Glioblastoma Survival Rate: 2025 Facts & Treatment
The glioblastoma survival rate remains challenging, with a median survival of 12-15 months following standard treatment. However, groundbreaking 2025 research from Mayo Clinic shows 56% of patients alive at 12 months using advanced protocols, with some patients achieving 22-month survival when favorable genetic markers are present. Stage 4 glioblastoma, the most aggressive malignant brain tumor, affects approximately 24,820 Americans annually.
When 58-year-old Michael learned he had a severe headache that wouldn’t respond to typical pain relievers, he initially dismissed it as stress. Three weeks later, after experiencing sudden vision changes and confusion, an MRI revealed what his neurologist called “a mass consistent with glioblastoma multiforme.” Michael’s world shifted in that moment—he had glioblastoma, the deadliest form of brain cancer.
Within days, Michael underwent maximal surgical resection at a comprehensive cancer treatment center recognized by the National Cancer Institute, followed by radiation and chemotherapy using the standard Stupp protocol. His tumor’s molecular profile showed MGMT promoter methylation—a favorable genetic marker that improved his glioblastoma prognosis significantly. Today, 19 months post-diagnosis, Michael continues treatment while maintaining quality time with his grandchildren. He monitors his overall health using tools like the BMI Calculator to track nutritional status during therapy, understanding that each patient’s glioblastoma life expectancy varies based on multiple biological and treatment factors.
Understanding the Numbers
| Survival Metric | 2025 Data | Evidence Source |
|---|---|---|
| Median overall survival (standard treatment) | 12-15 months | National Cancer Institute |
| 2025 Mayo Clinic advanced protocol | 13.1 months median, 56% alive at 12 months | Mayo Clinic Phase 2 trial |
| Favorable genetics (MGMT+) | Up to 22 months median | Recent clinical data |
| 2-year survival rate | 17.8%-30% | Population studies |
| 5-year survival rate | <10% (approximately 6.5%) | SEER database |
| Brain tumor survival rate (all types) | 33.0% at 5 years | SEER Cancer Statistics 2015-2021 |
What This Means For You: While these statistics represent population averages, your individual glioblastoma survival rate depends on critical factors including age at diagnosis, tumor molecular markers (particularly MGMT methylation status and IDH mutation), extent of surgical resection, and response to chemoradiation. Patients under 50 with MGMT-methylated tumors who receive complete resection followed by standard chemoradiotherapy show significantly better outcomes than average statistics suggest. The brain cancer survival rate for glioblastoma specifically remains lower than the overall 33% five-year rate for all brain and nervous system tumors, making personalized treatment planning and molecular testing essential steps after diagnosis. Use our Symptom Checker if you’re experiencing persistent neurological changes that concern you.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Glioblastoma diagnosis and treatment require individualized care from board-certified neuro-oncologists and neurosurgeons. Always consult your healthcare team before making treatment decisions.
Understanding Glioblastoma – Definition, Stages & Causes
What Is Glioblastoma? Understanding the Deadliest Brain Cancer
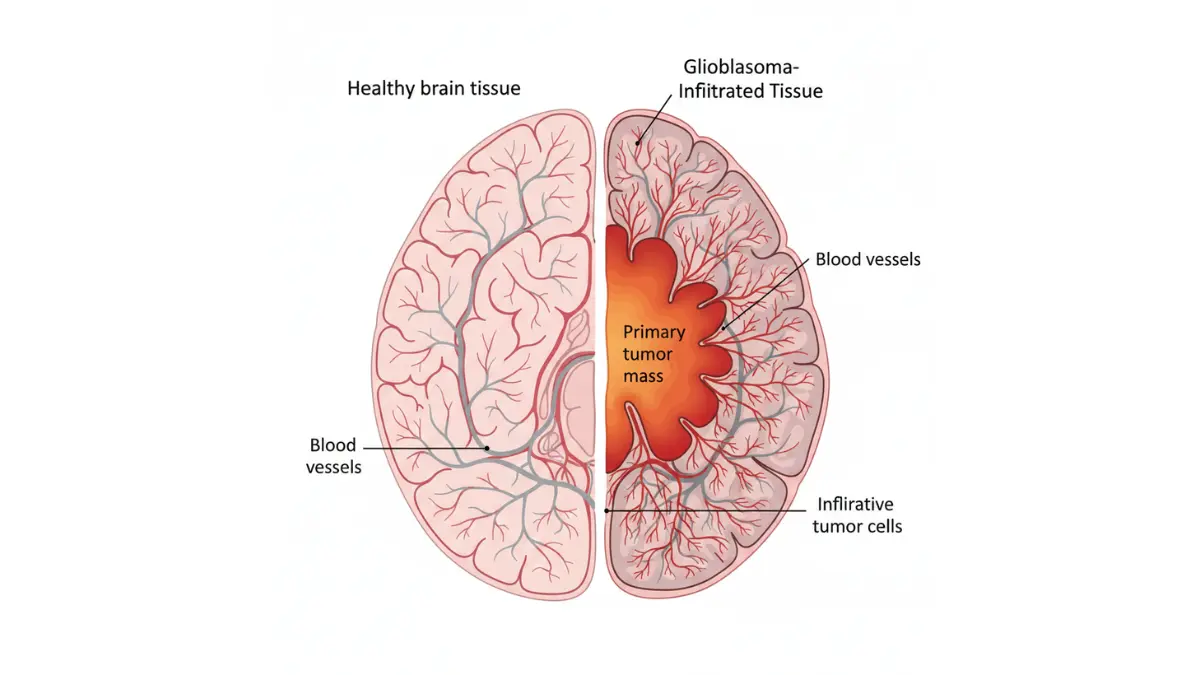
Glioblastoma multiforme represents the most aggressive and lethal form of primary brain cancer, classified by the World Health Organization as a Grade IV astrocytoma. This glioblastoma cancer originates from astrocytes—star-shaped support cells in the brain—and infiltrates surrounding brain tissue with remarkable speed and invasiveness. What is glioblastoma’s defining characteristic? Unlike benign brain tumors that grow in defined boundaries, this malignant brain tumor sends microscopic finger-like projections throughout brain tissue, making complete surgical removal virtually impossible.
The term “multiforme” in glioblastoma multiforme refers to the tumor’s highly varied cellular appearance under microscopic examination. Glioblastoma brain tumor cells display extreme heterogeneity, with different cells within the same tumor showing distinct genetic profiles and growth patterns. This cellular diversity contributes to treatment resistance, as therapies targeting one cell population may leave others unaffected. Understanding what is glioblastoma at the molecular level has become critical for developing targeted treatment approaches, which is why patients should consider using resources like the Genetic Risk Assessment Tool after diagnosis.
Key differences between glioblastoma and other gliomas include:
- Rapid growth rate: Glioblastoma brain tumor cells divide aggressively, doubling in size approximately every 17-62 days
- Necrosis presence: Dead tissue zones within the tumor, a hallmark feature distinguishing glioblastoma from lower-grade astrocytomas
- Microvascular proliferation: Abnormal blood vessel formation feeding tumor growth
- Blood-brain barrier disruption: Allows the National Cancer Institute-funded research to identify how glioblastoma cancer cells breach protective brain barriers
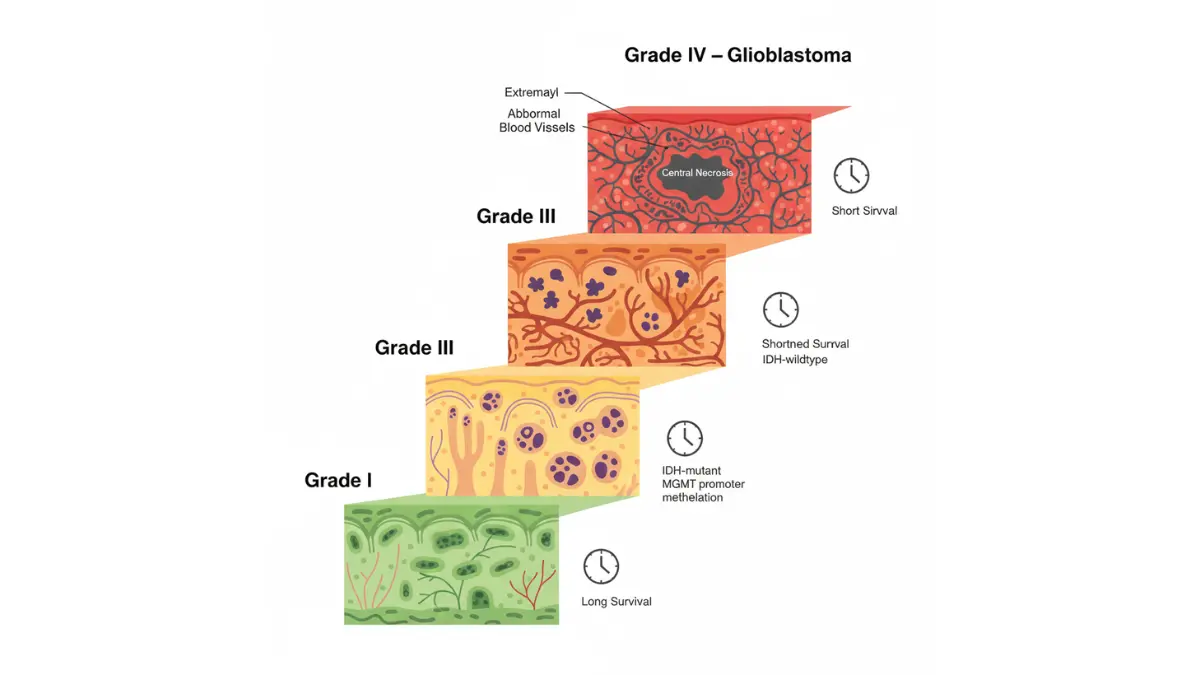
Glioblastoma Stages and Classification
The 2021 WHO Classification revolutionized how we categorize glioblastoma stages through molecular characteristics rather than appearance alone. Modern glioblastoma classification now prioritizes genetic markers that determine prognosis and treatment response over traditional microscopic features.
IDH-wildtype vs IDH-mutant glioblastoma stages represent fundamentally different diseases:
MGMT (O-6-methylguanine-DNA methyltransferase) promoter methylation status has emerged as the single most important biomarker in glioblastoma prognosis. When this DNA repair gene’s promoter is methylated (silenced), tumor cells cannot efficiently repair damage from chemotherapy, resulting in significantly improved treatment response. Approximately 40-45% of patients have MGMT-methylated tumors, translating to hazard ratios as low as 0.58 for mortality risk.
Additional molecular glioblastoma stages markers include:
- TERT promoter mutations: Present in 70-80% of IDH-wildtype glioblastoma, indicates aggressive biology
- EGFR amplification: Found in 40-50% of cases, associated with treatment resistance
- Chromosome 7 gain/Chromosome 10 loss (+7/-10): Classic signature of glioblastoma cancer
These molecular distinctions explain why two patients with identical-appearing tumors under the microscope may experience vastly different survival outcomes, making genetic testing through specialized health assessment tools increasingly standard practice.
Glioblastoma Causes and Risk Factors
The glioblastoma causes remain largely unknown, with approximately 80% of cases developing spontaneously without identifiable triggers. Unlike many cancers linked to lifestyle or environmental exposures, what is glioblastoma’s etiology continues to puzzle researchers despite decades of investigation.
Established glioblastoma causes include:
- Ionizing radiation exposure: The only definitively proven environmental risk factor, including prior therapeutic radiation for other cancers
- Rare inherited genetic syndromes: Li-Fraumeni syndrome (TP53 mutations), neurofibromatosis type 1, and Lynch syndrome account for fewer than 5% of cases
Factors NOT proven as glioblastoma causes despite extensive study:
Cell phone use, electromagnetic fields, dietary factors, and occupational exposures (except specific chemical solvents like carbon tetrachloride in high-exposure occupations). The CDC-supported Honolulu Heart Program study found no association with common lifestyle factors but identified dietary sugar intake as a potential area for further investigation.
Age and demographic patterns reveal:
- Peak incidence occurs between ages 55-60 years
- Men develop glioblastoma brain tumor at 1.6 times the rate of women
- Slightly higher rates in Caucasian populations compared to other ethnic groups
Early Warning Signs
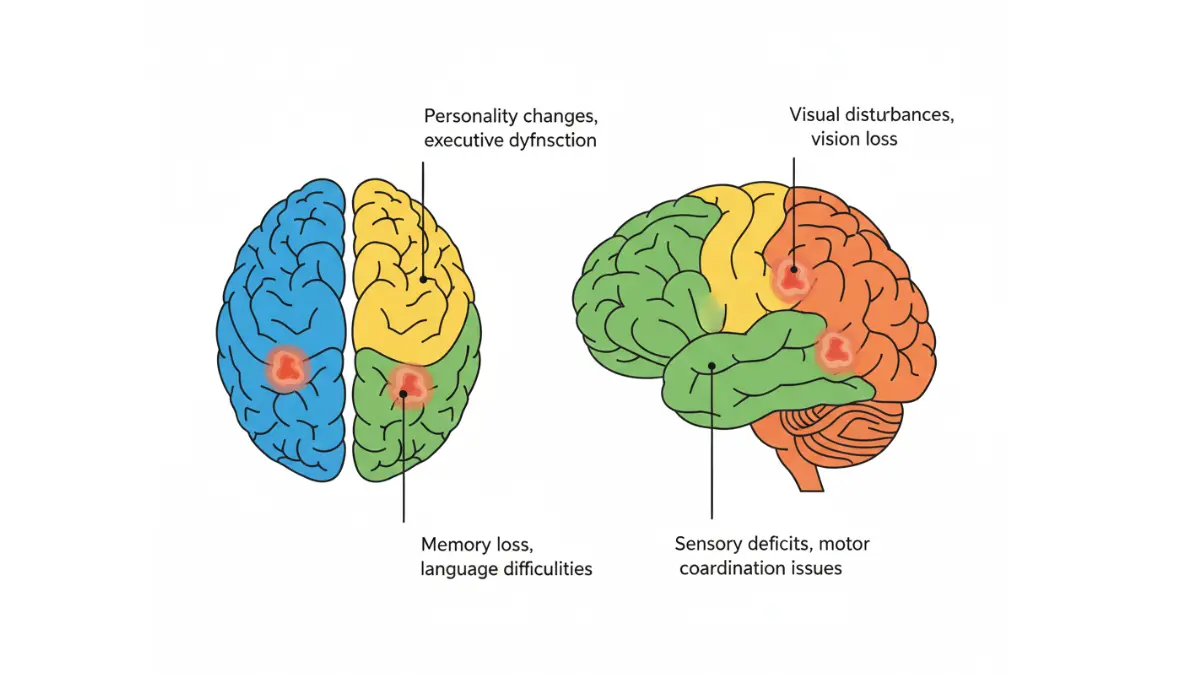
Glioblastoma symptoms typically develop rapidly over 3-6 months as the tumor grows and increases pressure within the skull. Because symptoms depend on tumor location, two patients may present with completely different warning signs.
Most common glioblastoma symptoms include:
- New-onset severe headaches (30-50% of patients) – especially headaches that worsen with lying down or upon waking
- Seizures (20-40% of initial presentations) – often the first symptom, even in patients with no seizure history
- Progressive neurological deficits – weakness, numbness, or coordination problems on one body side
- Cognitive and personality changes – memory problems, confusion, or behavioral shifts that family members notice first
- Vision problems – blurred vision, double vision, or visual field loss
- Speech difficulties – trouble finding words or understanding language
If you’re experiencing persistent neurological symptoms, use the Symptom Checker to document your symptoms before consulting a neurologist. Maintaining overall health through proper nutrition using tools like the BMI Calculator may support resilience during diagnosis and treatment planning.
2025 Survival Statistics – Deep Dive with Age & Molecular Factors
Glioblastoma Life Expectancy: 2025 Survival Data Breakdown
Median Survival Rates by Treatment Type
Glioblastoma survival rate outcomes in 2025 show meaningful improvements over historical data, with treatment selection and molecular profiling driving personalized survival expectations. The standard Stupp protocol—maximal safe surgical resection followed by concurrent radiation with temozolomide plus six months of adjuvant chemotherapy—produces a median survival of 12-15 months for most patients. However, pioneering work at Mayo Clinic in 2025 using hypofractionated stereotactic radiation achieved a 13.1-month median survival with 56% of patients alive at 12 months.
When comparing glioblastoma treatment options, extent of surgical resection dramatically affects glioblastoma prognosis: patients undergoing gross total resection achieve 12.9-month median survival compared to only 4.6 months for biopsy alone. The addition of tumor-treating fields (TTFields/Optune device) to standard chemoradiotherapy extends median survival to approximately 20.9 months in eligible patients. According to SEER Cancer Statistics data tracking brain tumor survival rate across populations, two-year survival improved from 15% in 2000-2001 to 26% by 2005-2006 following widespread adoption of temozolomide.
Patients seeking to track their overall wellness during treatment can utilize tools like the Body Fat Calculator to monitor nutritional status, as maintaining healthy body composition correlates with better treatment tolerance. For those enrolled in clinical trials, visit ClinicalTrials.gov to explore cutting-edge protocols that may extend glioblastoma life expectancy beyond current standards.
How Long Can You Live With Glioblastoma? Age Matters
Age remains one of the most powerful predictors of glioblastoma survival rate, with younger patients achieving dramatically longer survival than elderly patients receiving identical treatment. Analysis of SEER population-based cancer registries reveals striking age-related disparities in glioblastoma prognosis.
Age-stratified glioblastoma life expectancy data:
- Ages 18-44: Median survival 28 months, with some patients achieving 5+ year survival
- Ages 45-54: Median survival approximately 18-20 months
- Ages 55-64: Median survival 13.4 months
- Ages 65-74: Median survival 9-10 months
- Ages 75+: Median survival 7.3 months or less
The 30-day mortality rate following diagnosis stands at 5.1% overall, reflecting both tumor aggressiveness and surgical complications. How long can you live with glioblastoma after diagnosis depends critically on performance status at presentation: patients with excellent functional status (Karnofsky Performance Score ≥70) survive nearly twice as long as those with poor baseline function. Maintaining physical fitness through monitored activity—tracking metrics with tools like the Heart Rate Zone Calculator—may help preserve functional capacity during treatment.
Brain cancer survival rate trends from 2000-2021 show gradual improvement: the hazard ratio for death decreased from 1.0 in 2000-2001 to 0.648 in 2005-2006 following temozolomide adoption, representing a 35% mortality reduction for newly diagnosed patients. Despite these gains, the five-year survival rate for glioblastoma specifically remains below 10%, compared to 33% for all brain and nervous system tumors combined.
Evidence Confidence Level: High (based on population registries tracking 26% of U.S. cancer cases over two decades)
Molecular Markers That Predict Glioblastoma Prognosis
MGMT (O-6-methylguanine-DNA methyltransferase) promoter methylation status has emerged as the single most powerful molecular predictor of glioblastoma prognosis and treatment response. This epigenetic modification silences the MGMT DNA repair gene, preventing tumor cells from fixing damage caused by alkylating chemotherapy like temozolomide.
According to Thomas Jefferson University neuro-oncology research published in 2025, patients with MGMT-methylated tumors achieve median overall survival of 24.59 months with median progression-free survival of 9.51 months. In stark contrast, patients with unmethylated MGMT tumors have median survival of only 14.11 months with progression-free survival of 4.99 months. This represents a 40% reduction in mortality risk (hazard ratio 0.58) when MGMT methylation is present.
Key molecular biomarkers affecting glioblastoma survival rate:
- MGMT methylation: 40-45% of patients; associated with 10+ month survival advantage
- IDH mutation status: IDH-mutant tumors (rare in primary glioblastoma) show 28+ month median survival vs 12-15 months for IDH-wildtype
- TERT promoter mutations: Present in 70-80% of aggressive IDH-wildtype glioblastoma
- EGFR amplification: Found in 40-50% of cases; linked to treatment resistance
Genetic testing has become standard practice at comprehensive cancer centers, with National Cancer Institute genomic databases cataloging molecular profiles from thousands of glioblastoma brain tumor samples. Patients should request MGMT testing specifically, as this single biomarker determines whether aggressive temozolomide dosing is warranted. The Genetic Risk Assessment Tool can help patients prepare questions about hereditary cancer syndromes prior to genetic counseling consultations.
What This Means For You: Request comprehensive molecular profiling including MGMT methylation status, IDH mutation testing, and 1p/19q codeletion analysis at diagnosis. If your tumor shows MGMT methylation, you have significantly better odds of responding to standard chemotherapy. Unmethylated tumors may benefit from clinical trials exploring alternative therapies rather than standard temozolomide-based regimens.
Brain Cancer Survival Rate Trends
The brain cancer survival rate for glioblastoma specifically has shown modest but meaningful improvement over the past two decades, driven primarily by standardized adoption of concurrent chemoradiotherapy. Population-level data from SEER registries tracking long-term survival outcomes document three-year survival increasing from 8.0% to 10.5% between 2004-2013.
Malignant brain tumor survival improvements reflect multiple advances:
Contemporary glioblastoma survival rate benchmarks from 2020-2025 show median survival stabilizing at 15 months for patients receiving guideline-concordant care. The 2025 outlook appears cautiously optimistic, with immunotherapy trials, CAR-T cell therapies, and personalized vaccine approaches entering late-stage testing. Recent MIT research identifying new immunotherapeutic targets published December 2025 suggests future treatments may overcome glioblastoma’s notorious immune evasion mechanisms.
Global variations in glioblastoma prognosis exist, with developed nations achieving 12-15 month median survival compared to 6-9 months in resource-limited settings lacking access to radiation therapy and temozolomide. Regional survival disparities within the United States also persist, with patients treated at high-volume academic centers showing superior outcomes compared to community hospitals.
What This Means For You: Seek treatment at neuro-oncology centers performing high volumes of glioblastoma surgeries (50+ cases annually) with dedicated tumor boards reviewing molecular pathology. Request MGMT testing within one week of diagnosis to avoid treatment delays. Consider clinical trial enrollment early—trials typically achieve superior survival compared to standard care due to intensive monitoring and access to promising experimental agents. Use the Sleep Calculator to optimize recovery periods between treatment cycles, as adequate rest supports immune function during therapy.
Comprehensive Treatment Options – 2025 Standards
Glioblastoma Treatment: Evidence-Based Options for 2025
Standard Glioblastoma Treatment Protocol
The foundation of glioblastoma treatment remains the Stupp protocol—maximal safe surgical resection followed by concurrent radiation therapy with temozolomide chemotherapy, established as the standard of care since 2005. This multimodal approach begins with neurosurgical debulking to remove as much visible tumor as safely possible without causing permanent neurological deficits. The FDA-approved treatment pathway for newly diagnosed glioblastoma multiforme mandates completion of radiation therapy (typically 60 Gy delivered over 6 weeks) together with concomitant daily temozolomide at 75 mg/m².
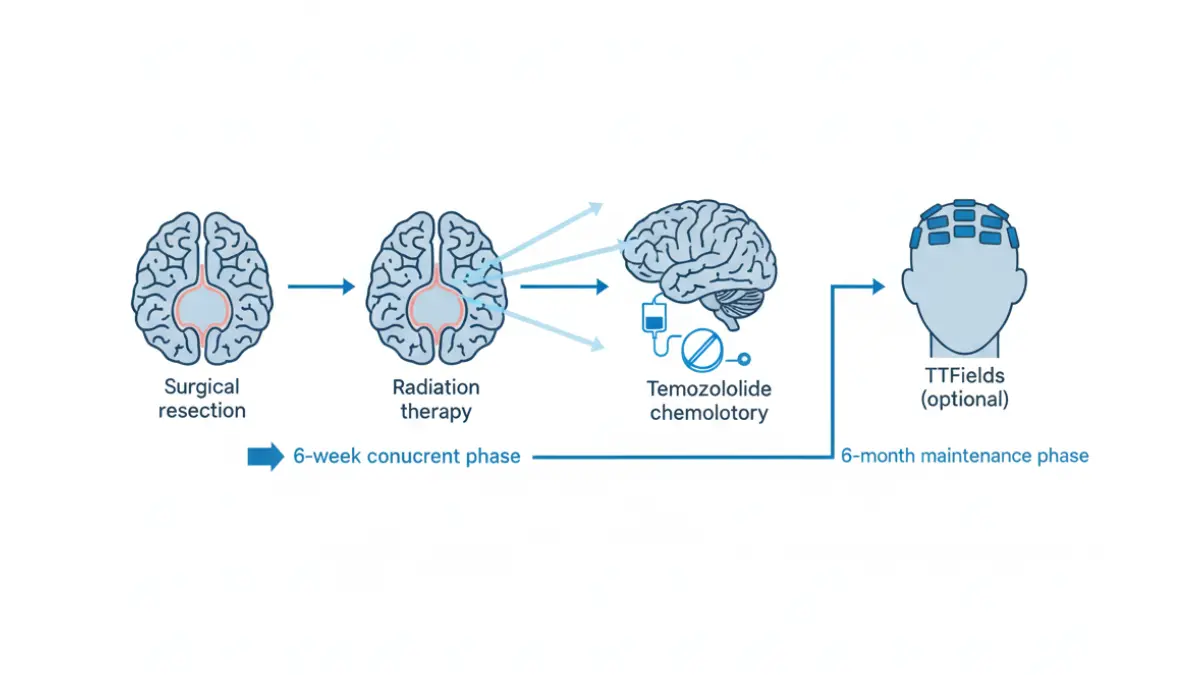
Following the 6-week chemoradiotherapy phase, patients receive maintenance temozolomide for six cycles at 150-200 mg/m² for five days every 28 days. NCCN guidelines stratify glioblastoma treatment options based on age, performance status (Karnofsky Performance Score), and critically, MGMT methylation status. For patients aged 70 or younger with KPS ≥60, concurrent chemoradiotherapy followed by adjuvant temozolomide represents the preferred regimen regardless of MGMT status. However, elderly patients (>70 years) with unmethylated MGMT tumors may receive hypofractionated radiation alone (40 Gy in 15 fractions), while those with methylated tumors benefit more from temozolomide-based therapy.
Maintaining nutritional status during intensive glioblastoma treatment correlates with better tolerance of therapy—patients can track their body composition using the Body Fat Calculator and optimize protein intake with the Protein Intake Calculator to preserve muscle mass during treatment. Adequate caloric intake calculated through the Calorie Deficit Calculator helps prevent cachexia, which independently predicts poorer glioblastoma prognosis.
Glioblastoma Treatment Options Beyond Standard Care
Tumor-treating fields (TTFields), marketed as the Optune device, received FDA approval in October 2015 for newly diagnosed glioblastoma after demonstrating significant survival improvement when added to maintenance temozolomide. This wearable device delivers alternating electric fields at 200 kHz frequency through transducer arrays placed on the shaved scalp, disrupting cancer cell division during mitosis without affecting non-dividing normal brain cells. The pivotal phase III trial showed patients receiving Optune plus temozolomide achieved 20.9-month median overall survival compared to 16.0 months with temozolomide alone—a 4.9-month survival advantage.
Stage 4 glioblastoma treatment landscape in 2025 includes several evidence-based additions:
- Bevacizumab (Avastin): Anti-VEGF antibody approved for recurrent glioblastoma cancer, extends progression-free survival but not overall survival
- Hypofractionated stereotactic radiation: Mayo Clinic’s 2025 protocol delivering 35 Gy in 10 fractions achieved 13.1-month median survival with reduced treatment burden
- Immunotherapy approaches: Checkpoint inhibitors (nivolumab, pembrolizumab) showing modest activity in selected patients
- CAR-T cell therapy: Harvard Medical School researchers developed CAR-TEAM cells targeting dual EGFR markers, with first-in-human trials showing dramatic but transient tumor reductions
According to ClinicalTrials.gov registry data, over 300 active trials are testing novel glioblastoma treatment approaches including personalized vaccines, oncolytic viruses, and combination immunotherapies. The University of Florida Cancer Center initiated CAR-T trials for pediatric high-grade gliomas in 2025, with adult glioblastoma trials also enrolling.
Pros and cons of advanced glioblastoma treatment options:
- TTFields/Optune:
- Bevacizumab:
- CAR-T immunotherapy:
Stage 4 Glioblastoma Treatment Realities
Why stage 4 glioblastoma remains incurable despite aggressive treatment relates to fundamental biological challenges: the tumor’s diffuse infiltration pattern means microscopic glioblastoma cancer cells invariably remain beyond surgical margins and radiation fields. The blood-brain barrier that protects healthy brain tissue also prevents most systemic chemotherapies from reaching therapeutic concentrations at tumor sites. Additionally, glioblastoma multiforme exhibits profound intra-tumoral heterogeneity, with individual cells within the same tumor harboring different genetic mutations and resistance mechanisms.
Treatment trade-offs for stage 4 glioblastoma patients involve balancing survival extension against quality of life preservation: aggressive multimodal therapy extends median survival from 4-6 months (supportive care alone) to 12-15 months (standard protocol). However, intensive treatment carries significant side effects including fatigue, cognitive decline, bone marrow suppression, and infection risks. Elderly patients or those with poor performance status often experience greater treatment toxicity with diminished survival benefit.
What This Means For You: Request a comprehensive tumor board review within two weeks of diagnosis to ensure your treatment plan incorporates the latest evidence. Ask your neuro-oncologist these specific questions:
- “Am I a candidate for TTFields/Optune based on my insurance coverage and lifestyle?”
- “Should we consider hypofractionated radiation given my age and performance status?”
- “Are there clinical trials I qualify for that might offer survival advantages over standard care?”
- “How do we balance aggressive treatment against maintaining quality time with my family?”
Experimental and Emerging Therapies
Cutting-edge glioblastoma treatment options entering clinical testing in 2025 include several promising modalities that may eventually supplement standard protocols. Laser interstitial thermal therapy (LITT) uses MRI-guided laser probes to ablate recurrent tumors in locations unsuitable for repeat surgery, offering local control with minimal invasiveness. Convection-enhanced delivery systems bypass the blood-brain barrier by infusing chemotherapy or immunotherapy directly into tumor tissue via surgically implanted catheters.
MIT researchers announced in December 2025 the identification of novel immunotherapeutic targets that may overcome glioblastoma’s notorious immune evasion mechanisms. These discoveries could enable next-generation immunotherapies to recognize and eliminate glioblastoma brain tumor cells that currently hide from immune surveillance. Oncolytic virus therapies, which selectively infect and destroy cancer cells while stimulating anti-tumor immunity, are advancing through phase II trials with encouraging preliminary results.
Accessing experimental glioblastoma treatment requires enrollment in clinical trials: visit ClinicalTrials.gov to search by location, eligibility criteria, and treatment type. Major academic medical centers conducting high-volume glioblastoma research typically offer the broadest trial access. Patients should undergo molecular profiling through the Genetic Risk Assessment Tool consultation to identify trials matching their tumor’s specific genetic alterations.
Integrative Support During Treatment
Lifestyle modifications that support glioblastoma treatment outcomes include evidence-based interventions that patients can implement alongside medical therapy. Adequate protein intake (1.2-1.5 g/kg body weight daily) helps preserve muscle mass during catabolic cancer treatment—calculate personalized needs using the Protein Intake Calculator. Proper hydration calculated through the Water Intake Calculator supports kidney function during chemotherapy and helps manage treatment side effects.
Sleep optimization using the Sleep Calculator may enhance immune function and treatment response, as circadian rhythm disruption independently predicts poorer cancer outcomes. Moderate physical activity tailored to performance status—monitored with the Heart Rate Zone Calculator—has shown associations with improved survival in multiple cancer types, though glioblastoma-specific data remains limited. Explore additional wellness strategies through our comprehensive Health Tips resource library.
Living With Glioblastoma – Quality of Life & Patient Guidance
Beyond Survival Statistics: Quality of Life With Glioblastoma
Managing Glioblastoma Symptoms Throughout Treatment
Glioblastoma symptoms evolve throughout the disease trajectory, requiring proactive medical management to maintain quality of life and functional independence. Seizures affect 30-50% of patients at some point during their illness, with 20-40% experiencing seizures as their initial presentation. According to Harvard Medical School and Dana-Farber Cancer Institute neuro-oncology guidelines, levetiracetam has emerged as the preferred antiepileptic drug for glioblastoma brain tumor patients due to its lack of drug interactions with chemotherapy, no requirement for blood level monitoring, and excellent tolerability profile.
Dexamethasone remains the cornerstone of managing vasogenic edema and associated neurological symptoms including headaches, focal deficits, and cognitive changes. Research published in the National Institutes of Health database demonstrates that dexamethasone administration significantly reduces headaches, vomiting, seizures, and focal neurological deficits in glioblastoma cancer patients. However, prolonged steroid use beyond 2-3 weeks at doses of 16 mg daily or higher produces frequent side effects including myopathy (weakness), mood disorders, hyperglycemia, and infections. Only 29% of high-grade glioma patients successfully taper off steroids three months post-radiation, highlighting the challenge of steroid dependency.
Key symptom management strategies for glioblastoma life expectancy optimization:
- Seizure control: Levetiracetam or lacosamide preferred over older enzyme-inducing anticonvulsants that interact with chemotherapy
- Steroid management: Start at lowest effective dose (4-8 mg dexamethasone daily for mild symptoms); taper aggressively when possible
- Fatigue mitigation: Monitor with the Sleep Calculator and maintain activity within tolerance using the Heart Rate Zone Calculator
- Cognitive preservation: Neuropsychological testing and occupational therapy for daily function maintenance
- Thrombosis prevention: 17-20% of patients develop venous thromboembolism within one year, requiring prophylaxis consideration
Maintaining nutritional status through calculated intake using the Protein Intake Calculator and Water Intake Calculator supports treatment tolerance. Use the Symptom Checker to document new or worsening symptoms between appointments.
Caregiver and Family Support
The emotional and physical burden on family caregivers of glioblastoma patients ranks among the highest in oncology, with caregiving responsibilities extending far beyond medication management to include coordination of complex medical care, emotional support, household management, and advocacy. According to Duke University’s Preston Robert Tisch Brain Tumor Center, caregivers must simultaneously track appointments, manage treatments, monitor symptoms, provide emotional reassurance, and help patients cope with personality and cognitive changes.
Caregiver burnout prevention requires:
- Building support networks: Connecting with other families through hospital support groups or online communities
- Respite care utilization: Taking breaks while professionals provide temporary care relief
- Professional counseling access: Addressing caregiver depression, anxiety, and anticipatory grief
- Advance care planning: Early discussions about goals of care, living wills, and healthcare proxies
The University of California San Francisco Caregiver Handbook emphasizes recognizing signs of patient depression and ensuring adequate mental health support alongside medical treatment. Explore additional wellness resources through our Health Tips library for both patients and caregivers.
Financial and Insurance Navigation
The economic burden of glioblastoma treatment remains substantial, with Medicare data showing average cumulative costs of $98,710 per patient, of which 58% occurs in the inpatient setting. According to National Institutes of Health analysis of SEER-Medicare data, patients receiving first-line systemic therapy incur mean costs of $124,138, with surgical resection alone averaging $5,527 and monthly tumor-treating fields (Optune) therapy approaching $20,000.
Financial considerations for glioblastoma cancer patients include:
- Treatment costs: Standard chemoradiotherapy ranges $79,000-$139,000 for six months post-surgery; costs increase substantially with each subsequent treatment line
- Supportive care expenses: 93% of patients require physical therapy, 84% occupational therapy, 72% speech therapy, and 72% enter hospice care
- Hospitalization burden: Most patients (98%) experience at least one hospitalization, with 86% requiring ICU admission
- Clinical trial coverage: Experimental treatments may have costs covered by trial sponsors; verify with ClinicalTrials.gov study coordinators
Insurance authorization for TTFields/Optune requires documentation of Karnofsky Performance Score ≥70 and completion of standard chemoradiotherapy. Medicare coverage for advanced imaging (MRI scans averaging 0.54 per month) and supportive medications (steroids, anticonvulsants) generally proceeds without prior authorization, though bevacizumab often requires step therapy documentation.
When to Seek Second Opinions
Second opinion consultation at high-volume academic neuro-oncology centers becomes particularly valuable when molecular tumor profiling reveals uncommon variants or when initial treatment fails. Major medical centers performing 50+ glioblastoma surgeries annually achieve superior survival outcomes compared to low-volume community hospitals, justifying referral consideration even after initial diagnosis.
Seek specialized consultation for:
- Unusual molecular profiles: IDH-mutant glioblastoma, BRAF mutations, or high tumor mutational burden that might qualify for novel therapies
- Rapid progression: Disease advancing within 3 months of completing standard chemoradiotherapy
- Young age: Patients under 50 may benefit from aggressive experimental approaches unavailable locally
- Treatment complications: Severe toxicity limiting standard therapy completion
Multidisciplinary tumor board review brings together neurosurgeons, neuro-oncologists, radiation oncologists, neuroradiologists, and molecular pathologists to collectively determine optimal treatment strategies. Request copies of your complete medical records including pathology reports, molecular testing results, and all imaging studies before second opinion appointments.
What This Means For You: Quality glioblastoma prognosis depends not just on tumor biology but also on comprehensive symptom management and support systems. Schedule regular check-ins with your care team about medication side effects, emerging symptoms, and caregiver needs. Consider palliative care consultation early in the disease course—studies show earlier palliative involvement improves quality of life without shortening survival. Use the BMI Calculator to monitor nutritional status monthly, as unintentional weight loss predicts poorer outcomes and warrants nutritional intervention.
Future Outlook & Patient Empowerment
The Future of Glioblastoma Survival Rates
Promising Research Directions
The glioblastoma survival rate landscape is poised for transformation through 2025-2030, with over 300 active clinical trials testing novel approaches listed on the National Cancer Institute’s treatment trial registry. Personalized dendritic cell vaccines represent one of the most promising immunotherapy breakthroughs: UCLA’s DCVax-L phase III trial achieved 23.1-month median survival, with nearly 30% of glioblastoma cancer patients surviving three or more years—dramatically surpassing the typical 15-17 month expectancy. Dr. Linda Liau’s research team at UCLA Jonsson Comprehensive Cancer Center demonstrated that this personalized vaccine, which uses each patient’s own tumor tissue combined with activated dendritic immune cells, creates durable anti-tumor immunity in a subset of exceptional responders.
CAR-T cell immunotherapy advances show dramatic initial responses in glioblastoma brain tumor patients, though durability remains a challenge. Stanford Medicine researchers achieved complete tumor disappearance in one pediatric patient with diffuse intrinsic pontine glioma using CAR-T therapy, while three others experienced 52-91% tumor shrinkage. The Cancer Moonshot Immuno-Oncology Translational Network coordinates collaborative efforts across 33 institutions to accelerate translation of immunotherapy discoveries from laboratory to clinical practice. This national initiative, established to achieve “a decade’s worth of progress in 5 years,” focuses specifically on defeating immunosuppressive tumor microenvironments that currently limit glioblastoma treatment effectiveness.
Additional cutting-edge approaches entering trials include:
- Dual immune checkpoint blockade: Combining ipilimumab with nivolumab for MGMT-unmethylated glioblastoma multiforme shows early promise
- IDH-mutant targeted vaccines: Peptide vaccines targeting IDH1 R132H mutations in precision medicine trials
- EGFR-targeted CAR-TEAM cells: Harvard researchers’ dual-targeting approach demonstrated transient but dramatic tumor reductions
- Laser interstitial thermal therapy combined with antiretrovirals: NCI-sponsored trials testing novel combinations for unresectable tumors
Patients can explore participation through ClinicalTrials.gov advanced search, filtering by location, age, and molecular biomarkers. Use the Genetic Risk Assessment Tool to understand which trials match your tumor’s specific genetic profile.
Empowering Patient Decisions
Understanding your glioblastoma prognosis requires active engagement with your pathology report and molecular test results. Request written copies of all diagnostic documents including MGMT methylation status, IDH mutation testing, chromosome 1p/19q codeletion analysis, EGFR amplification status, and TERT promoter mutation results within one week of diagnosis. These molecular markers fundamentally determine treatment strategy and inform realistic survival expectations based on population data rather than averages that may not apply to your specific tumor biology.
Key decisions requiring informed patient participation include:
- Aggressive treatment vs quality time trade-offs: Elderly patients with poor performance status may choose abbreviated radiation over full 6-week courses
- Clinical trial enrollment timing: Many trials require enrollment before starting standard treatment, making early research essential
- Extent of surgical resection: Balancing maximal tumor removal against neurological function preservation
- Participating in tissue banking: Contributing to research registries accelerates future discoveries without personal benefit
Maintaining overall health through proper nutrition using the Calorie Deficit Calculator and Macro Calculator may optimize treatment tolerance. The Pill Identifier helps track complex medication regimens that typically include chemotherapy, anticonvulsants, steroids, and supportive medications.
Hope Grounded in Reality
Long-term survivors of glioblastoma multiforme do exist, offering genuine hope while acknowledging the disease’s aggressive nature. UCLA’s vaccine trial documented 32.6% of participants still alive at analysis, with some exceeding five years from diagnosis—outcomes previously considered virtually impossible. These exceptional responders typically share favorable molecular profiles (MGMT-methylated, younger age, excellent performance status) combined with aggressive multimodal treatment and often participation in clinical trials.
Glioblastoma life expectancy continues improving incrementally rather than through revolutionary breakthroughs: the three-year survival rate increased from 8.0% to 10.5% between 2004-2013. The 2025 Mayo Clinic hypofractionated protocol extending median survival to 22 months in favorable-genetics patients represents meaningful progress. Each patient’s journey remains unique, with individual biology, treatment response, and support systems determining outcomes more accurately than population statistics predict.
Balancing optimism with pragmatism means:
- Recognizing that median survival statistics represent averages—half of patients exceed these timeframes
- Understanding that quality of life preservation may take precedence over survival extension at certain disease stages
- Appreciating incremental advances while maintaining realistic expectations about cure likelihood
Explore additional wellness resources and health optimization strategies through our comprehensive Health Tips library and utilize tools like the BMR Calculator to understand metabolic needs during treatment.
Medical Disclaimer
This article is for educational purposes only and does not constitute medical advice. Glioblastoma diagnosis and treatment require individualized care from board-certified neuro-oncologists, neurosurgeons, and radiation oncologists practicing at experienced medical centers. Statistics presented represent population averages from clinical trials and registries; individual outcomes vary substantially based on molecular tumor characteristics, age, performance status, treatment received, and biological factors not fully understood. Always consult your healthcare team before making treatment decisions.
The information provided does not replace professional medical consultation, diagnosis, or treatment recommendations. If you experience symptoms of brain tumors—including new-onset severe headaches, seizures, progressive neurological deficits, or personality changes—seek immediate medical evaluation. Clinical trial eligibility and suitability should be discussed with qualified oncologists familiar with your complete medical history.
Frequently Asked Questions About Glioblastoma Survival Rate
1. What is the survival rate for glioblastoma?
The median glioblastoma survival rate is 12-15 months with standard treatment. The 2-year survival rate is approximately 17.8%-30%, while the 5-year survival rate remains below 10% (around 6.5%). However, 2025 advanced protocols show some patients achieving 22-month survival with favorable genetic markers.
2. How long can you live with glioblastoma?
Most patients live 12-15 months after diagnosis with treatment. Younger patients (18-44 years) achieve median survival of 28 months, while those over 65 average 7-10 months. Individual survival depends on age, MGMT methylation status, extent of surgery, and treatment response.
3. What is glioblastoma multiforme?
Glioblastoma multiforme is the most aggressive Grade IV brain cancer originating from astrocyte cells. It’s characterized by rapid growth, microscopic brain tissue infiltration, and cellular heterogeneity. The term “multiforme” refers to the varied appearance of tumor cells under microscopic examination.
4. What are the stages of glioblastoma?
Glioblastoma is already Grade IV (stage 4) at diagnosis—the most advanced stage. Modern classification focuses on molecular markers: IDH-wildtype (aggressive, 12-15 month survival) versus IDH-mutant (28+ month survival). MGMT methylation status further stratifies prognosis within these categories.
5. What causes glioblastoma?
Approximately 80% of glioblastoma cases develop spontaneously without identifiable cause. The only proven environmental risk factor is ionizing radiation exposure. Rare inherited genetic syndromes (Li-Fraumeni, neurofibromatosis type 1) account for fewer than 5% of cases.
6. What are early glioblastoma symptoms?
Early symptoms include severe new-onset headaches (worse when lying down), seizures without prior history, progressive weakness or numbness, personality/cognitive changes, vision problems, and speech difficulties. Symptoms typically develop over 3-6 months as the tumor grows.
7. What is MGMT methylation and why does it matter?
MGMT methylation silences a DNA repair gene, making tumor cells vulnerable to chemotherapy. Patients with MGMT-methylated tumors achieve 24.6-month median survival versus 14.1 months for unmethylated tumors—a 40% reduction in mortality risk. Testing is essential for treatment planning.
8. What are the treatment options for stage 4 glioblastoma?
Standard treatment includes maximal surgical resection followed by radiation (60 Gy over 6 weeks) with concurrent temozolomide chemotherapy, then 6 months of maintenance temozolomide. Additional options include tumor-treating fields (Optune), bevacizumab for recurrence, and clinical trial immunotherapies.
9. Can glioblastoma be cured?
Glioblastoma currently has no cure due to microscopic brain infiltration beyond surgical/radiation reach, blood-brain barrier limiting drug delivery, and cellular heterogeneity causing treatment resistance. However, long-term survivors exist—UCLA’s vaccine trial showed 30% of patients surviving 3+ years.
10. What is the brain cancer survival rate compared to glioblastoma?
The overall brain and nervous system cancer 5-year survival rate is 33%, while glioblastoma specifically has <10% five-year survival. Glioblastoma represents the most lethal brain tumor type, significantly lowering overall brain cancer survival statistics.
11. Are there any promising new treatments for glioblastoma in 2025?
Yes. Mayo Clinic’s 2025 hypofractionated radiation achieved 56% one-year survival. UCLA’s personalized dendritic cell vaccine showed 30% three-year survival. CAR-T immunotherapies, dual checkpoint inhibitors, and over 300 active clinical trials offer hope for improved future outcomes.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











