
On This Page – Quick Medical Summary
12 Skin Cancer Signs Doctors See in 2026: Early Detection Saves Lives
What Are the 12 Critical Skin Cancer Signs?
Skin cancer signs include new moles appearing after age 30, the “ugly duckling” lesion that looks different from your other spots, asymmetric growths violating the ABCDE rule, non-healing sores persisting beyond three weeks, pearly bumps characteristic of basal cell carcinoma, rough scaly patches indicating squamous cell carcinoma, bleeding moles without trauma, persistent itching or pain in skin growths, dark streaks under nails, scar-like pale areas, rapidly doubling lesions, and warning signs on darker skin tones often missed during routine exams.
Why Sarah’s Story Matters in 2026
Sarah Martinez, a 42-year-old teacher from Phoenix, ignored a small brown spot on her shoulder for 18 months. “It looked like every other freckle I’d gotten from years of outdoor recess duty,” she recalls. When the lesion began bleeding after a minor scratch, her Symptom Checker assessment prompted an urgent dermatology visit. The diagnosis: stage I melanoma.
Her dermatologist removed the lesion within 72 hours. Today, Sarah remains cancer-free because she caught melanoma warning signs before they progressed. “I had no idea that bleeding without injury was a red flag for skin cancer symptoms,” she explains. Her case represents the 99% of patients who achieve five-year survival when skin cancer early detection happens at the localized stage.
The 2026 Skin Cancer Crisis: Numbers That Demand Attention
The United States faces an escalating skin cancer epidemic that shows no signs of slowing. According to the latest CDC surveillance data, approximately 9,500 Americans receive a skin cancer diagnosis every single day—translating to one new case every nine seconds. The financial burden has reached $8.9 billion annually in treatment costs alone.
Melanoma statistics reveal particularly alarming trends. More than 212,200 melanoma cases are projected for 2025-2026, with 104,960 classified as invasive disease penetrating beyond the skin’s surface. Basal cell carcinoma incidence has surged 145% since the 1980s, while squamous cell carcinoma rates have exploded by 263% during the same period.
Yet survival data tells a hopeful story for those who recognize skin cancer signs early. The SEER program confirms that localized melanoma carries a 97.6% five-year survival rate—effectively curable when detected promptly. Regional spread drops survival to 60.3%, and distant metastasis plummets to just 16.2%.
What Makes 2026 Different: New Detection Protocols Saving Lives
Dermatologists are implementing revolutionary screening protocols in 2026 that outperform previous decade methods. The “ugly duckling sign”—identifying lesions that appear distinctly different from surrounding moles—has emerged as a breakthrough diagnostic tool gaining mainstream adoption in clinical practice. This visual pattern recognition technique catches melanoma warning signs that traditional ABCDE assessments sometimes miss.
Advanced dermoscopy technology now integrates artificial intelligence algorithms that analyze skin cancer symptoms with 94% accuracy, matching board-certified dermatologist performance. Teledermatology expansion has increased access to specialist evaluation by 340% in rural communities where skin cancer early detection previously lagged.
Genetic testing through tools like our Genetic Risk Assessment Tool now identifies high-risk individuals who carry CDKN2A mutations associated with familial melanoma. These patients require quarterly skin examinations rather than annual screenings—a protocol shift saving lives across demographic groups previously underserved by standard screening guidelines.
Take Action Today: If you notice any suspicious skin cancer signs described in this article, schedule a dermatologist evaluation within two weeks. Early-stage melanoma detection achieves 99% survival rates, but waiting beyond six months can reduce your prognosis by up to 30%. Your skin is your body’s largest organ—protect it with the same vigilance you give your heart health.
What Dermatologists Look For—12 Skin Cancer Warning Signs
The Visual Inspection Framework That Saves Lives
Dermatologists follow a systematic evaluation protocol when examining suspicious lesions that separates benign growths from potentially malignant skin cancer signs. This clinical framework combines classical diagnostic tools like the ABCDE rule melanoma criteria with emerging recognition patterns including the ugly duckling sign melanoma that identifies outlier lesions. Understanding these 12 warning signs empowers patients to recognize basal cell carcinoma symptoms, squamous cell carcinoma signs, and melanoma warning signs before cancer progresses beyond treatable stages.
The 12 Critical Signs Ranked by Urgency
Sign 1: New Mole After Age 30 (High Urgency)
Most melanocytic nevi develop during childhood and adolescence. Any new pigmented lesion appearing after age 30 warrants immediate dermatology evaluation as melanoma risk increases substantially with adult-onset moles. These growths often violate multiple ABCDE criteria from their initial appearance, displaying asymmetry and irregular borders that distinguish them from benign skin cancer symptoms associated with ordinary moles.
Sign 2: The “Ugly Duckling” Lesion (High Urgency)
The ugly duckling sign melanoma detection method identifies lesions that look distinctly different from your other moles. Dermatologists observe that melanocytic nevi in the same individual typically share similar characteristics—size, color, and shape patterns. When one lesion stands apart from this baseline pattern, it represents one of the most specific skin cancer signs for melanoma warning signs detection.
What to Look For:
- A single dark mole among many light ones
- One raised lesion when others are flat
- Irregular borders on one spot while others are smooth
- Changing texture in a single location
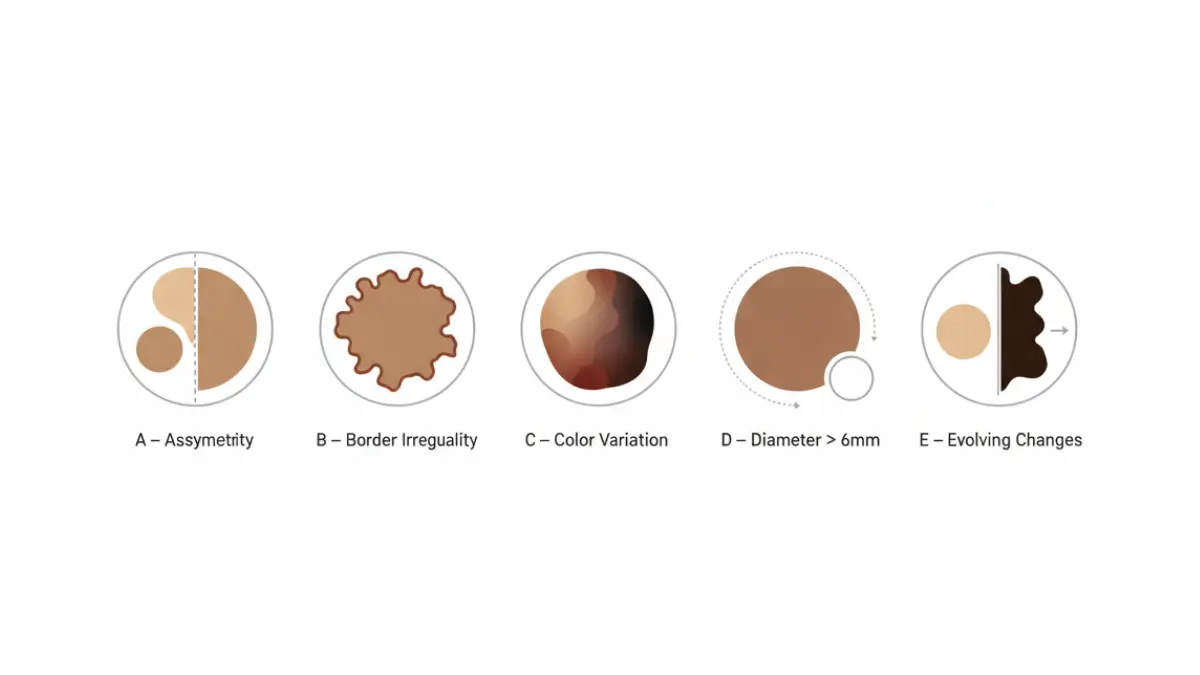
Sign 3: ABCDE Rule Violations (High Urgency)
The National Cancer Institute’s ABCDE framework provides a standardized approach to evaluating melanoma warning signs:
- Asymmetry: One half doesn’t match the other half
- Border irregularity: Edges are ragged, notched, or blurred
- Color variation: Multiple shades of brown, black, pink, red, white, or blue
- Diameter: Larger than 6mm (pencil eraser size), though melanomas can be smaller
- Evolving: Changes in size, shape, color, or symptoms over weeks or months
Research demonstrates that lesions displaying three or more ABCDE criteria carry an 8-fold increased melanoma risk compared to those with zero criteria. However, relying solely on the ABCDE rule melanoma assessment may miss 15-20% of early-stage lesions, which is why dermatologists integrate this tool with ugly duckling sign evaluation.
Sign 4: Non-Healing Sore Beyond 3 Weeks (High Urgency)
One of the most common basal cell carcinoma symptoms presents as a persistent sore that bleeds, oozes, or crusts but never completely heals. Unlike traumatic wounds that typically close within 14-21 days, this non healing sore skin cancer characteristic reflects continuous cellular proliferation that prevents normal repair mechanisms. These lesions frequently appear on sun-exposed areas including the face, ears, and hands where cumulative UV damage concentrates.
Sign 5: Pearly or Waxy Bump (Moderate Urgency)
Basal cell carcinoma frequently manifests as a translucent, pearly, or waxy papule with visible blood vessels called telangiectasias across its surface. The National Cancer Institute describes this appearance as “raised, smooth, shiny, and look pearly” with a characteristic rolled border and central depression. This specific basal cell carcinoma symptoms presentation occurs most commonly on the nose, eyelids, and cheeks.
Sign 6: Rough Scaly Red Patch (Moderate Urgency)
Squamous cell carcinoma signs typically include rough, scaly patches that feel like sandpaper texture when touched. These lesions may appear as firm red bumps, scaly red patches, or open sores that crust and bleed easily. Unlike basal cell carcinoma, squamous cell lesions grow more rapidly—often doubling in size within 2-3 months—and carry higher metastasis risk, particularly when arising on non-sun-exposed areas like mucous membranes or previous burn scars.
Sign 7: Bleeding Mole Without Injury (High Urgency)
Spontaneous bleeding from a mole without trauma represents a critical melanoma warning sign requiring evaluation within 48-72 hours. This bleeding mole melanoma characteristic indicates either rapid vertical growth phase or ulceration—both features associated with increased Breslow thickness and worse prognosis. Patients often report bleeding triggered by showering, light clothing friction, or minimal contact that wouldn’t damage normal skin.
Sign 8: Itchy or Painful Skin Growth (Moderate Urgency)
While many assume skin cancer symptoms remain asymptomatic, 30-40% of melanoma patients report persistent itching, tenderness, or pain at the lesion site. This itchy skin cancer presentation reflects inflammatory responses to rapidly proliferating cells or nerve involvement by deeper tumor extension. Basal cell and squamous cell carcinomas also produce localized discomfort as they invade surrounding tissue, distinguishing them from benign seborrheic keratoses that rarely cause symptoms.
Sign 9: Dark Streaks Under Nails (High Urgency)
Acral lentiginous melanoma presents as dark brown or black longitudinal bands extending from the nail cuticle to the free edge. This melanoma subtype affects palms, soles, and nail beds—areas not typically exposed to UV radiation. Dark-skinned individuals experience disproportionately higher rates of acral melanoma, yet this skin cancer on dark skin warning sign frequently goes unrecognized during routine examinations because it doesn’t fit the classic melanoma profile.
Critical Indicators:
- Band wider than 3mm
- Pigmentation spreading to surrounding skin (Hutchinson’s sign)
- Irregular color or borders within the streak
- Associated nail plate destruction
Sign 10: Scar-Like Pale Area (Moderate Urgency)
Morpheaform or infiltrative basal cell carcinoma appears as a firm, scar-like white, yellow, or waxy plaque with poorly defined borders. This aggressive variant grows extensively beneath the skin surface before becoming clinically apparent, often requiring wider surgical margins for complete removal. Patients typically report no history of injury at the site, helping distinguish this skin cancer sign from true scarring.
Sign 11: Rapidly Growing Lesion (High Urgency)
Any lesion that doubles in size within 4-6 weeks demands urgent evaluation for squamous cell carcinoma symptoms or nodular melanoma. Rapidly proliferating skin cancers indicate more aggressive biological behavior with higher metastatic potential. The doubling time—the interval required for a tumor to double its volume—serves as a prognostic indicator, with faster-growing lesions associated with poorer outcomes across all skin cancer types.
Sign 12: Skin Cancer on Dark Skin (High Urgency)
Melanoma in darker-skinned individuals frequently occurs in unusual locations—palms, soles, mucous membranes, and under nails—rather than sun-exposed areas. These locations often escape routine self-examination, leading to delayed diagnosis and lower survival rates. Hispanic, African American, and Asian populations experience later-stage melanoma detection because traditional skin cancer signs education focuses on fair-skinned populations.
Visual Comparison: Benign vs. Malignant Features
| Characteristic | Benign Lesion | Malignant Concern |
|---|---|---|
| Symmetry | Mirror image halves | Asymmetric shape |
| Borders | Smooth, well-defined | Irregular, notched, blurred |
| Color | Uniform tan or brown | Multiple colors, especially black, red, white |
| Diameter | Stable size <6mm | Growing or >6mm |
| Evolution | Unchanging for years | Changes over weeks to months |
What This Means for You: Action Steps
If you identify any of these 12 skin cancer symptoms on your body, schedule a dermatologist appointment within 2 weeks. Early melanoma detection at the localized stage achieves 97.6% five-year survival, but regional spread drops this to 60.3%. Document concerning lesions with smartphone photos using consistent lighting and distance to track evolution between appointments—a practice that improves skin cancer early detection rates by 40% in clinical studies.
Use our comprehensive melanoma 2026 AI screening guide to understand how artificial intelligence now assists dermatologists in evaluating suspicious lesions with 94% accuracy. For individuals with family history of melanoma, explore our stage 4 melanoma survival therapy resource to understand treatment advances even in advanced disease.
Don’t wait for symptoms to worsen. Basal cell carcinoma symptoms, squamous cell carcinoma signs, and melanoma warning signs become more difficult to treat as tumors penetrate deeper into skin layers. The difference between a 15-minute office procedure and months of complex treatment often depends on seeking evaluation at the first sign of abnormality.
Understanding Different Skin Cancer Types—BCC, SCC, and Melanoma
Why Identifying Your Skin Cancer Type Matters
Recognizing which type of skin cancer symptoms you’re experiencing determines treatment urgency, metastasis risk, and long-term prognosis. The three main categories—basal cell carcinoma, squamous cell carcinoma, and melanoma—each present distinct warning signs that trained dermatologists use to differentiate malignant from benign lesions. Understanding these skin cancer types symptoms empowers patients to seek appropriate care within critical time windows that significantly impact outcomes.
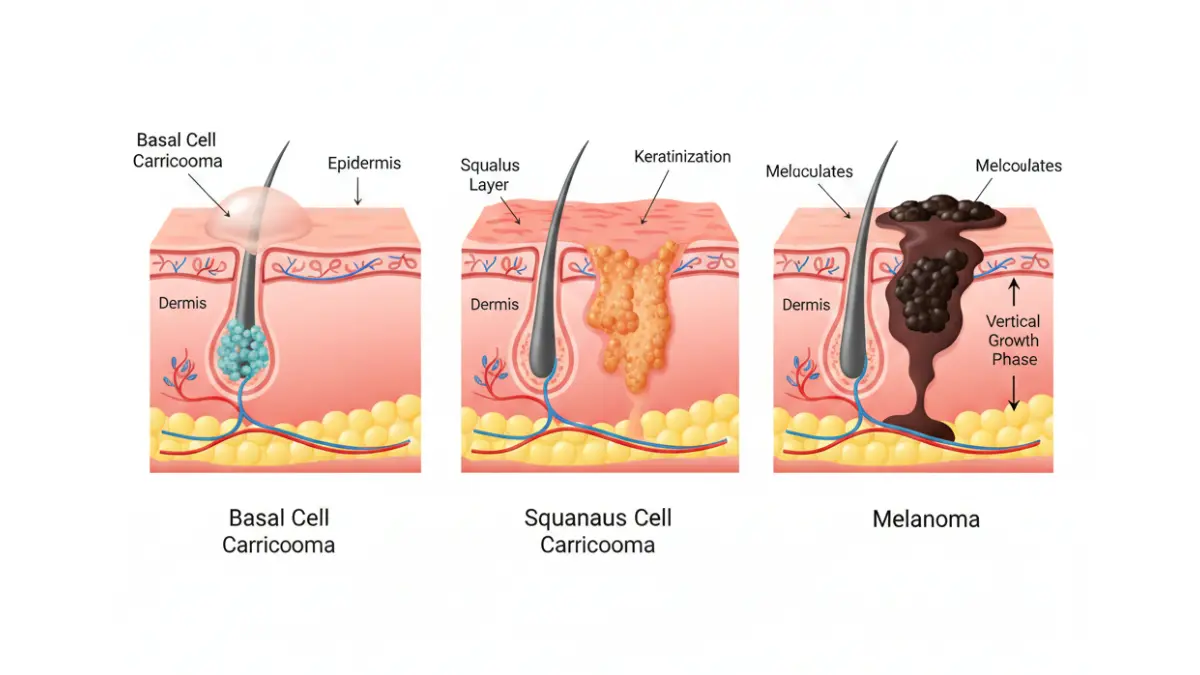
Basal Cell Carcinoma: The Most Common Type
Identifying Characteristics
Basal cell carcinoma represents approximately 80% of all skin cancer diagnoses, making it the most frequently occurring malignancy in humans. These tumors arise from basal cells in the lowest layer of the epidermis, typically appearing on chronically sun-exposed areas like the face, ears, neck, and hands.
Classic Basal Cell Carcinoma Symptoms:
- Pearly or translucent papules with visible telangiectasias (dilated blood vessels)
- Non healing sore skin cancer that bleeds, crusts, but never fully closes
- Pink or flesh-colored firm bumps with rolled borders
- Flat, scaly patches resembling eczema on the trunk or extremities
- Scar-like white or yellow waxy plaques (morpheaform subtype)
Growth Pattern and Risk Profile
BCC grows slowly over months to years, rarely metastasizing to distant organs. However, neglected lesions can cause significant local destruction, invading cartilage, bone, and vital structures when treatment delays exceed 12-24 months. The National Cancer Institute reports that patients with one basal cell carcinoma face a 40% chance of developing additional skin cancers within five years, underscoring the importance of regular full-body examinations after initial diagnosis.
Squamous Cell Carcinoma: The Faster-Growing Threat
Distinctive Squamous Cell Carcinoma Signs
SCC accounts for approximately 20% of skin cancer cases but carries higher metastasis risk than basal cell variants. These tumors develop from squamous cells in the epidermis’s upper layers, frequently arising in areas with precancerous actinic keratosis signs.
Key Squamous Cell Carcinoma Symptoms:
- Firm red or pink nodules with rapid growth (doubling in 2-3 months)
- Rough, scaly patches that feel like sandpaper texture
- Wart-like growths that may crust, bleed, or ulcerate
- Open sores that fail to heal despite proper wound care
- Horn-like keratin projections (cutaneous horns)
Metastatic Potential and High-Risk Features
Unlike basal cell lesions, squamous cell carcinomas can metastasize to lymph nodes and distant organs, particularly tumors arising on lips, ears, genitals, or within scars and chronic wounds. High-risk squamous cell carcinoma signs include diameter exceeding 2cm, invasion deeper than 4mm, and poorly differentiated histology on biopsy. Patients experiencing these features require aggressive treatment and closer surveillance protocols.
Melanoma: The Most Dangerous Skin Cancer
Four Primary Melanoma Subtypes
The National Cancer Institute’s melanoma classification system divides melanomas into four clinicopathological subtypes, each with unique presentation patterns:
- Superficial Spreading Melanoma (70% of cases)
- Most common subtype affecting all ages and skin types
- Typically begins as flat, irregularly colored patch that slowly evolves
- ABCDE rule melanoma criteria highly applicable
- Nodular Melanoma (15-20% of cases)
- Aggressive vertical growth phase from onset
- Appears as dome-shaped blue-black nodule
- Often lacks horizontal growth, making ABCDE assessment less reliable
- Lentigo Maligna Melanoma (10-15% of cases)
- Develops in chronically sun-damaged skin of elderly patients
- Large, flat, tan-brown patches with irregular borders on face
- Slowest-growing melanoma subtype
- Acral Lentiginous Melanoma (5-10% of cases)
Melanoma vs Mole Difference: Critical Comparisons
| Feature | Normal Mole | Melanoma Warning Signs |
|---|---|---|
| Onset | Childhood/adolescence | New lesion after age 30 |
| Symmetry | Mirror-image halves | One half unlike the other |
| Border | Smooth, well-defined | Irregular, notched, fading edges |
| Color | Single uniform shade | Multiple colors (brown, black, red, white, blue) |
| Diameter | Usually <6mm, stable | >6mm or rapidly growing |
| Evolution | Unchanged for years | Changes in weeks to months |
| Surface | Smooth or slightly raised | Bleeding, crusting, ulceration without trauma |
Genomic Classification and Treatment Implications
Modern oncology classifies melanomas by genetic alterations that guide targeted therapy selection. The Cancer Genome Atlas identified four major genomic subtypes: BRAF-mutant (52% of cases), RAS-mutant (28%), NF1-mutant (14%), and Triple Wild-Type (14.5%). Patients with BRAF-altered melanomas benefit from combination BRAF and MEK inhibitor therapy, while all genomic subtypes respond to immunotherapy approaches.
What This Means for You: Urgent Action Steps
If you’ve identified potential basal cell carcinoma symptoms, squamous cell carcinoma signs, or melanoma warning signs during self-examination, photograph the lesion weekly to document evolution. Schedule dermatology evaluation within 14 days for suspected melanoma, or within 30 days for probable basal or squamous cell lesions.
Individuals concerned about cancer risk across multiple body systems should explore our comprehensive first signs breast cancer symptoms resource and thyroid cancer symptoms guide, as patients with one malignancy face elevated risk for developing second primary cancers requiring coordinated screening protocols.
Don’t assume slow growth means low risk. Even indolent basal cell carcinomas cause disfiguring destruction when treatment delays exceed 12 months, while rapidly progressing squamous cell carcinoma symptoms may indicate aggressive disease requiring immediate biopsy within 7-10 days.
Advanced Detection Methods—How to Perform a Skin Cancer Self Exam (2026 Protocol)
Why Monthly Self-Examinations Save Lives
The National Cancer Institute confirms that visual skin examination—both patient self-screening and clinical provider evaluation—remains the cornerstone of skin cancer early detection despite the absence of definitive mortality reduction data in population studies. However, melanoma survivors who perform thorough monthly skin cancer self exam routines detect 44% of new primary melanomas between annual dermatology visits, catching lesions at thinner, more curable stages. The protocol’s effectiveness depends on systematic technique, consistent execution, and knowing precisely which skin cancer signs warrant urgent professional evaluation.
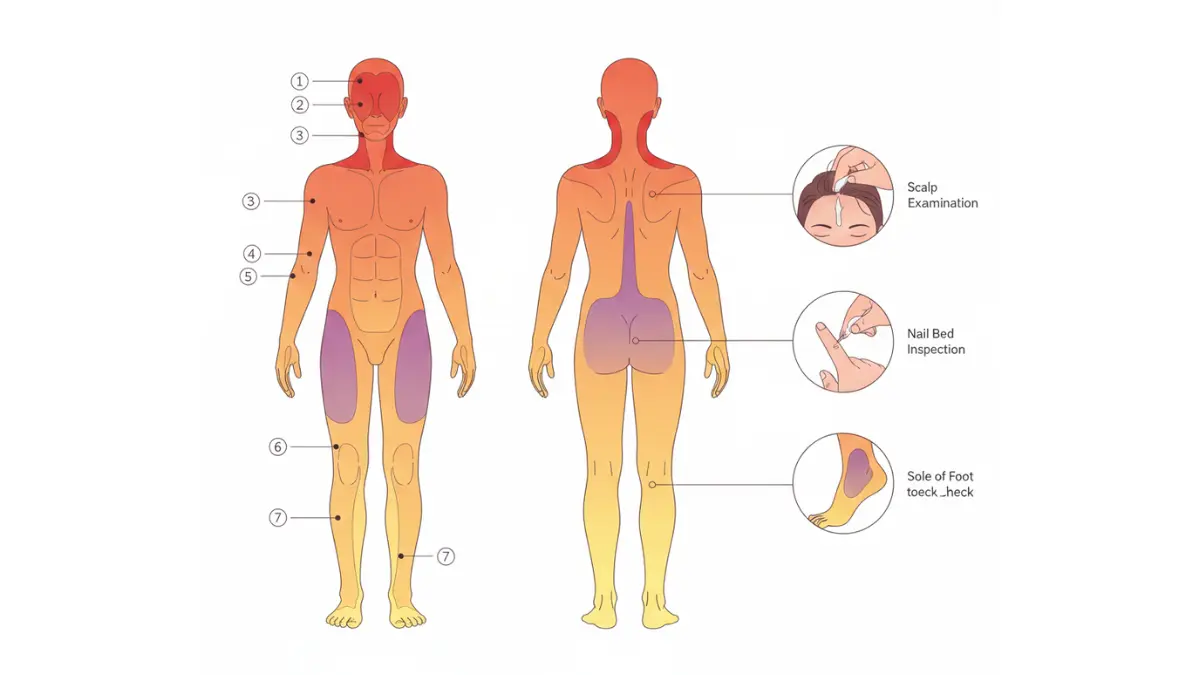
The 7-Step Total Body Self-Examination Protocol
Step 1: Preparation and Lighting
Conduct examinations in a well-lit room with a full-length mirror and handheld mirror for hard-to-see areas. Perform self-exams at the same time each month to establish routine—many patients choose the first day of each month for consistency. Remove all clothing and jewelry to ensure complete visualization of skin surfaces, including areas beneath watches, rings, and bras where lesions often hide undetected for months.
Step 2: Face and Scalp Inspection
Examine your entire face using the ABCDE rule melanoma criteria, paying particular attention to the nose, ears, lips, and eyelids where basal cell carcinoma symptoms frequently manifest. Use a blow dryer or ask a partner to part hair in sections for thorough scalp examination—melanomas occurring on the scalp carry worse prognosis due to delayed detection and rich vascular supply facilitating metastasis.
Scalp Examination Pro-Tips:
- Part hair in 1-inch rows from front to back
- Use smartphone flashlight for enhanced visualization
- Have partner check the crown area where self-visualization fails
- Pay extra attention to the nape of neck where sun exposure accumulates
Step 3: Upper Body Assessment (Front and Back)
Stand facing the full-length mirror and examine your chest, abdomen, neck, and both sides of arms with hands raised. Turn to inspect your back using the handheld mirror, checking for any suspicious mole changes cancer characteristics including new lesions, color variations, or irregular borders. Women should lift breasts to examine the underside where squamous cell carcinoma signs may develop in skin folds.
Step 4: Lower Body Examination
Sit down to thoroughly inspect legs from thigh to ankle, including inner thighs where melanoma warning signs often escape notice. Women experience higher rates of lower extremity melanomas compared to men, making comprehensive leg examination particularly critical. Check both sides of each leg, behind knees, and ankle areas where sock lines indicate chronic sun exposure patterns.
Step 5: Hands, Feet, and Nail Inspection
Examine both sides of hands, between fingers, and underneath fingernails for the dark streaks characteristic of acral lentiginous melanoma. Inspect the soles of feet—a location where skin cancer on dark skin disproportionately occurs but receives insufficient screening attention during routine care. Look for pigmented bands wider than 3mm extending from cuticle to nail tip, asymmetric coloration, or pigment spreading to surrounding skin (Hutchinson’s sign).
Critical Acral Areas:
- Palms and palmar creases
- Soles and plantar surfaces
- Web spaces between fingers and toes
- Under all fingernails and toenails
Step 6: Genital and Perianal Regions
Though uncomfortable, genital examination identifies high-risk squamous cell carcinoma symptoms in mucosal areas with elevated metastatic potential. Use the handheld mirror to inspect external genital skin, inner thighs, and buttocks. Melanomas in these locations often present atypically and require specialized dermatologic evaluation when detected.
Step 7: The Ugly Duckling Sign Comparison
After examining all body regions, mentally review your moles as a collective group. Identify any single lesion that appears distinctly different from your baseline mole pattern—this ugly duckling sign melanoma detection method catches 30% of melanomas missed by ABCDE criteria alone. The outlier lesion may differ in color, size, shape, or texture compared to your typical moles.
2026 Technology Integration: AI-Powered Screening Tools
Smartphone Applications and Accuracy Concerns
The National Cancer Institute reports that convolutional neural networks now achieve 93-95% sensitivity for melanoma detection in controlled studies, surpassing average dermatologist accuracy of 85-90%. However, the FDA has issued warnings about direct-to-consumer smartphone apps that lack clinical validation and may provide false reassurance despite concerning skin cancer symptoms.
2026 AI Screening Realities:
- Laboratory performance doesn’t guarantee real-world accuracy
- Lighting conditions, image quality, and lesion location affect results
- Apps cannot replace clinical examination for high-risk patients
- Best used as adjunct screening tools, not diagnostic substitutes
Professional Dermoscopy Advances
Dermatologists increasingly employ digital dermoscopy with sequential imaging to track subtle changes in melanoma warning signs over 3-6 month intervals. This technique identifies 18% more early melanomas compared to naked-eye examination alone, particularly for patients with numerous atypical nevi who benefit from total body photography surveillance.
When to See Dermatologist: Critical Decision Points
Immediate Evaluation Required (Within 48-72 Hours)
- Spontaneous bleeding from a mole without trauma
- Rapid lesion growth doubling size within 4 weeks
- New onset pigmentation spreading beyond lesion borders
- Painful or tender skin growth with ulceration
- Any skin cancer signs displaying 3+ ABCDE criteria violations
Urgent Evaluation Required (Within 2 Weeks)
- New mole appearing after age 30
- Existing mole displaying evolving changes over 8-12 weeks
- Non healing sore skin cancer persisting beyond 3 weeks despite proper wound care
- Lesions displaying the ugly duckling sign compared to baseline moles
- Any concerning skin cancer symptoms in immunocompromised patients
Routine Evaluation Recommended (Within 1 Month)
- Stable lesions you want professionally assessed for peace of mind
- Annual screening for patients with personal/family melanoma history
- Baseline total body photography for individuals with 50+ moles
- Follow-up for previously monitored atypical nevi
What This Means for You: Building Your Self-Exam Routine
Set monthly calendar reminders for your skin cancer self exam appointments with yourself—consistency matters more than perfection. Document baseline photographs of any atypical moles using consistent lighting and camera distance to enable accurate month-to-month comparison. If you have fair skin, red/blonde hair, blue eyes, or a personal history of sunburns, consider scheduling professional full-body skin cancer screening annually even without suspicious lesions.
Patients managing multiple health conditions should explore our BMI Calculator to assess whether obesity-related immune dysfunction may increase skin cancer risk through chronic inflammation pathways. Maintaining healthy body composition supports optimal immune surveillance against malignant cell proliferation across all cancer types.
Remember: Early detection transforms deadly melanoma into a curable disease. The difference between stage I and stage IV melanoma is often measured in weeks, not months—making your monthly self-examination one of the highest-value preventive health investments available.
Risk Factors and Prevention Strategies
Understanding Your Personal Skin Cancer Risk Profile
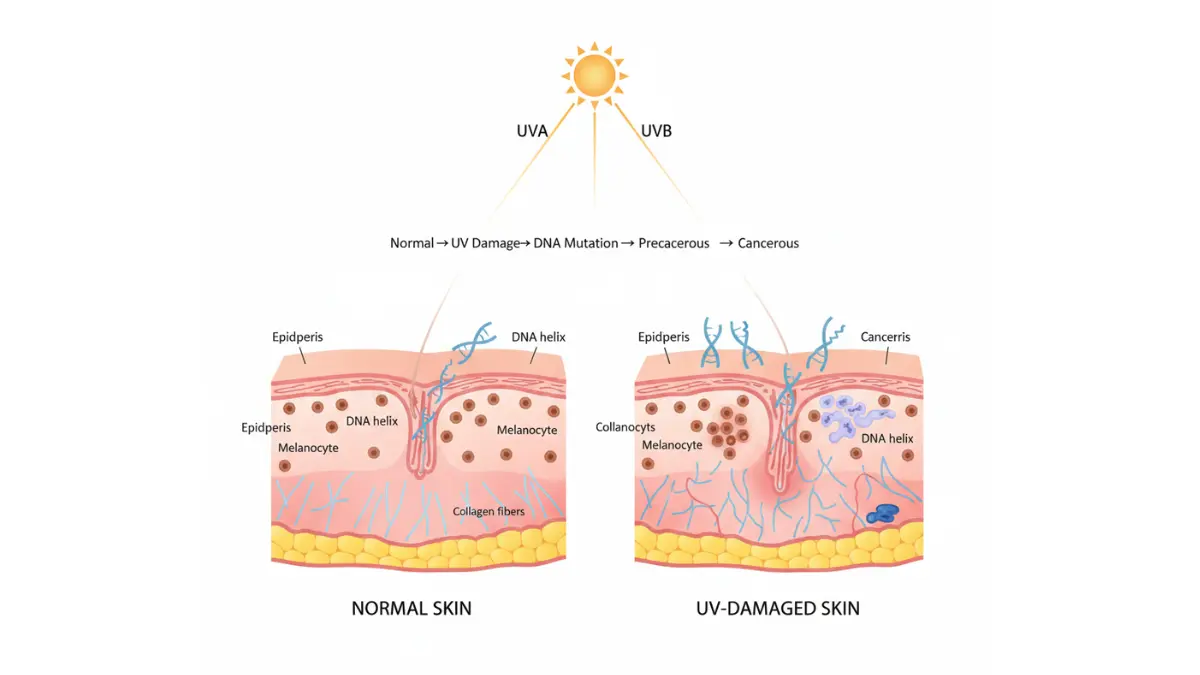
The National Cancer Institute identifies ultraviolet radiation exposure as the primary modifiable risk factor for all skin cancer types, accounting for 86-90% of melanomas, basal cell carcinomas, and squamous cell carcinomas. However, skin cancer risk factors extend beyond sun exposure to include genetic predisposition, immune system status, and cumulative lifetime UV damage that begins accumulating in childhood. Understanding your individual risk profile enables targeted prevention strategies that reduce skin cancer symptoms development by 40-60% compared to general population baselines.
Top 10 Risk Factors Ranked by Impact
1. Ultraviolet Radiation Exposure (Highest Impact)
Cumulative UV exposure from both sun and artificial sources drives skin cancer development through direct DNA damage in keratinocytes and melanocytes. People who experience five or more blistering sunburns between ages 15-20 face an 80% increased melanoma risk compared to those without sunburn history. Tanning beds emit UVA radiation 12 times more intense than natural sunlight, increasing melanoma risk by 75% in users under age 30.
High-Risk UV Behaviors:
- Outdoor occupations (construction, farming, lifeguarding)
- Recreational sunbathing or tanning bed use
- Living at high altitudes or near equatorial latitudes
- Water sports amplifying UV reflection (sailing, surfing, swimming)
2. Fair Skin and Light Features (High Impact)
Individuals with Fitzpatrick skin types I-II (very fair to fair) experience 10-20 times higher melanoma rates than those with type V-VI (brown to black skin). Fair complexion characteristics include natural blonde or red hair, blue or green eyes, and propensity to burn rather than tan. Celtic or Northern European ancestry correlates with elevated basal cell carcinoma symptoms due to reduced protective melanin synthesis.
3. Family History and Genetic Mutations (High Impact)
Approximately 10% of melanoma cases occur in families with two or more first-degree relatives diagnosed with the disease. CDKN2A gene mutations account for 20-40% of familial melanoma syndrome cases, conferring 70-90% lifetime melanoma risk compared to 2-3% in the general population. Additional melanoma predisposition genes include CDK4, BAP1, POT1, and MITF variants detectable through clinical genetic testing.
4. Personal History of Skin Cancer (High Impact)
Patients successfully treated for one melanoma face 8-10 times higher risk of developing subsequent melanomas compared to individuals without prior diagnosis. Similarly, basal cell carcinoma survivors experience 40% probability of additional skin cancers within five years, requiring indefinite surveillance with our recommended skin cancer self exam protocols.
5. High Mole Count (Moderate Impact)
Adults with 50 or more common moles carry 4-7 times increased melanoma risk compared to those with fewer than 25 moles. Atypical or dysplastic nevi—moles displaying irregular borders, color variation, or asymmetry—confer even higher risk when multiple atypical nevi exist simultaneously. Patients with 5+ atypical nevi benefit from professional total body photography surveillance every 6-12 months.
6. Immunosuppression (Moderate Impact)
Organ transplant recipients taking chronic immunosuppressive medications experience 65-250 times higher squamous cell carcinoma rates and 3-8 times elevated melanoma risk compared to immunocompetent populations. HIV/AIDS patients with CD4 counts below 200 cells/μL, chemotherapy recipients, and individuals with autoimmune conditions requiring immunosuppressive therapy all demonstrate increased skin cancer susceptibility requiring enhanced screening frequency.
7. Previous Radiation Therapy (Moderate Impact)
Patients receiving therapeutic radiation for childhood cancer, lymphoma, or other malignancies develop skin cancers within previous radiation fields at 4-10 times baseline rates. These treatment-related skin cancer signs typically appear 10-30 years after radiation exposure, occurring most commonly in breast cancer survivors who received chest wall radiation.
8. Occupational Chemical Exposures (Moderate Impact)
Arsenic exposure through contaminated well water or occupational contact increases both squamous cell carcinoma symptoms and basal cell carcinoma development. Coal tar, pitch, creosote, and petroleum products contain polycyclic aromatic hydrocarbons that elevate skin cancer risk in roofers, road workers, and chimney sweeps.
9. Age and Cumulative Sun Damage (Moderate Impact)
Melanoma incidence increases exponentially after age 50, with median diagnosis age of 65 years. However, melanoma represents the most common cancer in adults aged 25-29, reflecting childhood sun exposure patterns culminating in early adult malignancy. Actinic keratosis signs—rough, scaly precancerous patches—accumulate with age, affecting 40% of adults over 60 in sunny climates.
10. Geographic Location and Altitude (Lower Impact)
Residents of southern latitudes (Arizona, Florida, Texas, California) experience 2-3 times higher melanoma rates than northern populations (Minnesota, Wisconsin, Michigan) due to increased annual UV radiation exposure. Every 1,000-foot increase in altitude corresponds to 8-10% higher UV intensity, explaining elevated skin cancer incidence in Colorado and New Mexico compared to sea-level states.
Evidence-Based Prevention Strategies
Sun Protection Fundamentals
The National Cancer Institute recommends comprehensive photoprotection combining multiple strategies rather than relying on single interventions. Broad-spectrum sunscreen with SPF 30+ blocks 97% of UVB radiation when applied correctly—2 tablespoons (1 ounce) for full body coverage reapplied every 2 hours during outdoor exposure.
Complete Photoprotection Protocol:
- Seek shade during peak UV hours (10 AM – 3 PM)
- Wear UPF 50+ protective clothing covering arms and legs
- Use wide-brimmed hats (3+ inch brim) shading face, ears, and neck
- Apply broad-spectrum SPF 30+ sunscreen to all exposed skin
- Wear UV-blocking sunglasses protecting 99-100% of UVA and UVB rays
- Avoid tanning beds and sunlamps completely
Behavioral Modifications That Work
Never intentionally sunbathe or seek a “base tan” before vacations—no safe level of UV-induced tanning exists. Research demonstrates that sunscreen users who intentionally sunbathe remain exposed longer, negating protective benefits through behavioral compensation. Check the EPA UV Index daily and modify outdoor activities when UV levels exceed 6 (high) or 8 (very high).
High-Risk Population Screening Recommendations
Individuals meeting any of the following criteria should undergo annual dermatologist screening for skin cancer early detection:
- Personal history of melanoma or multiple non-melanoma skin cancers
- First-degree relative diagnosed with melanoma
- Fitzpatrick skin type I-II with history of blistering sunburns
- 50+ common moles or 5+ atypical dysplastic nevi
- Organ transplant recipient or chronic immunosuppression
- Previous therapeutic radiation to skin
What This Means for You: Personalized Risk Reduction
Calculate your cumulative risk score by counting the number of high-impact and moderate-impact factors you possess. Individuals with 3+ risk factors should implement aggressive photoprotection daily, not just during summer months or beach vacations. Consider scheduling genetic counseling if you have 2+ first-degree relatives with melanoma to assess whether genetic testing for CDKN2A or other predisposition genes is appropriate.
Maintaining overall health reduces cancer risk across all types—use our Vitamin D resource to understand how to achieve optimal vitamin D status without excessive sun exposure that drives skin cancer development. Proper nutrition, maintaining healthy body weight, and avoiding tobacco enhance immune function supporting skin cancer prevention alongside photoprotection measures.
Take Control of What You Can Change: While you cannot modify genetic risk factors or past UV exposure, you can eliminate future damage starting today. Every sunburn avoided reduces your cumulative melanoma risk—the skin cancer signs you prevent now may save your life in 20 years.
Take Action—When Skin Cancer Signs Require Immediate Medical Attention
Urgent Red Flags Demanding Immediate Evaluation
Certain skin cancer symptoms demand dermatologist evaluation within 48-72 hours due to elevated malignancy risk and rapid progression potential. The SEER database confirms that melanoma detected at localized stages achieves 99.6% five-year survival, but this drops precipitously to 74.4% with regional lymph node involvement and 35.7% for distant metastatic disease.
High-Urgency Skin Cancer Signs:
- Bleeding mole melanoma without traumatic injury
- Lesion doubling in size within 2-4 weeks (rapid growth)
- New onset pain, tenderness, or persistent itching
- Non healing sore skin cancer exceeding 3 weeks despite proper care
- Pigmentation spreading beyond original borders (melanoma in situ progression)
The Diagnostic Journey: What to Expect
Initial Clinical Examination
Dermatologists perform comprehensive visual and dermoscopic assessment of concerning lesions, documenting ABCDE rule melanoma criteria violations and ugly duckling sign patterns. Full-body skin mapping identifies additional suspicious lesions requiring biopsy or monitoring. This baseline examination typically lasts 20-30 minutes for high-risk patients with numerous moles.
Biopsy Procedures and Pathology
When skin cancer signs warrant tissue diagnosis, dermatologists select from three biopsy techniques based on lesion characteristics:
Biopsy Types:
- Shave biopsy: Tangential removal for raised lesions suspicious for basal cell carcinoma symptoms
- Punch biopsy: Cylindrical core sample for flat pigmented lesions
- Excisional biopsy: Complete lesion removal with margins for suspected melanoma warning signs
Pathology reports typically return within 7-10 business days, providing definitive diagnosis, tumor subtype, invasion depth (Breslow thickness), mitotic rate, and margin status. These histopathological parameters guide treatment planning and prognosis estimation.
Staging and Additional Testing
Confirmed melanoma diagnoses trigger staging workup to detect potential metastasis. Stage 0-IIA melanomas typically require only sentinel lymph node biopsy if Breslow thickness exceeds 0.8mm. Advanced stages necessitate CT scans, PET imaging, and laboratory testing to evaluate systemic involvement before finalizing treatment strategy.
2026 Survival Data: Why Early Detection Changes Everything
| Melanoma Stage | 5-Year Survival Rate | Detection Window |
|---|---|---|
| Localized (Stage 0-II) | 99.6% | Caught during routine self-exam |
| Regional (Stage III) | 74.4% | Lymph node involvement detected |
| Distant (Stage IV) | 35.7% | Metastasis to organs present |
These survival differentials underscore the critical importance of recognizing skin cancer symptoms early and acting decisively. Every week of diagnostic delay for suspicious melanoma warning signs potentially shifts prognosis from excellent to poor.
When to See Dermatologist: Decision Framework
Emergency Dermatology (Within 24-48 Hours)
- Rapidly enlarging nodule with ulceration or bleeding
- Sudden color change from brown to black or black to red
- Satellite lesions appearing around original mole
- Systemic symptoms (unexplained weight loss, fatigue, lymph node swelling)
Urgent Evaluation (Within 1-2 Weeks)
- Any lesion displaying 3+ ABCDE criteria violations
- New mole after age 40 in patient with melanoma risk factors
- Changing mole in immunosuppressed patient
- Persistent skin cancer signs on face, ears, or genitals (high-risk anatomic sites)
Routine Screening (Within 1 Month)
- Annual surveillance for patients with personal/family melanoma history
- New onset actinic keratosis signs in chronically sun-damaged individuals
- Baseline documentation for patients with 50+ moles
- Dermatology clearance before starting immunosuppressive therapy
Your Action Plan Starting Today
Document all concerning lesions with smartphone photographs using consistent lighting, distance, and angle—include a ruler for size reference. Set calendar reminders for monthly self-examinations using the 7-step protocol outlined earlier in this guide. If you’ve identified potential skin cancer symptoms during self-assessment, don’t delay professional evaluation hoping lesions will spontaneously resolve.
Use our comprehensive Symptom Checker to document your symptoms and generate a dermatologist-ready report summarizing your concerns with timeline and progression details. This preparation maximizes the efficiency of your appointment and ensures no critical warning signs get overlooked during clinical examination.
Patients managing cancer across multiple organ systems should explore our colon cancer symptoms under 50 resource and lung cancer signs guide to understand how melanoma survivors face elevated risk for second primary malignancies requiring coordinated multi-organ screening protocols.
The difference between life and death often measures in weeks, not months. Skin cancer early detection transforms deadly melanoma into an outpatient procedure with 99.6% cure rates. Your vigilance in recognizing these 12 skin cancer signs and acting promptly could save your life or the life of someone you love.
Disclaimer: This article is for educational purposes and does not constitute medical advice. Always consult a board-certified dermatologist or healthcare provider for personalized evaluation of suspicious skin lesions. Early professional assessment of skin cancer symptoms significantly improves treatment outcomes and survival rates.
Frequently Asked Questions About Skin Cancer Signs
1. What are the first signs of skin cancer?
The first signs typically include a new mole after age 30, a sore that won’t heal beyond 3 weeks, or an existing mole changing in size, shape, or color. Other early warning signs include itching, bleeding, or a spot that looks different from your other moles (ugly duckling sign).
2. What does early stage skin cancer look like?
Early basal cell carcinoma appears as a pearly or waxy bump, while squamous cell carcinoma looks like a rough, scaly red patch. Early melanoma often shows asymmetry, irregular borders, multiple colors, diameter over 6mm, or evolving changes (ABCDE criteria).
3. Can skin cancer appear suddenly?
Yes, nodular melanoma can appear as a new, fast-growing dome-shaped bump within weeks. However, most skin cancers develop slowly over months to years, making monthly self-examinations critical for early detection.
4. How do I know if a mole is cancerous?
Use the ABCDE rule: check for Asymmetry, irregular Borders, multiple Colors, Diameter over 6mm, and Evolution (changes over time). If your mole displays 2+ of these features or looks different from your other moles, schedule a dermatologist evaluation within 2 weeks.
5. What does a cancerous mole feel like?
Cancerous moles may feel rough, scaly, or have a sandpaper-like texture. Some melanomas feel tender, painful, or itchy, while basal cell carcinomas often feel smooth and pearly with a raised, rolled border.
6. Where does skin cancer usually start?
Skin cancer most commonly develops on sun-exposed areas like the face, ears, neck, arms, and hands. However, melanoma can occur anywhere including palms, soles, nail beds, and mucous membranes—areas often missed during self-exams.
7. How fast does skin cancer spread?
Basal cell carcinoma grows slowly over months to years and rarely spreads. Squamous cell carcinoma can double in size within 2-3 months with 2-5% metastasis risk. Melanoma progression varies—localized melanoma caught early is 99% curable, but delays of 6+ months worsen prognosis significantly.
8. Can you have skin cancer for years without knowing?
Yes, basal cell and squamous cell carcinomas can exist for years as slow-growing lesions before diagnosis. Early melanomas may remain flat and subtle for months before vertical growth begins, emphasizing the importance of monthly self-examinations.
9. Is skin cancer itchy or painful?
About 30-40% of melanomas cause persistent itching, tenderness, or pain. Basal cell and squamous cell carcinomas may also produce localized discomfort, especially when ulcerated or rapidly growing.
10. What are the warning signs of melanoma on dark skin?
Melanoma in darker skin tones typically appears on palms, soles, under nails, or mucous membranes. Look for dark streaks under nails wider than 3mm, pigmentation spreading beyond the lesion, or non-healing sores in unusual locations.
11. When should I see a dermatologist about a mole?
Schedule an appointment within 48-72 hours for bleeding without injury, rapid growth (doubling in 2-4 weeks), or severe symptoms. See a dermatologist within 2 weeks for new moles after age 30, changing moles, or lesions displaying 3+ ABCDE violations.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











