1) |
| Tubal ligation | 40-50% reduction | Strong (Multiple RCTs) |
| Pregnancy/Childbirth (1+ children) | 10-15% per pregnancy | Strong (Meta-analyses) |
| Breastfeeding (8-10+ months) | 20-30% reduction | Moderate-Strong |
| Risk-reducing salpingo-oophorectomy | 85-96% reduction | Strong for high-risk women |
| Maintaining healthy BMI (<25) | 30% reduction | Moderate |
Oral contraceptives remain the most accessible prevention method—research from the National Cancer Institute demonstrates that women who have ever used birth control pills have 30-50% lower ovarian cancer risk than women who never used them. This protective effect persists for up to 30 years after discontinuing oral contraceptives.
Women considering preventive strategies should track their health metrics using tools like our BMI Calculator and discuss personalized plans with gynecologists. For women with BRCA mutations, risk-reducing surgery provides the strongest protection at 85-96% risk reduction.
Treatment Options: Surgery, Chemotherapy & Targeted Therapy
Primary treatment for ovarian cancer combines surgical debulking with platinum-based chemotherapy. NIH research shows that complete surgical removal of all visible tumors represents the strongest predictor of long-term survival.
Standard chemotherapy regimen: Six cycles of carboplatin plus paclitaxel, administered intravenously every three weeks. Some advanced-stage patients receive neoadjuvant chemotherapy before surgery to shrink tumors.
Targeted therapies include PARP inhibitors for women with BRCA mutations and bevacizumab (anti-angiogenesis drug) for advanced disease. These treatments extend progression-free survival by 40-60% compared to chemotherapy alone.
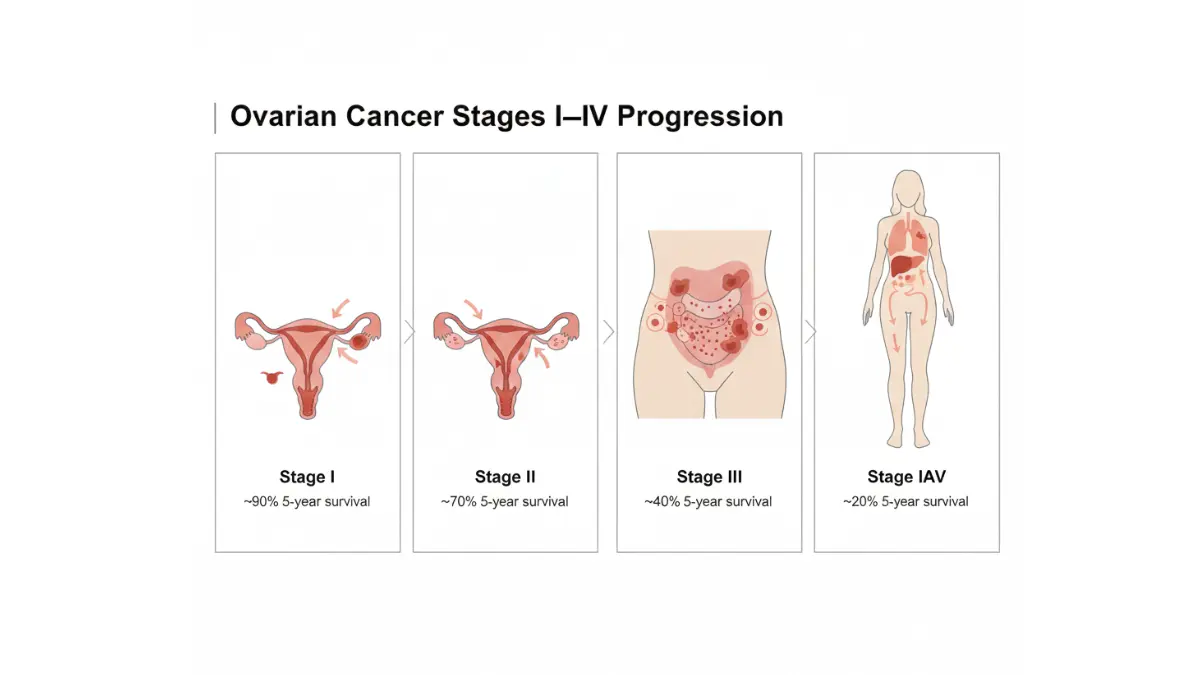
Survival Rates by Stage (SEER Data 2015-2021)
| Stage at Diagnosis | 5-Year Survival Rate | Percentage Diagnosed at This Stage |
|---|---|---|
| Localized (Stage I-II) | 93% | 17% of cases |
| Regional (Stage III) | 75% | 20% of cases |
| Distant (Stage IV) | 31% | 55% of cases |
| All Stages Combined | 50% | 100% |
Source: SEER Cancer Statistics
The dramatic survival difference between localized (93%) and distant-stage (31%) disease underscores why recognizing early signs of ovarian cancer remains absolutely critical.
Your 7-Day Action Plan
If you’re experiencing persistent ovarian cancer symptoms or have risk factors, implement these steps immediately:
Day 1-2: Document & Assess
- Track symptom frequency using our Symptom Checker (document daily for 2 weeks minimum)
- Complete the Genetic Risk Assessment Tool if you have family history
- Calculate your BMI and note any unexplained weight changes
Day 3-4: Schedule & Prepare
4. Call your gynecologist or primary care physician for an appointment within 7-10 days (request urgent slot if symptoms are severe)
5. Write down all ovarian cancer warning signs you’re experiencing with dates and frequency
Day 5-7: Medical Action
6. Attend your appointment with documented symptoms; explicitly request CA-125 blood test and transvaginal ultrasound to “rule out ovarian cancer”
7. If denied testing or symptoms are dismissed, schedule a second opinion with a gynecologic oncologist within 48-72 hours
Women with BRCA mutations should discuss genetic counseling and preventive surgery options between ages 35-45.
Real Patient Success Story
“I caught my stage I ovarian cancer because I trusted my instincts about persistent bloating and pelvic pressure,” shares Lisa Chen, 58, who completed treatment in 2023. “I used online symptom trackers to show my doctor I’d had symptoms 25+ times per month for six weeks. That documentation convinced her to order the ultrasound that saved my life. Two years later, I’m cancer-free.”
Lisa’s story demonstrates the power of early detection ovarian cancer strategies combined with self-advocacy.
Support & Resources
- National Cancer Institute Hotline: 1-800-422-6237 (1-800-4-CANCER)
- Ovarian Cancer Research Alliance (OCRA): Support groups and patient navigation
- FORCE (Facing Our Risk of Cancer Empowered): BRCA mutation support community
- National Ovarian Cancer Coalition: Educational resources and screening information
Explore additional health resources and monitoring tools to maintain comprehensive wellness tracking. For weight management strategies that may reduce ovarian cancer risk, utilize our Weight Loss Calculator as part of a holistic prevention approach.
Remember: Recognizing ovarian cancer symptoms women ignore and acting on them quickly can mean the difference between 93% and 31% five-year survival rates. Trust your body, document your symptoms, and demand thorough evaluation.
Frequently Asked Questions About Ovarian Cancer Symptoms
1. What are the first signs of ovarian cancer?
The earliest signs include persistent bloating (20+ days per month), pelvic or abdominal pain unrelated to menstruation, feeling full quickly after eating, and urgent or frequent urination without infection.
2. Can ovarian cancer be detected early?
3. What does ovarian cancer bloating feel like?
Ovarian cancer bloating feels like constant abdominal swelling that persists daily for weeks, often making clothes feel tight around the waist. Unlike menstrual bloating, it doesn’t come and go with your cycle.
4. Would a Pap smear detect ovarian cancer?
No. Pap smears only screen for cervical cancer and cannot detect ovarian cancer. You need transvaginal ultrasound and CA-125 blood tests to evaluate ovarian abnormalities.
5. How accurate is the CA-125 test?
6. Who is at highest risk for ovarian cancer?
7. Can birth control prevent ovarian cancer?
Yes. Women who use oral contraceptives for 5+ years reduce ovarian cancer risk by 30-50%, with protection lasting up to 30 years after discontinuation.
8. What is the survival rate for ovarian cancer?
Five-year survival rates are: 93% for localized (Stage I-II), 75% for regional (Stage III), and 31% for distant (Stage IV) disease. Overall survival across all stages is 50%.
9. When should I see a doctor about symptoms?
See a doctor immediately if you experience any combination of bloating, pelvic pain, or urinary urgency occurring 20+ times monthly for 2+ weeks, or any vaginal bleeding after menopause.
10. Does ovarian cancer run in families?
11. What causes ovarian cancer?
The exact cause remains unknown, but risk factors include inherited gene mutations (BRCA1/BRCA2, Lynch syndrome), age over 55, obesity, never being pregnant, endometriosis, and hormone replacement therapy.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











